Recognising assessing and treating ADHD - Prof Dave Coghill - RANZCP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Recognising assessing
and treating ADHD
Prof Dave Coghill
1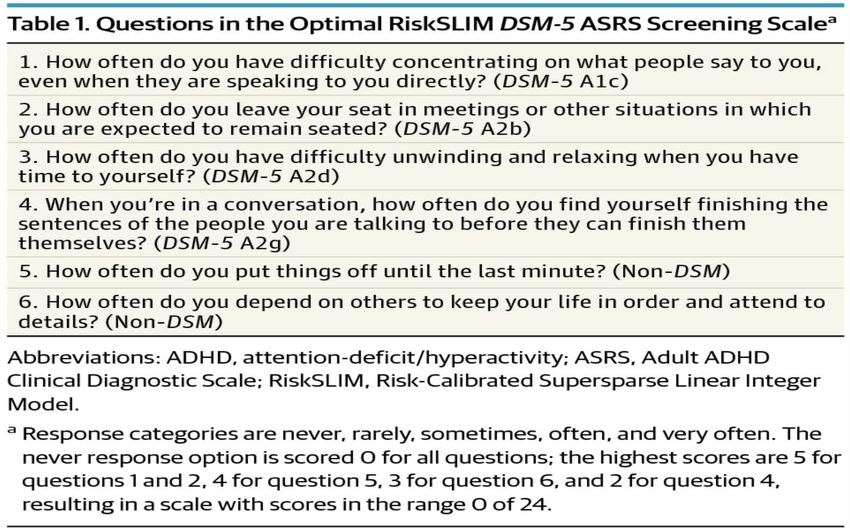
Recommended screening instruments
SCALE
Adult ADHD Self Report Scale - Freely available from WHO
(ASRS) - Main version: 18-items
- Short screening version: 6-items
DSM-IV symptom checklists Options:
(current, retrospective and - Barkley workbook scales
informant versions) - DuPaul rating scale
- Connors adult ADHD rating scale
(short, long and clinician versions)
Awareness of ADHD:
chronic trait-like symptoms with inattention, restlessness,
impulsiveness and emotional dysregulation
From: The World Health Organization Adult Attention-Deficit/Hyperactivity Disorder Self-Report Screening
Scale for DSM-5
JAMA Psychiatry. 2017;74(5):520-526. doi:10.1001/jamapsychiatry.2017.0298
Questions in the Optimal RiskSLIM DSM-5 ASRS Screening Scalea
Copyright 2017 American Medical Association.
Date of download: 2/23/2018
All Rights Reserved.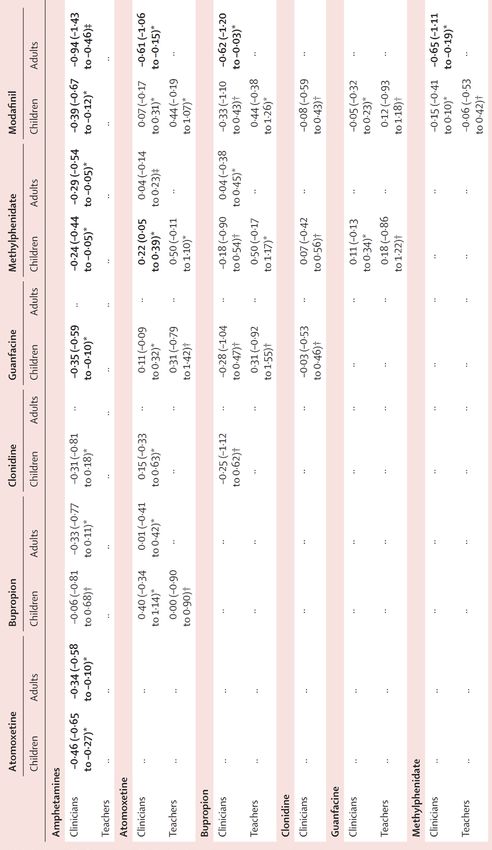
Assessing ADHD in the clinic Professor David Coghill
Key principles The diagnosis of ADHD can be distinguished from other common psychiatric disorders. Diagnosis is no more difficult to make than the evaluation of other common mental health disorders such as anxiety or depression. ADHD in adults is a symptomatic disorder (not just about behaviour) ADHD in adults is often misdiagnosed for other common adult mental health disorders ADHD in adults is in most cases treatable
When evaluating the diagnosis of ADHD in
adults there are several key points to consider:
• The DSM-5 criteria;
• diagnostic interviews;
• age-adjusted criteria for symptoms;
• ADHD symptoms are trait like;
• associated symptoms and functional impairments;
• behavioral aspects of the patient’s mental state during their clinical evaluation;
• obtaining accurate accounts of symptoms;
• compensatory mechanisms used by the patient.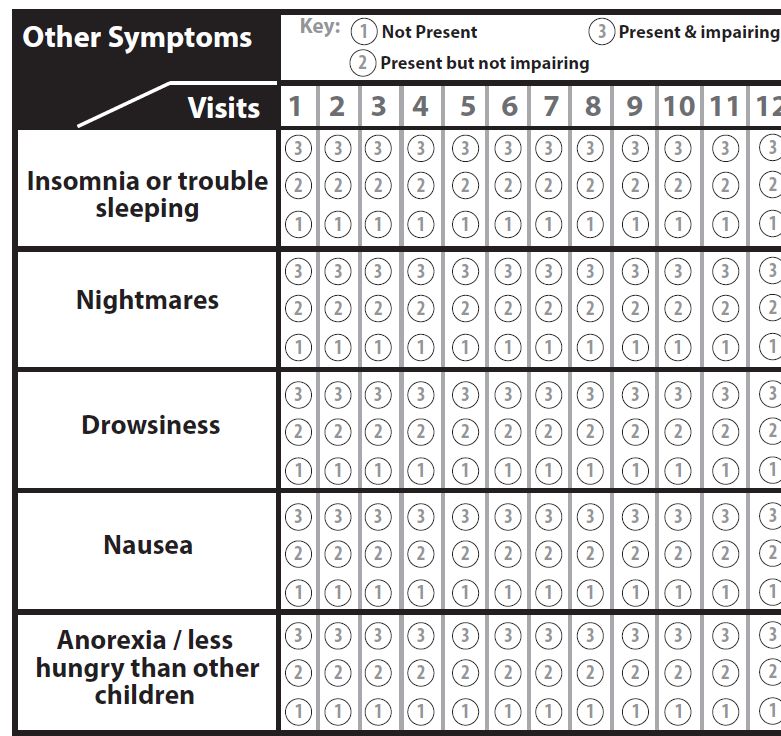
Diagnostic interview The diagnosis should be made following a detailed clinical interview to evaluate the presence of inattention, hyperactivity, and impulsivity when they are severe and impairing. The key elements are: • current ADHD symptoms; • common associated symptoms of ADHD that do not appear in the DSM criteria • retrospective (occurring in child or adolescent) ADHD symptoms; • impairments associated with ADHD symptoms; • comorbid symptoms, syndromes, and disorders.
