Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Thank you for viewing this presentation.
We would like to remind you that this
material is the property of the author.
It is provided to you by the ERS for your
personal use only, as submitted by the
author.
2016 by the authorASTHMA AND SLEEP-DISORDERED
BREATHING IN CHILDREN AND ADULTS
Kristie R Ross, MD, MS
Associate Professor of Pediatrics
Case Western Reserve University/Rainbow Babies and Children’s
Hospital
Cleveland, OH, USA
September 6, 2016Conflict of interest disclosure I have no real or perceived conflicts of interest that relate to this presentation. Affiliation / Financial interest Commercial Company Grants/research support: No relevant commercial grant unding; NIH funding for clinical trial for paediatric mild SDB Honoraria or consultation fees: none Participation in a company sponsored bureau: none Stock shareholder: none Spouse / partner: none Other support / potential conflict of interest: none This event is accredited for CME credits by EBAP and EACCME and speakers are required to disclose their potential conflict of interest. The intent of this disclosure is not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial products or services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remains for audience members to determine whether the speaker’s interests, or relationships may influence the presentation. The ERS does not view the existence of these interests or commitments as necessarily implying bias or decreasing the value of the speaker’s presentation. Drug or device advertisement is forbidden.
LEARNING OBJECTIVES 1. State the epidemiology the bidirectional epidemiologic relationship between the asthma and sleep disordered breathing. 2. Describe the proposed mechanisms linking asthma and sleep disordered breathing. 3. Apply evidence to personalize management of paediatric and adult patients with both conditions.
EPIDEMIOLOGY- ASTHMA
• Global prevalence • Risk factors / disease
– Adults and children 1-18% modifiers continued
– Rates in urban areas in – Allergen sensitization
children reported to be as and exposure
high as 25% – Infections / microbiome
• Risk factors / disease – Pollution
modifiers – Smoke exposure
– Genetic – Occupational exposures
– Obesity – Diet
– Demographics: Sex, race – GERD
– Neighborhood level factorsEPIDEMIOLOGY – SLEEP DISORDERED BREATHING
• Global prevalence • Risk factors / disease
– Adults 2-4% modifiers continued
– Children 1-4% – Social factors /
neighborhood level
exposures
• Risk factors / disease – Atopic disease
modifiers – Metabolic disease
– Genetic
– Neuromuscular disease
– Craniofacial structures
– Pollution
– Obesity
– Smoke exposure
– Demographics: Sex, race
– GERDHETEROGENEITY OF DISEASE • Asthma and sleep disordered breathing are heterogeneous conditions • Subgroups (phenotypes) defined by observable clinical, pathologic, physiologic characteristics • Endotypes refer to phenotypes with a specific underlying mechanism identified • Non-biased analytic approaches to define clusters in both disease • Progress in defining asthma phenotypes and endotypes further along than OSA • Relationship between phenotypes/endotypes and treatment responses has been largely disappointing in asthma to date
.
EPIDEMIOLOGY
In populations with asthma:
• ~2 fold increase in risk (cross sectional) for OSA/SDB in adults1-6 and
children7-10
• Relationship stronger with
– Comorbid rhinitis11
– More severe or difficult to control asthma12-14
– GERD3
– Female sex3, 16
– Use of ICS3
– Obesity9,18
• Increased risk of incident OSA19
• Dose dependent duration of asthma
– Strongest for symptomatic OSA RR 2.72 (95% CI 1.26-5.89)EPIDEMIOLOGY In populations with OSA/SDB: • Wide range of reported asthma prevalence in adults – No increase 4%15 – ~ 2 fold increase16, 20 – Up to ~ 7 fold increase in one study17 • Asthma rates ~ 30% in large retrospective study of children undergoing AT for SDB20 and in only RCT of AT for OSA21
EPIDEMIOLOGY
• Conflicting information about relationship between asthma and
OSA severity
– Asthma did not predict higher AHI in CHAT study21
– Poorly controlled asthma was associated with higher AHI in a smaller
prospective study of urban children22Why should we discuss the interaction?
