Racial Healing and Achieving Health Equity in the United States
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Embargoed
ISSUE BRIEF
until Tuesday,
December 17
at 10:00 AM ET
Racial Healing and Achieving Health
Equity in the United States
“Of all the forms of inequality, injustice in health care is the most shocking
and inhumane.”
-- Rev. Martin L. King, Jr.
The Truth, Racial Healing & Transformation promote positive and lasting change across
(TRHT) effort was created by the W.K. issues — including to:
Kellogg Foundation as a national and
1. Find ways to reinforce and honor our
community-based process to plan for and
common humanity and create space to
bring about transformational and sustainable
celebrate the distinct differences that
change and to address the historic and
make our communities vibrant;
contemporary effects of racism.
2. Acknowledge that there are still deep
Among the many aspects of TRHT is racial divisions in America that must be
the need to address serious racial and overcome and healed; and
ethnic health inequities — and the causes
that contribute to them. Good health is 3. Commit to engage people from all racial, eth-
essential to ensuring everyone is able to live nic, religious and identity groups in genuine
a high-quality life, be engaged with their efforts to increase understanding, communi-
families, communities and workplaces, and cation, caring and respect for one another.1
have the opportunity to flourish and thrive This issue brief was developed to help identify
in everything they do. TRHT’s National and acknowledge health inequities, influencing
Day of Racial Healing identifies key steps factors and policy recommendations that can
that will help take collective action to help the nation achieve health equity.
“Health equity means that everyone has a fair and just opportunity to be
as healthy as possible. This requires removing obstacles to health such as
JANUARY 2018
poverty, discrimination, and their consequences, including powerlessness
and lack of access to good jobs with fair pay, quality education and
housing, safe environments and health care.”2
REACHING FOR
Health Equity
Reducing health disparities brings us closer to reaching health equity. The programs
below are examples of how addressing disparities can advance health equity.
T HEALT T HEALT
ES ES
H
H
B
B
PO PO
SSIBLE SSIBLE
Future
Strategies
Case management and home visits by Client and provider reminders
community health workers decreased Ongoing and patient navigators increased
asthma-related hospitalizations Efforts colorectal cancer screening rates
Expanded vaccination recommendations Personalized counseling reduced Programs and policies supporting
eliminated some disparities in HIV risk behaviors better neighborhood conditions
Hepatitis A disease reduced violence
Curriculum for living well with a Tribally driven efforts to reclaim Lay health advisors reduced HIV
disability improved quality of life traditional food systems facilitated risk behaviors
dialogue about health
PROGRAMS
POPULATIONS
Black and Racial/ethnic People living Men who have American Indian Low income High risk Hispanic and Latino
Hispanic children minority groups with disabilities sex with men and Alaska Native populations and communities immigrant men
populations Alaska Natives
HEALTH EQUITY is when HEALTH DISPARITIES are differences in health outcomes and
everyone has the opportunity to be their causes among groups of people.
as healthy as possible.
EXAMPLE: African American children are more likely to die
from asthma compared to non-Hispanic White children.
2 TFAH • healthyamericans.org
Learn more about these programs at:
Existing Inequities
The causes of health inequities are multifaceted and often intertwined with lower socioeconomic
status, differential access to opportunities and other factors that influence health, such as quality
healthcare, income, education, housing, transportation and others, sometimes referred to as the
“social determinants of health.”