Obtain accurate accounts of attention deficit
hyperactivity disorder symptoms
Adult informants tend to minimize their symptoms.
Adults may also have only a poor recall of their symptoms and behaviors as children.
It is also not unusual to find a patient who appears too eager to be diagnosed with ADHD and perceives
the diagnosis as a solution to problems that are unrelated to ADHD.
The diagnosis of ADHD can nevertheless be established in most cases by:
• accurate use of the DSM criteria;
• enquiring after detailed accounts of problems related to ADHD symptoms;
• obtaining collateral information from relatives, partners, or work colleagues whenever possible;
• review of written reports (eg, school or work reports) whenever possible.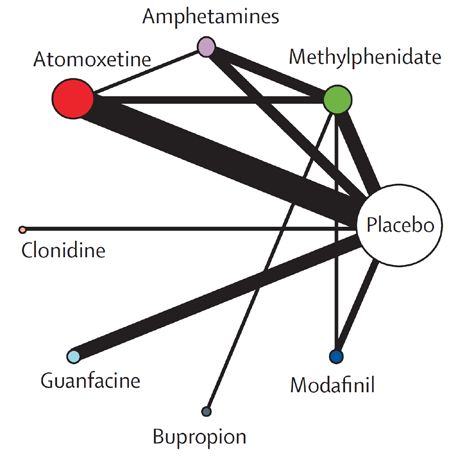
Compensatory mechanisms reduce apparent
impairments
• support by a member of the family or paid assistant;
• support of an organized partner;
• flexible work schedule;
• occupations or activities where impulsivity may be a positive factor or where high levels
of risk may be involved (eg, emergency services, adventure sports);
• excessive preplanning and checking to compensate for difficulties in organizing,
planning ahead, and forgetfulness;
• use of electronic aids such as smart phones with alarms, reminders, and electronic
calendars.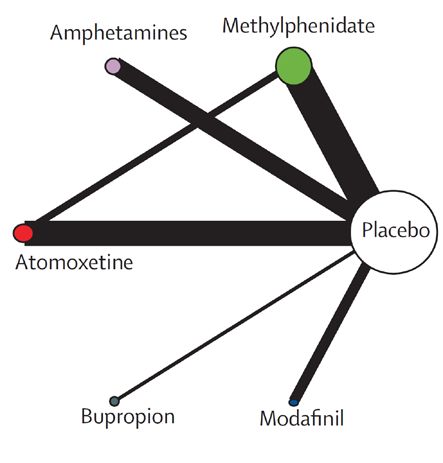
www.divacenter.eu
ADHD and Comorbidity Professor David Coghill
ADHD: Comorbid Conditions
60
50
40%
40
30–35%
(%)
30
20–25% 15–25%
15–20% 20% 19%
20
15%
10
0
Oppositional Language Anxiety Learning Mood Conduct Smoking4 Substance
defiant disorder2 disorders3 difficulties2 disorders2 disorder3 use
disorder1 disorder5
1MTA Cooperative Group. Arch Gen Psychiatry 1999; 56: 1076-86
2Barkley.Attention-deficit Hyperactivity Disorder. A Handbook for Diagnosis and Treatment, 2nd ed. New York: Guilford
Press, 1993
3Biederman. Am J Psychiatry 1991; 148: 565-77
4Milberger. J Am Acad Child Adolesc Psychiatry 1997; 36: 37-44
5Biederman. J Am Acad Child Adolesc Psychiatry 1997; 36: 21-9Sub-threshold psychopathology in ADHD in
non-comorbid Adult ADHD
9
8
7
6
Odds
Ratio
5
4
3
2
1
0
• Kessler RC, et al. Am J Psychiatry 2006;163:716––23.
• PTSD: post-traumatic stress disorder; OCD: obsessive-compulsive disorder; SUD: substance abuse disorderSub-threshold psychopathology in a sample of non-comorbid Adult ADHD Skirrow & Asherson 2013, Journal of Affective Disorders