OSA adversely effects asthma severity, control, and QOL
• Asthma severity in children23
– Cohort of 108 children followed in a tertiary care center
– SDB conferred 3.62 fold increase (95% CI 1.26-10.40) in risk of poorly
controlled asthma after one year of guidelines based treatment
• Asthma control in adults24
– 472 adults with asthma followed in tertiary asthma care program
– High OSA risk defined by questionnaire, asthma control by ACQ
– High OSA risk associated with 2.87 (1.54-5.32) fold increased odds of
poor asthma control (controlled for obesity, GERD, demographics, other
co-morbidities)Why should we discuss the interaction?
• OSA associated with increased asthma symptom burden in
severe and non severe asthma5
– Severe Asthma Research Program
• Severe asthma
• Non severe asthma
• Healthy controls (add on study)
– Severe and non severe asthma subjects higher risk for OSA by
questionnaire compared with controls
– High OSA risk by questionnaire associated with more symptoms
(day and night), quick relief medication use, health care
utilizationWhy should we discuss the interaction?
OSA adversely effects asthma severity, control, and QOL
• Asthma exacerbations25
– Exacerbator phenotype in a difficult to treat asthma program had 3.4
fold increased odds of OSA (95% CI 1.2-10.4).
• Older adults26
– OSA was only independent predictor of severe asthma in adults 60-75y
– Relationship in older adults (OR 6.67) much stronger than younger (OR
2.16)
• Inflammation5
– SARP participants with high OSA risk higher PMNs in induced sputumMechanisms • Physiologic effects • Immunologic/inflammatory • Intermittent hypoxemia/ROS • Rhinitis • Obesity • GERD • Treatment effects of corticosteroids • Sleep fragmentation
PHYSIOLOGIC INTERACTIONS
Reduced tracheal tug
increased upper airway
Increased resistance resistance27
OSA
load31 Interdependence of
inspiratory and expiratory
Vagal mediated flow resistance28
bronchoconstriction49
Bronchocontriction
Exacerbation of sleep reduction in pharynx cross
induced FRC reductions sectional area49
increased resistance32
ASTHMA Sleep disruption effects on
upper airway muscle tone30INFLAMMATION AND OXIDATIVE STRESS
Local inflammation
Neutrophils, NFKB,
cysteinyl leukotrienes33-36 OSA Inflammatory
spillover from
Intermittent hypoxemia rhinosinusitis
-neutrophilic inflammation
-vagal
bronchoconstriction37-39 Chronic low grade
inflammationforce
Systemic inflammation ASTHMA generation properties of UA41
CRP, TNF-a, NFKB,
cysteinyl
leukotrienes34,40OTHER INTERACTIONS
Leptin / adipokines44 GERD induced upper
OSA airway changes42
GERD induced Additive effects of
bronchoconstriction, smoking/pollution on upper
respiratory epithelium airway collapsibility and
damage42 inflammation
ASTHMA Treatment effects of
Sleep disruption30,32 steroids on UA tone
and calibre42,43SHARED RISK FACTORS • Central obesity phenotype associated with greatest risk for both OSA and asthma • OSA induced intermittent hypoxemia leptin-ghrelin hormonal changes – Exacerbates further weight gain – Pro-inflammatory response (systemic and airway) • Metabolic abnormalities (insulin resistance) • GERD
CASE PRESENTATION -1 • 2 year with autistic spectrum disorder, speech delay, evaluated for chronic cough • Cough improved on low dose inhaled corticosteroids used for about 4 months then stopped • Snoring/restless sleep/choking/gasping started at age 3 • Snoring/gasping worsened during that time • PSG showed mild obstructive sleep disordered breathing – Technical challenges – oAHI around 3 (no nasal pressure signal) • Adenotonsillectomy performed at age 3 ½ • Snoring resolved, significant progression in language
CASE PRESENTATION -1 • Returned to pulm clinic about 6 months after AT • Last visit ~ 1 year before – 4 unscheduled primary care doctor visits for wheezing – Albuterol use for 5-7 days each episode – Oral corticosteroids during 3 episodes, low dose ICS restarted – Last episode 1 month prior to surgery • No significant exacerbations since surgery • 2 “colds” in the winter without significant lower resp tract symptoms • “Can we stop ICS?”