Health inequities have a high economic housing provide significant opportunities l Infants born to Black women are 1.5 to
cost. A study by the Urban Institute found to be healthier.12 almost 3 times more likely to die than
that for a set of preventable diseases (dia- l ow-income neighborhoods are less
L infants born to women of other
betes, heart disease, high blood pressure, likely to have places where children can races/ethnicities regardless of
renal disease and stroke), differences be physically active or have access to education level.25 American Indian and
in the rates of diseases among Blacks, fully-stocked supermarkets with healthy, Alaska Native infants die from Sudden
Hispanics and Whites cost the healthcare affordable foods — contributing Infant Death Syndrome (SIDS) at
system $23.9 billion annually.3 By 2050, to higher rates of obesity and poor about twice the rate of White infants. 26
this is expected to double to $50 billion a nutrition in these communities.13, 14, 15 l Asthma rates for Black children grew
year.4 Eliminating health inequities could by 50 percent between 2001 and
l ow-income and minority communities
L
lead to reduced medical expenditures 2009, while the overall asthma rates
also experience higher air pollution,
of $54 to $61 billion a year, and recover increased 15 percent.27 Differences in
which affects respiratory and cardiovas-
around $13 billion annually due to work asthma rates between Black and White
cular health as well as birth outcomes.16
lost by illness and around $240 billion per children reached a peak in 2011 (with
year due to premature deaths (2003-2006 Examples of some health inequities Black children twice as likely as White
spending).5,6 According to the U.S. Cen- include: children to have asthma).28 And,
ters for Disease Control and Prevention l American Indians and Alaska Natives asthma-related hospitalizations and
(CDC), the rate of preventable hospital- are twice as likely to have diabetes deaths are more than twice as high
izations for Blacks is almost double that of as Whites, and diabetes rates among among Blacks as Whites.29, 30
Whites — which contributes to over a half Blacks and Hispanics are more than l Blacks, Hispanics, and American Indians
million hospitalizations and $3.7 billion in 1.5 times higher than for Whites.17 and Alaska Natives received worse
hospitalization costs annually.7
l Blacks are seven to nine times more care than Whites for about 40 percent
The following are a number of examples likely to die from HIV, and are six times of quality measures, according to the
highlighting factors that contribute to more likely to die from homicide.18 2015 National Healthcare Quality and
inequity: l Black children have the highest rate of Disparities Report.31 Blacks and Hispanics
l lacks and Latinos have lower median
B lead poisoning (5.6 percent).19 were more likely than Whites to report
household incomes than Whites and poor communication from healthcare
l Blacks have the highest death rate
are more likely to live in poverty.8 providers. Some examples of implicit
and shortest survival for most cancers
bias in healthcare identified by The
l lack men earned 70 cents for every
B of any racial and ethnic group in the
Joint Commission, Division of Health
dollar earned by White men in 2014 United States.20
Care Improvement include: non-White
and Hispanic men earned 60 cents on l lack women with breast cancer are 40
B patients receive fewer cardiovascular
the dollar.9, 10 percent more likely to die than White interventions and renal transplants;
l People living in neighborhoods with high women with breast cancer, despite non-White patients are less likely to be
levels of poverty have a higher risk of less similar incidence rates of the disease.21, 22 prescribed pain medications; Black men
healthy behaviors —such as smoking, l lack men are about twice as likely to
B are less likely to receive chemotherapy
physical inactivity or poor nutrition— die from prostate cancer as Whites. 23 and radiation therapy for prostate
which are related to inequities in the cancer; and patients of color are more
l Hispanic women are more than 1.5
physical and social environment.11 likely to be blamed for being too passive
times as likely to have cervical cancer
Access to safe neighborhoods and about their healthcare.32
as Whites. 24
amenities, supermarkets and quality
TFAH • healthyamericans.org 3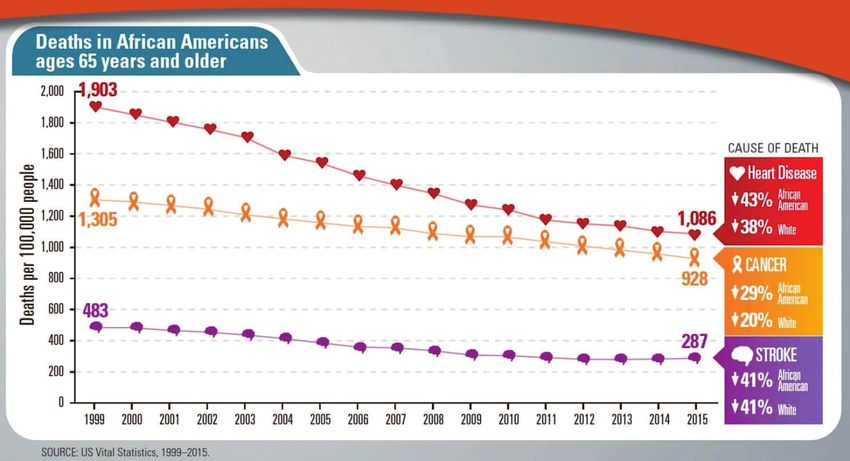
INEQUITIES IN LIFE EXPECTANCY
Life expectancy rates vary by as much as As of 2014, five counties had life comprised of more than 75 percent
20 years between counties in the United expectancies below 70 years (the lowest non-Hispanic White.
