Recommendations for Prevention and Control of Influenza in Children, 2014-2015
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Organizational Principles to Guide and Define the Child
Health Care System and/or Improve the Health of all Children
POLICY STATEMENT
Recommendations for Prevention and Control of
Influenza in Children, 2014–2015
COMMITTEE ON INFECTIOUS DISEASES
KEY WORDS
abstract
influenza, immunization, live attenuated influenza vaccine, The purpose of this statement is to update recommendations for rou-
inactivated influenza vaccine, vaccine, children, pediatrics
tine use of seasonal influenza vaccine and antiviral medications for the
ABBREVIATIONS prevention and treatment of influenza in children. The American Acad-
AAP—American Academy of Pediatrics emy of Pediatrics recommends annual seasonal influenza immuniza-
ccIIV3—trivalent cell culture-based inactivated influenza vaccine
CDC—Centers for Disease Control and Prevention tion for all people 6 months and older, including all children and
FDA—US Food and Drug Administration adolescents. Highlights for the upcoming 2014–2015 season include
GRADE—Grading of Recommendations Assessment, Development, the following:
and Evaluation
HCP—health care personnel 1. The influenza vaccine composition for the 2014–2015 season is
ID—intradermal unchanged from the 2013–2014 season.
IIV—inactivated influenza vaccine
IIV3—trivalent inactivated influenza vaccine 2. Both trivalent and quadrivalent influenza vaccines are available in
IIV4—quadrivalent inactivated influenza vaccine the United States for the 2014–2015 season.
IM—intramuscular
LAIV—live attenuated influenza vaccine
3. Annual universal influenza immunization is indicated with either
LAIV4—quadrivalent live attenuated influenza vaccine a trivalent or quadrivalent vaccine (no preference).
NAIs—neuraminidase inhibitors
4. Live attenuated influenza vaccine (LAIV) should be considered for
PCR—polymerase chain reaction
PCV13—13-valent pneumococcal conjugate vaccine healthy children 2 through 8 years of age who have no contra-
pH1N1—influenza A (H1N1) pandemic virus indications or precautions to the intranasal vaccine. If LAIV is not
RIV3—trivalent recombinant influenza vaccine readily available, inactivated influenza vaccine (IIV) should be used;
This document is copyrighted and is property of the American vaccination should not be delayed to obtain LAIV.
Academy of Pediatrics and its Board of Directors. All authors have
filed conflict of interest statements with the American Academy of 5. The dosing algorithm for administration of influenza vaccine to
Pediatrics. Any conflicts have been resolved through a process children 6 months through 8 years of age reflects that virus
approved by the Board of Directors. The American Academy of
strains in the vaccine have not changed from last season.
Pediatrics has neither solicited nor accepted any commercial
involvement in the development of the content of this publication.
The guidance in this policy statement does not indicate an exclusive As always, pediatricians, nurses, and all other health care personnel
course of treatment or serve as a standard of care. Variations,
taking into account individual circumstances, may be appropriate.
should be immunized themselves and should promote influenza vac-
cine use and infection control measures. In addition, pediatricians
Policy statements from the American Academy of Pediatrics
benefit from expertise and resources of liaisons and internal should promptly identify clinical influenza infections to enable rapid
(AAP) and external reviewers. However, policy statements from antiviral treatment, when indicated, to reduce morbidity and mortality.
the American Academy of Pediatrics may not reflect the views of Pediatrics 2014;134:1–17
the liaisons or the organizations or government agencies that
they represent.
All policy statements from the American Academy of Pediatrics
automatically expire 5 years after publication unless reaffirmed, INTRODUCTION
revised, or retired at or before that time.
The American Academy of Pediatrics (AAP) recommends annual
(Continued on last page)
seasonal influenza immunization for all people 6 months and
older, including all children and adolescents, during the 2014–
2015 influenza season. In addition, special effort should be made to
vaccinate people in the following groups:
PEDIATRICS Volume 134, Number 5, November 2014 1
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015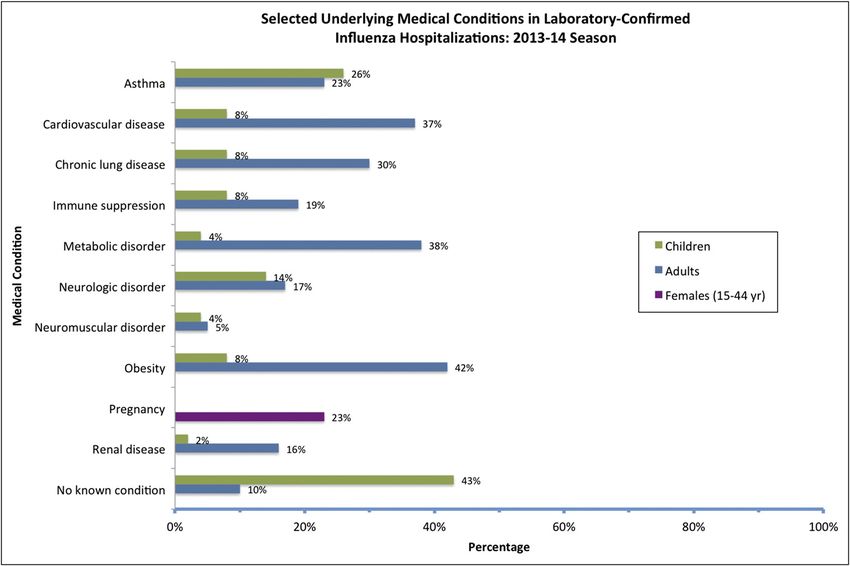
All children, including infants born more than two-thirds of children virus, and 2 deaths were associ-
preterm, who are 6 months and younger than 6 years and almost ated with dual infection with both
older with conditions that increase all children 6 years and older influenza A and B viruses. Although
the risk of complications from influ- spend significant time in child children with certain conditions
enza (eg, children with chronic med- care or school settings outside are at higher risk of complications,
ical conditions, such as asthma, the home. Exposure to groups of 47% of the deaths occurred in chil-
diabetes mellitus, hemodynamically children increases the risk of con- dren with no high-risk underlying
significant cardiac disease, immuno- tracting infectious diseases. Chil- medical condition. Among children
suppression, or neurologic and neu- dren younger than 2 years are at hospitalized with influenza and for
rodevelopmental disorders); elevated risk of hospitalization and whom medical chart data were
Children of American Indian or complications attributable to influ- available, approximately 43% had
Alaska Native heritage enza. School-aged children bear no recorded underlying condition,
a large influenza disease burden whereas 26% had underlying asthma
All household contacts and out-of- or reactive airway disease (Fig 1). A
and have a significantly higher
home care providers of
chance of seeking influenza-related recent preliminary observation of
Ø Children with high-risk condi- medical care compared with the 2013–2014 influenza season
tions healthy adults. Reducing influenza noted a high number of healthy peo-
Ø Children younger than 5 years, virus transmission (eg, appropriate ple (ranging from infants to older
especially infants younger than adults) who needed care in the ICU,
hand hygiene, respiratory hygiene/
6 months 91% of whom were not previously
cough etiquette) among children
All health care personnel (HCP) who attend out-of-home child care vaccinated.