ADENOTONSILLECTOMY IN CHILDREN WITH
ASTHMA
• Adenotonsillectomy is first line treatment in children with
OSAS who are surgical candidates
• Asthma was a risk factor for incomplete response to AT in non-
obese children in retrospective study44
• No RCT data on asthma outcomes in AT
– CHAT study did not collect this data
– 18 asthma AE’s in watchful waiting vs 3 in early AT group21ADENOTONSILLECTOMY IN CHILDREN WITH ASTHMA
35 had AT +
58 (43%) follow up data
OSA + 23 (48% ) ??
135 poorly controlled 92 had
asthmatics (3y, single center)45 PSG 34 (25%) 24 had follow
OSA - up data
10 (30%) ???
43 (32%) ?? 76 (56%)
???
OSA + with AT and fu No OSA with f/u
Pre AT Post AT p Pre PSG Post PSG p
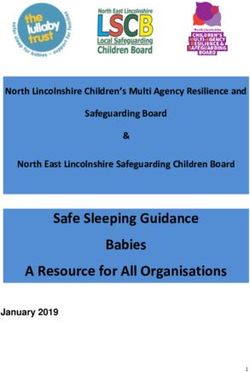
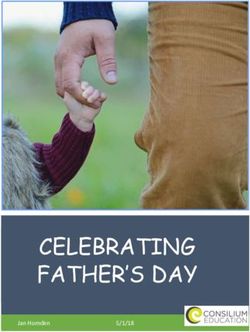
Asthma exacerbations/yr 4.1 + 1.3 1.8 + 1.4ADENOTONSILLECTOMY IN CHILDREN WITH ASTHMA MarketScan database of more than 25 M US privately insured children from 2003-2010 queried46 • 13,506 cases identified out of 51,794 possibles – Asthma diagnosis – AT procedure code – 1 year pre and 1 year post data • 27,012 controls (greedy selection, 2:1 match) out of 932,606 – Asthma diagnosis – No AT procedure code – 1 year pre and 1 year post data • Mean age 7 ½ years, 55% boys
ADENOTONSILLECTOMY IN CHILDREN WITH ASTHMA
Percent reduction in second year46 • Driven by children < 8y
• Similar reductions in
AT + AT -
coding for
0
• Wheezing
-5
• Bronchospasm
-10 • Continuous
-15 albuterol
-20 • Reductions in filling
-25 • Bronchodilators
-30
• ICS
• LTRAs
-35
• Oral corticosteroids
-40
Acute exacerbation Status asthmaticusADENOTONSILLECTOMY IN CHILDREN WITH ASTHMA
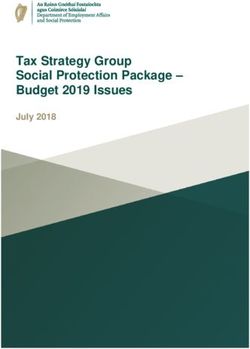
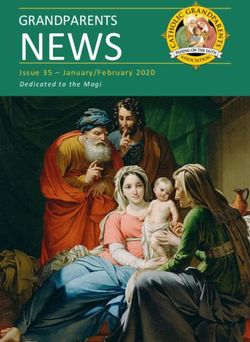
Health insurance database query47 Use of respiratory
8 medications
• Represents ~40% of Belgian
7
population
6
• 11114 children 0-15 y who
Number of boxes
5
underwent tonsillecomty (+/- 4
adenoidectomy) over a 21 3
month period
2
• 1 year pre and 1 year post health 1
data 0
• 4654 used respiratory Pre Post Pre Post
medications in year 1, mostADENOTONSILLECTOMY AND ASTHMA • Current prospective multi-centre randomized controlled trial • Children with mild obstructive SDB single blind allocation: – Watchful waiting – Early adenotonsillectomy • Co-primary outcomes are behavioral tests after 1 year of follow up • Secondary outcomes include asthma health care utilization, severity using composite score
CASE PRESENTATION -1
• Low dose ICS stopped 1 year ago
• Use of short acting bronchodilators on 3 occasions since then
with colds
– Duration less than 1 day for each episode
• No exercise limitation
• No sleep disturbance
• Continues to make progress in therapies
• No oral steroidsCASE PRESENTATION 2
• 29 year old presenting for asthma management
• Frequent asthma admissions between ages 4 and 10
• Period of asthma “remission” ages 12 to early 20s
• Recurrence of symptoms as a young adult
• Exercise induced wheezing/tightness frequently
• Using quick relief inhaler several times per week
