ON PATIENT CARE - Review of Optometry
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
24th edition
ON PATIENT CARE
Formerly “The Clinical Guide to Ophthalmic Drugs”
See the practice of
optometry through the
eyes of three experts.
Ron Melton, OD
Randall Thomas, OD, MPH
Patrick Vollmer, OD
A Supplement to
Supported by an unrestricted grant from Bausch + Lomb
FROM THE AUTHORS
CLINICAL
On the Virtues of Change PERSPECTIVES
ON PATIENT CARE
In a tumultuous year, we still have much to be excited about.
Section I:
T he COVID-19 virus has unequivocally altered all of our lives and practices. Two
of us (Drs. Melton and Thomas) have tested positive for the virus—and survived.
Once this terrible storm passes, however, our patients will once again be in need of
Strategies for Success
Page 3 See the practice of
optometry through the
eyes of three experts.
our professional services. We hope the clinical information in this supplement will
further equip you to more fully care for your patients in the post-COVID era. Section II:
Anterior Segment Care
Ron Melton, OD
You’ll also notice some radical changes to this annual publication. We are
broadening our scope of topics this year. Why? Because optometric practice has Page 18 Randall Thomas, OD, MPH
broadened, too. Simply giving a run-down of drug categories, as we did when this
started back in the 1990s, just doesn’t live up to the present moment for optometry. Section III: Patrick Vollmer, OD
Posterior Segment Care
A Supplement to
After nearly 25 years of producing a “drug guide,” we want you to get an up-close Supported by an unrestricted grant from Bausch + Lomb
look at how we three clinicians actually practice, and think about, all facets of Page 34
optometric care. Thus, Clinical Perspectives on Patient Care is born!
Imagine this supplement as a chance to sit alongside us as we consider literally Supported by an
hundreds of different day-to-day challenges. We’ll give you our unvarnished take unrestricted grant from
Bausch + Lomb
on all of them. If there is no literature reference, consider the statement to be our
professional opinion. Other doctors will no doubt have their own approaches, and
that’s fine. Our aim is not to present every conceivable idea—just our own, earned
through countless hours in the clinic.
For better or worse, we have now managed to accumulate over 80 combined years
of intensive clinical experience. Our practice pattern has always been to care for
patients with non-surgical eye conditions ourselves. We hold ophthalmic surgeons
in high regard, and are most happy to work collegially with them in caring for our
patients with surgical needs; otherwise, we manage the extensive gamut of medical eye Randall K. Thomas,
conditions within our own optometric practices. OD, MPH, FAAO
Rather than chapters per se, this new approach will share a somewhat random
selection of topics germane to bringing you up to date on a wide variety of eye
conditions and issues, organized in three main sections. Note that we cannot condense
four years of clinical training into a single supplement. We are assuming a strong
foundation of clinical knowledge by the reader, and are only attempting to add
succinct, salient “pearls” to this foundation.
Our goal in writing this guide is to help further equip our colleagues with
knowledge to provide a broader range of top-quality patient care services. Of all the Ron Melton,
conditions we need to master, the two most important ones are glaucoma and dry eye OD, FAAO
disease. We encourage you to attentively read these discussions, pay attention to the
professional journals and exhaustively seek lectures on glaucoma.
As always, we are grateful to Bausch + Lomb Pharmaceuticals for their unwavering
support of this optometric educational product through the years, and to the editorial
team at Review of Optometry for helping shape this supplement into a highly readable
work.
We hope and pray that each of you and your loved ones endure this viral assault,
and come out of this disaster stronger and more resolute than ever before. Patrick M. Vollmer,
OD, FAAO
With our best wishes,
Drs. Melton, Thomas and Vollmer
Disclosure: Drs. Melton and Thomas are consultants to, but have no financial interests in, the following
companies: Bausch + Lomb and Icare. Dr. Vollmer has no financial interests in any company.
A PEER-REVIEWED
Note: The authors present unapproved and “off-label” uses of specific drugs in this publication. SUPPLEMENT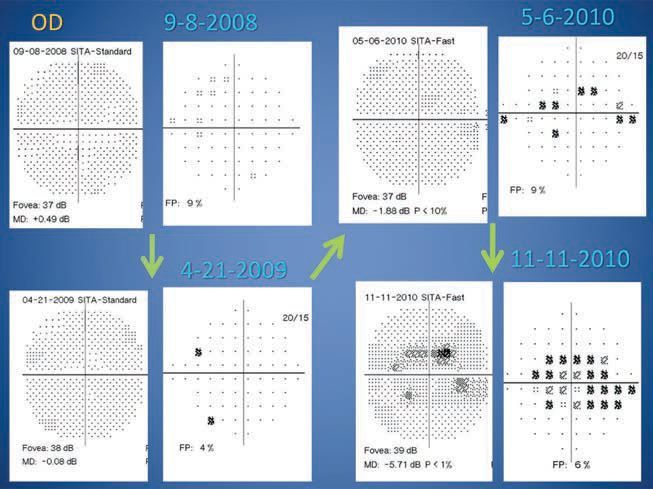
SECTION I: STRATEGIES FOR SUCCESS
Warning: Major Changes Coming to Optometry
If you think you can rely on dispensary income and routine eye exams, you may be
in for a rude awakening.
