PEDIATRIC DIABETIC KETOACIDOSIS (DKA) - Faculty Disclosure - CECentral
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
6/15/2019
PEDIATRIC DIABETIC
KETOACIDOSIS (DKA)
Alba E. Morales, MD
Associate Professor of Pediatrics
Barnstable Brown Diabetes Center/ UK Healthcare
June 15, 2019
Faculty Disclosure
• No relevant financial relationships to disclose.
1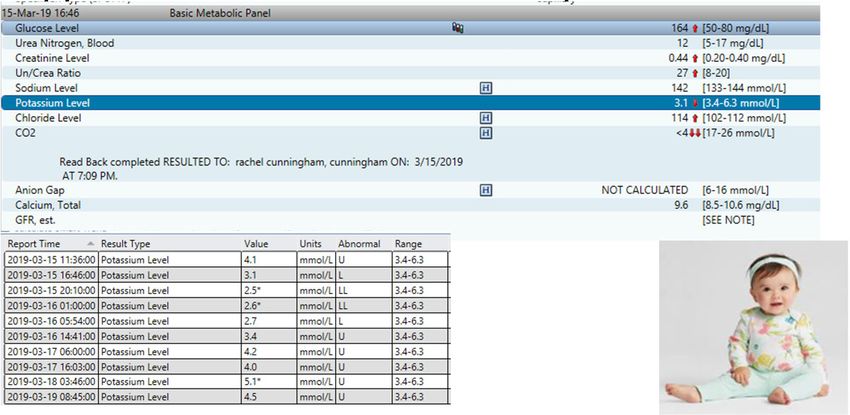
6/15/2019
Objectives
Upon completion of this educational activity, you will be able to:
• Describe the diagnostic criteria of pediatric DKA
• Calculate the fluid and insulin requirements for a child with DKA
• Identify the risk factors for cerebral edema in pediatric DKA
Expected Outcome
• Participants will become familiar with the early assessment and management of
pediatric DKA
2
6/15/2019
CASE
• 10 month old female • Sent to nearby emergency department
Labs‐ large ketonuria, hyperglycemia,
• Unremarkable past medical history acidosis, HbA1c= 9.8%
• Looked sick for 3 days, anorexia for 1
day
• To clinic for fast breathing
• Finger‐stick “Hi” in clinic
• 1 lb. weight loss as per clinic chart
Symptoms and signs of diabetes in
childhood
Neonates and infants Toddlers, older children
• Shock • New or worsening enuresis (parents
expect UTI)
• Weight loss
• Daytime “accidents”
• Sepsis‐like picture
• Weight loss, obesity + weight loss
• Tachypnea, respiratory distress
• Acute abdomen, vomiting
• “by the book” presentation
• Yeast infection
3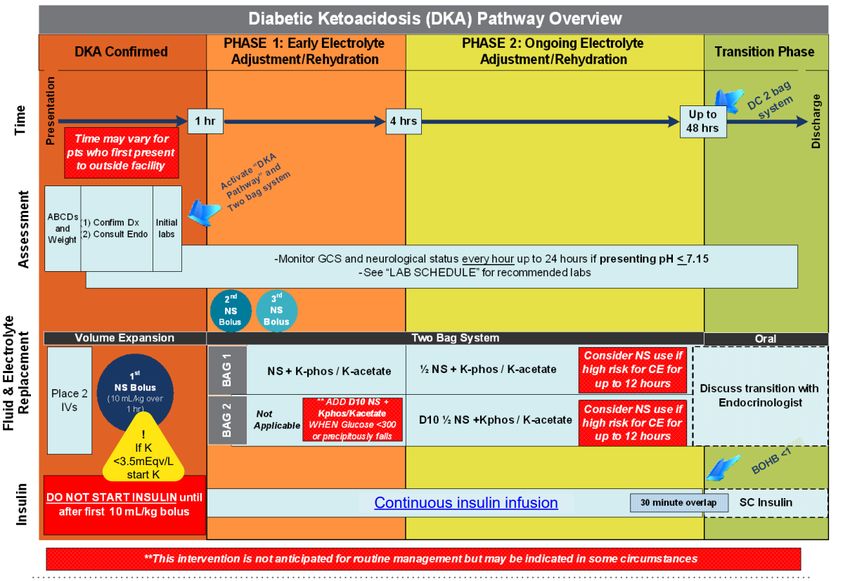
6/15/2019
ED
• Drowsy
• Grunting respirations, RR= 60‐75,
HR=120‐166
• Dry lips and tongue
• Clear lungs
• Tachycardia but no murmur
• Soft benign abdomen
• Cap refill?