States.33 Race/ethnicity, socioeconomics at 66.8 years) — with four of those
l Of the 50 counties with the lowest
and healthcare explained the differences counties having high American Indian
life expectancy rates (72.6 years and
by 74 percent, 60 percent and 27 populations. Two counties had life
lower), seven had majority American
percent respectively. expectancies above 86 years.
Indian populations (with five above 79
l Of the 50 counties with the highest life percent) and 18 had majority Black
expectancy rates (82 years and above), populations (with nine at 70 percent
35 of them had a population that was or above).
THE BLACK WHITE MORTALITY GAP
Currently, on average, the life expectancy
for Black men is 4.5 years shorter than
for White men; and 3 years shorter for
Black women than White women.34
The mortality gap among Blacks and Whites
has narrowed by around half — from 33
percent to 16 percent — over the past 17
years. Blacks experienced a 25 percent
decline in overall death rates during this
time compared to a 14 percent decrease
among Whites.35
Still, Blacks are more likely to die at
relatively younger ages from a wide range
of causes — including that Blacks ages
18 to 49 were nearly twice as likely to die
from diabetes, heart disease and stroke
than Whites. However, Blacks ages 65 and
older have a lower death rate than Whites
ages 65 and older from heart disease,
cancer and stroke. CDC attributes the
consequences of psychosocial, economic
and environmental stressors are the key
contributors to these disparities.
4 TFAH • healthyamericans.org
Age-adjusted death rates for selected populations: United States, 2015 and 201636
1,200 2015 2016
21,081.2
1,070.1
1,000
Deaths per 100,000 U.S. standard population
881.3 879.5
800
733.1 1
728.8 731.0 734.1
644.1 1637.2 628.9 631.8
600
438.3 436.4
400
200
0
To tal Black male Black female White male White female Male Female
Non-Hispanic Hispanic
1
Statistically significant decrease in age-adjusted death rate from 2015 to 2016 (p < 0.05).
2
Statistically significant increase in age-adjusted death rate from 2015 to 2016 (p < 0.05).
NOTE: Access data table for Figure 2 at: https://www.cdc.gov/nchs/data/databriefs/db293_table.pdf#2
.
SOURCE: NCHS,
Source: NCHS, National
NationalVitalVital
Statistics System, System,
Statistics Mortality. Mortality.
AMERICAN INDIAN LIFE EXPECTANCY
Life expectancy for a number of counties
with high American Indian populations
are 20 percent lower than other counties
in the United States.37,38 Much of the
difference is attributed to socioeconomics
and access to healthcare in addition to
race/ethnicity. For instance, Oglala Lakota
County in South Dakota, which includes
the Oglala Sioux Tribe’s reservation, had
the lowest life expectancy in the country
in 2014 — at 66.8 years, and three other
counties with tribal communities were also
among the five lowest for life expectancy
arindambanerjee / Shutterstock.com
rates (Todd County, South Dakota with
overall national rates also increased.
the Rosebud Sioux Tribe; Buffalo County,
For instance, the Oglala Lakota County
South Dakota with the Crow Creek Sioux
average life expectancy increased by 5.4
Tribe; and Sioux County, North Dakota
years during this time, from 61.3 years in
which includes the northern portion of the
1980 to 66.8 years in 2014. However,
Standing Rock Sioux Tribe reservation).
the average life expectancy for those in
Life expectancy rates in nearly all predominantly American Indian counties
counties with tribal communities is 12.5 years shorter than the overall life
increased between 1980 and 2014, as expectancy rate in South Dakota.
