Original Article Analysis of risk factor for pediatric intensive care unit delirium in children: a case-control study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Am J Transl Res 2021;13(8):9143-9151
www.ajtr.org /ISSN:1943-8141/AJTR0129097
Original Article
Analysis of risk factor for pediatric intensive care unit
delirium in children: a case-control study
Xiao-Hua Ge1,2*, Wan-Rui Wei3*, Tie-Nan Feng4, Li-Li Xu5, Ya-Qin Hu5, Chang-Rong Yuan1,6
1
School of Nursing, Naval Medical University, Shanghai, China; 2Department of Nursing, Xinhua Hospital Affiliated
to Shanghai Jiao Tong University School of Medicine, Shanghai, China; 3School of Nursing, Shanghai Jiao Tong
University, Shanghai, China; 4Clinical Research Institute, Shanghai Jiao Tong University School of Medicine,
Shanghai, China; 5Pediatric Intensive Care Unit, Xinhua Hospital Affiliated to Shanghai Jiao Tong University School
of Medicine, Shanghai, China; 6School of Nursing, Fudan University, Shanghai, China. *Equal contributors.
Received December 27, 2020; Accepted May 14, 2021; Epub August 15, 2021; Published August 30, 2021
Abstract: Objective: This study aimed to survey the prevalence of delirium in the pediatric intensive care unit (PICU)
and explore the associated risk factors. Design: A retrospective case-control study. Setting: Two PICUs within a
tertiary-A general hospital. Patients: Patients aged from 1 month to 7 years who stayed in either PICU for at least 1
day were included. Methods: A total of 639 patients admitted to PICU of a tertiary-A general hospital from December
2018 to August 2019 were enrolled. Demographic, clinical, laboratory data and length of stay in the PICU were col-
lected. The patients were screened twice a day with the Chinese version of Cornell Assessment of Pediatric Delirium
(CAPD), and were divided into the delirium group and the non-delirium group. A risk factor analysis was conducted,
with ICU pediatric delirium as primary outcome, by performing a multivariable logistic regression analysis. Results:
Of the 639 patients, the prevalence of ICU pediatric delirium was 31.30%. Of the 200 children with delirium across
3703 study days, 36% children were hyperactive, 41% were hypoactive, and 23% displayed the mixed type of de-
lirium. Univariate analysis and multivariate logistic regression analysis showed that age, PRISM IV score (OR, 2.20;
95% CI, 1.42-3.41), hypoxia (OR, 2.69; 95% CI, 1.53-4.71), metabolic dis-function (OR, 3.73; 95% CI, 2.08-6.71),
duration of infection (OR, 1.22; 95% CI, 1.10-1.36), and mechanical ventilation (OR, 3.78; 95% CI, 2.25-6.35) were
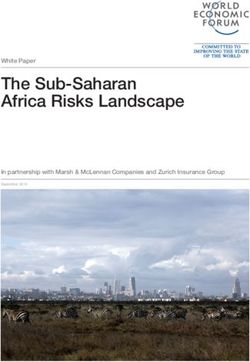
statistically correlated with ICU pediatric delirium. The ROC curve analysis shows the combination CRP with dura-
tion of infection has good predictive performance. Conclusions: Age, PRISM IV score, ICU retention time, metabolic
dis-function, duration of infection, hypoxia, CRP and mechanical ventilation were the independent risk factors for
ICU pediatric delirium. We suggest that active preventive measures should be taken to reduce the occurrence of
ICU pediatric delirium.
Keywords: Pediatric, children, critical care, delirium, risk factor
Introduction ians of children suffering from delirium in PICU
often have to afford higher healthcare costs [5].
Delirium refers to an acute fluctuating change A longer duration with ICU pediatric delirium is
in the state of consciousness, which is defined reported to be linked to worse outcomes [6].
by impairment of cognition, attention, and
behavior [1]. The specific features of pediatric Reported prevalence rates of pediatric delirium
delirium include delayed responses, sustained in critically ill children ranged from 12% to 47%
agitation, abnormal and implacable crying [7-15], and in a recent study were even up to
along with many other types of changes in psy- 56% in children below 2 years of age [8].
