OVARIAN CANCER 101 JESSICA MCALPINE, MD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ovarian Cancer 101 Jessica McAlpine, MD
Outline: Ovarian Cancer •Different types of ovarian cancer: •Presentation, behavior, site of origin •Primary treatment: surgery, chemo, +/-radiation •Role of geneticsempowering decision making •Screening (lack of) and PREVENTION! •Surveillance: screening for other cancers, treatment effects, interplay of other health issues
Old School….
Germ Cell Sex Cord-Stromal
(3%-5%) (2%-3%)
Secondary
(Metastatic)
Epithelial (EOC)
(5%)
(90%)
Figure modified from Gartner, L.P. & Hiatt, J.L. eds. In Color Atlas of Histology.
3rd ed. (2000) Lippincott Williams & Wilkins: Philadelphia, PA.
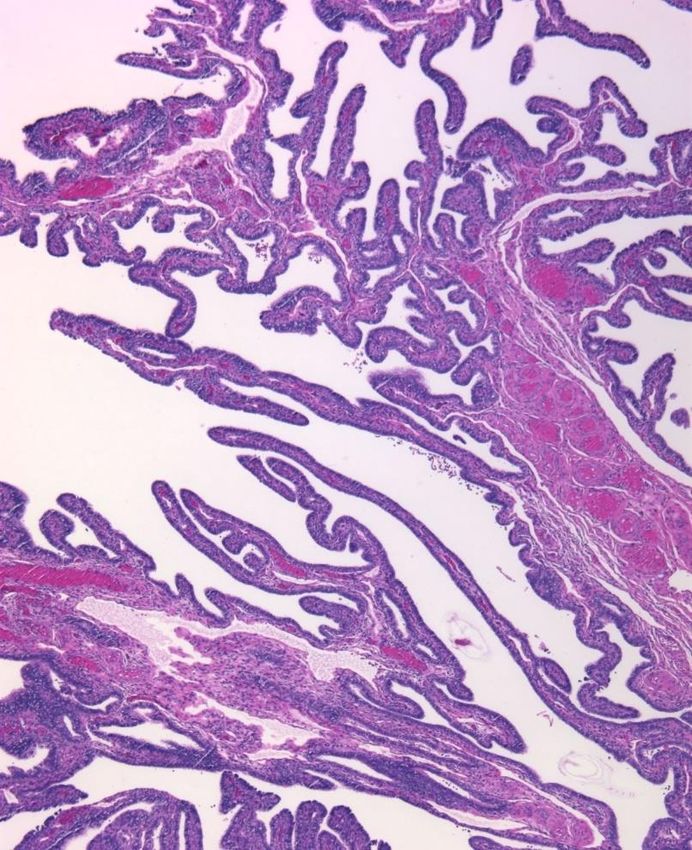
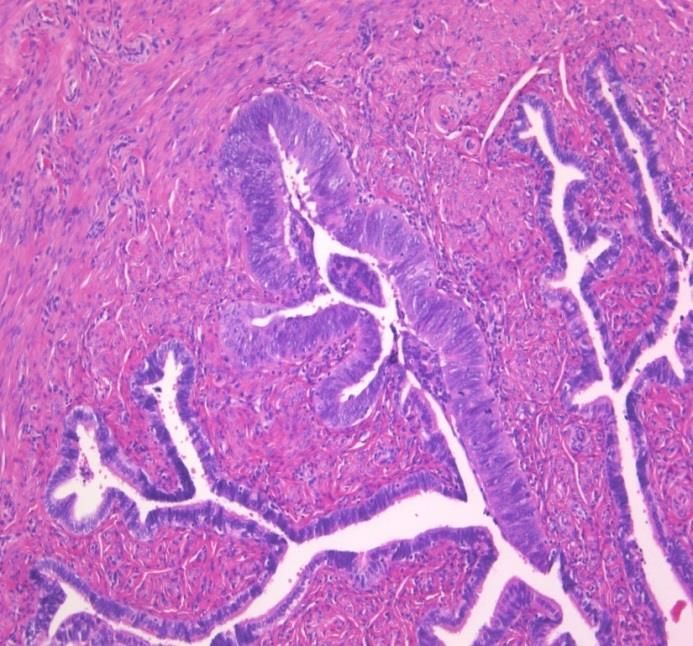
New Era: “epithelial ovarian cancer”
encompasses ~5 distinct diseases
Serous Endometrioid Mucinous Clear cell Transitional Undifferentiated
Grade 1 3.5% 10%
4%
Grade 2
10%
Grade 3 70%
2% NOS
Grouping reflects epidemiology, germline genetics,
somatic genetics, clinical presentation and response to
therapy
New Era!