Comorbid symptoms, syndromes and disorders
Symptoms of ADHD: symptoms of ADHD that mimic other
common mental health disorders: Genes regulating
neurotransmitter systems have been implicated in ADHD
Overlapping neurodevelopmental disorders: autism spectrum
disorders and specific learning difficulties
ADHD as a developmental risk factor: development of comorbid
mental health disorder (e.g. substance abuse, personality disorder,
anxiety, depression, bipolar disorder)
Asherson et al., Lancet Psychiatry, 2016, 3: 568-78Symptoms and impairments of ADHD that can
mimic other disorders
Anxiety: excessive mind wandering, worrying about performance deficits, feeling overwhelmed,
feeling restless, avoidance of situations due to ADHD symptoms (e.g. waiting in queues, social
situations requiring focused attention), and sleep problems linked to mental restlessness
Depression: chronic low self-esteem unstable moods, impatience, irritability, poor concentration,
sleep disturbance
Personality disorder (e.g. borderline): chronic trait-like psychopathology, behavioural problems,
emotional instability, impulsive behaviour, poor social relationships
Bipolar disorder: Restlessness and overactivity, sleep disturbance, mood instability, ceaseless
unfocused mental activity, distractibility
Asherson et al., Lancet Psychiatry, 2016, 3: 568-78Overlapping neurodevelopmental disorders
Neurodevelopmental conditions occur more frequently in ADHD due to
largely to shared genetic risk factors. These include:
Dyslexia (overlapping genetic risk factors)
Dyspraxia
Specific and general learning difficulties (overlapping genetic risk factors,
inattention)
Pervasive developmental disorders (Aspergers, Autism, PDD NOS)
Tic disorders / Tourette’s disorder
ADHD: Attention-deficit hyperactivity disorder.
17The ‘Risk Model’: ADHD as a risk factor for the development
of co-occurring conditions later in life
Antisocial behaviour
ADHD Addiction
Depression/low self-esteem
Anxiety
Environmental and genetic risks
(e.g. maltreatment / COMT genotype)ADHD increases risk for adolescent /
adult onset comorbidities
Depression and Anxiety disorders
- accumulation of adverse life events, emotional dysregulation,
low self-esteem, functional impairments
Anti-social behavior, personality disorder and substance misuse
disorders
- increased level of psychosocial risk factors, impaired
psychosocial development, emotional dysregulation,
impulsivity, self-treatment
ADHD: Attention-deficit hyperactivity disorder.