All child care providers and staff or school has been shown to de- 3. Both trivalent and quadrivalent in-
All women who are pregnant, are crease the burden of childhood fluenza vaccines are available in
considering pregnancy, are in the influenza and transmission of influ- the United States for the 2014–
postpartum period, or are breast- enza virus to household contacts 2015 season. Neither vaccine for-
feeding during the influenza sea- and community members of all mulation is preferred over the
son ages. other. Both vaccines contain an A/
2. The percentage of outpatient visits California/7/2009 (H1N1)–like vi-
KEY POINTS RELEVANT FOR THE for influenza-like illness, rates of rus, an A/Texas/50/2012 (H3N2) vi-
2014–2015 INFLUENZA SEASON hospitalization, and deaths attrib- rus, and a B/Massachusetts/2/
uted to pneumonia and influenza 2012–like virus (B/Yamagata line-
1. Annual seasonal influenza vac-
age). The quadrivalent influenza
cine is recommended for all were lower during the 2013–2014
influenza season when compared vaccines include an additional B
people 6 months and older, in-
with the previous season. As of virus (B/Brisbane/60/2008–like vi-
cluding all children and adoles-
August 23, 2014, 107 laboratory- rus [B/Victoria lineage]). These
cents, during the 2014–2015
confirmed influenza-associated pe- strains are unchanged from those
influenza season. It is impor-
diatric deaths were reported to in the 2013–2014 seasonal influ-
tant that household contacts and
the Centers for Disease Control enza vaccines.
out-of-home care providers of chil-
dren younger than 5 years, es- and Prevention (CDC) during the 4. Optimal protection is achieved
pecially infants younger than 6 2013–2014 influenza season. The through annual immunization. An-
months, and children of any age 2009 influenza A (H1N1) pandemic tibody titers wane to 50% of their
at high risk of complications (pH1N1) viruses predominated, but original levels 6 to 12 months af-
from influenza (eg, children with influenza A (H3N2) and influenza B ter vaccination. Although the vac-
chronic medical conditions, such viruses also were reported in the cine strains for the 2014–2015
as asthma, diabetes mellitus, he- United States. Of the 107 deaths, 87 season are unchanged from last
modynamically significant cardiac were associated with influenza A season, a repeat dose this season
disease, immunosuppression, or viruses, and 16 deaths were asso- is critical for maintaining protec-
neurologic and neurodevelopmen- ciated with influenza B viruses. tion in all populations.
tal disorders) receive annual influ- Two deaths were associated with 5. Using the Grading of Recommen-
enza vaccine. In the United States, an undetermined type of influenza dations Assessment, Development,
2 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015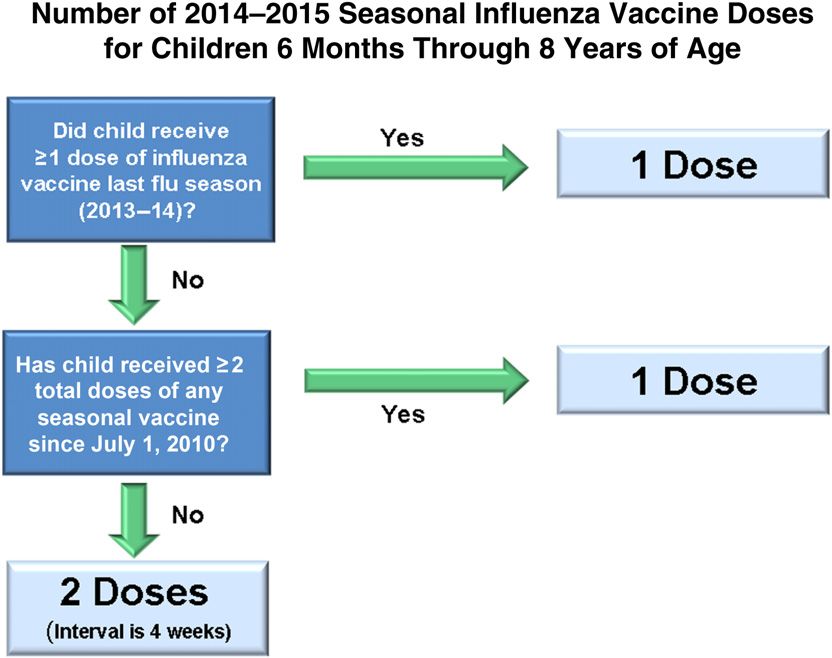
FROM THE AMERICAN ACADEMY OF PEDIATRICS
FIGURE 1
Selected underlying medical conditions in patients hospitalized with laboratory-confirmed influenza, FluSurv-NET 2013–2014. Source: Centers for Disease
Control and Prevention. FluView 2013–2014 Preliminary Data as of August 23, 2014. Available at: http://gis.cdc.gov/grasp/fluview/FluHospChars.html.