The only true “ovarian” cancers=germ cell and sex
cord stromal
EOC=primarily non-ovarian
HGS: from the FT
Clear cell and EM: from endometrioisis
Mucinous: ? Paratubal cysts
Kurman and Shih, 2011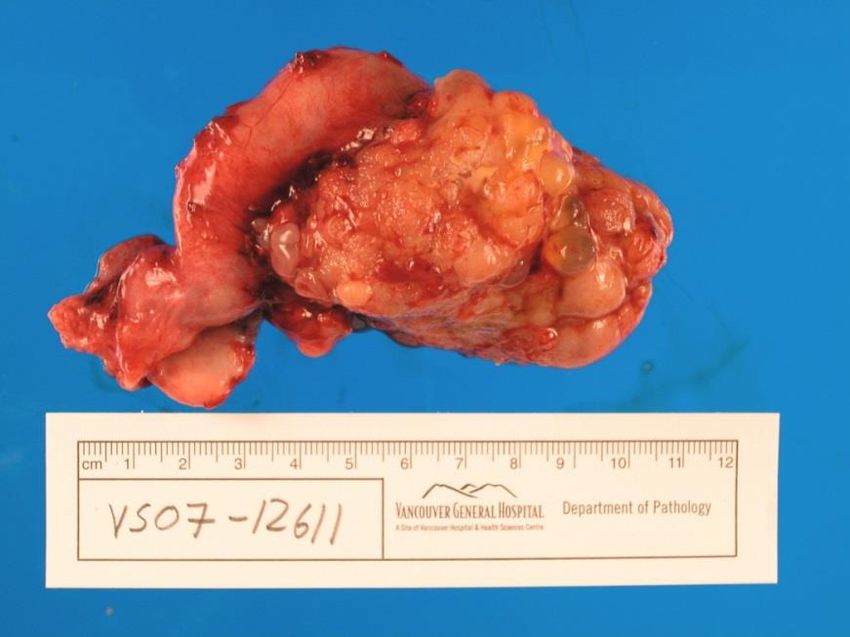
Anatomy 101
HGS: site of origin is the fallopian
tube
Does the fallopian tube make sense? • Histology of the fallopian tube epithelium is serous • The surface area of the fimbriated end of the tube is massive compared the ovary
Evidence: ascending inflammation
Increases risk: Decreases risk:
-Tubal ligation
-PID -OCP
-Tubal infertility -Pregnancy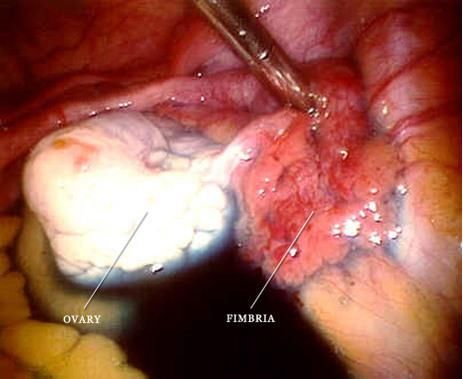
Anatomy: why are symptoms vague? Symptoms frustrating as non-specific : Gastrointestinal Bladder Pelvic
Stage and Grade: what do the mean? Stage basics: I-confined to one or both ovary(ies) II-confined to pelvis III-spread to abdomen (microscopicbig or nodes) IV-distant Grade: how abnormal the cells look….aggressive features like high ratio nuclei : cytoplasm, mitoses
Treatment for ovarian cancer
• Surgery: remove ovaries, tubes, uterus,
omentum…”debulk”
+ =>Treatment for ovarian cancer • Most patients will undergo 6 cycles of outpatient intravenous and/or intraperitoneal chemotherapy • Chemotherapy may start before surgery (i.e., for 3-4or even 6 cycles) or after…. • Most common agents used: – carboplatin and paclitaxel every 3-4 weeks • IV~3-5 hours to administer=outpatient
Chemotherapy Treatment for ovarian cancer • Intraperitoneal chemotherapy (IP) may be combined with IV. Drugs are injected into the abdominal cavity by a catheter attached to a port. Longer infusion. • Theory of “bathing the cells in drug”, higher dose absorbed…better survival in some series but weekly taxol and other regimens ~ comparable (?!) • It is inserted at staging or interval debulking surgery • Side effects (especially nausea) can be more severe than traditional chemotherapy
Intraperitoneal chemotherapy
Side effects of treatment • First few days post Rx: fatigue, nausea, bony aches • Nausea adjustment medications/options • 7-12 days post treatment: more vulnerable to infection, low blood counts/anemia • Loss of hair after 1st or 2nd cycle • Tingling/paresthesias in stocking-glove distribution
Treatment for ovarian cancer • Radiation sometimes used …primarily for endometrioid and clear cell histologies
Communicate your symptoms! MD needs to listen!
What about family?
Lifetime risk Family history • General pop lifetime risk: 1.6% • If only one first-degree relative is affected by ovarian cancer: 5% • BRCA 1: 40-63% by age 70 • Lifetime risk breast cancer 60-80% • BRCA 2: 20-27% risk by age 75 • Lifetime risk breast cancer 60-80% • HNPCC: 10-12% lifetime risk • Lifetime risk colorectal cancer 60-80%
Considerations for family members • Both HNPCC and BRCA mutations are inherited in an autosomal dominant fashion • This means a child who has a parent with a mutation has a 50% chance of inheriting that mutation. A brother, sister, or parent of a person who has a mutation also has a 50% chance of having the same mutation.