19Bipolar disorder
Bipolar disorder ADHD
Usually adolescent or adult onset Usually onset during early childhood
Episodic course and clear change from pre- Trait like course and no change from pre-morbid
morbid state state
Grandiose and elated/irritable mood – client Excitable but not grandiose or elated – client
reports high levels of function reports being unable to function
Episodes of depression Chronic low self-esteem
Depressive episodes at increased rate in ADHD
Tends to lack insight Usually has insight and complains of changeable
moods and inability to focus/function
Reduced need for sleep Complains of difficulty sleeping
Subjective sense of sharpened mental abilities Complains of being unable to concentrate/focus
Impaired/abnormal functioning during episodes Variable levels of function – generally unrelated
of depression or hypomania to mood state
Over activity, often linked to unrealistic Restlessness (fidgety, difficulty sitting still)
ideas/plans May prefer to be on the go. Impulsive style
(taking excessively/interrupting people)
ADHD: Attention-deficit hyperactivity disorder.
20Emotional lability (EL)
Excessive emotional reactions , frequent mood
changes: Irritability, volatility, hot temper1
Mood Emotional
instability dysregulation
Affective
lability
EL Emotional
impulsivity
Deficient
emotional self
regulation
60-70% heritable2
1Skirrow et al (2009); 2van Beijsterveldt et al (2004)ADHD With Comorbid Anxiety
Approximately 25% patients with ADHD are often
comorbid with anxiety disorders
Anxiety in ADHD may
• partially inhibit the impulsivity and response inhibition deficits
• make working memory deficits worse
• may be qualitatively different from more phobic types of
anxiety seen in pure anxiety samples
Schatz DB and Rostain AL. J Atten Disord 2006;10:141-149Three main reasons for the association of
ADHD with substance use disorders
High stimulus/novelty-seeking behavior and Impulsivity
– inherent features of ADHD
– shared genetic risk
Impaired social/academic/work function
– secondary consequence of psychosocial impairments
Relief from symptoms
– self-treatment of symptoms (e.g. cannabis, alcohol, cocaine)
And conduct disorderThe challenges in diagnosing adult ADHD in
patients with comorbidities
1. Overlapping symptoms and impairments
2. Non-specifc symptoms include emotional instability, sleep problems and impulsive
behaviour
3. Lack of awareness of the characteristic features of ADHD among mental health
professionals and primary care physicians
4. Clinical features of ADHD may mimic other disorders
4. Dual diagnosis is common
5. Symptoms may not be apparent during assessment appointments, but reflect difficulties
experienced in daily activities.Psychoeducation, accommodations and lifestyle modification– the first line treatment for all
Psychoeducation
Requires you the clinician to really know what they are talking about and to
be able to answer the questions from the patient and their family.
• What are the causes of ADHD? • What is the best treatment?
• His father says that ADHD is not • How long will he need to be on
real medication for
• Is it my fault? • Wont medication just turn him
• Will he grow out of it? into a zombie?
• Will he get addicted?Treatment Planning and decision making
Aim is to have a holistic shared treatment plan It is important to regularly discuss with
that addresses psychological, behavioural and people with ADHD, and their family
occupational or educational needs. Take into
account:
members or carers, how they want to be
involved in treatment planning and
• the severity of ADHD symptoms and
impairment, and how these affect or may
decisions
affect everyday life (including sleep) Such discussions should take place at
• their goals intervals to take account of changes in
• their resilience and protective factors circumstances (e.g. the transition from
• the relative impact of other
children's to adult services) and
neurodevelopmental or mental health developmental level, and should not
conditions. happen only once.
27Key points for discussion
• The benefits and harms of non- • The ways that other mental health or
pharmacological and pharmacological neurodevelopmental conditions might
treatments affect treatment choices
• the efficacy of medication compared with no • The importance of adherence to
treatment or non-pharmacological
treatments
treatment and factors that may affect
• potential adverse effects and non-response • Reassure people with ADHD, and their
rates families or carers as appropriate, that
• The benefits of a healthy lifestyle, they can revisit decisions about
including exercise treatments.
• Their preferences and concerns –
understanding what is impacting on
these 28Structured discussion about ADHD
• The positive impacts of receiving a • Education issues
diagnosis, such as: • Employment issues (for example,
• improving their understanding of impact on career choices and rights to
symptoms reasonable adjustments in the
• identifying and building on individual workplace)
strengths • Social relationship issues
• improving access to services
• The increased risk of substance misuse
• The negative impacts of receiving a and self-medication
diagnosis, such as stigma and labelling
• The possible effect on driving
• The importance of environmental
modifications to reduce the impact of
ADHD symptoms 29Supporting Families and Carers
• Offer advice about the • Explain to parents and carers • Offer advice to families and
importance of: that any recommendation of carers of adults with ADHD
• positive parent– and carer– parent-training/education about:
child contact does not imply bad parenting • How ADHD may affect
• clear and appropriate rules • The aim is to optimise relationships
about behaviour and parenting skills to meet the • How ADHD may affect the
consistent management above-average parenting person's functioning
• structure in the child or needs of children and young • The importance of structure
young person's day. people with ADHD. in daily activities.