A
quick look at the profes- upon this reality, one could rationally
MEDICAL EYE CONDITIONS
sional literature clearly and accurately assume that the pub-
ALL ODs SHOULD MANAGE
shows major sea changes lic’s quest for competent, thorough,
• Assessing hydroxychloroquine
in how eye care is being medically-oriented eyecare is valued (Plaquenil) retinotoxicity risk
delivered. Online refractions, eye- far more than just “refraction.” This
• Diabetic retinopathy
glasses and contact lenses are already is a powerful observation, and one
available in many places of the world, that we should take to heart. • The glaucomas
and are now available in the United • Acute symptomatic posterior
vitreous detachments
States. The 3-D printers are making NO TIME TO WASTE
complete eyeglasses, and this technol- A comprehensive consensus of these • Acute red eyes: allergic, bacterial,
viral, chlamydial
ogy will only improve. Drugs to push observations should compel think-
back presbyopia will also be here ing optometrists to reevaluate their • Injuries and abrasions
soon, thus dampening the bifocal practice modus operandi and develop • Blepharitis
market. Autorefractors and auto- strategies to remain viable in the face • Meibomian gland dysfunction
mated subjective systems are already of these tidal waves of changes com- • Dry eye disease
here, and they too, will continue to ing our way. • Zoster ophthalmicus
improve. Eyeglasses are heavily pro- Our relatively straightforward • Eye pain: trichiasis, ectropion,
moted for as little as $6.95! plan is to simply begin keeping all entropion, lagophthalmos
The Department of Veterans the patients who present to us. Stated • Bell’s palsy
Affairs (VA) now has operational another way, it is imperative that we • Corneal dystrophies
programs in place in which layper- stop hemorrhaging patients through
• Optic neuritis
sons are trained to perform essen- referrals, and that we provide a much
• Macular degeneration
tially full eye examinations, including broader base of comprehensive medical
refraction, and patient satisfaction is care services; this is critical to our sur- • Presurgical cataract care
reported to be “high.” For decades, vival as a profession. For perspective, • Epiphora
ophthalmologists have had high the table at right is a near-comprehen- • Post-op care for numerous surgeries
school graduates performing their sive list of medical eye conditions • Lid infections: acute hordeola, styes
refractions, and people that attentive and caring • The gamut of contact lens
flock to their prac- ODs can readily complications
tices. Based address. • Episcleritis/scleritis
• Giant cell (temporal) arteritis
• Recurrent corneal erosion
THREATS TO OPTOMETRY • Contact blepharodermatitis
• Superior limbic keratoconjunctivitis
• Bargain-basement tactics by
STRATEGIES FOR SUCCESS
• Phlyctenular keratoconjunctivitis
eyewear discounters
• Eroding tarsal concretions causing
• Online refractions foreign body sensation
• Online contact lens sales • Thygeson’s superficial punctate
• Bottom line: dispensary is keratopathy
dying • Transient vision loss from carotid
artery disease
• Ocular migraines
• Corneal infiltrates and ulcers/CLARE
• Giant papillary conjunctivitis
• Epithelial basement membrane
assessment and monitoring
REVIEW OF OPTOMETRY JUNE 15, 2020 3
SECTION I: STRATEGIES FOR SUCCESS
radical some of these changes and Another resource to keep you
approaches may seem, but we im- attuned to the latest research is the
plore you to begin to become proac- website www.practiceupdate.com.
tive and not find yourselves scram- You can sign up to have a daily
bling to play “catch-up” when you email newsletter sent to you each
are faced with technological advance- morning with important studies in
ments; they indeed are coming. eye care.
Yet another way to increase your
KEEP UP WITH RESEARCH professional abilities is to call upon
A very enriching way to fast-forward a colleague to gain his or her advice.
your expertise in these areas is to There is nothing wrong in asking for
If you want to insulate your practice from
the threat of online refraction services,
subscribe (as we do) to the following help, or getting an opinion, but keep
evolve to a medical foundation. journals. These can be readily ac- your patients in your practice.
cessed via a simple Google search: What about being “on call”?
Caring for patients with these 1. Ophthalmology Doctors like to receive after-hours
conditions, especially the glaucomas, 2. American Journal calls about as much as patients like
holds massive potential for building of Ophthalmology undergoing air-puff tonometry; how-
a dynamic practice, and possesses a 3. JAMA Ophthalmology ever, as doctors we need to develop a
strong firewall against technological 4. Survey of Ophthalmology system whereby optometric patients
advancements into traditional op- You can read these journals solely have at least consultative access to
tometry. “Refraction” is a technical on your own, but perhaps a wiser optometric care outside of normal
procedure, and bright, sharp, friendly way to increase your knowledge base office hours.
high school graduates can be rapidly would be to develop monthly “jour- Here again is where coming to-
trained to perform this data-collec- nal clubs” where four of you each gether as teams provides the perfect
tion task, thus freeing the doctor up subscribe to one of these journals, solution. Find six or seven like-
to have more time doing those tasks then get together over a nice dinner minded, patient-centric colleagues
only a doctor can do. As doctors, it one weekday per month to review and form a formal call group. In
is our duty and responsibility to have salient, relevant articles. The four of this way, an OD is available to meet
quality-assurance oversight on the you will grow exponentially! Trying the needs of our collective opto-
final refraction; thus, looking at the to feed yourselves via continuing edu- metric patient population. If you
current eyeglasses prescription, the cation meetings provides a very low consider your fellow ODs only as
autorefraction, and the technician’s yield in professional growth, whereas competitors, that is a shallow, rather
performance of subjective refraction perusing optometric and ophthalmo- desperate view, and quite simply, is
accomplishes such. logical journals is a high-yield pitiable. We should all work together
Now, we are keenly professional growth as colleagues in an effort to enhance
aware of how exercise. patient care, and to keep optometric
patients as optometric patients! Your
practices will thrive, your patients
will be well served, and public health
REFRACTIONIST OR DOCTOR? will be enhanced. Remember, above
all, you are your brother’s keeper.
• A new world of vision testing and eye wear sales is dawning now
that refractions and prescription fulfillment are being offered online. OUR PRACTICAL ADVICE
• These developments may not be a negative for ophthalmology Now that we have comprehensively
practices and patients. laid the groundwork and have made
» Visibly » Myeyelab.com » Vmax Vision the case for expanded care by ODs,
we turn to sharing the knowledge
» EyeNetra » Smart Vision » Warby Parker
Labs
gleaned from the literature and
» MyVisionPod our combined 80 years of clinical
• Optometrists: Expand your scope of patient care services to protect practice. It is our hope that what we
your future! share herein enables you to fur-
• The AOA is aggressively fighting for optometry: Join the AOA! ther enhance your competence as a
patient-centric caregiver and medical
practitioner of the eye.
4 REVIEW OF OPTOMETRY JUNE 15, 2020
Optometry “On Call”: A Not-So-Novel Concept
It’s commonplace in other fields, yet somewhat rare in our profession. Patients who
need urgent care deserve the attention and expertise that ODs can provide.
A
s we all know, eye care ner—that is, form such a call group no matter the time of day or night.
provided by anyone with your colleagues to provide For perspective, the vast majority of
outside of optometry or emergency patient care. To allow these calls can be dealt with by phone;
ophthalmology is abysmal. your office phone to simply ring only rarely is there a need to meet the
Whether one practices in a group, and ring after hours is completely patient in the office in the middle of
private practice, a retail/commercial irresponsible; instructing your after- the night. Most emergencies can wait
setting or in any other setting, there hours answering service to direct the until office hours to be seen.
should be one uncompromising goal: caller to an emergency department or Let’s understand our role as a pa-
providing optometric patient access to urgent care center is even worse. tient caregiver, and develop a creative,
optometric care 24/7. We are a healthcare profession, collaborative system to meet our pa-
First, it is the rare individual who doctors, and our collective patients tients’ after-hours emergency medical
enjoys being “on call.” It is encum- deserve to be seen by an optometrist needs. We would want nothing less
bering, but the cases are usually when an ocular emergency arises, for ourselves!
stimulating and can stretch your clini-
cal confidence.
It is our collective perspective
that patients should have access to
emergency medical optometric care
whenever the need arises. When a pa-
tient calls her or his optometrist, there
should be an answering machine/ser-
vice guidance as to how to contact the
optometrist on call!