chomotor activity. In ICU settings, pediatric Children at a young age (< 2 years), disease
delirium was linked with increased hospital severity, infectious diseases, inflammation,
mortality, prolonged mechanical ventilation mechanical ventilation, and antiepileptic drugs
and length of hospital stay. Pediatric patients were identified as important risk factors for ICU
may be at risk of exposure to both short-term pediatric delirium [10, 16, 17]. It is vital to care-
and long-term hazards [2-4]. Meanwhile, guard- fully identify the specific independent risk fac-Analysis of risk factor for ICU pediatric delirium
tors linked to pediatric delirium as later this Richmond agitation sedation scale (RASS) < -3;
information can help to develop significant and 2) Patients had delirium before admission; 3)
effective preventive strategies in patients. Patients had previously undergone neurosur-
gery or neurological surgery; 4) Patients had
According to Maldonado [18, 19], the develop- been diagnosed with mental illness or develop-
ment of delirium in patients is thought to be mental delay and continued to be administered
based on at least six pathophysiology and antipsychotic drugs; 5) Patients presented with
seven neuro-pathogenesis theories. Based on hearing or visual impairment; 6) Patients had
the neuroinflammation hypothesis represented missed or incomplete delirium score; 7)
by Cerejeira [20], infection may introduce spe- Patients were non-Chinese or non-English lan-
cific triggering factors that may then provoke guage users.
the inflammatory cascade activation, which
would include hypoxia, blood transfusions, ele- Data collection
vated hormone levels, and so on. These neuro-
inflammatory changes lead to the destruction The PICU responsible nurses explained this
of the permeability of the blood-brain barrier, research to the children’s legal guardians and
and then result in neurobehavioral and cogni- gave detailed instructions on what it would
tive symptoms of delirium [21]. Systemic inflam- involve. Participants would be included after
mation, which may be caused by injury (includ- their legal guardians signed an informed con-
ing surgical injury) or infection, has been widely sent form containing detailed information
known as a triggering cause of delirium [19]. about the research. The study was registered in
However, few studies have examined C-reactive the Chinese Clinical Trial Registry (Registration
protein (CRP), one of the most common mark- number: ChiCTR1800019825 http://www.chic-
ers for systemic inflammation, as a risk factor tr.org.cn/showproj.aspx?proj= 33238).
for pediatric delirium. The aim of this research
was to survey the prevalence of delirium in Each patient, 1 month-7 years of age, was
PICU and explore the associated risk factors. screened for delirium twice daily by the
researchers using the Cornell Assessment of
Material and methods Pediatric Delirium (CAPD). The CAPD score > 9
and RASS > -3 were considered as ICU pediat-
Study approval ric delirium positive and a child who has been
assessed as delirium positive at least once dur-
Informed consent was obtained from parents/ ing his/her stay in PICU was defined as pediat-
guardians of all patients in accordance with a ric delirium. Meanwhile, we identified a priori-
protocol reviewed and approved by the institu- defined, non-mutually exclusive phenotypes of
tional ethical review board of Xinhua Hospital delirium per the presence of hypoxia, sepsis,
Ethics Committee Affiliated to Shanghai Jiao sedative exposure, or metabolic (e.g., renal)
Tong University School of Medicine, Shanghai, dysfunction. Delirium in the absence of hypox-
China (Approved No. of ethic committee: ia, sepsis, sedation, and metabolic dysfunction
XHEC-C-2018-097). was considered to be unclassified. In addition,
the data were collected by the researcher her-
Patient population self and PICU nurses, and the researchers were
authorized by the scale inventor and the trans-
This retrospective observational study was con- lator for the Chinese version. The CAPD was
ducted in 2 PICUs at Xinhua Hospital affiliated validated for use in children and was reliable
to Shanghai Jiao Tong University, which is a for detecting delirium in children of all ages
tertiary-A general hospital in Shanghai, China. (including infants) in PICU. The pilot experiment
Patients admitted to PICU from Dec. 2018 to (n = 20) in this study measured Cronbach’s α of
Aug. 2019 were included. The inclusion criteria CAPD as 0.97. Severity of illness was measured
were as follows: 1) ICU check-in time was more by Pediatric Risk of Mortality IV (PRISM IV) [22]
than 24 hours; 2) Age was between 1 month within 4 hours of being admitted to PICU. The
and 7 years; 3) Informed consent was obtained higher the score, the more severe the condi-
from the parent/guardian. The exclusion crite- tion. Demographic and clinical indicators were
ria were as follows: 1) After being admitted, extracted from the Hospital Information
patients were in a coma or deep sedation with System, including gender, age, duration of
9144 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
mechanical ventilation and sedative drug, CRP delirium with duration of 1 day. The average
and length of PICU etc. was 1.79 (SD = 1.49) days for duration of ICU
pediatric delirium, and the median was 1 day.