Definition of DKA
• 1. Hyperglycemia > 200 mg/dl AND
• 2. Ketonemia (BOHB > 1 mmol/L) AND
• 3. Venous pH < 7.3 or HCO3 < 15 mEq/L
• Classification‐
• mild pH 16
• moderate pH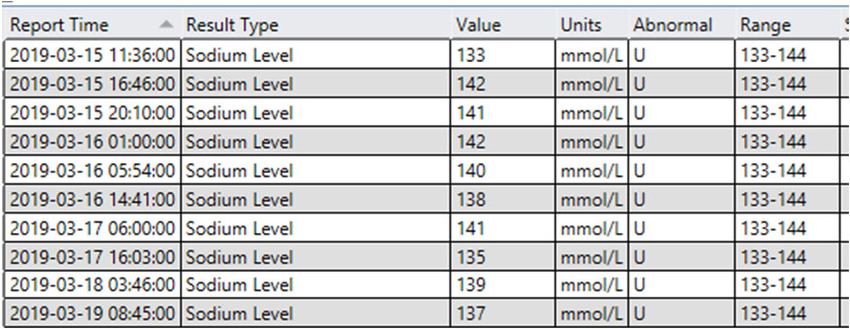
6/15/2019
Source of Metabolic Acidosis in DKA
• Ketonemia (insulin deficiency)
• Lactic acidosis (dehydration)
• Renal dysfunction (dehydration)‐ loss of bicarbonate in urine
Other causes of metabolic acidosis
• Sepsis/septic shock
• Hyperosmolar non‐ketotic diabetic coma
• Alcoholic ketoacidosis
• Uremia due to underlying kidney or liver disease
• Salicylate overdose
5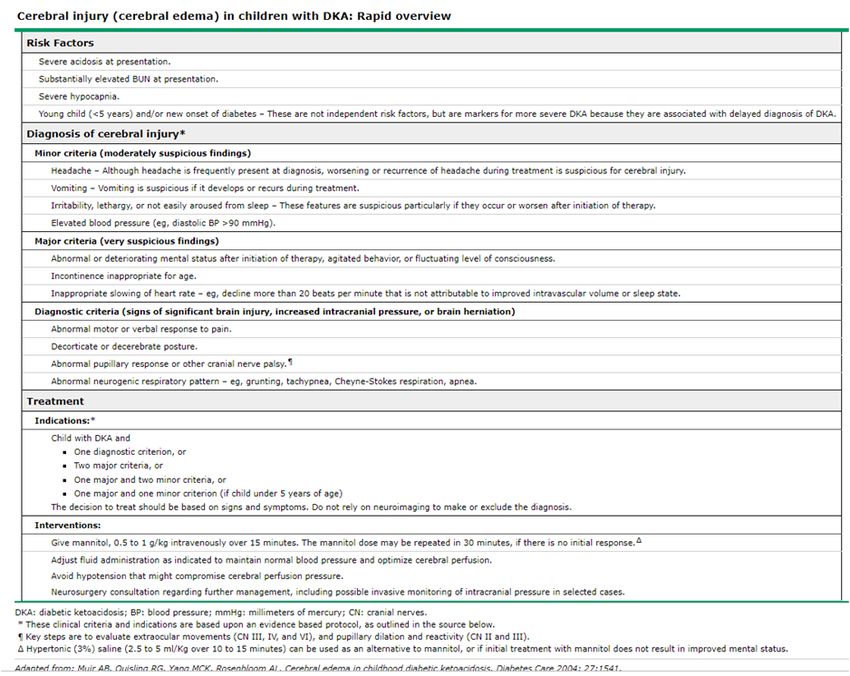
6/15/2019
Who is at risk of DKA?