Here we share a parallel example
of how many dental practices meet
the needs of their patients: six to eight
dentists come together and form a call
group, such that a single dentist is on
call for the group every six to eight
weeks. By spreading the responsibil-
ity, they move from being “always on
call” (which, in reality, we all are), to
being on call only every six or eight
weeks. With this shared call system,
emergency patients always have ready
STRATEGIES FOR SUCCESS
access to a dentist. If we had a dental
emergency, called our dentists and the
answering machine said “Our office
is now closed,” or if we were directed
to contact an emergency department/
urgent care, the three of us would be
finding other dentists!
We urge our optometric colleagues
to become proactive in a like man-
Vision Source supports its members by (Practice Name)
(Practice Phone Number)
offering this promotional flyer on the
vital emergency care ODs provide.
REVIEW OF OPTOMETRY JUNE 15, 2020 5
SECTION I: STRATEGIES FOR SUCCESS
Ophthalmologic PATIENTS ARE READY FOR REMOTE EYE EXAMS—ARE YOU?
Perspective on A company called DigitalOptometrics is offering full-time and part-
Emergency Eye Care time positions to optometrists who are willing to perform remote
comprehensive eye
N
ow that more and more examinations during
eye surgeons have (or have the day, evenings and/
access to) outpatient surgery or weekends from their
centers, and use those rather than home office or other
hospital operating rooms, there is a location of choice.
shrinking need for such surgeons to DigitalOptomet-
serve on-call for hospital emergency rics, which operates in
departments. This leaves a vacuum the United States and
relative to emergency eye care. An Canada, uses live video-
article in EyeNet magazine (December conferencing technology
2019) shed light on the matter: to enable comprehensive
“If ophthalmologists continue eye health and vision analysis remote eye examinations performed
removing themselves from emergency by licensed optometrists. The goal, according to the company, is
medicine and remain unwilling to to make comprehensive eye exams convenient to patients in both
urban and remote locations by having exams performed remotely
provide care outside of their offices
by licensed optometrists.
[…] it is only creating a void that oth-
Our take: These technologies are in their infancy and will only
ers will be more than happy to fill.”
grow. Refraction-centric practices will be hurt. Medically-centric
“Optometrists and non-ophthalmic practices should be protected. Give this great contemplation.
providers are organized and ready to Fortunately, our colleagues at the AOA already have. The AOA
jump in. They see the gap in care. If kicked off a national public awareness campaign this year on the
a hospital can’t depend on ophthal- importance of an annual, in-person, comprehensive eye examination
mologists, why wouldn’t they send with an AOA family doctor of optometry—turning a moment (the
patients elsewhere? Why wouldn’t tie-in of year 2020 and 20/20 vision) into a movement.
optometrists become gatekeepers?”
Everywhere else in medicine, non- can say with authority that the need If both optometrists and ophthal-
surgeons are the gatekeepers, thus for an eye surgeon is exceedingly rare. mologists would proactively educate
it seems perfectly appropriate for As there is always the remote their collective patients to “call us
optometrists to fill this role. Having possibility for surgical need, an eye first” before going to an emergency
been on-call for our respective surgeon needs to always be department, several things could hap-
hospital emergency available, and this just pen:
departments, we makes sense. • Patient care would be greatly
enhanced.
• Patients would save significant
time and money.
THE EYE AND THE ED • Those caring practices would
enjoy enhanced revenue.
• Most common ICD diagnoses:
• Emergency department physi-
Conjunctivitis ..................33%
cians, who have a variably limited
Corneal injury...................13%
skill set for eye problems, would
Corneal foreign body ...... 8%
Hordeolum .........................4% become unencumbered from eye
• Mean ED charge: $989.30 for eye visit emergencies.
• Eye visits: 1.5% of all visits We all need to step up to the
—Vazini K, et al. Ophthalmology 2016;123(4):917-19
plate and reach out to this subset of
patients with urgent eye care needs.
• “Approximately 387,000 patients per year present to US emer-
We applaud those optometrists
gency departments with eye injuries, and children represent up
to one-third of those injured.”
already providing such emergency eye
services, and to our friends at Vision
—JAMA Ophthalmology, August 2018
Source for being formally proactive in
this regard.
6 REVIEW OF OPTOMETRY JUNE 15, 2020
Optometrists Can Rise to the Occasion
Build your practice around caring for your patients—especially those with emergency
medical needs—and you’ll be ready for anything, even a global pandemic.
T
his year, the world has been response. They don’t
overwhelmed by the corona- want to deal with eye
virus pandemic, which filled issues right now. A
hospitals with COVID-19 patients lot of these patients
and ground the everyday workings of are getting funneled
society to a halt. Like most doctors, into my clinic day and
the majority of optometrists closed night.”
their offices to routine care. Some He sees each
opened to emergency cases, but only patient one at a
if they had the clinical skills and com- time, so there is
munity reputation to make it work. never more than one
Practices that rely too heavily on patient in the clinic.
refractions and are mostly perceived To further ensure
as an outlet for glasses fared poorly. safety, Dr. Vollmer
One of our number—Patrick wears an N-95 mask
Vollmer, OD—made the transi- and gloves, and all
tion easily. Urgent care was nothing patients also receive
new to Dr. Vollmer, who provided masks and gloves
emergency eye care the first day he at the door. When
walked in the door of his practice, the patient leaves,
long before COVID-19 struck. everything is disin-
“I worked tirelessly in my com- fected. The procedure
munity to establish medical and is a bit tedious “but it
emergency eye care,” he says. “This works,” he says.
has proven to be a virtuous deci- Many of Dr.
sion. To my knowledge, pretty much Vollmer’s current
all of the hospitals, Urgent Cares emergency patients
and primary care offices are a bit tell him they would’ve Dr. Vollmer and his patient each wear masks and gloves to
minimize risk of contagion.
overwhelmed with the COVID-19 normally gone to the
ER or Urgent Care, but they were nice to be appreciated, but I get more
worried about being in a hospital set- fulfillment in knowing I helped some-
COMORBIDITIES AND
ting currently. “I take this opportuni- one in need.”
COVID-19 DEATHS
ty to educate these new patients that Continuing to see patients who
In a large study, the most they shouldn’t go the ER anyway. called in for urgent issues filled a
common comorbidities were A lot of patients simply don’t know critical patient care need and kept
STRATEGIES FOR SUCCESS
hypertension (57%), obesity this despite going to their eye doctors Dr. Vollmer’s practice busy during
(42%) and diabetes (34%)—all for years. Optometry cannot assume the downtime. “One of the important
conditions that in most cases can
patients know to come to their clinics aspects that I learned,” he explains,
be mitigated by lifestyle changes,
for ocular emergencies,” he says. “is how important it is to diversify
and/or medications. Something
Patients are appreciative of your practice. If it wasn’t for emer-
to ponder as we, as a society,
emergency care regardless, but they gency patients and ‘urgent’ needs, life
prepare for future pandemics.
are especially grateful during this would have been pretty slow.” Now
1. Richardson S, Hirsch JS, Narasimhan M, et outbreak, Dr. Vollmer says. “I don’t that the practice is seeing routine care
al. Presenting characteristics, comorbidities,
and outcomes among 5700 patients hospital- charge an after-hours fee right now, again, patients are more motivated
ized with COVID-19 in the New York City area.