When a patient’s arterial blood oxygen pres- The longest duration was 9 days, while the
sure (PaO2) was less than 80 mmHg, the patient shortest was 1 day.
was judged to be hypoxia. When a patient’s
white blood cell count, neutrophil ratio, and Descriptions of patient population
daily maximum body temperature were out of
the normal range, the patient was judged to be Demographics and clinical characteristics of
infected. In addition, sepsis data were obtained the study population are shown in Table 1.
from Nosocomial Infection Monitoring System Pediatric delirium occurred in 200 of 639
(NIM). patients (31.3%) after PICU admission. There
were no statistically significant differences in
Statistical analysis the distribution of sex, gestational age, surgery
or not, pain, head injury, opioid exposure
SPSS 22.0 statistical software was used to between the case group and the control group
analyze and process the data. First, Univariate (P > 0.05), but the differences in the distribu-
analysis (Chi-squared test) was conducted to tion of age, admission diagnosis, emergency
examine the distributions of selected charac- check-in, mechanically ventilated, restrict, ben-
teristics for cases and controls. Moreover, uni- zodiazepine or dexmedetomidine exposure,
variate model analysis and multivariate condi- LOS, PRISM IV score, duration of infection or
tional logistic regressions were used to exam- hypoxia, and CRP were statistically significant
ine whether delirium was with different clinical (P < 0.05).
phenotypes. The associations were presented
as odds ratios (ORs) with 95% confidence inter- Risk factors
vals (CIs). Two-sided P values < 0.05 were con-
sidered statistically significant. The area under As shown in Table 2, a single delirium pheno-
the ROC curve (AUC) was used to determine type was present in only 51 (25.5%) of the 200
the diagnostic performance, and values > 0.75 children with ICU delirium, two phenotypes
were considered to represent good perfor- account for 42%, whereas three or more pheno-
mance. types were present among 47 (23.5%) delirium
patients. Hypoxic delirium was the most com-
Results mon type (61%).
Description of delirium Multivariable logistic regression model for risk
factors of ICU pediatric delirium is shown in
A total of 639 patients met the criteria and Table 3. The risk of ICU delirium in critically ill
were finally admitted to this study. Among 3703 children with mechanical ventilation is 3.78
study days (the sum of the enrollment days of times that of non-mechanical ventilation (95%
all patients), delirium occurred in 581 (15.69%) CI, 2.25-6.35), and the risk of delirium in chil-
study days. It was found that 36% of patients dren with metabolic dysfunction is 3.73 times
with delirium were hyperactive, 41% were hypo- that of metabolic function (95% CI, 2.08-6.71).
active and 23% showed a mix of the types. The The risk of delirium in PICU patients with high
average age was 19.51±23.58 months. The PRISM IV score is 2.2 times that of children
prevalence rate of pediatric delirium in PICU with low PRISM IV score (95% CI, 1.42-3.41).
settings was 31.30%. Among the 200 children Additionally, age of children, hypoxia (OR, 2.69;
with delirium, the first onset of pediatric deliri- 95% CI, 1.53-4.71), duration of infection (OR,
um occurred within the first seven admission 1.22; 95% CI, 1.10-1.36), LOS and CRP are
days to PICU. Among them, 176 cases (88%) of independent risk factors.
delirium occurred for the first time within 72
hours of admission to PICU, 148 cases (74%) Figure 1 shows the area under an ROC curve
occurred for the first time within 48 hours of for combination CRP with duration of infection.