Asthma includes a medical diagnosis of asthma or reactive airway disease. Cardiovascular diseases include conditions such as coronary heart disease,
cardiac valve disorders, congestive heart failure, pulmonary hypertension, and aortic stenosis; does not include hypertension disease only. Chronic lung
diseases include conditions such as chronic obstructive pulmonary disease, bronchiolitis obliterans, chronic aspiration pneumonia, and interstitial lung
disease. Immune suppression includes conditions such as immunoglobulin deficiency, leukemia, lymphoma, HIV/AIDS, and the use of immunosuppressive
medications. Metabolic disorders include conditions such as diabetes mellitus, thyroid dysfunction, adrenal insufficiency, and liver disease. Neurologic
disorders include conditions such as seizure disorders, cerebral palsy, and cognitive dysfunction. Neuromuscular disorders include conditions such as
multiple sclerosis and muscular dystrophy. Obesity was assigned if indicated in patient’s medical chart or if BMI >30 kg/m2. Pregnancy percentage
calculated by using number of female cases aged between 15 and 44 years of age as the denominator. Renal diseases include conditions such as acute or
chronic renal failure, nephrotic syndrome, glomerulonephritis, and impaired creatinine clearance. No known condition indicates that the case did not
have any known underlying medical condition indicated in medical chart at the time of hospitalization.
and Evaluation (GRADE) frame- age). The risk of adverse events tion on the basis of demonstration
work, the CDC Advisory Committee after immunization, including fe- of superior efficacy of LAIV (ages 2
on Immunization Practices (ACIP) ver, wheezing, and serious adverse through 6 years) and for program-
systematically reviewed the evi- events, appears to be similar for matic consistency (8 years is the
dence pertaining to the efficacy LAIV and IIV. Therefore, LAIV should upper age limit for receipt of 2
of live attenuated influenza vaccine be considered for healthy children doses of influenza vaccine in a pre-
(LAIV) and inactivated influenza 2 through 8 years of age who have viously unvaccinated child).
vaccine (IIV) for healthy children. no contraindications or precau- 6. The number of seasonal influenza
It concluded that there is greater tions to the intranasal vaccine. If vaccine doses to be administered
relative efficacy of LAIV as com- LAIV is not readily available, IIV in the 2014–2015 influenza season
pared with IIV against laboratory- should be used; vaccination should depends on the child’s age at the
confirmed influenza among younger not be delayed to obtain LAIV. The time of the first administered
children (based on 2 studies in- age of 8 years is selected as the dose and his or her vaccine his-
cluding children up to 6 years of upper limit for this recommenda- tory (Fig 2):
PEDIATRICS Volume 134, Number 5, November 2014 3
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015 Influenza vaccines are not li- providing influenza immunization shown higher rates of outpatient
censed for administration to for parents and other care pro- visits and antimicrobial use asso-
infants younger than 6 months. viders of children if the practice ciated with influenza-like illnesses
Children 9 years and older is acceptable to both pediatricians than older children.
need only 1 dose. and the adults who are to be vac- 8. As soon as the seasonal influenza
cinated.1 There are important medi-
Children 6 months through 8 cal liability issues and medical
vaccine is available locally, pedia-
years of age receiving the sea- tricians or vaccine administra-
record documentation require- tors should immunize HCP, notify
sonal influenza vaccine for the
ments that must be addressed parents and caregivers of vaccine
first time should receive a sec-
before a pediatrician begins immu- availability and the importance of
ond dose this season at least 4 nizing adults (see details at www.
weeks after the first dose. annual vaccination, and immu-
aapredbook.org/implementation). nize children 6 months and older
Children 6 months through 8 Pediatricians are reminded to per recommendations, especially
years of age need only 1 dose document the recommendation those at high risk of complications
of vaccine in 2014–2015 if they for adult immunization in the vul- from influenza. Health care pro-
have received it according to nerable child’s medical record. In vider endorsement plays a major
any of the following scenarios: addition, adults should still be role in vaccine uptake. A strong
✓ At least 1 dose of 2013– encouraged to have a medical
correlation exists between health
2014 seasonal influenza home and communicate their
care provider endorsement of
vaccine. immunization status to their pri-
influenza vaccine and patient ac-
✓ 2 or more doses of sea- mary care provider. Offering im-
ceptance. Prompt initiation of
sonal vaccine since July 1, munizations in the pediatric
influenza immunization and contin-
2010. practice setting would not be
uance of immunization throughout
intended to undermine the adult
✓ 2 or more doses of seasonal the influenza season, whether or
medical home model but could
influenza vaccine from any not influenza is circulating (or
serve as an additional venue for
previous season and at least has circulated) in the community,
parents and other care providers
1 clearly documented dose of are critical components of an ef-
for children to receive vaccina-
a pH1N1-containing vaccine fective immunization strategy.
tions. Immunization of close con-
(ie, any seasonal vaccine Administering the vaccine early
tacts of children at high risk of
since July 1, 2010 or a mono- during the influenza season is
influenza-related complications
valent pH1N1 vaccine during not believed to pose a significant
is intended to reduce their risk
the 2009–2010 season). risk that immunity might wane be-
of contagion (ie, “cocooning”).