JAMA 2020; April 22. [Epub ahead of print].
and the most I charge for any office than ever to come in because they
Published online April 22, 2019. visit is around $150 if they have no know this is a doctor they can count
insurance or a high deductible. It’s on even in the toughest times.
REVIEW OF OPTOMETRY JUNE 15, 2020 7
SECTION I: STRATEGIES FOR SUCCESS
Clinical Pearls You Can Count On
Heed these time-honored insights gleaned through 80+ years of patient visits.
E
very patient is unique, and • Unless the cause for foreign
deserves to be treated as such, body sensation is clearly evident (and
but these tips have proven sometimes even when it is), always
correct again and again in numer- evert the upper eyelid after instilling
ous encounters the three of us have fluorescein dye. There is always a
amassed throughout our careers. cause for foreign body sensation, so
• If there is any unexplained al- look for things like:
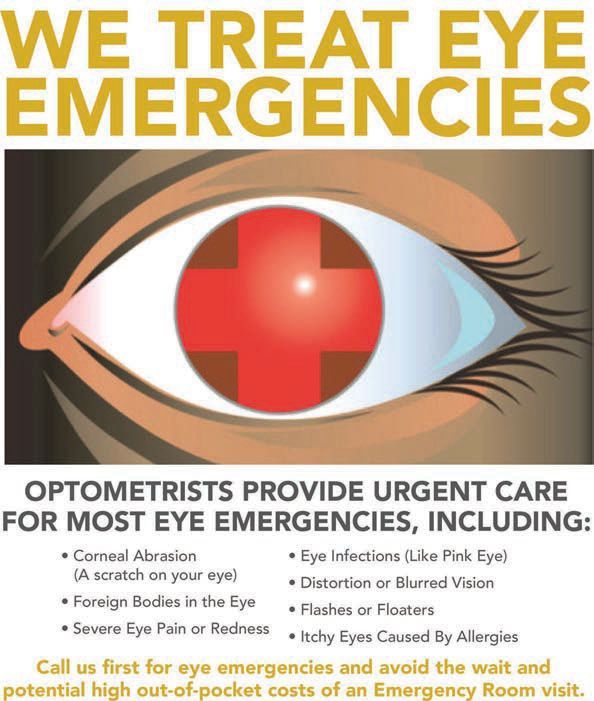
Eyes in primary gaze appear healthy.
teration of visual function, always do – subtle epithelial basement mem-
a retrospective review of any changes brane dystrophy
of the patient’s medicines, especially – Thygeson’s superficial punctate
if they are on any new medicines or keratopathy
changes to dosing have been made. – eroding tarsal conjunctival con-
By doing so, often a cause-and-effect cretions
relationship can be established that – occult trichiasis
provides a rational explanation for – a loose lash in the puncta
the change in visual status. For conjunctival foreign bodies, we Upon downgaze, the diagnosis of SLK is
obvious, thus emphasizing the necessity
• Studies have confirmed that try not to use an anesthetic, so once of lifting the eyelids to search for the
patients prefer their doctors to wear a the foreign body has been removed, cause of his presenting symptoms.
lab coat with their nametag on it. We the patient can give immediate con-
prefer our nametags to have our first firmation of relief, rather than having
and last names, then OD, rather than to wait 20 to 30 minutes while the
“Dr. Last Name.” We are proud to anesthetic wears off before making
be ODs, and on occasion, it provides such a determination.
an opportunity to explain to our • If the eye is pretty much white
patients exactly what an OD is. To yet the patient has miserable, irritated
display our degree allows us to share eyes with foreign body sensation, These eroding calcific bodies caused this
our unique expertise in eye care, and always think about superior limbic patient’s foreign body sensation.
to confirm to our patients that they keratoconjunctivitis (SLK). Confirm-
are, indeed, seeing the right ing this diagnosis takes two that you can examine the superior
doctor. Be proud to be steps: have the patient bulbar conjunctiva, and then stain the
an OD! look down so globe with lissamine green dye. Allow
30 to 60 seconds for adequate stain-
ing. If these bulbar and tarsal conjunc-
tival tissues have become idiopathical-
SUPERIOR LIMBIC KERATOCONJUNCTIVITIS ly keratinized, the mechanical rubbing
of these two interfacing tissues is the
• Both sexes affected, women more cause for the distressing symptoms.
• Main symptoms: distressingly irritated eyes We initially use 0.5% silver nitrate
compounded solution to help diminish
• Dry eyes common companion finding these keratinized tissues. After the
• Symptoms disproportionate to clinical findings patient takes your prescription to a
known ophthalmic compounding
• Spontaneous exacerbations and remissions
pharmacy and obtains the solution,
• 25% to 40% have some thyroid dysfunction have him or her bring the drop back
• Tx (difficult): 0.5% silver nitrate, optimum lubrication, pressure to the office where topical propara-
patching, therapeutic soft lenses, surgical resection, cryotherapy caine is instilled twice (about 30
seconds between each drop). We then
dip a sterile cotton swab into the com-
pounded solution, flick off the excess,
8 REVIEW OF OPTOMETRY JUNE 15, 2020
and have the patient look down, evert
the upper eyelid(s) and “paint” the
superior tarsal tissues. EYELID CLEANSING TREATMENTS FOR BLEPHARITIS
This is just like painting a wall
with a paint roller; do this for about • Study compared “dedicated eyelid cleanser to diluted baby
20 seconds. Then un-evert the eyelid shampoo”
and have the patient look down. Now
• Cleaning was done BID for four weeks
perform the same procedure to the
affected superior bulbar conjunctival • Conclusion: improvements occurred with both treatments
tissues.