• To enable them to provide
scaffolding to enable their
child to thrive
Consider the particular needs of the parent with ADHD who has a
child with ADHD 30School based accommodations for ADHD
Preferential seating away from distraction Extended time for testing
• away from door, window, pencil sharpener or Modification of test format and delivery
distracting students
• oral exams
• near the teacher • use of a calculator
• a quiet place to complete school work or tests • chunking or breaking down tests into smaller
• seating student by a good role model sections to complete
/classroom "buddy")
• providing breaks between sections
• quiet place to complete tests
• multiple choice or fill in the blank test format
instead of essay
31School based accommodations for ADHD
Modifications in classroom and homework Providing student with a copy of class notes, peer
assignments assistance with note taking, audio taping of
• shortened assignments and/or extended time lectures
to complete assignments Providing clear and simple directions for
homework and class assignments
• reduced amount of written work
• breaking down assignments and projects into Schedule classes that require most mental focus
segments with separate due at the beginning of school day
• allowing student to dictate or tape record Schedule in regular breaks for student throughout
responses and/or use computer for written the day to allow for physical movement and "brain
work rest,"
• oral reports or hands-on projects to Card system to allow out of class when things get
demonstrate learning of material too tough
Wobble cushions
32LIFESTYLE MODIFICATION
For Adults with ADHD
1. Sleep
2. Exercise
3. Emotional regulation techniques
4. Work / Education guidance
5. Communication & relationships
6. Addressing addictions
7. Networks and ‘Integration’
8. Dietary changes
9. Outside help: Counselling / Coaching / Therapy
10. Time management, Organisation & StructureTreating ADHD
34Which treatments work for
ADHD?
*
1.4
1.2
1 1.00
Effect Size
0.8
0.6
0.4
0.51
0.42
0.29
0.2 0.24
0.16
0 0.02
-0.2
-0.4
Restrictive Artificial Omega 3 Cognitive Neurofeedback Parent Stimulant
elimination food fatty acids Training training Medications
diets colourings (fish oils) (e.g. Ritalin)Negative parenting
Parent Training
Does Improve
SMD Parenting and
0.43
Conduct Problems
Conduct Problems
Positive parenting
SMD
SMD 0.31
0.63
Which treatments work for
ADHD?
1.4
1.2
1 1.00
Effect Size
0.8
0.6
0.51
0.4 0.42 0.29
0.2 0.24
0.16
0 0.02
-0.2
-0.4
Restrictive Artificial Omega 3 Cognitive Neurofeedback Parent Stimulant
elimination food fatty acids Training training Medications
diets colourings (fish oils) (e.g. Ritalin)ADHD medications are very effective in children and adolescents
Effect Size Number Needed to Treat
Methylphenidate 1.0 4
Amfetamine 1.0 4
Atomoxetine 0.7 4
(maybe higher when given for longer)
Guanfacine/Clonidine 0.6-0.7 4
SSRI for depression in adults 0.5 10