admission, 95 cases (47.5%) occurred for the ROC curve analysis revealed that the area
first time within 24 hours of admission of PICU. under ROC curve (AUC) of combination CRP
Moreover, 107 cases (53.5%) were pediatric with duration of infection on predicting delirium
9145 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
Table 1. Demographics and clinical characteristics of the study population (n = 639)
Never deliriums Ever deliriums Overall Cohort
Characteristic P Value
(n = 439), N (%) (n = 200), n (%) (n = 639), N (%)
Age (month)
37 M 95 (21.6) 20 (10.0) 115 (18.0)
Sex
male 238 (54.2) 110 (55.0) 348 (54.5) 0.461
female 201 (45.8) 90 (45.0) 291 (45.5)
Gestational
Preterm 37 (8.4) 21 (10.5) 58 (9.1) 0.241
No preterm 401 (91.3) 179 (89.5) 581 (90.9)
Admission diagnosis
Sepsis/ARDS 78 (17.8) 63 (31.5) 141 (22.1) 0.008**
Surgery 264 (60.1) 102 (51.0) 366 (57.3)
Asthma, other pulmonary disease 31 (7.1) 12 (6.0) 43 (6.7)
Congestive heart failure, myocardial infarction, or cardiogenic shock 6 (1.4) 3 (1.5) 9 (1.4)
Airway protection 17 (3.9) 7 (3.5) 24 (3.8)
Other 43 (9.8) 13 (6.5) 56 (8.8)
Pain
Yes 178 (89.00) 398 (90.66) 576 (90.01) 0.510
No 22 (11.00) 41 (9.34) 65 (10.17)
Head injury
Yes 3 (1.50) 4 (0.91) 7 (1.10) 0.510
No 197 (98.50) 435 (99.09) 632 (98.90)
Emergency check-in
Yes 90 (20.5) 55 (27.5) 145 (22.7) 0.033*
No 349 (79.5) 145 (72.5) 494 (77.3)
Mechanically ventilated
Yes 45 (10.3) 93 (46.5) 138 (21.6) 0.000**
No 394 (89.7) 107 (53.5) 501 (78.4)
Restrict
Yes 385 (87.7) 192 (96.0) 577 (90.3) 0.000**
No 54 (12.3) 8 (4.0) 62 (9.7)
Opioid exposure
Yes 16 (3.6) 12 (6.0) 28 (4.4) 0.128
No 423 (96.4) 188 (94.0) 611 (95.6)
Dexmedetomidineor exposure
Yes 18 (4.1) 22 (11.0) 40 (6.3) 0.001**
No 421 (95.9) 178 (89.0) 599 (93.7)
Benzodiazepine exposure
Yes 72 (16.4) 66 (33.0) 138 (21.6) 0.000**
No 367 (83.6) 134 (67.0) 501 (78.4)
LOS 0.000**
1-2 183 (41.7) 32 (16.0) 215 (33.6)
3-4 120 (27.3) 48 (24.0) 168 (26.3)
5-6 69 (15.7) 29 (14.5) 98 (15.3)
>7 67 (15.3) 91 (45.5) 158 (24.7)
PRISM IV Score 0.000**
1-6 376 (86.4) 93 (46.7) 469 (74.0)
7-11 53 (12.2) 86 (43.2) 139 (21.9)
≥ 12 6 (14.0) 20 (10.1) 26 (4.1)
CRP (mg/L) 0.001**
< 10 143 (32.6) 40 (20.0) 183 (28.6)
10-50 261 (59.5) 131 (65.5) 392 (61.3)
> 50 35 (8.0) 29 (14.5) 64 (10.0)
9146 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
Duration of Infection 0.81±1.86 4.4±7.60 0.000**
Duration of Hypoxia 0.53±1.46 3.14±6.19 0.000**
Note: *P < 0.05, **P < 0.01. CRP: C-reactive protein; LOS: Length of stay; PRISM IV Score: Pediatric Risk of Mortality IV Score; Duration of Hypoxia: Sum of days of
hypoxia during ICU stay; Duration of Infection: Sum of days of infection during ICU stay.