TFAH • healthyamericans.org 5
Policy Recommendations
TFAH has issued the following set of and universities, must be taken into
recommendation to help the nation account in this process. Proven,
achieve health equity: effective programs, such as CDC’s
REACH (Racial and Ethnic
l reate strategies to optimize the
C
Approaches to Community Health)
health of all Americans, regardless
should be fully-funded and expanded.
of race, ethnicity, income or where
they live. All levels of government l ollect data on health and related
C
must invest in analyzing needs and equity factors — including social
increasing effective policies and determinants of health — by
programs to address the systematic neighborhood. There should be a
inequities that exist and the factors priority on improving data collection
that contribute to these differences, at a very local level to understand
including poverty, income, racism connections between health status
and environmental factors. These and the factors that impact health to
should include community-driven help identify concerns and inform
approaches, including using place- the development of strategies to
based approaches to target programs, address them. Collecting and
policies and support effectively. reporting data by neighborhood at
a zip code or even more granular
l xpand cross-sector collaborations
E
neighborhood level are essential.
addressing health equity. Improving
equity in health will require supporting l upport Medicaid coverage and
S
and expanding cross-sector efforts to reimbursement of clinical-community
make communities healthy and safe. programs to connect people to
Efforts should engage a wide range of services that can help improve health.
partners, such as schools and businesses, Medicaid should reimburse efforts
to focus on improving health through that support improved health beyond
better access to high-quality education, the doctor’s office — programs such
jobs, housing, transportation and as asthma and diabetes prevention and
economic opportunities.39 care management and community-
based initiatives, can help better
l ully fund and implement health
F
address the root causes that contribute
equity, health promotion and
to inequities.
prevention programs in communities.
Partner with a diverse range of l ommunicate effectively with diverse
C
community members to develop community groups. Federal, state,
and implement health improvement local and tribal officials must design
strategies. Federal, state, local and culturally competent, inclusive
tribal governments must engage and linguistically appropriate
communities in efforts to address communication campaigns that use
both ongoing and emergency health respected, trusted and culturally
threats. The views, concerns and competent messengers to communicate
needs of community stakeholders, their message. Communication
such as volunteer organizations, channels should reflect the media
religious organizations and schools habits of the target audience.
6 TFAH • healthyamericans.org
l rioritize individual and community
P
resiliency in health emergency
preparedness efforts. Federal, state,
local and tribal government officials
must work with communities and
make a concerted effort to address
the needs of low-income, minority and
other vulnerable groups during health
emergencies. Public health leaders
must develop and sustain relationships
with trusted organizations and
stakeholders in diverse communities on
an ongoing basis—including working
to improve the underlying health of
at-risk individuals, sub-population
groups and communities, so these
relationships are in place before a
disaster strikes. Communication and
community engagement must be
ongoing to understand the disparate
needs of various populations.
Linda Parton / Shutterstock.com
l liminate racial and ethnic bias
E l I ncorporate strategies that foster
in healthcare. Policies should community agency—or a community’s
incentivize equity and penalize collective ability and opportunity to
unequal treatment in healthcare, and make purposeful choices—into the
there should be increased support design, implementation and governance
for programs to increase diversity of multi-sector collaborations. Building
in and across health professions. community agency can contribute
Some of The Joint Commission’s to improved community health by
recommendations for combatting yielding a deeper understanding of
implicit bias include: assiduously the challenges and opportunities
practicing evidence-based medicine; influencing a community, and relies
supporting cultural understanding on an asset-based approach to leverage
and avoiding stereotypes; supporting existing community strengths and
the National Standards for Culturally resources. Multi-sector collaborations
and Linguistically Appropriate Services should include dedicated resources for
in Health and Health Care; and fostering and measuring community
supporting techniques that de-bias care, agency. Efforts should maximize and
including through training, perspective- bolster community voice and power as
taking, emotional expression and a means to influencing larger policy-
counter-stereotypical exemplars.40 In and systems-level changes (including
addition, efforts should be increased those within and outside of the
to train more healthcare professionals traditional health sector).
from under-represented populations so
that the workforce reflects the diversity
of the patient population.
TFAH • healthyamericans.org 7
Examples The following examples illustrate several current initiatives
that target the higher rates of preventable injuries, illnesses
of Programs
and deaths. They highlight diverse practices that incorporate
Addressing organizations and individuals from multiple sectors including
Health Equity education, criminal justice and business as well as public health
and healthcare. While every community and effort is unique,
they all share an approach of focusing on equity and inclusive
work at the local community level.