New onset diabetes (Type 1 most
commonly) Established diabetes
• Age < 4 years • 1‐10% per patient/ year= risk of DKA
• Children with NO 1st degree relative • Poor metabolic control
with diabetes
• Previous episodes of DKA
• Lower SE status
• Adolescent girls
• Unusual triggers:
• Steroids • Youth with eating disorders/ other
psychiatric illness
• Atypical antipsychotics
• Diazoxide • Difficult family circumstances/ low SE
• Immunosuppressive drugs status
Morbidity and Mortality of DKA in
Children
• Mortality has been constant at 0.15% (USA)
• Cerebral edema (CE) accounts for 57‐87% of all DKA deaths
• Depending on the study, CE incidence in patients with DKA varies from 1‐4%
approximately and has been stable over last decade or so
• Mortality rates from CE in population studies have been reported as high as 25%
6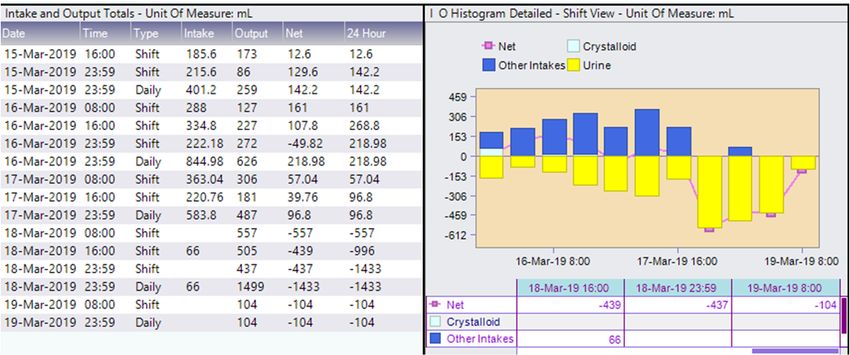
6/15/2019
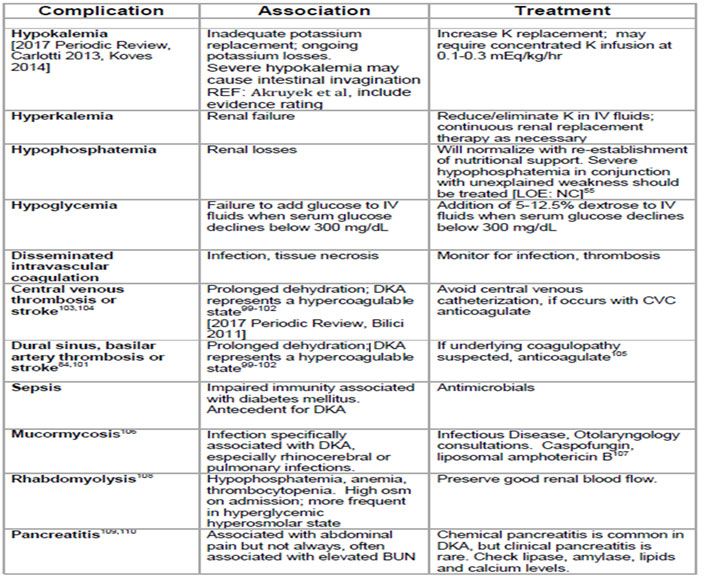
Other causes of mortality and severe
morbidity‐
• Hypokalemia
• Hyperkalemia
• Hypoglycemia
• Other CNS complications
• Hematoma, thrombosis, sepsis, infections, ARDS
• Late sequelae of cerebral edema (hypothalamic/ pituitary deficiencies)
Pathophysiology
• Complete or relative insulin deficiency gives rise to accelerated, unchecked
ketogenesis and hyperglycemia (CATABOLIC STATE)
• Hyperglycemia causes progressive dehydration that can lead to renal dysfunction
and severe loss of electrolytes (HYPOKALEMIA)
• Volume depletion and acidosis cause increased production of counter‐regulatory
hormones which in turn worsen the above
• Glucagon, catecholamines, GH, cortisol all contribute to increased gluconeogenesis and
impaired peripheral glucose utilization leading to worsening hyperglycemia and
hyperosmolality
7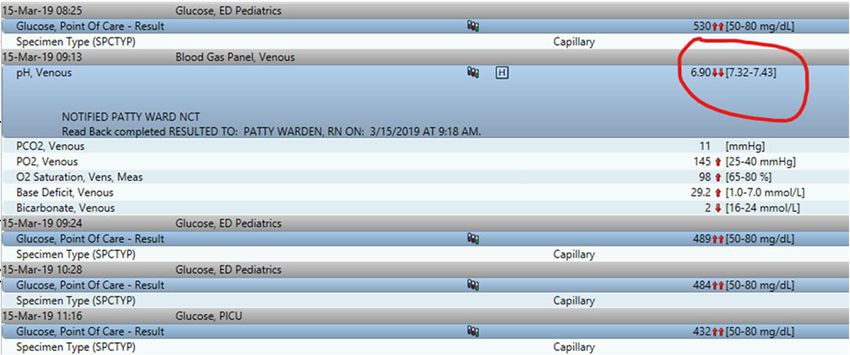
6/15/2019
DKA is caused by insulin deficiency
SEVERE DEPLETION OF WATER AND ELECTROLYTES FROM THE INTRA ‐AND