Table 2. Univariate analysis of delirium with different clinical phenotypes (n = 639)
Overall Cohort (n = 639) Never deliriums (n = 439) Ever deliriums (n = 200)
Clinical Phenotype F P Value
n (%) n (%) n (%)
Hypoxic 1
100.28 0.000**
No 426 (66.7) 348 (79.3) 78 (39.0)
Yes 213 (33.3) 91 (20.7) 122 (61.0)
Septic2 16.01 0.000**
No 532 (83.3) 383 (87.2) 149 (74.5)
Yes 107 (16.7) 56 (12.8) 51 (25.5)
Metabolic3
No 463 (72.5) 369 (84.1) 94 (47.0) 94.53 0.000**
Yes 176 (27.5) 70 (15.9) 106 (53.0)
Sedative-associated4
None 367 (57.4) 273 (62.2) 94 (47.0) 23.18 0.000**
No benzodiazepines 134 (21.0) 94 (21.4) 40 (20.0)
Benzodiazepines 138 (21.6) 72 (16.4) 66 (33.0)
co-exist 140.15 0.000**
1 type 235 (36.8) 184 (41.9) 51 (25.5)
2 types 142 (22.2) 58 (13.2) 84 (42.0)
3-4 types 73 (11.4) 26 (5.9) 47 (23.5)
unclassified 189 (29.6) 171 (39.0) 18 (9.0)
Note: **P < 0.01. 1. Hypoxia (PaO2 < 80 mmHg) or shock. 2. Known sepsis or systemic inflammatory response syndrome criteria. 3. Blood urea
nitrogen > 6.4 mmol/L or serum creatinine > 62 μmol/L. 4. Receipt of benzodiazepine or propofol or dexmedetomidine.
Table 3. Multivariate logistic regression result of risk factors (n = 639)
95% C.I.
Variable B S.E, Wald P Value OR
lower limit upper limit
Age -0.37 0.11 12.11 0.001** 0.69 0.56 0.85
Mechanically ventilated 1.33 0.26 25.32 0.000** 3.78 2.25 6.35
LOS 0.09 0.03 12.99 0.000** 1.10 1.04 1.16
Hypoxia 0.99 0.29 11.90 0.001** 2.69 1.53 4.71
Metabolic dysfunction 1.32 0.30 19.36 0.000** 3.73 2.08 6.71
PRISM IV Score 0.79 0.22 12.49 0.000** 2.20 1.42 3.41
CRP 0.01 0.00 8.60 0.003** 1.01 1.00 1.02
Duration of Infection 0.20 0.05 13.83 0.000** 1.22 1.10 1.36
constant -3.38 0.59 33.04 0.000 0.03
Note: **P < 0.01. CRP: c-reactive protein; LOS: Length of stay; PRISM IV Score: Pediatric Risk of Mortality IV Score; Duration of
Infection: Sum of days of infection during ICU stay.
occurrence was 0.81, when the cut-off value Discussion
was over 0.28, the sensitivity was 75%, and the
specificity was 76%. The predicted results of Delirium is caused by a significantly large range
the independent risk factors were in good of brain dysfunctions rather than specific local
agreement with the actual occurrence of ICU brain disorders. It is a reversible response of
pediatric delirium. The combination CRP with brain tissue to hypoxia, infection, metabolic
duration of infection had good predictive and endocrine imbalances, and certain drugs.
performance. The study results showed that age, mechani-
9147 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
reported that the peripheral
inflammatory response caused
by infection or surgery could
induce the activation of brain
parenchymal cells, promote the
expression of inflammatory
markers in the central nervous
system, and lead to neuronal
and synaptic dysfunction, which
in turn led to delirium. Hoog-
land et al. included a systema-
tic review [28] of 51 animal
experiments, and their conclu-
sions supported this hypothe-
sis. Among critically ill children
suffering from infectious or
inflammatory diseases, it was
found that PICU patients had
the highest prevalence of deliri-
um [10]. Nevertheless, Dechnik
et al. [29] found that there was
no association between CRP
levels and ICU pediatric deliri-
um. In addition, delirium was
also thought to be secondary
complication of systemic infec-
Figure 1. Predictive efficacy of duration of infection and CRP for delirium.
AUC: 0.81; Sensitivity: 0.75; Specificity: 0.76.
tion [30] and regarded as a
result of neuroinflammation in
the brain with associated
cally ventilated, LOS, hypoxia, metabolic dys- release of brain cytokines causing direct neuro-
function, PRISM IV score, CRP, and duration of nal damage [18]; infection may lead to inflam-
infection were the risk factors for ICU pediatric mation stress, and finally increases the preva-
delirium. lence of delirium.