Children in this age group for fore the end of the season. The
The practice of cocooning may
whom one of these conditions help protect infants younger than seasonal vaccine is not 100% effec-
is not met need 2 doses in 6 months, because they are too tive, but it still is the best strategy
2014–2015 to be adequately young to be immunized with in- available for preventing illness
primed. Vaccination should fluenza vaccine. Infants younger from influenza. It is moderately ef-
not be delayed to obtain a spe- than 6 months also can be pro- fective in reducing the risk for out-
cific product for either dose. tected through vaccination of their patient medical visits caused by
Any available, age-appropriate mothers during pregnancy, with circulating influenza viruses by
trivalent or quadrivalent vac- resulting transplacental transfer approximately one-half to three-
cine can be used; IIV and LAIV of antibodies. The risk of influenza- quarters in most people. Even
are considered interchange- associated hospitalization in healthy during seasons when the vaccine
able. A child who receives only children younger than 24 months is only moderately effective, influ-
1 of the 2 doses as a quadriva- has been shown to be greater enza vaccine has been shown to
lent formulation is likely to be than the risk of hospitalization reduce illness, antibiotic use, doc-
less primed against the addi- in previously recognized high- tor visits, time lost from work,
tional B virus. risk groups, such as older adults, hospitalizations, and deaths.
7. Pediatric offices may choose to during influenza season. Children 9. Providers should continue to offer
serve as an alternative venue for 24 through 59 months of age have vaccine until the vaccine expiration
4 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
native care sites, such as
emergency departments, to ex-
pand venues for administering
vaccine. If a child or adult re-
ceives influenza vaccine out-
side his or her medical home,
such as at a pharmacy, retail-
based clinic, or another practice,
appropriate documentation of
immunization should be pro-
vided to the patient for his or
her medical home and entered
into the state immunization reg-
istry where possible.
Concerted efforts among the
aforementioned groups, plus
vaccine manufacturers, distrib-
utors, and payers, also are
necessary to prioritize distrib-
FIGURE 2
Number of 2014–2015 seasonal influenza vaccine doses for children 6 months through 8 years of age.
ution appropriately to the pri-
For simplicity, this algorithm takes into consideration only doses of seasonal influenza vaccine received mary care office setting and
since July 1, 2010. As an alternative approach in settings where vaccination history from before July 1, patient-centered medical home
2010 is available, if a child aged 6 months through 8 years is known to have received 2 or more doses
of seasonal influenza vaccine from any previous season and at least 1 clearly documented dose of before other venues, especially
a pH1N1-containing vaccine (ie, any seasonal vaccine since July 1, 2010 or a monovalent pH1N1 vaccine when vaccine supplies are de-
during the 2009–2010 season), then the child needs only 1 dose for 2014–2015. layed or limited.
Vaccine safety, effectiveness,
date (June 30, marking the end of should collaborate to develop im- and indications must be com-
the influenza season), because in- proved strategies for planning, municated properly to the pub-
fluenza is unpredictable. Protec- communication, and administra- lic. Pediatricians and office staff
tive immune responses persist tion of vaccines. should explain the importance
throughout the influenza season, Plan to make seasonal influ- of annual influenza vaccination
which can have >1 disease peak enza vaccine easily accessi- for children and emphasize
and may extend into March or later. ble for all children. Examples when a second dose of vaccine
Although the peak of influenza ac- include alerts to families is indicated. HCP should act as
tivity in the United States tends to that vaccine is available (eg, role models by receiving in-
occur in January through March, e-mails, texts, and patient por- fluenza immunization annually
influenza activity can occur in early tals); creating walk-in influ- and recommending annual im-
fall (ie, October and November) or enza clinics; extending hours munizations to both colleagues
late spring (eg, influenza circulated beyond routine times during and patients. Influenza immu-
through the end of May during the peak vaccination periods; ad- nization programs for HCP ben-
2013–2014 season). This approach ministering influenza vaccine efit the health of employees,
also provides ample opportunity to during both well and sick vis- their patients, and members
administer a second dose of vac- its; considering how to immu- of the community.2
cine when indicated, as detailed nize parents, adult caregivers, 11. Antiviral medications also are im-
in Key Point 6 above. In addition, and siblings at the same time portant in the control of influenza
international travel may result in in the same office setting as but are not a substitute for in-
potential exposure to influenza children1; and working with fluenza immunization. The neur-
throughout the year. other institutions (eg, schools, aminidase inhibitors (NAIs) oral
10. HCP, influenza campaign organiz- child care programs, and reli- oseltamivir (Tamiflu; Roche Labo-
ers, and public health agencies gious organizations) or alter- ratories, Nutley, NJ) and inhaled
PEDIATRICS Volume 134, Number 5, November 2014 5
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015zanamivir (Relenza; GlaxoSmithKline, B viruses have circulated globally. Vac- a microinjection with a shorter needle
Research Triangle Park, NC) are cination against 1 B viral lineage con- than needles used for IM administra-
the only antiviral medications rec- fers little cross-protection against the tion. The most common adverse events
ommended for chemoprophylaxis other B viral lineage. Thus, trivalent are redness, induration, swelling, pain,
or treatment of influenza during vaccines offer limited immunity against and itching, which occur at the site of
the 2014–2015 season. Intravenous circulating influenza B strains of the administration; although all adverse
preparations of oseltamivir, zana- lineage not present in the vaccine. events occur at a slightly higher rate
mivir, and peramivir are not ap- Furthermore, in recent years it has with the IM formulation of IIV3, the rate
proved by the US Food and Drug proven difficult to predict consistently of pain was similar between ID and IM.