Referral to Hereditary Cancer Program • Local Hereditary Cancer program-when to refer, who, how….. – Family history good but will miss MANY – Histology based referral very effective – >20% HGS cancers will have BRCA1/2 mutation • ANY high grade serous ovarian cancer should be referred for BRCA testing OR ANY clear cell or endometrioid ovarian or endometrial cancer patient where pathology comments on absent MMR proteins should be tested for HNPCC **Now recommends referral on pathology form in a growing number of centers**
What about screening?
Screening • 3 large randomized controlled trials have thus far shown no appreciable difference in outcomes with an unacceptable amount of unnecessary surgery (even in high risk women) • We recommend to NOT order CA125 levels and/or ultrasounds in the absence of specific symptoms suggesting presence of disease
What can we do? • Annual abdominal and pelvic examination (including pelvirectal) • Risk reduction with oral contraceptive pill • Risk reducing surgery: tubal ligation, salpingectomy, and for BRCA mutation carriers/HNPCC consider BSO at completion of childbearing
Prevention
Fallopian tube in situ lesions are precursor to
“ovarian cancer”….
Remove the precursor!Change Surgical Convention • ~18% of BC’s population of women with ovarian cancer had undergone hysterectomy • Hysterectomy and tubal ligation are common • WHY NOTE REMOVE THE FALLOPIAN TUBE? • Perform salpingectomy with hysterectomy and consider in place of tubal ligation September 2010 Campaign
Projected Outcome
• Conservatively, up to 40% reduction in ovarian
cancer deaths after 20 years
– Through salpingectomy at time of hysterectomy
– Through salpingectomy instead of tubal ligation
– Through risk-reducing BSO in patients with BRCA
mutationsLiving with ovarian cancer • Goal (and truly can be) =curable disease!
Survivorship encompasses the physical, psychological, social, and spiritual domains of individuals with cancer from the time of diagnosis, through treatment, and on…
Even for 1 disease the survivorship needs can vary with different QOL considerations
over the course of care e.g., along the survivorship continuum
Diagnosis and Primary
Treatment
A. Physical Treatment for
nausea emesis recurrent or
neuropathy End-of-Life
Maintenance/ refractory disease
nephropathy Support/Palliation
fatigue Consolidation Therapy A – E. as in primary
therapy A. Physical
hair loss A. Physical Pain
cumulative
bone health • cumulative toxicities Bowel obstruction
treatment toxicities
hormonal changes F. Socioeconomic Pleural effusions
Increase
sexual health • additional costs and visits Ascites
hypersensitivity
infertility C – D. Psychosocial &
reactions
pain socioeconomic
(platinum)
change in bladder or
Advance directives
bowel function
Power of attorney
B. Cognitive Cancer Surveillance/ E. Spiritual
memory loss Observation Peace/resolution;
concentration A. Physical friends/family/self/
C. Psychosocial fatigue God(s)
anxiety sequelae of chemotherapy
depression or surgery (i.e.,
fear of recurrence neurotoxicity)
partners/family B – E. as in primary therapy
relationships
F. Preventive health Long-term (>5 years) Survival
body image A. Physical
(re-)initiation of general
D. Socioeconomic healthcare sequelae of treatment
cost of treatment guidelines/screening - i.e., neurotoxicity
demand of hospital visits referral to hereditary -i.e., end organ disease
consideration of end-of- cancer program - i.e., secondary cancers
life financial planning fracture risk/bone health B – E. as in primary therapy
E. Spiritual F. Preventive health
personal strength & as in surveillance period + screening for secondary cancers
growthSurveillance:
• Regular intervals w/ physical examinations
• Some reliance on symptoms/changes
• We DON’T tend to do:
– Routine imagingradiation dose accumulation
– Routine CA125 no improvement in survival and
risk of decreasing the amount of good QOL timeWhat can we do/what should we ask? • What type was my cancer, what was done, what is known about this specific disease now? • Family testing and follow-up with action if + • Side effects; perhaps we can help? • Catch up on general health recommendations! • Support and empowerment: Inspire Health, OCC, OCNA, patient and family counseling…. • New changes/symptoms; maybe we should examine?
Recurrence: not doom and gloom! Chemical vs. Imaging vs. Symptomatic recurrence • OR/Surgery – for isolated recurrence or very long time since primary – disease that is resistant to chemotherapy – for bowel obstruction/acute event • Chemotherapy for ~ all others-consider clinical trials or molecular targeted therapy? Rarely radiation. • Observation or supportive care?
• Questions? BCCA 604 877 6000 x 2367 jessica.mcalpine@vch.ca
You can also read

















