Hypoxia was one of the major risk factors for The severity of the illness affected the occur-
delirium in ICU [1]. Despite the association of rence of ICU pediatric delirium. In this study,
hypoxia with pediatric delirium has not been the scores were divided into three groups: safe
fully explored in children, studies in adults have observation group (1-6), boundary risk group
reported conflicting effects of hypoxia on both (7-11), high risk group (more than 11). Higher
the occurrence and the development of deliri- PRISM IV scores showed trends towards more
um [23-26]. Lopez et al. [27] found that hypoxia delirium (OR, 2.02; 95% CI, 1.42-3.41; P =
was not an independent risk factor for postop- 0.000). The reason for this result may be that
erative delirium, while intraoperative hypoxia as the PRISM IV score of ICU patients increas-
cerebral reperfusion was a risk factor. Hypoxia es, the function of various organs decreases,
is able to cause edema, brain tissue damage including a decline in central cognitive function
and central nervous system disability, which and executive ability. In addition, the critically ill
can result in a decrease in the synthesis and children have excessive stress response, which
release of acetylcholine, and an increase in leads to neuro-endocrine disorders and devel-
dopamine concentration and delirium. opes ICU pediatric delirium. Therefore, the
management of critically ill children should be
Multivariable logistic regression analysis indi- strengthened and improved. Intervention and
cated that elevated c-reactive protein and dura- treatment of the primary disease should take
tion of infection were independent risk factors place as soon as possible to improve the func-
for PICU delirium. The neuroinflammatory tional status of key organs and minimize the
hypothesis represented by Cerejeira et al. [20] risk of delirium [26].
9148 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
There are some limitations in the research. were in accordance with the ethical standards
First, it’s a retrospective observational study of the institutional and/or national research
and can only suggest an association and not committee, as well as the 1964 Helsinki decla-
establish causality. While reporting the inde- ration and its subsequent amendments or
pendent risk factors of ICU pediatric delirium, comparable ethical standard. The guardians of
we did not present intraoperative cerebral oxy- enrolled children gave written informed con-
genation, the degree of hypoxia, infection and sents to participate this research project.
metabolic dysfunction. Therefore, the relation-
ship should be further examined in future stud- Disclosure of conflict of interest
ies. Second, there’re some other factors that
may lead to the occurrence of delirium, such as None.
sleep disturbance and deprivation, sedative
and analgesia drugs, and family members visit- Address correspondence to: Xiao-Hua Ge and
ing, which are not included in our study. Finally, Chang-Rong Yuan, School of Nursing, Naval Medical
the study was conducted in a single hospital in University, 800 Xiangyin Road, Shanghai 200433,
Shanghai, so the conclusions may not be widely China. E-mail: gexiaohua@xinhuamed.com.cn (XHG);
generalizable. Multi-location studies are need- yuancr@fudan.edu.cn (CRY)
ed to validate the independent risk factors of
ICU pediatric delirium. References
Conclusions [1] Van Tuijl SG, Van Cauteren YJ, Pikhard T, Engel
M and Schieveld JN. Management of pediatric
delirium in critical illness: a practical update.
In conclusion, this study demonstrated that
Minerva Anestesiol 2015; 81: 333-341.
age, PRISM IV score, ICU retention time, meta-
[2] Salluh JI, Wang H, Schneider EB, Nagaraja N,
bolic dis-function, duration of infection, hypox- Yenokyan G, Damluji A, Serafim RB and
ia, and mechanical ventilation were the inde- Stevens RD. Outcome of delirium in critically ill
pendent risk factors for ICU pediatric delirium. patients: systematic review and meta-analysis.
These important and notable findings deserve BMJ 2015; 350: h2538.
more consideration when it comes to patho- [3] Madden K, Turkel S, Jacobson J, Epstein D and
physiology and the treatment that will deter- Moromisato DY. Recurrent delirium after sur-
mine its practical and clinical benefit in critical gery for congenital heart disease in an infant.
care pediatric patients. We suggest that active Pediatr Crit Care Med 2011; 12: e413-415.
preventive measures should be taken to reduce [4] Turkel SB, Jacobson JR and Tavaré CJ. The di-
agnosis and management of delirium in infan-
the occurrence of PICU delirium.
cy. J Child Adolesc Psychopharmacol 2013;
Acknowledgements 23: 352-356.
[5] Traube C, Mauer EA, Gerber LM, Kaur S, Joyce
C, Kerson A, Carlo C, Notterman D, Worgall S,
Clinical Trial Registry Number: ChiCTR18000-
Silver G and Greenwald BM. Cost associated
19825 (date of clinical registration: 30/11/ with pediatric delirium in the ICU. Crit Care
2018). This research was conducted at Xinhua Med 2016; 44: e1175-e1179.