EXTRA‐ CELLULAR FLUID COMPARTMENTS
Diabetic Ketoacidosis
• PREVENTION is best
• All families with diabetic children are educated on DKA prevention
• Provided with an educational magnet to keep handy
8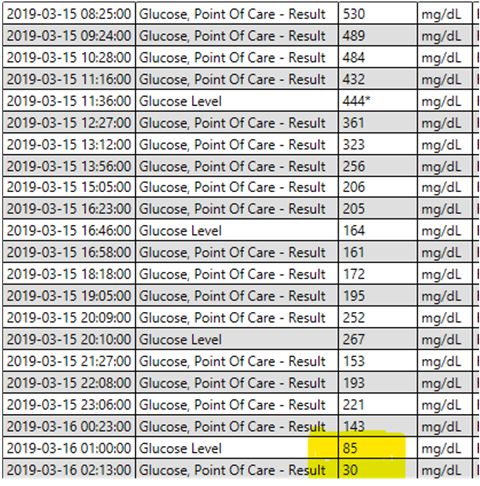
6/15/2019
DKA prevention magnet
provided to all families
Where should DKA be managed?
• Unit should have
• Experienced nursing staff trained in monitoring and management
• Written guidelines for DKA management in children
• Access to laboratories able to provide frequent and timely measurements of
biochemical variables
• Specialist/ consultant pediatrician with training and expertise to guide management
• Severe DKA, those with mental status changes, compromised circulation, and children
under age 4‐5 should be managed in an intensive care setting
9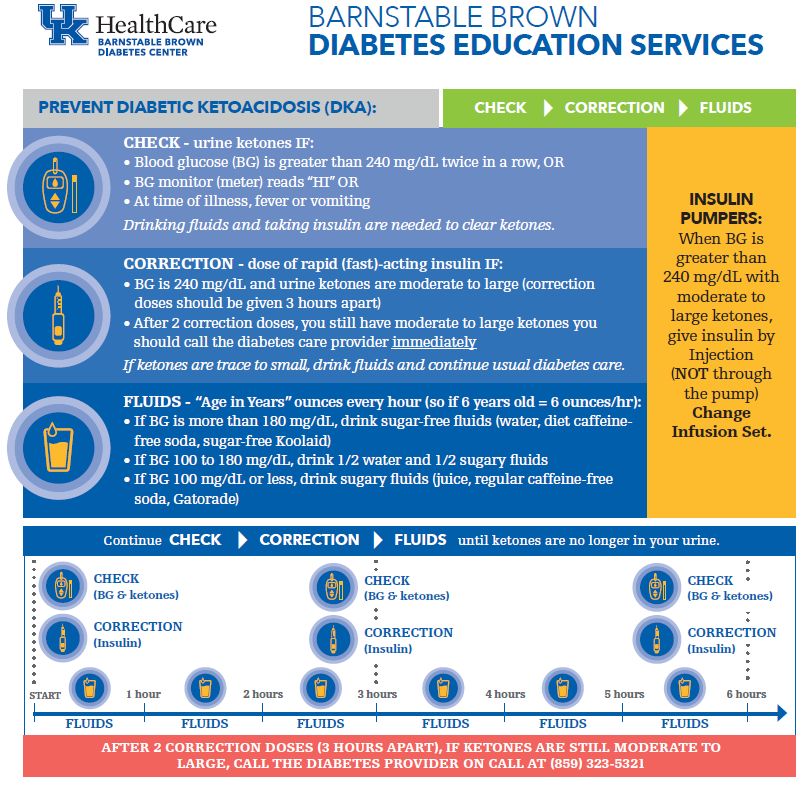
6/15/2019
Disposition
• Admission
• New onset diabetes
• Mild and moderate DKA to floor if no other risk factors for Cerebral edema
• Unable to manage DM, ketosis at home
• Discharge mild DKA with no risk factors home after consultation with specialist
• Insulin pump malfunction‐ must have access to long acting insulin, injections at home
• Good PO intake
• Well‐trained family
Disposition
New onset T1DM Established T1DM
• Will always need hospital admission • Mild DKA and improving, tolerating
PO and well trained family‐ may be
• PICU discharged home
• Floor • Severe and Moderate DKA‐
admission will be required
• PICU
• Floor
106/15/2019
Disposition‐ consider intensive care transfer‐
o Presenting BUN > 30
o Patient received IV bicarbonate or insulin bolus
o Calculated mOsm > 350
[Calculated osmolality= 2xNa + (glucose/18) + (BUN/2.8)]
o Patient received > 40 mL/kg total initial volume replacement (include fluids
received prior to arrival to SCH)
o Corrected Na< 140 mEq/L or decreasing at 2 hour labs