• 2 courses of oral steroids in the last 6 months (ED visits)
• Lung function: moderate obstruction with reveresibility,
exhaled NO 40CASE PRESENTATION - 2 • History of loud snoring as a young child – Improved with adenotonsillectomy at ~ age 8 • Snoring recurred as a teen, described as about as loud as talking • Nightly sleep disturbance – Primarily describes cough • Accompanied by substantial weight gain • Recent elevated BP readings and “pre-diabetes”
CASE PRESENTATION -2
Severe OSA: AHI 46, SpO2 nadir 79%, SpO2 below 90 for 6% sleep time
OSA controlled with modest CPAP pressuresIMPACT OF CPAP ON ASTHMA
• Initial report of treatment of patients with severe asthma and
OSA with CPAP in 1988 (uncontrolled series, n=9, 1 female)48
– Asthma was severe and uncontrolled despite oral corticosteroids
– AHI was 15 or less in 6 out of 9
– BMIs 25-36
– Concern that CPAP would worsen asthma did not hold up
– During 2 weeks of CPAP compared with 2 weeks pre and post:
• Improved PEFR
• Reduced day and night asthma symptoms
• Reduced bronchodilator use (twice per night to 0 per night)IMPACT OF CPAP ON ASTHMA
• Uncontrolled series of 10 adult and 5 adolescent males (1988)49
– Reduction in nocturnal asthma attacks
• Effect of CPAP on lung function may be different in those with
and without OLD50
– 3 groups: asthma (n=15), COPD (n=13), no OLD (n=22)
– Spirometry and ABG done after ~ 1 yr CPAP
– Improved gas exchange overall
– Asthma and COPD: No change in lung function
– No OLD: worsening FEV1, FEV1/FVC, more bronchial hyper-
responsiveness after treatmentIMPACT OF CPAP ON ASTHMA
• Uncontrolled study of 43 adults with nocturnal
asthma despite optimal medical management51
– 19 adults found to have moderate to severe OSAS (mean AHI 44
+ 50)
– Treated with CPAP for 2 months – 16 tolerated and met
adherence crit
– Nighttime asthma symptoms improved in 10 out of 16 (sig)
– No change in pulmonary function measuresIMPACT OF CPAP ON ASTHMA
• Uncontrolled series of 20 adults with OSA and
asthma52
– 33 eligible subjects with well controlled asthma (1/2 on no
controller) and newly diagnosed moderate to severe OSA (mean
AHI 48)
– 6 ineligible (poor asthma control), 7 withdrawn (adherence/other)
– Improvement in asthma and OSA related QOL after 6 weeks of
CPAP
– No change in lung functionCPAP AND CHRONIC COUGH • Retrospective study in a community based practice53 – OSA common (44%) in isolated chronic cough – Cough improved with OSA treatment (93%) • Follow up prospective study of CPAP use by same group54 – 19 out of 28 had PSG proven OSA – Female predominance, most obese, GERD co-morbid in many – Cough questionnaire improved with CPAP treatment (p=0.002)
CASE PRESENTATION - 3 • 10 year old admitted in acute respiratory failure requiring non invasive ventilation for 2 days • History of chronic cough, exercise induced wheezing/dyspnea • Pulmonary function showed moderate obstruction with reversibility • Sensitized to multiple aeroallergens • Diagnosed with uncontrolled asthma based on history, testing, and severe exacerbation • Prescribed long acting beta agonist/inhaled corticosteroid combination