Hospital of Shanghai Jiao Tong University. We [6] van den Boogaard M, Schoonhoven L, van der
would like to thank the patients and their fami- Hoeven JG, van Achterberg T and Pickkers P.
lies who participated in the investigation and Incidence and short-term consequences of de-
acknowledge all PICU staffs of Xinhua Hospital lirium in critically ill patients: a prospective ob-
for the data collection. This research received servational cohort study. Int J Nurs Stud 2012;
support from Foundation of Shanghai Municipal 49: 775-783.
Education Commission-Gaoyuan Nursing Grant [7] Schieveld JN, Leroy PL, van Os J, Nicolai J, Vos
(Hlgy1804dxk). The funding bodies played no GD and Leentjens AF. Pediatric delirium in crit-
ical illness: phenomenology, clinical correlates
role in the design of the study and collection,
and treatment response in 40 cases in the pe-
analysis, and interpretation of data and in writ- diatric intensive care unit. Intensive Care Med
ing the manuscript. This study was approved by 2007; 33: 1033-1040.
the Ethics Committee of Xinhua Hospital Affi- [8] Smith HA, Gangopadhyay M, Goben CM,
liated to Shanghai Jiao Tong University School Jacobowski NL, Chestnut MH, Savage S,
of Medicine (approval number: XHEC-C-2018- Rutherford MT, Denton D, Thompson JL,
097). All procedures performed in this study Chandrasekhar R, Acton M, Newman J, Noori
9149 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
HP, Terrell MK, Williams SR, Griffith K, Cooper Castro-Faria-Neto HC. Cognitive dysfunction is
TJ, Ely EW, Fuchs DC and Pandharipande PP. sustained after rescue therapy in experimental
The preschool confusion assessment method cerebral malaria, and is reduced by additive
for the ICU: valid and reliable delirium monitor- antioxidant therapy. PLoS Pathog 2010; 6:
ing for critically ill infants and children. Crit e1000963.
Care Med 2016; 44: 592-600. [18] Maldonado JR. Pathoetiological model of de-
[9] Smith HA, Brink E, Fuchs DC, Ely EW and lirium: a comprehensive understanding of the
Pandharipande PP. Pediatric delirium: monitor- neurobiology of delirium and an evidence-
ing and management in the pediatric intensive based approach to prevention and treatment.
care unit. Pediatr Clin North Am 2013; 60: 741- Crit Care Clin 2008; 24: 789-856, ix.
760. [19] Maldonado JR. Neuropathogenesis of deliri-
[10] Traube C, Silver G, Reeder RW, Doyle H, Hegel um: review of current etiologic theories and
E, Wolfe HA, Schneller C, Chung MG, Dervan common pathways. Am J Geriatr Psychiatry
LA, DiGennaro JL, Buttram SD, Kudchadkar 2013; 21: 1190-1222.
SR, Madden K, Hartman ME, deAlmeida ML, [20] Cerejeira J, Firmino H, Vaz-Serra A and
Walson K, Ista E, Baarslag MA, Salonia R, Beca Mukaetova-Ladinska EB. The neuroinflamma-
J, Long D, Kawai Y, Cheifetz IM, Gelvez J, tory hypothesis of delirium. Acta Neuropathol
Truemper EJ, Smith RL, Peters ME, O’Meara 2010; 119: 737-754.
AM, Murphy S, Bokhary A, Greenwald BM and [21] Dantzer R, O’Connor JC, Freund GG, Johnson
Bell MJ. Delirium in critically Ill children: an in- RW and Kelley KW. From inflammation to sick-
ternational point prevalence study. Crit Care ness and depression: when the immune sys-
Med 2017; 45: 584-590. tem subjugates the brain. Nat Rev Neurosci
[11] Traube C, Silver G, Kearney J, Patel A, Atkinson 2008; 9: 46-56.
TM, Yoon MJ, Halpert S, Augenstein J, Sickles [22] Pollack MM, Holubkov R, Funai T, Dean JM,
LE, Li C and Greenwald B. Cornell assessment Berger JT, Wessel DL, Meert K, Berg RA, Newth
of pediatric delirium: a valid, rapid, observa- CJ, Harrison RE, Carcillo J, Dalton H, Shanley T,
tional tool for screening delirium in the PICU.
Jenkins TL and Tamburro R. The pediatric risk
Crit Care Med 2014; 42: 656-663.
of mortality score: update 2015. Pediatr Crit
[12] Silver G, Traube C, Kearney J, Kelly D, Yoon MJ,
Care Med 2016; 17: 2-9.