Administration (FDA). However, in which B lineage will predominate dur- Headache, myalgia, and malaise may
consultation with infectious dis- ing a given influenza season. Therefore, occur and tend to occur at the same
eases specialists, investigational in- a quadrivalent influenza vaccine with rate as that with the IM formulation of
travenous zanamivir should be influenza B strains of both lineages IIV3. There is no preference for IM or
considered for critically ill children, should offer greater protection. Post- ID immunization with IIV3 in people
especially those who are immuno- marketing safety and vaccine effec- 18 years or older. Therefore, pedia-
compromised or cannot tolerate or tiveness data are not yet available, tricians may choose to use either the
absorb oral or enterically admin- precluding a full risk–benefit analy- IM or ID product for their young adult
istered oseltamivir. Recent viral sis of newer versus previously available patients and for any adults they are
surveillance and resistance data products. vaccinating (ie, as part of a cocooning
indicate that the majority of cur- For the 2014–2015 season, IIVs will be strategy).
rently circulating influenza viruses available for intramuscular (IM) in- IIV4 is available in IM but not ID for-
likely to cause 2014–2015 seasonal jection in both trivalent (IIV3) and mulations. One formulation of IIV4 is
influenza in North America con- quadrivalent (IIV4) formulations. The licensed for use in children as young as
tinue to be sensitive to oseltamivir intranasally administered LAIV will be 6 months of age. In children, the most
and zanamivir. In contrast, amanta- available only in a quadrivalent formu- common injection site adverse reac-
dine and rimantadine should not lation (LAIV4). All quadrivalent vaccines tions were pain, redness, and swelling.
be used, because circulating influ- will contain the identical influenza The most common systemic adverse
enza A viruses currently have levels strains anticipated to circulate during events were drowsiness, irritability,
of resistance to these drugs, and the 2014–2015 influenza season. loss of appetite, fatigue, muscle aches,
they are not effective against influ- IIVs contain no live virus. IIV3 for- headache, arthralgia, and gastroin-
enza B viruses. Because resistance mulations are available for IM and testinal tract symptoms. These events
characteristics can change rapidly, intradermal (ID) use. The IM formula- were reported with comparable fre-
pediatricians should verify suscep- tion of IIV3 is licensed and recom- quency among participants receiving
tibility data at the start of the in- mended for children 6 months and the licensed comparator trivalent vac-
fluenza season and monitor them older and adults, including people with cines. IIV4 is an acceptable vaccine for
throughout the season. Up-to-date and without chronic medical con- people 6 months or older when oth-
information can be found on the ditions. The most common adverse erwise appropriate and may offer
AAP Web site (www.aap.org or events after IIV administration are lo- broader protection than IIV3. The rela-
www.aapredbook.org/flu), through cal injection site pain and tenderness. tive quantity of doses of IIV4 that will be
state-specific AAP chapter Web Fever may occur within 24 hours after available is not certain and likely to be
sites, or on the CDC Web site immunization in approximately 10% to limited.
(www.cdc.gov/flu/index.htm). 35% of children younger than 2 years During the 2 influenza seasons span-
but rarely in older children and adults. ning 2010–2012, there were increased
SEASONAL INFLUENZA VACCINES Mild systemic symptoms, such as reports of febrile seizures in the
Before the 2013–2014 influenza sea- nausea, lethargy, headache, muscle United States in young children who
son, only trivalent influenza vaccines aches, and chills, may occur after received IIV and the 13-valent pneu-
that included a single influenza B administration of IIV3. mococcal conjugate vaccine (PCV13)
strain were available. However, since An ID formulation of IIV3 is licensed for concomitantly, but this has not been
1985, 2 antigenically distinct lineages use in people 18 through 64 years of observed in more recent seasons. Si-
(ie, Victoria or Yamagata) of influenza age. ID vaccine administration involves multaneous administration of IIV and
6 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
PCV13 for the 2014–2015 influenza licensed IIV3 comparator vaccines. The benefits of protecting children
season continues to be recommended Although ccIIV3 is manufactured from against the known risks of influenza are
when both vaccines are indicated. virus propagated in Madin Darby ca- clear. Therefore, children should receive
LAIV4 is a quadrivalent live attenuated nine kidney cells rather than embry- any available formulation of IIV rather
influenza vaccine that is administered onated eggs, before production, seed than delaying immunization while wait-
intranasally. It is licensed by the FDA for virus is created from the World Health ing for reduced thimerosal-content or
previously healthy people 2 through Organization reference virus strains, thimerosal-free vaccines. Although some
49 years of age. The most common- which have been passaged in eggs. formulations of IIV contain only a trace
ly reported reactions in children However, egg protein is not detectable amount of thimerosal, certain types can
were runny nose or nasal congestion, in the final vaccine, and egg allergy is be obtained thimerosal free. LAIV4 does
headache, decreased activity or leth- not mentioned as a contraindication not contain thimerosal. Vaccine manufac-
argy, and sore throat. LAIV4 should not in the package insert. Other contra- turers are delivering increasing amounts
be administered to people with notable indications to vaccine delivery are of thimerosal-free influenza vaccine each
nasal congestion that would impede similar to those for other IIVs. The year.
vaccine delivery. The safety of LAIV in most common solicited adverse reac-
people with a history of asthma, tions included injection site pain, er- INFLUENZA VACCINES AND EGG
diabetes mellitus, or other high-risk ythema at the injection site, headache, ALLERGY
medical conditions associated with an fatigue, myalgia, and malaise.