CASE PRESENTATION - 3 • Readmitted 4 months later with rapid onset dyspnea, wheezing, chest tightness • RML/RLL atelectasis • Admitted to ICU for non invasive ventilation for 2 days • Improved, discharged on LABA/ICS combo therapy • Follow up 4 weeks later – rare symptoms – lung function mild obstruction – CXR improved
CASE PRESENTATION - 3 • Readmitted 4 months later with rapid onset dyspnea, wheezing, chest tightness, hypoxemia • RML/RLL atelectasis recurred • Admitted to ICU for non invasive ventilation for 2 days • Additional testing not revealing – Bronchoscopy/BAL – Sweat testing – Immune testing • Improved, discharged on LABA/ICS combo therapy and airway clearance
CASE PRESENTATION - 3 • Readmitted 4 weeks later with rapid onset dyspnea, wheezing, chest tightness, hypoxemia • RML/RLL atelectasis recurred • Admitted to asthma unit • CPAP started empirically • Improved, discharged on LABA/ICS combo therapy, airway clearance, and CPAP auto 6-12 cm H2O • Subsequent PSG showed mild OSA with AHI 5, SpO2 nadir 89% • Should we continue CPAP?
CASE PRESENTATION - 3 • Ambulatory follow up approximately every 6 months over the last 2 years • Uses CPAP reasonably well – Use on ~75% of nights – Average use of 7 hours – Residual AHI 0.8 • Fill rates of LABA/ICS still spotty • Last spirometry was normal • No admissions or oral steroids since May 2014
CASE PRESENTATION - 4 • 14 year old evaluated for worsening asthma • PMH sig for – Epilepsy – Short stature – Developmental delay (mild) – Delayed puberty • Last visit to asthma clinic 3 years earlier – Normal lung function – Asthma mild and controlled on low dose ICS
CASE PRESENTATION - 4 • 6 months prior to visit he had foot surgery complicated by osteomyelitis (unable to ambulate for several months) • Significant and progressive dyspnea developed • Rapid weight gain (BMI went from 28 to 33) • Decline in lung function • Increasing seizure frequency • Snoring and witnessed apneas noted along with daytime symptoms – Not clear from history if they were related to nocturnal seizures • Chest CT, PSG ordered and started on ICS/LABA therapy
CASE PRESENTATION - 4 • Follow up 2 months later • Some improvement in shortness of breath and cough on ICS/LABA but significant dyspnea still present • Normal chest CT • Modest improvement in FEV1 from 70 to 76% predicted • Confirmed technique, filling prescription • Snoring, daytime sleepiness, trouble concentrating unchanged
CASE PRESENTATION - 4
?
Mild OSA: AHI 5, SpO2 nadir 92%, mild hypercapniaCASE PRESENTATION - 4
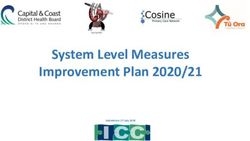
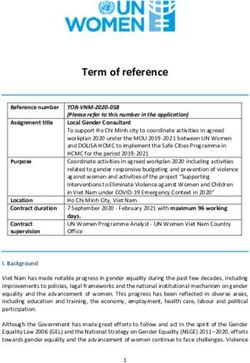
• CPAP titration done and CPAP started Feb 2014
• Sleepiness, seizures, dyspnea, and lung function improved
FEV1 BMI
110 35
100 30
90
25
80
20
70
60 15