The California Endowment’s Building Healthy Communities
The California Endowment (TCE) created an undocumented; the promotion of healthy
ambitious $1 billion, 10-year project called school environments and altered school
Building Healthy Communities (BHC) in policies such as those related to discipline
2010. Its goal is to improve the health and and suspension; the reform of the justice
well-being of young people in underserved system; and the implementation of multiple
communities by reducing or eliminating local changes that make communities
harmful conditions. It has provided funding safer and more walkable.
to 14 community-based organizations
BHC is noteworthy in its commitment to
across the state to undertake activities
developing long-term relationships with
that were customized to the specific local
specific partners, placing the decision-
conditions but which had the potential
making authority for the usage of the
to affect state policies and practices
grants at the community level and focusing
as well. As a result of its work, BHC
on youth leadership and organizing.
has seen improvements in healthcare
coverage, including for those who were
8 TFAH • healthyamericans.org
Minnesota Public Health Department
The Minnesota Department of Health Triple Aim of Health Equity
prioritized work on health equity. It created
Assess & Influence the Crosswalk to the 7 Foundational Practices
an internal Center for Health Equity and
Policy Context
a Health Equity Advisory and Leadership
(HEAL) Council as part of a broad effort. Lead with an Equity Focus
The Center has awarded scores of grants Use Data to Advance Health
to community agencies including ones Build Partnerships Equity
that identify and address the social and & Community Develop Workforce via
Capacity Implement Health Continuous Learning
economic conditions that contribute to in All Policies
inequities and ones that support the Use & Target Resources
Strategically
improvement of the health status of
groups with poorer health. The Health
Department has taken steps to establish Expand the
an open participatory process for this Strengthen Expand Understanding of
work, including many members of the Community Understanding Health
populations at highest risk of illness, injury Capacity of Health
and preventable deaths on the Advisory
Council and holding statewide meetings to
discuss progress toward health equity.
policies, expanding the understanding state including materials on emergency
It has developed a framework for of health and strengthening community communications, paid sick leave and health
considering the work that is known as capacity. The Health Department has statistics (http://www.health.state.mn.us/
the Triple Aim of Health Equity with three developed a series of reports and resources divs/opi/healthequity/resources/).
components: implementing health in all on the topic for those in and beyond the
Roadmap to Health Equity
The health indicators for the Black nutrition and provide them with healthy
population of Mississippi are significantly foods. It offers a leadership program for
worse than for the White population. Black young students that provides educational
residents live on average 4 years less than lessons in school-work, presentation
Whites and have more deaths from cancer, skills and beneficial eating and exercising
heart disease, HIV and many other chronic practices.
conditions. The Mississippi Roadmap
For adults, the Roadmap runs a Mobile
to Health Equity, Inc., a community-
Farmer’s Market that delivers fresh fruit
based organization in Jackson, is actively
and vegetables to older residents of
engaged in improving those statistics with
geographically isolated housing complexes.
its focus on changing the conditions in the
And it runs a fitness center for adults and
lives of the low-income Black population.
children that is accessible and affordable
It has a strong focus on the health of with minimal membership fees. Support
children by supporting food and nutrition for the Roadmap has been provided
awareness policies within schools. It is by the W. K. Kellogg Foundation. More
responsible for multiple school gardens information on the Roadmap is available at
that are used to teach children about http://mississippiroadmap.org/.
TFAH • healthyamericans.org 9
Colorectal Cancer Screening
Racial and ethnic minority populations
often have lower colorectal cancer
screening rates than White populations
(U.S. White rates were 65 percent
compared to 62 percent, 54 percent and
50 percent rates for Black, American Indian
and Latino populations respectively).41
Specialized outreach and education Colorectal Health
Protect Yourself, Your Family, and Our Community
C
Prote
programs have been shown to be effective
at closing the gap by using multiple targeted
approaches such as patient reminders
The Washington State program utilized pa-
and patient navigators for outreach and
tient care coordinators at community health
assistance. Two examples of such successful
center sites to implement client and provider
efforts are the Alaska Native Tribal Health
telephone and electronic health record re-
Consortium and Washington State’s Breast,
minder systems and to provide staff training
Cervical and Colon Health program.
on the protocols for scheduling of screening.
The Alaska Consortium collaborated with
Colorectal
In both cases, colonoscopy
Protect Yourself,
Health
rates
Your Family, and Our for popula-
Community
C
Prote
regional tribal health organizations to hire tions of color dramatically increased,
patient navigators to do outreach and one- sometimes doubling what they were
on-one patient education and to assist before.42, 43 More information about evi-
with transportation and other barriers to dence-based programs to reduce chronic dis-
accessing appointments. In addition, they eases that disproportionately affect specific
developed an electronic system to send both populations is available at https://www.cdc.
clinician and client informational reminders. gov/chronicdisease/healthequity/index.htm.