Although most IIV and LAIV vaccines
elevated risk of complications from RIV3 is a recombinant baculovirus– are produced in eggs and contain
influenza (see Contraindications and expressed hemagglutinin vaccine pro- measurable amounts of egg protein,
Precautions) has not been established. duced in cell culture. It is indicated recent data have shown that IIV ad-
In a postlicensure surveillance of LAIV for people 18 through 49 years of age ministered in a single, age-appropriate
over 7 seasons, the Vaccine Adverse and is administered via IM injection. dose is well tolerated by most recipi-
Event Reporting System (VAERS), jointly The most frequently reported adverse ents with a history of egg allergy. More
sponsored by the FDA and CDC, did not events were pain, headache, myalgia, conservative approaches in children
identify any new or unexpected safety and fatigue. There are no egg proteins with a history of egg allergy, such as
concerns, although there were reports in this version of influenza vaccine. skin testing or a 2-step graded chal-
of use of LAIV in people with a contra- Tables 1 and 2 summarize information lenge, no longer are recommended. No
indication or precaution. The use of LAIV on the types of 2014–2015 seasonal data have been published on the safety
in young children with chronic medical influenza vaccines licensed for im- of administering LAIV to egg-allergic
conditions, including asthma, has been munization of children and adults. It is recipients.
implemented outside the United States, likely that more than 1 type or brand As a precaution, pediatricians should
but the vaccine is not licensed for these of vaccine may be appropriate for continue to determine whether the
indications in the United States. vaccine recipients. However, vaccina- presumed egg allergy is based on
Two trivalent influenza vaccines man- tion should not be delayed to obtain a mild (ie, hives alone) or severe re-
ufactured using technologies that do a specific product. action (ie, anaphylaxis involving car-
not use eggs will also be available for A large body of scientific evidence de- diovascular changes, respiratory or
people 18 years or older during the monstrates that thimerosal-containing gastrointestinal tract symptoms, or
2014–2015 season: cell culture–based vaccines are not associated with ele- reactions that necessitate the use of
inactivated influenza vaccine (ccIIV3) vated risk of autism spectrum dis- epinephrine). Pediatricians should
and recombinant influenza vaccine orders in children. Therefore, the AAP consult with an allergist for children
(RIV3). These manufacturing methods extends its strongest support to the with a history of severe reaction. Most
would probably permit a more rapid recent World Health Organization rec- vaccine administration to patients with
scale-up of vaccine production when ommendations to retain the use of egg allergy can occur without the need
needed, such as during a pandemic. thimerosal in the global vaccine supply. for referral. Data indicate that only
ccIIV3 is a trivalent cell culture–based Some people may still raise concerns approximately 1% of children have
inactivated influenza vaccine indicated about the minute amounts of thimer- immunoglobulin E–mediated sensitiv-
for people 18 years or older, admin- osal in IIV vaccines, and in some states ity to egg, and of those, a rare mi-
istered as an IM injection. ccIIV3 has there is a legislated restriction on the nority have a severe allergy. The Joint
comparable immunogenicity to US- use of thimerosal-containing vaccines. Task Force on Practice Parameters,
PEDIATRICS Volume 134, Number 5, November 2014 7
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015TABLE 1 Recommended Seasonal Influenza Vaccines for Different Age Groups: United States, 2014–2015 Influenza Season
Vaccine Trade Name Manufacturer Presentation Thimerosal Mercury Age Group
Content (μg of Hg per
0.5-mL dose)
Inactivated
IIV3 Fluzone Sanofi Pasteur 0.25-mL prefilled syringe 0 6–35 mo
0.5-mL prefilled syringe 0 ≥36 mo
0.5-mL vial 0 ≥36 mo
5.0-mL multidose vial 25 ≥6 mo
IIV3 Fluzone Intradermal Sanofi Pasteur 0.1-mL prefilled microinjection 0 18–64 y
IIV3 Fluzone HD Sanofi Pasteur 0.5-mL prefilled syringe 0 ≥65 y
IIV3 Fluvirin Novartis 0.5-mL prefilled syringe ≤1.0 ≥4 y
5.0-mL multidose vial 25 ≥4 y
IIV3 Fluarix GlaxoSmithKline 0.5-mL prefilled syringe 0 ≥36 mo
IIV3 FluLaval ID Biomedical Corporation of 5.0-mL multidose vial 25 ≥36 mo
Quebec (distributed by
GlaxoSmithKline)
IIV3 Afluria CSL Biotherapies 0.5-mL prefilled syringe 0 ≥9 ya
(distributed by Merck)
5-mL multidose vial 24.5 ≥9 ya
ccIIV3 Flucelvax Novartis Vaccines 0.5-mL prefilled syringe 0 ≥18 y
IIV4 Fluzone Quadrivalent Sanofi Pasteur 0.25-mL prefilled syringe 0 6–35 mo
0.5-mL prefilled syringe 0 ≥36 mo
0.5-mL vial 0 ≥36 mo
IIV4 Fluarix Quadrivalent GlaxoSmithKline 0.5-mL prefilled syringe 0 ≥36 mo
IIV4 FluLaval Quadrivalent ID Biomedical Corporation of 5.0-mL multidose vial 25 ≥36 mo
Quebec (distributed by
GlaxoSmithKline)
Recombinant
RIV3 FluBlok Protein Sciences 0.5-mL vial 0 18–49y
Live attenuated
LAIV4 FluMist Quadrivalent MedImmune 0.2-mL sprayer 0 2–49 y
Sources: American Academy of Pediatrics, Committee on Infectious Diseases. Recommendations for prevention and control of influenza in children, 2013–2014. Pediatrics. 2013;132(4):
e1089–e1104; and Centers for Disease Control and Prevention. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization
Practices (ACIP)—United States, 2014–2015 influenza season. MMWR Recomm Rep. 2014;63(32):691–697.