• “However, only the dedicated eyelid cleanser proved
We then instill a moderate amount
effective in reducing inflammation and was the preferred
of generic Maxitrol (neo-poly-dex)
ophthalmic ointment, which we keep therapy.”
in our lab coat pockets. We encour- —The Ocular Surface, October 2017
age these patients to frequently instill
lipid-based artificial tears to the eye(s)
over the course of the day and to use
a preservative-free artificial tear oint-
ment at bedtime until they return to us agnosed condition. Being thorough dystrophy. Instillation of fluorescein
in one month, at which time we repeat in your diagnostic pursuit will easily dye can help uncover these two subtle
the “painting” procedure. We keep reveal the cause for the patient’s visit. presentations. There is always an
the patient’s silver nitrate solution in While rare, SLK is yet another oppor- explanation for monocular diplopia;
our refrigerator, clearly marked with tunity to care for our patients. our duty is to find the correct cause
the patient’s name, date of birth and • Baby shampoo for treatment of and treat it appropriately.
medical record # until that time. blepharitis has gone the way of the • Ethambutol is commonly used to
While this process is highly benefi- horse and buggy. There are numerous treat tuberculosis, but it can lead to
cial, there may be occasional recalci- commercially prepared “eyelid cleans- toxic optic neuropathy. Color vision
trant-to-treatment patients. If, after ers” readily available over-the-coun- is commonly compromised in this
this two-step therapeutic intervention, ter, and we exclusively recommend situation, so, if possible, be sure to
the patient is still not below symptom- these when eyelid scrubs are indicated perform a color vision test to establish
atic threshold, a consult with a cornea in the care of patients with symptom- a baseline prior to starting therapy
and external disease surgical subspe- atic blepharitis. for tuberculosis. The general toxic
cialist for a conjunctival resection of • Monocular “diplopia” can threshold is 30mg/kg per day, so the
these afflicted tissues is in order. result from a couple of subtle corneal greater the dose, the higher the risk of
Superior limbic keratoconjunctivitis conditions: unilateral Thygeson’s SPK neuronal toxicity. Beyond color vision
is a commonly missed and/or misdi- and epithelial basement membrane testing, certainly establish best visual
acuity and baseline 10-2, as well.
MIND YOUR MEDICINES Depending upon dosage, follow these
patients quarterly and repeat testing as
An OD recently encountered a woman in her late 20s whose chief deemed necessary.1
complaint was near blur. She did not have • A recent review in a cardiology
hyperopia nor did she have latent hyper- journal notes that diagnoses of COPD
STRATEGIES FOR SUCCESS
opia on cycloplegic refraction. Her exam
were incorrect in about 62% of cases.
was normal except for “presbyopia.”
The authors caution, “Physicians
With a +2.50, she saw a crisp 20/20.
need to do a better job of identifying
Reviewing her medical record, it was
seen that she was taking Qbrexa for
patients with COPD and not over-
her axillary sweating which has a diagnosing it. Performing spirometry
significant anticholinergic effect, before and after administration of
thus causing her symptom. This a bronchodilator is essential before
perfectly illustrates the impor- making a diagnosis.”2
tance of being attentive to any new Our take: This seems to be
medicines when encountering an unusual somewhat parallel to the challenges
patient complaint. that eye doctors face with regard to
glaucoma. Obviously, it is essential to
REVIEW OF OPTOMETRY JUNE 15, 2020 9
SECTION I: STRATEGIES FOR SUCCESS
perform an appropriate and compre- coming down the road. Anticipate the
hensive workup prior to initiating emergence of these innovative drugs THE BENEFITS OF
therapy. and how they might impact your DRINKING WATER
• An internal medicine journal practices.4 “Clinicians should use simple,
notes “soft drink consumption has • Looking into resolution of clear messaging on the role
been associated, not only with weight congenital nasolacrimal duct obstruc- of water as the primary drink
gain and obesity, but also with excess tion, JAMA Ophthalmology recently for all children, adolescents,
mortality in US studies. Associations stated, “The rate of spontaneous reso- and young adults when
were found for both sugar-sweetened lution plateaued after nine months, discussing healthy habits
and artificially sweetened drinks.”3 and initial probing success declined with families.”
Our take: Play outside and be after 15 months.”5 Rosinger AY, Bethancourt H, Francis
active. For the most part, try to eat a Of course, different articles seem to LA. Association of caloric intake from
sugar-sweetened beverages with water
plant-based diet; wear your seat belts; consistently find different outcomes. intake among us children and young
don’t drink alcohol (or soft drinks) This is always so frustrating. A study adults in the 2011-2016 National Health
excessively; sleep adequately; certainly from the December 2019 British and Nutrition Examination Survey. JAMA
Pediatric. 2019;173(6):602-04.
do not smoke; and if you wear contact Journal of Ophthalmology found that
lenses, do not sleep in them! “spontaneous resolution occurred in
• Presbyopia-“correcting” eye 45% of patients at a mean of 17.8 ignorance of the professional litera-
drops are coming. The bifocal market months of age.” ture seems to fail to deter sales-centric
is about to take a hit! This first Our take: We would recommend opticals. Because blue light can
sentence is to get your attention; the appropriate lacrimal sac massage for modify our circadian rhythms, all of
following discussion is to explain the several weeks, but if treatment is not these articles advise us not to work
pharmacologic mechanisms to reduce successful, we would recommend a pe- at a screen two to three hours before
the demand for bifocal lenses. diatric ophthalmological consultation bedtime, however.
There are two primary approaches: at about nine to 10 months of age. • In a similar vein, the alleged ben-
(1) miotic induction to create a pin- While we still hold to this recommen- efit of wearing yellow-tinted glasses
hole effect in a non-dominant eye, and dation, if the parent(s) prefer to con- to enhance contrast has been found
(2) restoration of crystalline lens in- tinue to try massage up to 15 months to be a myth.6 Now, we all have
trinsic elasticity. The former approach of age, that may well be reasonable. patients who swear by these, and we
may come to market first; however, • Blue light protection glasses. see no practical reason to rain on their
we are excited for the latter approach. There have been a number of articles parades. However, it is important that
It’s a year or two too early to get published regarding blue light protec- we are all aware of this research—
into the details, but we feel an obliga- tion of late. There is no consensus that’s why we read the journals!
tion to put our colleagues that such “protection” serves • Topical antibiotics play a very
on notice that mega- any humanitarian limited role in contemporary eye care,
changes are purpose, yet as their only indication is for the treat-
ment of bacterial infection, which is
relatively uncommon as compared to
inflammatory eye conditions.7 There
YELLOW-TINTED GLASSES AND NIGHT DRIVING are three prime uses for antibiotics:
− children with bacterial conjunc-
• “Wearing yellow-lens glasses tivitis
did not improve (i.e., more likely − prophylaxis when using a ban-
worsened) performance either dage contact lens
with or without headlight glare.”
− bacterial corneal ulcers
When we encounter adults with
• “These findings do not appear acute bacterial infections, we treat
to support having eye-care with a combination antibiotic-steroid
professionals advise patients to such that we address the infection and
use yellow-lens night-driving
the secondary inflammation simulta-
glasses.”
neously. For more advanced bacte-
—JAMA Ophthalmol., August 2019 rial infections, we most commonly
prescribe generic moxifloxacin or
Besivance. Note that Besivance is an
10 REVIEW OF OPTOMETRY JUNE 15, 2020ophthalmic suspension and needs to
be shaken before each instillation. For
this reason, when used for prophy- HOW IMPORTANT IS IT TO BE “PRESERVATIVE-FREE”?
laxis in the setting of a bandage soft
contact lens, we would choose generic • “Published studies have not demonstrated any clear benefits of
moxifloxacin, since it is a solution. the BAK-Free formulations.”