Healthy Heartlands
The Healthy Heartlands initiative is an the social determinants of health for low-
eight-state network of public health income communities and communities
professionals and faith-based community of color using a racial health equity lens.
organizers working to reduce health Leaders from across the participating
inequities through democracy building and Midwestern states gather regularly to
policy and system changes.44 The initiative share best practices and advance an
combines the research, institutional action agenda for racial and health equity.
legitimacy and content expertise of public Past efforts have included campaigns to
health leaders with the local voice, power increase employment opportunities for
and engagement capacities of community formerly incarcerated persons, expand
organizers. Through their collaborative access to healthy food and promote free,
actions, the network of interdisciplinary quality early education.
leaders works to identify and address
10 TFAH • healthyamericans.orgRobert Wood Johnson Foundation Culture of Health Sentinel
Communities—Stockton, CA
Located in Northern California, Stockton and community stakeholders to
has long been plagued by crime and improve their city’s safety, education,
poverty. The crime rate in Stockton housing, job creation, and health.
is more than three times the rate in RSSC deploys four outreach workers to
California. And there are high levels of build trust and relationships between
poverty, which are highest among racial community members and government
and ethnic minority communities, where officials, assess community needs
nearly 50 percent of Black residents and appropriately connect residents
and more than 29 percent of Hispanic to available services/supports. Other
residents were living below the federal efforts include a 2014 ¾ cent tax to
poverty level (compared with less than increase the capacity of the police force
17 percent of White residents).45 from 400 officers in 2015 to a goal of
485 by 2017.
Community members and public officials
are collaborating to address these Stockton, CA is one of RWJF’s 30 Sentinel
issues by elevating early intervention Communities chosen to collect, analyze
and education, fostering cross-sector and disseminate community-level data
collaboration, reducing barriers to to provide insight on the best practices
housing and homeownership, and and lessons for improving health and
strengthening integration of health wellbeing. Baseline data was collected
services and systems. In 2015, city in 2016 and future community snapshot
council and community members reports will include more in-depth analysis
created the Reinvent South Stockton and insight on health equity outcomes
Coalition (RSSC) to empower residents and process measures.
TFAH • healthyamericans.org 11Endnotes
1 W.K. Kellogg Foundation. Taking Collective 18 Cunningham TJ, Croft JB, Liu Y, Lu H, Eke PI, 34 N ational Center for Health Statistics. Health,
Action for Racial Healing. http://healourcom- Giles WH. Vital Signs: Racial Disparities in Age- United States, 2015: With Special Feature on
munities.org/ndorh-2018/. Specific Mortality Among Blacks or African Amer- Racial and Ethnic Health Disparities—Table 18.
2 Braveman P, Arkin E, Orleans T, Proctor D, icans — United States, 1999–2015. MMWR Morb Hyattsville, MD: National Center for Health
and Plough A. What Is Health Equity? And Mortal Wkly Rep 2017;66:444–456. DOI: http:// Statistics, 2016
What Difference Does a Definition Make? Princ- dx.doi.org/10.15585/mmwr.mm6617e1. 35 C unningham TJ, Croft JB, Liu Y, Lu H, Eke
eton, NJ: Robert Wood Johnson Foundation, 19 T rust for America’s Health, Blueprint for a PI, Giles WH. Vital Signs: Racial Disparities in
2017. https://www.rwjf.org/content/dam/ Healthier America 2016: Policy Priorities and Age-Specific Mortality Among Blacks or Afri-
farm/reports/issue_briefs/2017/rwjf437343. Recommendations for the Next Administration and can Americans — United States, 1999–2015.