Nash Moyal W, Gangopadhyay M, Shao H and
[23] Jayaswal AK, Sampath H, Soohinda G and
Ward MJ. Detecting pediatric delirium: devel-
Dutta S. Delirium in medical intensive care
opment of a rapid observational assessment
units: incidence, subtypes, risk factors, and
tool. Intensive Care Med 2012; 38: 1025-
outcome. Indian J Psychiatry 2019; 61: 352-
1031.
358.
[13] Smith HA, Boyd J, Fuchs DC, Melvin K, Berry P,
[24] Şenel G, Uysal N, Oguz G, Kaya M, Kadioullari
Shintani A, Eden SK, Terrell MK, Boswell T,
N, Koçak N and Karaca S. Delirium frequency
Wolfram K, Sopfe J, Barr FE, Pandharipande
PP and Ely EW. Diagnosing delirium in critically and risk factors among patients with cancer in
ill children: validity and reliability of the pediat- palliative care unit. Am J Hosp Palliat Care
ric confusion assessment method for the in- 2017; 34: 282-286.
tensive care unit. Crit Care Med 2011; 39: [25] Wang J, Li Z, Yu Y, Li B, Shao G and Wang Q.
150-157. Risk factors contributing to postoperative de-
[14] Silver G, Traube C, Gerber LM, Sun X, Kearney lirium in geriatric patients postorthopedic sur-
J, Patel A and Greenwald B. Pediatric delirium gery. Asia Pac Psychiatry 2015; 7: 375-382.
and associated risk factors: a single-center [26] Tang B, Wang XT, Chen WJ, Zhu SH, Chao YG,
prospective observational study. Pediatr Crit Zhu B, He W, Wang B, Cao FF, Liu YJ, Fan XJ,
Care Med 2015; 16: 303-309. Yang H, Xu QH, Zhang H, Gong RC, Chai WZ,
[15] Daoud A, Duff JP and Joffe AR. Diagnostic ac- Zhang HM, Shi GZ, Li LH, Huang QB, Zhang LN,
curacy of delirium diagnosis in pediatric inten- Yin MG, Shang XL, Wang XM, Tian F, Liu LX, Zhu
sive care: a systematic review. Crit Care 2014; R, Wu J, Wu YQ, Li CL, Zong Y, Hu JT, Liu J, Zhai
18: 489. Q, Deng LJ, Deng YY and Liu DW. Experts con-
[16] Traube C, Silver G, Gerber LM, Kaur S, Mauer sensus on the management of delirium in criti-
EA, Kerson A, Joyce C and Greenwald BM. cally ill patients. Zhonghua Nei Ke Za Zhi 2019;
Delirium and mortality in critically ill children: 58: 108-118.
epidemiology and outcomes of pediatric deliri- [27] Lopez MG, Pandharipande P, Morse J, Shotwell
um. Crit Care Med 2017; 45: 891-898. MS, Milne GL, Pretorius M, Shaw AD, Roberts
[17] Reis PA, Comim CM, Hermani F, Silva B, LJ 2nd and Billings FT 4th. Intraoperative cere-
Barichello T, Portella AC, Gomes FC, Sab IM, bral oxygenation, oxidative injury, and delirium
Frutuoso VS, Oliveira MF, Bozza PT, Bozza FA, following cardiac surgery. Free Radic Biol Med
Dal-Pizzol F, Zimmerman GA, Quevedo J and 2017; 103: 192-198.
9150 Am J Transl Res 2021;13(8):9143-9151Analysis of risk factor for ICU pediatric delirium
[28] Hoogland IC, Houbolt C, van Westerloo DJ, van [30] Munjal S, Ferrando SJ and Freyberg Z.
Gool WA and van de Beek D. Systemic inflam- Neuropsychiatric aspects of infectious diseas-
mation and microglial activation: systematic es: an update. Crit Care Clin 2017; 33: 681-
review of animal experiments. J Neuroinflam- 712.
mation 2015; 12: 114.
[29] Dechnik A, Mauer EA, Gerber LM and Traube C.
C-reactive protein and procalcitonin levels may
not predict delirium in critically ill children.
Pediatr Crit Care Med 2020; 21: e967-e971.
9151 Am J Transl Res 2021;13(8):9143-9151You can also read