a
Age indication per package insert is ≥5 y; however, the Advisory Committee on Immunization Practices recommends Afluria not be used in children 6 mo through 8 y of age because of
febrile reactions reported in this age group. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child 5 through 8 y of age who has a medical
condition that increases the child’s risk of influenza complications, Afluria can be used; however, pediatricians should discuss with the parents or caregivers the benefits and risks of
influenza vaccination with Afluria before administering this vaccine.
representing the American Academy of Appropriate resuscitative equip- severity who are 18 through 49 years
Allergy, Asthma & Immunology (AAAAI) ment must be readily available. 3 of age and do not have other contra-
and the American College of Allergy, The vaccine recipient should be ob- indications. However, vaccination of pa-
Asthma & Immunology (ACAAI), recently served in the office for 30 minutes tients with mild egg allergy should
published an updated recommenda- not be delayed if RIV3 or ccIIV3 is not
after immunization, the usual observa-
tion that special precautions regarding available. Instead, any licensed, age-
tion time for receiving immunotherapy.
medical setting and waiting periods af- appropriate IIV should be used.
ter administration of IIV to egg-allergic Providers may consider use of ccIIV3
recipients beyond those recommended or RIV3 vaccines produced via non–
egg-based technologies for patients VACCINE STORAGE AND
for any vaccine are not warranted. This
18 years or older with egg allergy in ADMINISTRATION
concept has not been universally ac-
cepted by all allergists, so the AAP rec- settings in which these vaccines are The AAP Storage and Handling Tip
ommendation has not changed. available and otherwise age appropri- Sheet provides resources for practices
Standard immunization practice should ate. ccIIV3, which does contain trace to develop comprehensive vaccine
include the ability to respond to acute amounts of ovalbumin, should be ad- management protocols to keep the
hypersensitivity reactions. Therefore, ministered according to the guidance temperature for vaccine storage con-
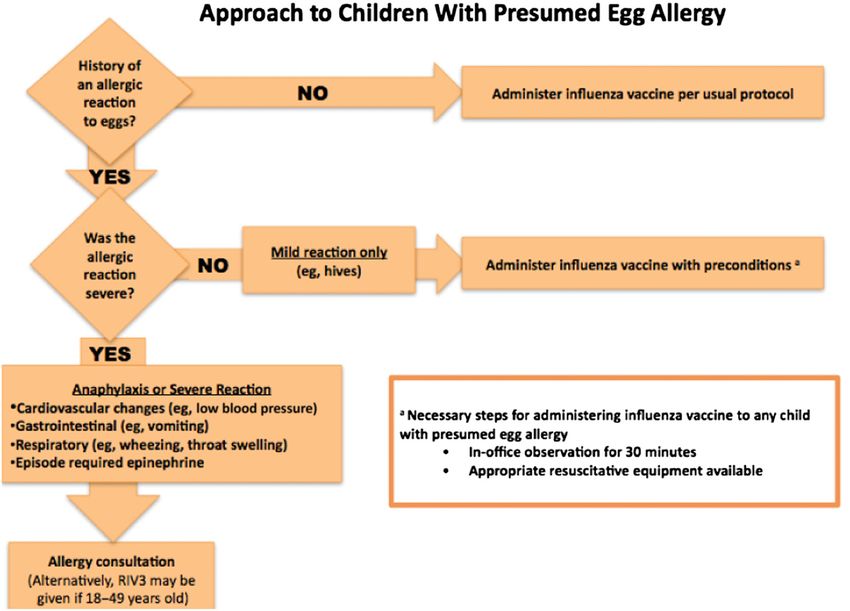
influenza vaccine should be given to for other IIVs (Fig 3). RIV3, which con- stant during a power failure or other
children with egg allergy with the tains no ovalbumin, may be adminis- disaster (www2.aap.org/immunization/
following preconditions (Fig 3): tered to people with egg allergy of any pediatricians/pdf/DisasterPlanning.pdf).
8 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 2 LAIV4 Compared With IIV3 and IIV4
Vaccine Characteristic LAIV4 IIV3 IIV4
Route of administration Intranasal spray Intramuscular or Intramuscular injectiona
intradermal injectiona
Type of vaccine Live virus Killed virus Killed virus
Product Attenuated, cold adapted Inactivated subvirion Inactivated subvirion or
or surface antigen surface antigen
No. of included virus strains 4 (2 influenza A, 3 (2 influenza A, 1 influenza B) 4 (2 influenza A,
2 influenza B) 2 influenza B)
Vaccine virus strains updated Annually Annually Annually
Frequency of administrationb Annually Annually Annually
Approved age groups All healthy people aged All people aged ≥6 mo All people aged ≥6 mo
2–49 y (ID 18–64 y)
Interval between 2 doses in children 4 wk 4 wk 4 wk
Can be given to people with medical risk factors for influenza- Not preferred Yes Yes
related complications?