13.nov. 14.janv. 14.avr. 15.janv. nov..13 janv..14 avr..14 janv..15Conclusion • Asthma and Obstructive Sleep Disordered Breathing are prevalent conditions • Physiologic, inflammatory, metabolic, and shared environmental and co-morbidities may explain the interaction between them • Heterogeneity of both diseases makes it difficult to study • Personalized approach considering physiology, phenotype, and endotype may be helpful
DISCUSSION
REFERENCES 1. Teodorescu et al, J Asthma 2012; 49:620-8; 2. Shen T-C PLoS ONE 2015;10(6):e0128461; 3. Teodorescu M et al; Chest 2009; 135:1125-32; 4. Jonassen TM et al, Clin Respir J. 2016 Mar 7. 5. Teodorescu M et al, JACI in Practice 2015; 3:566-75 6. Auckley D et al, Sleep Med 2008; 9:494-99. 7. Brockmann PE et al, Sleep Med Rev 2014; 18:393-7; 8. Greenberg-Dotan S et al, Sleep. 2007;30:1173-80; 9. Redline S Am J Respir Crit Care Med. 1999;159:1527-32; 10. Ross KR Peds Pulm 2010 11. Braido F, Respir Care 2014; 59:1851-6. 12. Byun MK Yonsei Med J 2013; 54:942-8. 13. Julien JY JACI 2009; 124:371-6. 14. Guven SF et al, Asian Pac J Allergy Immunol 2014; 32:153-9 15. Pinto JA et al, Int Arch Otorhinolaryngol. 2016; 20:145-50;
16. Greenberg-Dotan S et al, Sleep Breath. 2014; 18:69-75; 17. Alharbi M et al, Prim Care Respir J 2009; 18:328-30; 18. Sulit LG et al, Am J Respir Crit Care Med. 2005;17:659-64 19.Teodorescu M et al; JAMA 2015:156-64. 20.Bhattacharyya N et al, Otolaryngol Head Neck Surg. 2012; 147:1154-7; 21. Marcus CL, NEJM 2013; 368(25):2366-2376 22. Ramagopal M et al, J Asthma. 2009; 46:895-9, 23. Ross KR et al, J Peds 2012; 160:736-42 24. Teodorescu M et al, Chest 2010:138:543-50 25. Ten Brinke A et al, Eur Resp J 2005; 26:812-8. 26. Teodorescu M et al, Sleep Disord; 2013:251567 27. Van de Graaff WB. J Appl Physiol. 1988;65(5):2124-2131. 28. Tamisier R et al. Sleep. 2004;27(2):240-248 29. Guilleminault C et al. Eur Respir J. 1988;1(10):902-907
30. Leiter JC, Am Rev Respir Dis. 1985;132(6):1242-1245 31. Bijaoui EL, Am J Respir Crit Care Med. 2002;165(8):1055-1061 32. Ballard RD, J Appl Physiol. 1990;68(5):2034-2041 33. Goldbart AD, Chest. 2004;126(1):13-18. 34. Israel LP, Sleep. 2013;36(12):1947-1955. 35. Salerno FG, Respir Med. 2004;98(1):25-28. 36. Boyd JH, Am J Respir Crit Care Med. 2004;170(5):541-546. 37. Dewan NA Chest. 2015;147(1):266-274. 38. Denjean A, Respir Physiol. 1991;83(2):201-210 39. Denjean A,. Am Rev Respir Dis. 1988;138(4):789-793. 40. Nadeem R, J Clin Sleep Med. 2013;9(10):1003-1012. 41. Reid MB. Am J Respir Crit Care Med. 2002; 166(4):479-484. 42. Kasasbeh A Sleep Med Rev 2007; 11:47-58 43. Yigla M. J Asthma. 2003;40(8):865-871.
44. Bhattacharjee R, Am J Respir Crit Care Med. 2010;182(5):676-683 45. Kheirandish-Gozal L,. Pediatr Pulmonol. 2011;46(9):913-918 46. Bhattacharjee R, PLoS Med. 2014;11(11):e1001753. 47. Piessens PInt J Pediatr Otorhinolaryngol. 2012;76(6):906-910. 48. Chan CS, Am Rev Respir Dis. 1988;137(6):1502-1504. 49. Guilleminault C, Eur Respir J. 1988;1(10):902-907. 50. Bonay M, Respir Med. 2003;97(7):830-834. 51. Ciftci TU, Respir Med. 2005;99(5):529-534. 52. Lafond C, Eur Respir J. 2007;29(2):307-311. 53. Sundar KM, Cough. 2010;6(1):2. 54. Sundar KM. Cough. 2013;9(1):19.
You can also read