[Corrected Na = Measured Na + (Serum glucose – 100)/100 X 1.6)]
ED
• 10 cc/kg NS bolus via IO line
• Transferred to PICU
116/15/2019
Assessment, new diabetes diagnosis, confirm DKA
(Ideally within first 30 minutes)
Consider RISK factors HPI Signs Laboratory investigation
Prior DKA episodes Polyuria Dehydration Blood glucose
Insulin omission (poor Polydipsia Kussmaul breathing Blood gas
adult supervision) New enuresis Fruity smell of breath Na, K, Cl, HCO3, Ca,
Adolescent females Nocturia Emesis Mg, Phos
Negative Social factors Weight loss Abdominal tenderness BUN, Cr
Recent illness, Abdominal pain (diffuse) BOHB
infection Severe fatigue Mental status changes Blood culture if febrile
Psychiatric disorder Nausea Lethargy
Eating disorder Weakness
Surgery, trauma, Headache
obesity Confusion
Use of diabetogenic Candida infection
meds Drowsiness
126/15/2019
ABCD and WEIGHT
• Airway (PALS)
• Breathing (PALS)‐ deep rhythmic fast (Kussmaul) , hypoxia
• Circulation‐ shock? Dehydration‐ cap refill time > 2 sec, etc.
• Disability/ Neurological evaluation
• GCS at admission and at least every hour for at least 12 hours
• Headache history documentation
• Developmental delay, non‐verbal patients *
• Will need exact weight to calculate all fluids and insulin doses
Assess neurologic stability
• Glasgow coma scale in children > 5 years of age
• Verbal response criteria for children under 5 years
136/15/2019
GCS
Disposition‐ consider intensive care transfer‐
o Age ≤ 24 months
o Developmental delay or any condition that compromises communication
o GCS ≤ 13 after volume resuscitation
o Abnormal neurological exam after volume replacement
o Other organ system dysfunction
o Presenting pH ≤ 7.15
o Presenting HCO3 ≤ 5
o Presenting PCO2 < 10
146/15/2019
Goals of therapy
• Resolve acidosis as evident by anion gap < 15
• Prevent complications such as cerebral edema, hypoglycemia, hypokalemia, etc.