3 Waidmann, TA. Estimating the Cost of Racial Congress (2015) (available at http://tfah.org/ MMWR Morb Mortal Wkly Rep 2017;66:444–
and Ethnic Health Disparities. Washington, assets/files/TFAH-2016-Blueprint-FINAL.pdf) 456. DOI: http://dx.doi.org/10.15585/
DC: Urban Institute, 2009. 20 Cancer Facts and Figures for African Ameri- mmwr.mm6617e1
4 Ibid. cans. In American Cancer Society. http://www. 36 K ochanek KD, Murphy SL, Xu JQ, Arias E.
cancer.org/research/cancerfactsstatistics/ Mortality in the United States, 2016. NCHS Data
5 LaVeist TA, Gaskin D, Richard P. Estimat- cancer-facts-figures-for-african-americans (ac- Brief, no 293. Hyattsville, MD: National Cen-
ing the economic burden of racial health cessed September 2016). http://www.cancer. ter for Health Statistics. 2017.
inequalities in the United States. Int J Health org/research/cancerfactsstatistics/cancer- 37 D wyer-Lindgren L, Bertozzi-Villa A, Stubbs
Serv. 2011;41(2):231-8. facts-figures-for-african-americans RW, Morozoff C, Mackenbach JP, van Lenthe
6 LaVeist TA, Gaskin D, Richard P. The Economic 21 Hunt BR, Whitman S and Hurlbert MS. Increas- FJ, Mokdad AH, Murray CJL. Inequalities
Burden Of Health Inequalities in the United ing Black: White disparities in breast cancer mor- in Life Expectancy Among US Counties,
States. Washington, DC: Joint Center for Po- tality in the 50 largest cities in the United States. 1980 to 2014Temporal Trends and Key Driv-
litical and Economic Studies, n.d. Cancer epidemiology. Apr 30;38(2):118-123, 2014. ers. JAMA Intern Med. 2017;177(7):1003–1011.
7 Centers for Disease Control and Prevention. doi:10.1001/jamainternmed.2017.0918
22 Breast Cancer Rates by Race and Ethnicity. In
CDC Health Disparities and Inequalities Report — Centers for Disease Control and Prevention. http:// 38 K rul, DU. Life Expectancy Falling in the US
United States, 2013. Atlanta, GA: CDC, 2013. www.cdc.gov/cancer/breast/statistics/race.htm — But in Tribal Communities Not So Much.
8 Proctor BD, JL Semega and MA Kollar. Income Indian Country Today. May 11, 2017. https://
23 Prostate Cancer Rates by Race and Ethnicity.
and Poverty in the United States: 2016. Wash- indiancountrymedianetwork.com/culture/
In Centers for Disease Control and Prevention.
ington , DC: United States Census Bureau, health-wellness/life-expectancy-falling-us-
http://www.cdc.gov/cancer/prostate/statis-
2016. https://www.census.gov/content/dam/ tribal-communities-not-much/.
tics/race.htm
Census/library/publications/2016/demo/
24 Cervical Cancer Rates by Race and Ethnicity. 39 N ational Prevention Council. National
p60-256.pdf.
In Centers for Disease Control and Prevention. Prevention Strategy: Elimination of Health
9 Wilson, V. “New Census Data Show No Prog- Disparities. Washington, DC: National
http://www.cdc.gov/cancer/cervical/statis-
ress in Closing Stubborn Racial Income Gaps. Prevention Council, 2014.
tics/race.htm
Working Economics Blog September 16,
25 Centers for Disease Control and Prevention. 40 T he Joint Commission. Implicit Bias in Health
2015. https://www.epi.org/blog/new-census-
CDC Health Disparities and Inequalities Report — Care. April 2016. https://www.jointcom-
data-show-no-progress-in-closing-stubborn-ra-
United States, 2013. Atlanta, GA: CDC, 2013. mission.org/assets/1/23/Quick_Safety_
cial-income-gaps/ https://www.epi.org/blog/ Issue_23_Apr_2016.pdf
new-census-data-show-no-progress-in-closing- 26 Sudden Unexpected Infant Death and Sud-
stubborn-racial-income-gaps/. den Infant Death Syndrome. In Centers for 41 https://www.cancer.org/content/dam/can-
Disease Control and Prevention. http://www.cdc. cer-org/research/cancer-facts-and-statistics/
10 DeNavas-Walt C, Proctor BD. Income and
gov/sids/data.htm colorectal-cancer-facts-and-figures/colorectal-
Poverty in the United States: 2014. Washing- cancer-facts-and-figures-2017-2019.pdf
ton , DC: United States Census Bureau, 2015. 27 Centers for Disease Control and Prevention.
Vital Signs: Asthma in the U.S. Atlanta, GA: 42 J oseph DA, Redwood D, DeGroff A, Butler
11 C
ubbin C, Pedregon V, Egerter, S, Braveman P.