Antipsychotics for schizophrenia in 0.25 10
adultsADHD
Response to Stimulants
Meta-analysis of within-subject comparative trials evaluating response
to stimulant medications
40
About 70% of patients
respond to methylphenidate,
36%
38%
30 70% respond to amfetamine
Best
Response and overall26%
95% respond to
(Percent)
20 one or the other
10
0
Dextroamfetamine Methylphenidate Equal response
to either
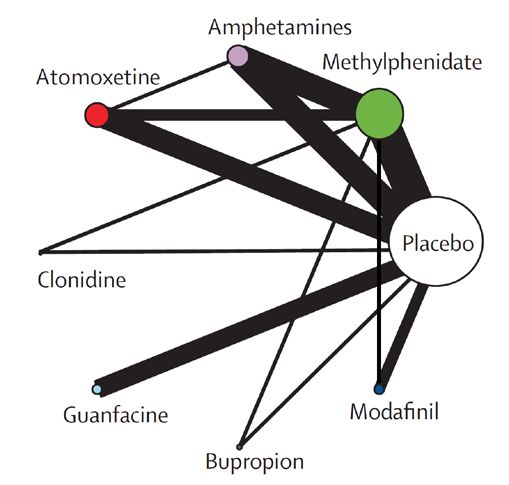
Greenhill et al. JAACAP 1996;35:1304. stimulant133 double-blind RCTs, >24,500 participants
Drugs vs placebo - Efficacy
Mean change in ADHD symptoms
CHILDREN & ADOLESCENTS ADULTS
Drug SMD [95% CI] SMD [95% CI]
Amphetamines - 1.02 [-1.19,-0.85] - 0.79 [-0.99,-0.58]
Atomoxetine - 0.56 [-0.66, -0.45] - 0.45 [-0.58,-0.32]
Bupropion - 0.96 [-1.69, -0.22] - 0.46 [-0.85,-0.07]
Clonidine - 0.71 [-1.17, -0.24] no data
Guanfacine - 0.67 [-0.85, -0.50] no data
Methylphenidate - 0.78 [-0.93, -0.62] - 0.49 [-0.64,-0.35]
Modafinil - 0.62 [-0.84, -0.41] 0.16 [-0.28,0.59]
-1 -0.5 0 0.5 -1 -0.5 0 .05
Favors drug Favors placebo Favors drug Favors placebo
Drugs vs placebo - Acceptability
Methylphenidate in C&A only and amphetamines in adults only were
significantly better than placebo (OR 0·69 and 0·68, respectively)Drugs vs placebo - Tolerability
Dropouts due to adverse events
CHILDREN & ADOLESCENTS ADULTS
Drug OR [95% CI] OR [95% CI]
Amphetamines 2.30 [1.36, 3.89] 3.26 [1.54,6.92]
Atomoxetine 1.49 [0.84, 2.64] 2.33 [1.28,4.25]
Bupropion 1.51 [0.17, 13.27] 2.55 [0.33,19.93]
Clonidine 4.52 [0.75, 27.03] no data
Guanfacine 2.64 [1.20, 5.81] no data
Methylphenidate 1.44 [0.90, 2.31] 2.39 [1.40,4.08]
Modafinil 1.34 [0.57, 3.18] 4.01 [1.42,11.33]
0.5 1 2 4 10 0.5 1 2 4 10
Favors drug Favors placebo Favors drug Favors placebo
• Weight decreased by AMPH and MPH in C&A + adults.
• Systolic blood pressure increased by AMPH in C&A only, and MPH in adults only
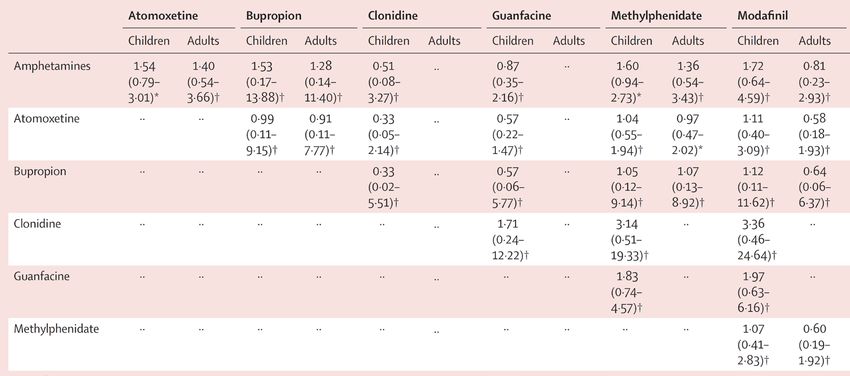
• Diastolic blood pressure increased by AMPH in C&A only, and MPH in C&A + adults.Drugs vs drugs - Efficacy
Drugs vs drugs - Tolerability • Need to investigate specific adverse events
NICE ADHD Guideline - 2018
Diagnosis
Children age 5 to 18
Persisting impairment in ≥ 1
Information +
ADHD focussed
domain after environmental
modifications?
yes
support
ADHD w/o ODD/CD
First-line
methylphenidate
Switch to:
no Effective?
1st: Lisdexamphetamine
2nd: atomoxetine or
guanfacine Persisting
impairment in yes
yes ≥1 domain?
Individual-based
CBT/SST
Effective?
no
Tertiary opinion review
reviewNICE ADHD Guideline - 2018
Diagnosis
Children age 5 to 18
Persisting impairment in ≥ 1
Information +
ADHD focussed
domain after environmental
modifications?
yes
support
ADHD w/o ODD/CD
First-line
ADHD + ODD/CD Complex/ methylphenidate
refuse
Offer group
Switch to:
no Effective?
Group parent training* 1st: Lisdexamphetamine
2nd: atomoxetine or
guanfacine Persisting
impairment in yes
yes ≥1 domain?