• Supportive therapy, including improvement in hydration status and management of
electrolyte abnormalities
Reverse DKA
Rehydrate Stop ketogenesis
• 1st HOUR: • INSULIN
• resuscitation fluids (10‐20 ml/kg • No bolus needed and may be
0.9%NS bolus, repeat if needed up to associated with increased risk for
30 ml/kg total) cerebral edema
• Overt shock‐ 20 ml/kg 0.9% NS bolus
• 0.1 unit/ kg/hour regular insulin is
• Subsequent fluids need to be default rate
calculated to replace deficit and
provide maintenance fluids using
body weight as reference
156/15/2019
Rehydration
• 10 ml/kg 0.9%NS bolus over one hour, may repeat if needed up to 30 ml/kg total
resuscitation fluids
• Subsequent fluids: (in tandem with insulin infusion)
• Assume 7% dehydration (replace deficit and calculate maintenance fluids over 24‐
36 hours)
• Equal to 1.5‐2X maintenance rate
• 2 bag system (D10 bag and NS or ½ NS bag with additives)
Example
• 35 Kg child with BG= 380 mg/dl; serum K=4.8; Na= 138
• 350 ml NS bolus over 1 hour, then re‐assess need for another bolus
• AFTER NS bolus:
• DO NOT give insulin bolus
• Start insulin 0.1 unit/kg/hr In tandem with rehydration fluids
• 1.5‐2 X maintenance for 35 kg child= 2700‐3600/ 24 hours = 112 – 150 ml/hr
• Replacement IV fluid order for this child: (remember to add potassium)
• 0.9%NS + 20 meq KCL and 20 meq/L Kphos at 112‐150 ml/hr
• Insulin‐ 3.5 units/hr
166/15/2019
Subsequent IV fluids order:
• 12 hours after first bolus or once serum chloride is ~ 110 meq/L (still using 2 bags)
• Bag # 1‐‐‐‐D10 ½ NS + 20 meq KCL + 20 meq Kphos
• Bag #2‐‐‐‐½ NS+ 20 meq KCL + 20 meq Kphos
• BG > 300‐ use only fluids with no dextrose
• BG 200‐300 use both types of fluids (50‐50)
• Bg < 200 use only D10 containing fluids
• Decreasing NaCl content in IV fluids will help avoid hyperchloremic acidosis, a common
complication of DKA therapy
Sodium trend
176/15/2019
Hyperglycemia vs acidosis
How much dextrose in IV fluids?
D10 + 40 meq K bag NS or ½ NS + 40 meq K bag
BG > 300 n0 100 % of rate
BG 200‐300 50% of rate 50% of rate
BG< 200 100 % of rate n0
If BG < 70 and still acidotic‐ consider use of D12.5 or increase rate of D10 bag, if acidosis resolved,
should be able to eat and transition to SQ insulin
UK PICU DKA Protocol
Hyperglycemia will always resolve faster than acidosis
186/15/2019
Hypokalemia‐ common complication
Monitoring
• Continuous cardiorespiratory monitoring
• Bedside finger‐stick BG q 1 hour – alert MD if BG < 70 or > 400
• Neurochecks q 1 hour if ANY mental status alteration or risk factors for CE present
• BMP q 4 hours , measure serum BOHB (β‐hydroxybuterate) ‐ < 1 mmol/L indicates
resolution of DKA
• Bedside ketonemia monitoring available ( ideally using handheld meters that measure
both glucose and ketones in capillary blood)
196/15/2019
Monitor I’s and O’s very closely
use HR, perfusion as hydration indicators
DKA complications
206/15/2019
Take home messages
DO AVOID
• Have a high index of suspicion for • Use of Bicarbonate
diabetes in children of all ages
(incidence of T1DM has been • > 40 ml/kg as bolus
increasing in infants and toddlers)
• Lowering insulin infusion rate due to
• Know diagnostic criteria for DKA dropping BG levels if acidosis still
• Timely rehydration will normalize present
intravascular volume/ peripheral • Using imaging studies to “confirm”
perfusion and will help normalize suspected cerebral edema
counter‐regulatory hormone levels
• Insulin will shut down ketogenesis
and will reverse catabolic state
Boston, MA, Chicago, IL, Columbus, OH, Denver, CO, Houston,
TX, New York, NY, Philadelphia, PA, Providence, RI, Sacramento,
CA, Salt Lake City, UT, St. Louis, MO, Washington, DC, and
Wilmington, DE.