For corneal ulcers, we would use be- • “There is a lack of evidence of clinically significant harm from
sifloxacin because of it superiority as a small number of BAK preserved drops in patients without
demonstrated in the ARMOR study OSD. This means that generally more expensive PF glaucoma
(see p. 29 for the 2020 ARMOR medications should only be recommended for those on poly
data). pharmacy or those with OSD but are not necessarily required for
• Some patients with migraine all patients.”
headaches, blepharospasm and post- —Br J Ophthalmol, July 2018
concussion suffer from quality-of-life
–altering photophobia. An FL-41 (FL
stands for fluorescent) spectacle lens
coating can filter out certain wave-
lengths of blue/green light that have
been shown to contribute to light study, neomycin allergy developed man medical care, these sites will im-
sensitivity.8 Of course, it is important in only 1.5% of subjects. When such prove over time, and while they may
to rule out ocular surface disease, so does occur, it is only a mild annoy- be helpful adjunctively to clinic-based
conduct a trial of topical corticoste- ance or aggravation. Discontinuation care, nothing will replace the care and
roids QID for two weeks to address of the offending drop, optional use of attention of a face-to-face doctor visit.
any inflammatory component before cool compresses and/or triamcinolone • Thankfully, newer, better and
suggesting FL-41 coating. Address- 0.1% cream can be used for two to easier to use antithrombotic medi-
ing severe photophobia may require three days. cines are dampening the prevalence
multiple approaches, but do be aware An article in the British literature of Coumadin (warfarin). However,
of such options. provides a more practical perspective there is still an abundance of people
• Steroids are simple: we prescribe on BAK (see slide above). on warfarin for stroke prevention. A
Durezol (Novartis) for advanced cases Further, it is well known that the blood assay known as the Internation-
of anterior uveitis and episcleritis; for original 0.3% Lumigan (Allergan) al Normalized Ratio (INR) quantifies
everything else, we prescribe Lotemax caused a fair amount of conjunctival thrombotic control. It is yet another
SM (Bausch + Lomb). As emulsions, and eyelid irritation. It was refor- blood test beyond CBC, sed rate and
neither require shaking prior to instil- mulated to a much more tolerable C-reactive protein (CRP) with which
lation. There are times when regula- 0.1%. However, there is four times we all need to be familiar. In our tire-
tory formularies limit us to generic more BAK in the 0.1% formulation. less pursuit of simplicity, just know
prednisolone acetate, which must be Deductive reasoning will now soften INR generally needs to be between
shaken well before each use. the accusations against this maligned 2 and 3 for warfarin patients. This
• Regarding eyedrops, we our- preservative. metric is not applicable to any other
selves personally demonstrate to our • What about online “symptom- drug. Essentially, if the INR is 3, the risk of hemorrhagic events is
STRATEGIES FOR SUCCESS
ceiling while pulling down the lower interesting article in the June 2019 increased.
eyelid, and having the bottle tip about JAMA Ophthalmology found that • There are three commonly used
a half-inch away from the eye. This the WebMD site listed the correct antibiotic-steroid combinations. From
is especially important for our new diagnosis as the first diagnosis in 26% oldest to newest, these are: Maxitrol
glaucoma patients. Most people have of cases. The correct diagnosis was (neomycin, polymyxin-B and dexa-
an incomplete understanding of the not on the list at all in 43% of cases. methasone, Novartis), which comes in
proper technique, and giving them a Their euphemistic conclusion: “There both suspension and ointment forms;
live demonstration greatly enhances is room for improvement in the TobraDex suspension and ointment
the efficacy of therapy. domain of online symptom-checkers (tobramycin with dexamethasone,
• While neomycin and benzalko- for ophthalmic symptoms.” Bottom Eyevance); and Zylet (tobramycin and
nium chloride (BAK) suffer much line—just see an optometrist! loteprednol, Bausch + Lomb), which
abuse, neither merit it. In a large Like all technologies affecting hu- is only available as a suspension.
REVIEW OF OPTOMETRY JUNE 15, 2020 11SECTION I: STRATEGIES FOR SUCCESS
− From least to most expensive, not fully control the allergic response, wear time are significant maneuvers in
these are: generic Maxitrol (about then “an intranasal antihistamine such the ultimate resolution of symptoms.
$25), Zylet (with a coupon it is about as azelastine can be added, albeit at the According to Mathea Allansmith,
$35) and generic TobraDex (about expense of dysgeusia.”9 MD, a renowned ocular allergist at
$60-80). These prices may vary • Giant papillary conjunctivitis Harvard, and our esteemed colleague
depending upon insurance plans and continues to be a menace. It could be Jimmy Bartlett, OD (professor emeritus
geographic location of the patient. relegated to history if everyone could/ at UAB), loteprednol is the steroid of
− From safest to least safe (all are would wear daily disposable contact choice in treating this condition.
relatively safe): Zylet, Maxitrol and lenses. For symptomatic patients, such • An FDA program called “Rx to
TobraDex. All three suspensions as in the image below, we have them OTC” recently brought both 0.1%
need to be shaken before instillation. cease contact lens wear for at least a olopatadine (Patanol, Alcon) and
Regarding antibiosis, these medicines week, and preferably for two weeks. 0.2% olopatadine (Pataday, Alcon)
are all clinically effective. There is OTC. These drops can no longer be
no debate that Zylet is the “pick of prescribed. This will bring two more
the litter” here, especially for chronic products onto the already-crowded
conditions such as staphylococcal OTC shelves. Since all these histamine
blepharitis, because of the ester-based type 1 receptor blockers perform simi-
steroid. When cost is truly imperative, larly, the advice we give our patients is
generic Maxitrol is the best choice, to select a 10mL bottle when it costs
but only for acute conditions that about the same as a 5mL competitor.
generally need treatment for no more Use any of these drops BID for a week,
GPC remains common among the contact
than seven to 10 days, because of the lens population but is easily managed. then try to drop back to once daily use
dexamethasone. as needed to control ocular itching.