Effective? no Individual-based
CBT/SST
Effective?
yes no
Individual-based
Parent Training Tertiary opinion review
review
review
* Developed for treatment of conduct disorderNICE ADHD Guideline - 2018
Diagnosis
Adults Persisting impairment
in ≥ 1 domain after
ADHD focussed
Diagnosis ADHD information
environmental
modifications?
yes
First-line
Lisexamphetamine
or methyphenidate
Group or individual offer Persisting impairment Effective?
psychological in ≥ 1 domain?
treatment (CBT) yes
no
Switch to 2nd
stimulant
yes or atomoxetine
reviewADHD: Easy to treat Hard to treat well
MTA ADHD Symptoms – MTA Group 1999
2.5
2
1.5
1
Combined Medication and Behavioural
0.5
0
0 14
Months Post Randomization
At the end of the 14 month trial
Medication alone better than Behavioural alone
Medication alone better than Community Care (60% CC on medication)
Combined Medication and Behavioural not much better than medication alone
Behavioural as good as Community Care (60% CC on medication)SNAP or ADHD IV Rating Scales 2.5 2 1.5 1 0.5 0
MTA ADHD Symptoms – MTA Group 1999
2.5
2
1.5
1
Combined Medication and Behavioural
0.5
0
0 14
Months Post Randomization
At the end of the 14 month trial
Medication alone better than Behavioural alone
Medication alone better than Community Care (60% CC on medication)
Combined Medication and Behavioural not much better than medication alone
Behavioural as good as Community Care (60% CC on medication)Dundee CAMHS before development of
ADHD care pathway
SNAP or ADHD IV Rating Scales
2.5
2.5
2
1.5
1.6
1
0.5
0
Baseline In
Treatmen
tDifferences between MTA “medication
protocol” and “community care”
“Medication” group were
• treated with doses 10 mg/day greater
• Had 3x–daily dosing VS. twice-daily dosing
• Started treatment with intensive 28 day double blind
titration trial
• Received supportive counselling and reading
materials
• Monthly dosage adjustments informed by
standardised outcome measures and teacher
consultationsDifferences between MTA “medication
protocol” and Dundee Clinical Care
“Medication” group were
• treated with higher doses
• Had 3x–daily dosing VS. twice-daily dosing
• Started treatment with intensive 28 day double blind
titration trial
• Received supportive counselling and reading
materials
• Monthly dosage adjustments informed by
standardised outcome measures and teacher
consultationsESCAP 2007
Most parents are reasonably satisfied with their child’s treatment
Q: Overall, how satisfied are you with your child’s current ADHD treatment? Please
rate your level of satisfaction based on a scale of 1–7, where 1 is “not at all
satisfied” and 7 is “extremely satisfied.”
Not at all satisfied Extremely satisfied
1 2 3 4 5 6 7
4% 4% 9% 15% 28% 25%
15%
5.0
Mean score = 5.0
Baseline: All qualified respondents whose child currently receives prescribed medication (n=350)
Survey conducted bySurvey
Harris Interactive,
conducted withInteractive,
by Harris the supportwith of
theJanssen-Cilag EMEA, aEMEA,
support of Janssen-Cilag division of Janssen
a division Pharmaceutica
of Janssen Pharmaceutica NV.
NV.
1st March – 21st June 2007The same parents reported that their children
with ADHD find the whole day challenging
80 Q: What time(s) of day does your child find challenging, if any?
Norms Non Rx
60 6-8 hrs 12 hrs
%
40
20
0
Baseline: all qualified respondents (norms survey, n= 995; ADHD survey, n=910)
Survey conducted bySurvey
Harris Interactive,
conducted withInteractive,
by Harris the supportwith of
theJanssen-Cilag EMEA, aEMEA,
support of Janssen-Cilag division of Janssen
a division Pharmaceutica
of Janssen Pharmaceutica NV.
NV.
1st March – 21st June 2007The Dundee ADHD care pathway • Had to be effective and cost effective • A modified version of the MTA MED protocol (perhaps MTA light) • Standardised approach to all consultations with uniform protocols and standardized outcomes • Initial 4 week titration with aim to optimize symptom outcomes and minimize adverse effects • Ongoing follow up using the same standardized approach to consultations (with an added focus on “other problems”) • Nurse led with medical back up (the floating doctor)
2.5 Dundee
Mean SNAP item scores
2.5
2.0 CAMHS
Remission rate
before
44%
1.5 1.6 development
1.0 of ADHD
0.5 care
0
pathway
Baseline In
treatmentStandardized titration protocols
Maximum response at minimum dose
Routine use of standardized outcomes at every
visit
Nurses providing most face to face careDundee ADHD clinic protocol Delivered by nurses with medical backup (floating doctor) Fixed protocol with rigorous outcome measurements for continuing care • SNAP IV (clinician delivered) • SKAMP (teacher) • Height, weight, pulse and BP • AEs (framed as ‘other symptoms’) • Screen for “other problems” and arrange treatment as required
Coghill D & Seth S. Child Adolesc Psychiatry Ment Health 2015;9:52
2.5
Mean SNAP item scores
2.5
2.0
1.5 Remission rate
67%
1.0
0.5 0.7 0.8
0
Baseline End of Most recent
titration visit
Mean duration of treatment (range): 43 months (1–119 months)
Mean dose of MPH: 52 mg/daySWANSON, NOLAN & PELHAM (SNAP IV - clinician-scored)
Child’s Name………………………… Date of Birth ……………………………...