216/15/2019
Therefore‐ new suggested fluid guidelines
Key points in regards to cerebral edema
• Regard cerebral edema as a complication of DKA that can happen at any time during
presentation (BEFORE and during DKA therapy)
• Detailed and frequent monitoring for CNS changes is key for early intervention
• Markers of severity of DKA (AT PRESENTATION) are useful as markers for increased risk of
cerebral edema:
• Increased BUN
• Greater hypocapnia
• Severity of acidosis
• Younger age= delayed diagnosis and more severe DKA
• Use of bicarbonate for treatment of acidosis
• Attenuated rise in serum Na during treatment
• Serum sodium should rise by approximately 1.6 mEq/L for every 100 mg/dL (5.5 mmol/L) decrease in
glucose concentration
226/15/2019
Clinical Cerebral Edema assessment
Diagnostic Criteria * Major Criteria Minor Criteria
Abnormal motor or verbal response Altered mentation/ fluctuating level Emesis
to pain of consciousness
Decorticate or decerebrate posture Sustained heart rate deceleration Headache (especially if new/
(more than 20/min) not attributable recurrent after therapy started or if
to improved intravascular volume worsening in nature)
or sleep
Cranial nerve palsy (especially III, IV, Age‐inappropriate incontinence Lethargy ; not easily arousable
and VI) may result in double vision
Abnormal neurogenic respiratory Diastolic BP > 90 mm Hg
pattern (grunting, central
hyperventilation, apneusis, Cheyne‐
Stokes)
Age < 5 years
• 1 diagnostic, or 2 major, or 1 major and 2 minor criteria have a sensitivity of 92%, a specificity of 96% and a
false positive rate of only 4% for the recognition of DKA CE early enough for effective intervention
• In children < 5; 1 major and 1 minor criteria could be sufficient
Emergent Treatment of Cerebral Edema
• Maintain patent airway, ventilation/oxygenation and stable hemodynamics
• Elevate HOB 30 degrees
• Mannitol 1 g/kg I V (cerebral edema); 3% NS (5ml/kg) can also be used if not
responding to Mannitol
• STAT non contrast CT scan of the head, look for CE, thrombosis, hemorrhage
• STAT neurosurgery consult
UK PICU Protocol
236/15/2019
Bibliography
1. Waller SL, Delaney S, Strachan MWJ . Does an integrated care pathway enhance the management • 9. Glaser N, Kuppermann N. Fluid treatment for children with diabetic ketoacidosis: How do the
of diabetic ketoacidosis? Diabetic Medicine.2007:24;359 ‐63. results of the pediatric emergency care applied research network Fluid Therapies Under
Investigation in Diabetic Ketoacidosis (FLUID) Trial change our perspective? Pediatr Diabetes.
2. I lag LL, Kronick S, Ernst RD, Grondin L. Alaniz C. Liu L. Herman WH . Impact of a critical pathway on
2019;20:10–14. https://doi.org/10.1111/pedi.12795
inpatient management of diabetic ketoacidosis. Diabetes Research and Clinical Practice.
2003:62;23‐32.
• PECARN DKA FLUID Study Group. Clinical Trial of Fluid Infusion Rates for Pediatric Diabetic
3. Bull SY, Douglas IS, Foster M , Albert RK. Mandatory protocol for treating adult patients with Ketoacidosis. N Engl J Med. 2018 June 14; 378(24): 2275–2287.
diabetic ketoacidosis decreases intensive care unit and hospital lengths of stay: results of a doi:10.1056/NEJMoa1716816
nonrandomized trial. Critical Care Medicine. 2007:35;4 I‐46
• Wolfsdorf JI, Glaser N, Agus M, et al.ISPAD Clinical Practice Consensus Guidelines 2018:
4. Dunger DB, Sperling MA , Acerini CL, etal. European Society for Paediatric Endocrinology/ Lawson Diabeticketoacidosis and the hyperglycemic hyperosmolar state.Pediatr Diabetes.