These combination drugs are real (Every contact lens wearer with a func- Different insurance plan formularies
workhorses in routine clinical care. tionally significant prescription needs a may mean that, cost-wise, you provide
Do bear in mind, however, that unless backup pair of eyeglasses!) a better service to your patient by
there is a breach in the integrity of We prescribe Lotemax SM for these prescribing a brand name–protected
the corneal epithelium, an antibiotic patients QID for one to two weeks, Rx anti-allergy drop, such as Bepreve
is generally not needed, and only a then BID for two more weeks. During (bepotastine, Bausch + Lomb), rather
straight steroid should be employed. the last two weeks, we instruct the than asking them to purchase an OTC
• Intranasal steroids are the treat- patient to instill a drop 10 minutes product. By being attentive to this
ment of choice for allergic rhinitis in prior to lens application and a second cost-saving maneuver, you can wisely
patients over age 12; adding an oral drop at the end of the work or school and compassionately keep down out-
antihistamine confers no ben- day when lenses are removed. of-pocket expenses for your patients!
efit. If the intranasal ste- Getting new lenses • A young man presented to
roid alone does and decreasing us with his third episode of some
sort of dermatitis to the eyelid and
periocular tissues in six months. He
had seen his internist twice before,
TREATMENT OF OCULAR ALLERGIES about three months apart, and was
treated successfully (albeit temporarily)
with oral prednisone. This time, the
patient wanted to try an eye doctor.
It appeared to be a 4+ case of contact
dermatitis so severe that he was getting
secondary ectropion from the epider-
mal inflammation.
He was treated with 40mg of
prednisone (it was not known what his
prior dosage had been) for five days,
along with 0.1% triamcinolone cream
applied to the affected tissues QID for
five days. The cynical saying “no good
deed goes unpunished” applies here,
12 REVIEW OF OPTOMETRY JUNE 15, 2020in that the patient never returned for
follow-up, and his phone mailbox was
full or his phone simply rang and rang. BILATERAL PERIORBITAL IMPETIGO — DERMATITIS
Finally, after about four months,
we were able to see him. He shared • Impetigo is a Staph. aureus infection, often seen in patients with
with us that his condition had quickly eczema
resolved and had not recurred during • Usually seen in children and young adults
this four-month period. That’s great,
• Can cause a secondary inflammatory dermatitis
but we still only had a presumptive di-
agnosis of contact dermatitis. This was • Can create cicatricial ectropion
in May 2018. Fortuitously, in the June
• Tx with oral antibiotic and topical antibiotic/steroid or steroid
2018 issue of Ophthalmology, there ointment
was an article that grabbed our atten-
tion. Looking at the pictures, it clearly —Ophthalmol, June 2018
reminded us of this patient. Well, it
turns out that the diagnosis was more
than contact dermatitis—it was impe-
tigo! Because we consistently read the
literature, we were able to grow our and seasonal allergic conjunctivitis.” • Festoons. These are fluid-filled,
clinical knowledge. Should this patient However, their use in prevention “squishy” pockets gravitationally
ever return with similar symptoms, we of postoperative cystoid macular exacerbated by age-related laxity of
now know to how to address his issue edema is central in their prescribing the upper facial muscles. They can also
more definitively and competently. In frequency. accompany inflammatory dermatolog-
addition to the steroid, we will also – “Alarmingly, topical NSAIDs ic diseases; most relevant to us, herpes
prescribe an oral antibiotic such as may be used by eyecare practitioners zoster ophthalmicus. These non-tender
cephalexin 500mg BID or Augmentin for extended periods of time without festoons look bad but carry no patho-
875mg BID, depending upon our clini- a clear diagnosis or indication.” logical relevance. The treatment is pa-
cal judgment; it’s an art. – “Corneal complications of topical tient reassurance, or if he/she desires, a
NSAIDs include superficial punctate referral for facial plastic surgery.
keratopathy (punctate epithelial • Medicines that can cause dysgeu-
erosions), corneal infiltrates, and epi- sia: prednisolone acetate, lifitegrast,
thelial defects; the most severe of all is topical carbonic anhydrase inhibitors
corneal melt.” and azelastine.
– “An intriguing aspect of such
1. Stuart A. Drug Toxicity to the Retina and Optic Nerve: Are You
melt is the apparent requirement for a Missing It? EyeNet Magazine. September 2019. Available at: https://
compromised cornea for it to occur.” www.aao.org/eyenet/article/drug-toxicity-to-the-retina-and-optic-
nerve?september-2019 (last accessed April 14, 2020).
It appears that compromised epithelial 2. Sator L, Horner A, Studnicka M, et al. Overdiagnosis of COPD in
subjects with unobstructed spirometry: a BOLD analysis. Chest. 2019
Note the secondary ectropion to this cells respond differently to NSAIDs Aug;156(2):277-88.
patient with impetigo. than healthy ones. 3. Mullee A, Romaguera D, Pearson-Stuttard J, et al. Association be-
tween soft drink consumption and mortality in 10 European countries.
– “Some ocular surface diseases JAMA Intern Med. 2019;179(11):1479-90.
4. Thompson V. Examining presbyopia treatments. Eye World.
• What’s the risk for corneal melt such as dry eye are considered rela- December 2019. Availablee at: https://www.eyeworld.org/examining-
with the use of topical nonsteroidal tive—and for most experts—absolute presbyopia-treatments (last accessed April 14, 2020).
STRATEGIES FOR SUCCESS
5. Sathiamoorthi S, Frank RD, Mohney BG. Spontaneous resolution
anti-inflammatory drugs (NSAIDs)? contraindications to the use of ocular and timing of intervention in congenital nasolacrimal duct obstruction.
Anti-inflammatory drops are routinely NSAIDs.” JAMA Ophthalmol. 2018; Nov 1;136(11):1281-6.
6. Hwang AD, Tuccar-Burak M, Peli E. Comparison of pedestrian
used postoperatively, and only rarely detection with and without yellow-lens glasses during simulated night
driving with and without headlight glare. JAMA Ophthalmol. 2019;
do they cause problems. An important Aug 1.
recent article in Survey of Ophthal- 7. Keen M, Thompson M. Treatment of acute conjunctivitis in the
united states and evidence of antibiotic overuse: isolated issue or a
mology offers these insights:10 systematic problem? 2017; Aug; 124(8):1096-8.
8. Migraines & FL-41 Tinted Lenses. University of Utah Health/Moran
– “The FDA has approved oph- Eye Center. Available at: https://healthcare.utah.edu/moran/optom-
thalmic NSAIDs for use in four areas: etry/fl41-lenses.php (last accessed April 14, 2020).
9. Wallace DV, Dykewicz, Oppenheimer J, et al. pharmacologic treat-
pain and inflammation associated ment of seasonal allergic rhinitis: synopsis of guidance from the 2017
Joint Task Force on Practice Parameters. Annals of Internal Medicine.
with cataract surgery, pain associ- 2017; Dec. 19.
ated with corneal refractive surgery, Patients may be anxious about festoons
10. Rigas B, Huang W, Honkanen R. NSAID-induced corneal melt:
Clinical importance, pathogenesis, and risk mitigation. Surv Ophthal-
inhibition of intraoperative miosis, but they are harmless. mol. 2020 Jan-Feb;65(1):1-11.
REVIEW OF OPTOMETRY JUNE 15, 2020 13SECTION I: STRATEGIES FOR SUCCESS
Perspective on Pupillary Dilation
Patients may not like this experience but that’s no excuse for avoiding a vital step
that can make or break a diagnosis.