Date Completed ………………….....
Never or Sometimes Often Very Ofte Never or Sometimes Often Very Ofte
INATTENTION (INATT) rarely (never) (mild) (moderate) (severe) HYPERACTIVITY/IMPULSIVITY (HYP/IMP) rarely (never) (mild) (moderate) (severe)
1 Fails to give close attention to details or 0 1 2 3 10 Fidgets with hands or feet or squirms in 0 1 2 3
makes careless mistakes in schoolwork seat
2 Has difficulty sustaining attention in tasks 0 1 2 3 11 Leaves seat in classroom or in other 0 1 2 3
or play activities situation in which remaining seated is
expected
3 Does not seem to listen when spoken to 0 1 2 3
directly 12 Runs about or climbs excessively in 0 1 2 3
situations in which it is inappropriate
4 Does not follow through on instructions and 0 1 2 3
13 Has difficulty playing or engaging in leisure 0 1 2 3
fails to finish schoolwork, chores or duties
activities quietly
5 Has difficulty organising tasks and activities 0 1 2 3
14 Is “on the go” or acts as if “driven by a 0 1 2 3
motor”
6 Avoids tasks (e.g. schoolwork, homework) 0 1 2 3
that requires sustained mental effort 15 Talks excessively 0 1 2 3
7 Loses things necessary for tasks or 0 1 2 3
activities (e.g. toys, school assignments, 16 Blurts out answers before questions have 0 1 2 3
pencils or books) been completed
8 Is easily distracted 0 1 2 3 17 Has difficulty waiting turn 0 1 2 3
9 Is forgetful in daily activities 0 1 2 3 18 Interrupts or intrudes on others 0 1 2 3
INATT TOTAL SCORE: = INATT SUMMARY SCORE (TOTAL SCORE/9) = HYP/IMP TOTAL SCORE: = HYP/IMP SUMMARY SCORE (TOTAL SCORE/9) =Assessing symptom outcome
ADHD-RS-IV or SNAP-IV questionnaire score (ii) Post-treatment monitoring
Total score (range 0–54) Mean item total scorea Clinical interpretation
0–18 ≤1 Very good/optimal response: symptoms well within
normal range
Good response: symptoms within normal range but may
19–26 2 Need to assess other factorsWhat to do if response clinically inadequate after titration? • Switch to the other stimulant if available • May consider atomoxetine or α2 agonist where MPH is not tolerated or associated with significant safety issues • although this should not be automatic • But if the non stimulants are the only alternative don’t forget that they are also effective medications
With such good outcomes why does it seem so hard to
change routine clinical practice?
•I’m pretty sure you don’t need help to
come up with reasons why this would
be too hard in your clinical setting
•Our view was that it needed to shift
thinking from problem finding to
solution focused.Standardized titration protocols
Maximum response at minimum dose
Routine use of standardized outcomes at every
visitAdverse effects of medication taken very seriously
Other symptoms
Not Present but Present and Present and
Write note↓
present not impairing severely
impairing impairing
Insomnia or trouble sleeping 0 1 2 3
Nightmares 0 1 2 3
Drowsiness 0 1 2 3
Nausea 0 1 2 3
Anorexia (Less hungry than other 0 1 2 3
children)
Stomach-aches 0 1 2 3
Headaches 0 1 2 3
Dizziness 0 1 2 3
Sad/unhappy 0 1 2 3
Prone to crying 0 1 2 3
Irritable 0 1 2 3
Thoughts of self-harm 0 1 2 3
Suicidal ideation 0 1 2 3
Euphoric/unusually happy 0 1 2 3
Anxious 0 1 2 3
Tics or nervous movements 0 1 2 3
“Spaced-out” / “Zombie-like” 0 1 2 3
Less talkative than other children 0 1 2 3
Less sociable than other children 0 1 2 3Managing symptoms is clearly only
part of the battle
Need to seek and address “other problems”
• Structured prompts to ask about other mental and physical health
problems
• Structured assessment of potential adverse effects of medication
• Height weight and blood pressure charted against norms
• Discussion about school/college/work functioning
• Family relationships and functioning
• Peer relationships and community activities
71Thank you
You can also read