Wilkins Pediatric Endocrine Society Consensus Statement on Diabetic Ketoacidosis i n Children and 2018;19(Suppl. 27):155–177. https://doi.org/10.1111/pedi.12701
Adolescents. Pediatrics 2004; 113;e 133‐e 140.
5. Felner EI, White PC. Improving Management of Diabetic Ketoacidosis in Children. Pediatrics
2001:108; 735.
6. Wolfsdorf J, Glaser N, Sperling, M. Diabetic Ketoacidosis i n I nfants, Children, and Adolescents.
Diabetes Care 2006;29; 1 150‐1 158.
7. Joseph Wolfsdorf, Maria E Craig, Denis Daneman, David Dunger, Julie Edge, WR Warren Lee,
Arlan Rosenbloom, Mark A Sperling, Ragnar Hanas. Published in Pediatric Diabetes 2009(Suppl
12);10:118‐133. (International Society for Pediatric and Adolescent Diabetes Clinical Practice
Consensus Guidelines chapter 10).
8. Modified with permission from: Muir AB, Quisling RG, Yang MC, Rosenbloom AL. Cerebral
edema in childhood diabetic ketoacidosis: natural history, radiographic findings, and early
identification. Diabetes Care 2004; 27:1541. Copyright ©2004 The American Diabetes
Association.
Thank you!
• Questions
• Contact info
• AMO278@uky.edu
246/15/2019
Re‐examining theories about CE cause
• Elevated urea nitrogen levels (suggesting greater dehydration) and hypocapnia,
both with the potential to decrease cerebral perfusion, have been associated with
risk of brain injury in several well‐controlled studies
• Elevated levels of inflammatory mediators during DKA have been documented in
both human and animal studies, and findings in studies by same group document
patterns of inflammation consistent with those observed in ischemia/ reperfusion
injury
• Cerebral injury may be more common than previously thought; clinically apparent
cerebral injury may depend on severity of DKA at presentation
• Rate and composition of IV fluids may not be relevant to risk of cerebral injury
Poor outcome factors‐
• Risk factors for death or survival in a vegetative state were identified in a
retrospective multicenter study of 61 children
• Elevated blood urea nitrogen at the time of initial presentation
• Intubation with aggressive hyperventilation (targeting a partial pressure of carbon dioxide
[pCO ] of less than 22 mmHg)
• Severe neurologic compromise at diagnosis of cerebral injury (all patients who either died
or survived in a persistent vegetative state had Glasgow Coma Scale [GCS] scores ≤7 when
cerebral injury was diagnosed)
256/15/2019
The PECARN FLUID Trial found no
significant differences
New since 2018‐ between study arms in either mental status
changes (assessed by GCS
and digit span scores) during DKA
treatment, clinical diagnoses of
brain injury, or cognitive testing scores at
follow‐up
In plain terms:
• Fast administration rate of fluids= 2X maintenance for initial 12 hours, then 1.5
maintenance over next 24 hours (given after 20 cc/kg/NS bolus)
• NS vs ½ NS to replace deficit
• Slow administration of fluids= 1.5 maintenance for 48 hours duration of IV fluids (given
after a 10 cc/kg bolus)
• NS vs ½ NS to replace deficit
• No difference in GCS outcomes; brain injury; or short term memory after DKA episode
• Children with severe DKA who were rehydrated at a faster rate improved their short term
memory sooner than those who were rehydrated at the slower rate (not significant).
266/15/2019
Fluids‐ modern take
• In summary, the PECARN FLUID Trial provided the first high‐quality data
investigating the effects of fluid infusion rates and NaCl content on neurological
outcomes of DKA in children. The FLUID Trial data suggest that a range of fluid
infusion protocols can be used safely in children with DKA and intravenous fluids
should not be restricted unnecessarily due to concerns about causing brain
injuries. Children with DKA should receive fluid resuscitation similar to children
with other conditions involving similar degrees of dehydration.
27You can also read

















