Centers for Disease Control and Prevention, EL. Use of evidence-based interventions
Issue Brief 3: Neighborhoods and Health. Princ-
2011. http://www.cdc.gov/vitalsigns/asthma/ to address disparities in colorectal cancer
eton, NJ: Robert Wood Johnson Foundation, screening. MMWR Suppl 2016:2016;65(No.
Commission to Build a Healthier America, 2008. 28 Akinbami LJ, Simon AE and Rossen LM. Suppl 1).
12 Meyer PA, Yoon PW, Kaufmann RB. Introduc- Changing trends in asthma prevalence
among children. Pediatrics, 137(1):1-7, 2016. 43 C ommunity Preventive Services Task Force.
tion: CDC Health Disparities and Inequalities Updated recommendations for client- and
Report — United States, 2013. Morb Mort Sur- 29 Centers for Disease Control and Prevention. provider-oriented interventions to increase
veil Summ, 2013; 62(3): 3-5 National Surveillance of Asthma: United States, breast, cervical, and colorectal cancer screen-
13 Powell L, Slater S, and Chaloupka F. The 2001-2010. National Center for Health Sta- ing. Am J Prev Med 2012;43:92–6 .
Relationship between Community Physical tistics Data Brief, 2012. http://www.cdc.gov/
nchs/data/series/sr_03/sr03_035.pdf 44 H ealthy Heartlands. In ISAIAH. https://isa-
Activity Settings and Race, Ethnicity and So- iahmn.org/healthy-heartlands/
cioeconomic Status. Evidence-Based Preventive 30 Most Recent Asthma Data — Mortality. In Cen-
Medicine, 1(2): 135-44, 2004. ters for Disease Control and Prevention. http:// 45 RWJF. RWJF Culture of Health Sentinel Commu-
www.cdc.gov/asthma/most_recent_data.htm nity Snapshot: Stockton, California. Princeton,
14 Bell JF, Wilson JS, and Liu GC. Neighborhood NJ: RWJF, 2017. https://www.cultureofhealth.
Greenness and 2-Year Changes in Body Mass 31 2 015 National Healthcare Quality and Disparities org/content/dam/COH/PDFs/stockton-
Index of Children and Youth. American Jour- Report and 5th Anniversary Update on the National california-full-snapshot.pdf
nal of Preventive Medicine, 35(6): 547-553, 2008. Quality Strategy. Rockville, MD: Agency for
15 Why Low-Income and Food Insecure People Healthcare Research and Quality; April 2016.
are Vulnerable to Obesity. In Food Research AHRQ Pub. No. 16-0015. http://www.ahrq.
and Action Center. http://frac.org/initiatives/ gov/sites/default/files/wysiwyg/research/
hunger-and-obesity/why-are-low-income-and- findings/nhqrdr/nhqdr15/2015nhqdr.pdf
food-insecure-people-vulnerable-to-obesity/. 32 The Joint Commission. Implicit Bias in Health
16 Miranda ML, Edwards SE, Keating MH, Paul Care. April 2016. https://www.jointcom-
CJ. Making the Environmental Justice Grade: mission.org/assets/1/23/Quick_Safety_
The Relative Burden of Air Pollution Expo- Issue_23_Apr_2016.pdf
sure in the United States. Int J Environ Res 33 Dwyer-Lindgren L, Bertozzi-Villa A, Stubbs
Public Health. 2011 Jun; 8(6): 1755–1771. RW, Morozoff C, Mackenbach JP, van Lenthe
FJ, Mokdad AH, Murray CJL. Inequalities
1730 M Street, NW, Suite 900
17 Centers for Disease Control and Prevention. Di-
abetes Report Card 2014. Atlanta, GA: Centers for in Life Expectancy Among US Counties, Washington, DC 20036
1980 to 2014Temporal Trends and Key Driv-
Disease Control and Prevention, 2015. http://
ers. JAMA Intern Med. 2017;177(7):1003–1011.
(t) 202-223-9870
www.cdc.gov/diabetes/pdfs/library/diabetes-
reportcard2014.pdf (accessed September 2016). doi:10.1001/jamainternmed.2017.0918. (f) 202-223-9871You can also read

















