N
o one enjoys being dilated;
no woman enjoys having a
Papanicolaou (Pap) smear;
no man enjoys a prostate examina-
tion; however, all three examina-
tion procedures are important and
represent excellent healthcare. Face
it—in life, many vitally important
functions, procedures and activities
are just not fun.
Certainly, there are technologies
to image the retina without phar-
macologic dilation, and in some This case of synechial anterior uveitis finally yielded to atropine, Durezol and 10%
cases, these can be useful. However, phenylephrine. The residual lens face “tattooing” of iris pigments will largely
community standards of care and dissipate over the years.
prestigious medical centers fully
embrace the dilated eye examina- countless other conditions to dilate most of our patients is
tion. In most cases, a dilated exam is We explain to our patients that the instillation of Paremyd (0.25%
essential to: if they were being seen at any tropicamide with 1% hydroxyam-
– diagnose pseudoexfoliation prestigious medical center, their phetamine hydrobromide, Akorn).
– meticulously examine for dia- eyes would be dilated; thus, why This combination drug provides
betic retinopathy and maculopathies should we provide our patients with rapid, short-lived dilation with a
– search for subtle retinal tears anything less than the very best of considerably truncated cycloplegic
(for example, associated with symp- care? We rarely have patients ada- effect.
tomatic posterior vitreous detach- mantly decline dilation, and when For older, diabetic patients
ments) we do, we document in our medical (who typically are more difficult to
– identify pars planitis or ciliary record that the patient refused AMA achieve dilation), we revert back
body tumors (against medical advice). to the traditional use of 1% tropi-
– assist with visu- One maneuver we camide and 2.5% phenylephrine.
alization of typically use Post-mydriatic sunglasses are always
provided. As healthcare profes-
sionals, we have an obligation to
provide our patients the highest
PAREMYD OPHTHALMIC SOLUTION levels of care, and pharmacological
dilation represents the gold standard
• A combination of tropicamide 0.25% and 1% in this regard.
hydroxyamphetamine HBr, an indirect acting Given that “failure to diagnose”
sympathomimetic (adrenergic agonist). is by far the most common reason
• An excellent, less intrusive dilating drug we use optometrists are successfully sued,
for routine dilation. we have yet another good reason
(beyond our desire to provide
• For patients who are of African origin and/or
excellent patient care) to embrace
patients with diabetes, we commonly use 1%
the inconvenient virtue of pupillary
tropicamide with 2.5% phenylephrine.
dilation.
• Marketed by Akorn in a 15ml bottle During one of Dr. Thomas’s
externships, the brilliant ophthal-
mologist’s routine dilation protocol
was use of 1% tropicamide and
14 REVIEW OF OPTOMETRY JUNE 15, 202010% phenylephrine. There was
no adverse event with any of these
hundreds upon hundreds of mostly SAFETY OF PHENYLEPHRINE
elderly patients.
We share this to provide a “Phenylephrine 2.5% leads to no clinically
perspective on the safety of both meaningful change in blood pressure or heart
phenylephrine concentrations. Since rate and can be considered safe to use in clinical
the 2.5% formulation (in combina- routine. The changes in BP and HR seen with
tion with 0.5% or 1% tropicamide) phenylephrine, 10%, are short lived and of
provides ample dilation, we rarely uncertain clinical relevance.”
have a practical need to use the Stavert B, McGuinness MB, Harper CA, Guymer RH, Finger RP.
10% concentration. However, we Cardiovascular Adverse Effects of Phenylephrine Eyedrops:
A Systematic Review and Meta-analysis. JAMA Ophthalmol.
do find the 10% concentration can 2015;133(6):647–652. doi:10.1001/jamaophthalmol.2015.0325
be adjunctively helpful in breaking
some recalcitrant synechiae, and for
subsequent visits of patients known
to dilate poorly.
GUEST COMMENTARY, by Richard Edlow, OD
The Not-So-Secret Strategy to Turbocharging Practice Growth
We were certainly right in thinking the year 2020 would be special for all of us—just not the way we anticipated.
T he world and the way we inter-
act is changing, perhaps forever.
Optometry’s practice patterns must
age 64 and under is only 1.9%, while
the 65-and-older increase is 30.5%.
The demand for medical eye care
will produce approximately 460 new
entrants each year, and 420 practitio-
ners will be exiting, for a net increase
also change, but not in the ways one services will grow 20 times more rap- of 400 ophthalmologists over the
might be thinking. idly than the demand for vision exams. entire decade—just 40 each year for
I will share a number of data points The latter are defined as ICD-10 refrac- the entire country. To just provide
that should be a wake-up call for all tive diagnosis codes, while medical for the increase in cataract surgical
optometrists, regardless of practice eye care exams are those that have a procedures, we would require 3,500
environment, to fully embrace provid- medical diagnosis. Eye care providers surgeons.
ing medical eye care services. The data (ECPs) will need to collectively deliver Ophthalmologists will find them-
is a compilation from sources includ- two million additional vision exams per selves more and more in the operating
ing CMS/Medicare, Census Bureau, year, 10.8 million additional diagnostic
room, less and less in the office setting.
tests per year, 16 million additional
National Eye Institute, optometric and The message is clear: Optometry
medical eye exams per year and 1.4
ophthalmology training programs and must rapidly embrace providing
million additional cataract surgeries
insurance utilization statistics. medical eye care services in their prac-
per year—all above and beyond what
The following projection (net tices. If one uses Medicare Provider
we are providing today in 2020. For
changes from 2020 to 2030) reveals a Utilization & Payment data as a proxy
perspective, current levels are 111.4 mil-
unique opportunity for the growth of lion vision exams, 64 million diagnostic for how engaged optometry is in pro-
STRATEGIES FOR SUCCESS
optometric practice over the next 10 tests, 60.4 million medical eye exams viding medical eye care, it is at a very
to 20 years. An aging population, the and 4.2 million cataract surgeries. low level—less than 28% of optom-
prevalence of age-related eye condi- etrists provide any level of care.
tions and a relative shrinking supply SUPPLY OF ECPs It is incumbent upon the entire
of ophthalmologists presents a once- The supply of optometrists will eye care industry to rapidly increase
in-a-lifetime open window to embrace increase at a pace somewhat greater optometry’s involvement in medical
medical eye care. than overall population growth but services and turbocharge practices,
much slower than the 65 and older regardless of practice setting. n
GROWING DEMAND & MARKET SIZE demographic.
The US population is expected to grow The game-changer is that the sup- Dr. Edlow, AKA “The Eyeconomist,”
6.7% this decade. Of greater signifi- ply of ophthalmologists is almost flat. practices in Catonsville, MD, and is
cance: projected growth among those Ophthalmology residency programs known for strategic trend analysis.
REVIEW OF OPTOMETRY JUNE 15, 2020 15You can also read