Can be given to children with asthma or children aged 2–4 y Noc Yes Yes
with wheezing in the previous year?
Can be simultaneously administered with other vaccines? Yesd Yesd Yesd
If not simultaneously administered, can be administered within No, recommended to Yes Yes
4 wk of another live vaccine? space 4 wk apart
Can be administered within 4 wk of an inactivated vaccine? Yes Yes Yes
Sources: American Academy of Pediatrics, Committee on Infectious Diseases. Recommendations for prevention and control of influenza in children, 2013–2014. Pediatrics. 2013;132(4):
e1089–e1104; and Centers for Disease Control and Prevention. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization
Practices (ACIP)—United States, 2014–2015 influenza season. MMWR Recomm Rep. 2014;63(32):691–697.
a
The preferred site of IIV intramuscular injection for infants and young children is the anterolateral aspect of the thigh.
b
See Fig 2 for decision algorithm to determine number of doses of seasonal influenza vaccine recommended for children during the 2014–2015 influenza season.
c
LAIV4 is not recommended for children with a history of asthma. In the 2- through 4-y age group, there are children who have a history of wheezing with respiratory illnesses in whom
reactive airway disease is diagnosed and in whom asthma may later be diagnosed. Therefore, because of the potential for increased wheezing after immunization, children 2 through 4 y
of age with recurrent wheezing or a wheezing episode in the previous 12 mo should not receive LAIV4. When offering LAIV4 to children in this age group, a pediatrician should screen those
who might be at higher risk of asthma by asking the parents or guardians of 2-, 3-, and 4-y-olds (24- through 59-mo-olds) the question, “In the previous 12 months, has a health care
professional ever told you that your child had wheezing?” If the parents answer “yes” to this question, LAIV4 is not recommended for these children.
d
LAIV4 coadministration has been evaluated systematically only among children 12–15 mo of age with measles–mumps–rubella and varicella vaccines. IIV coadministration has been
evaluated systematically only among adults with pneumococcal polysaccharide and zoster vaccines.
Any of the influenza vaccines can be preferably over the deltoid muscle and CURRENT RECOMMENDATIONS
administered at the same visit with all only using the device included in the Seasonal influenza immunization is rec-
other recommended routine vaccines. vaccine package. Vaccine is supplied in
ommended for all children 6 months and
a single-dose, prefilled microinjection
older. LAIV should be considered for
Intramuscular Vaccine system (0.1 mL) for adults. The pack-
healthy children 2 through 8 years of age
The IM formulation of IIV is shipped age insert should be reviewed for full
who have no contraindications or pre-
and stored at 2°C to 8°C (35°F–46°F). It administration details of this product.
cautions to the intranasal vaccine. This is
is administered intramuscularly into
Live Attenuated (Intranasal) based on a GRADE analysis done by the
the anterolateral thigh of infants and
Vaccine CDC, which concluded that there is
young children and into the deltoid
greater relative efficacy of LAIV as
muscle of older children and adults. The cold-adapted, temperature-sensitive
compared with IIV against laboratory-
The volume of vaccine is age depen- LAIV4 formulation currently licensed in
dent; infants and toddlers 6 months confirmed influenza among younger
the United States must be shipped and
through 35 months of age should re- children. If LAIV is not readily available, IIV
stored at 2°C to 8°C (35°F–46°F) and
ceive a dose of 0.25 mL, and all people administered intranasally in a prefilled, should be used; vaccination should not
3 years (36 months) and older should single-use sprayer containing 0.2 mL of be delayed to obtain LAIV. Particular fo-
receive 0.5 mL/dose. vaccine. A removable dose divider clip cus should be on the administration of
is attached to the sprayer to administer IIV for all children and adolescents with
Intradermal Vaccine 0.1 mL separately into each nostril. Af- underlying medical conditions associated
The ID formulation of IIV also is shipped ter administration of any live virus with an elevated risk of complications
and stored at 2°C to 8°C (35°F–46°F). It vaccine, at least 4 weeks should pass from influenza, including the following:
is administered intradermally only to before another live virus vaccine is ad- Asthma or other chronic pulmonary
people 18 through 64 years of age, ministered. diseases, including cystic fibrosis
PEDIATRICS Volume 134, Number 5, November 2014 9
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015FIGURE 3
Precautions for administering IIV to presumed egg-allergic children.
Hemodynamically significant car- rodevelopmental disorders, spinal is in the postpartum period, or is
diac disease cord injuries, seizure disorders, or breastfeeding during the influ-
Immunosuppressive disorders or neuromuscular abnormalities enza season. Studies have shown
therapy Although universal immunization for all that infants born to immunized
women have better influenza-related
HIV infection people 6 months and older is recom-
health outcomes. However, accord-
mended for the 2014–2015 influenza
Sickle cell anemia and other hemo- ing to Internet panel surveys con-
season, particular immunization ef-
globinopathies ducted by the CDC, only 51% of
forts with either IIV or LAIV should be
Diseases that necessitate long- made for the following groups to pre- pregnant women reported receiv-
term aspirin therapy, including ju- ing an influenza vaccine during the
vent transmission of influenza to those
venile idiopathic arthritis or Kawasaki 2012–2013 season, even though
at risk, unless contraindicated:
disease both pregnant women and their
Household contacts and out-of-home
Chronic renal dysfunction care providers of children younger
infants are at higher risk of com-
plications. In addition, data from
Chronic metabolic disease, includ- than 5 years and at-risk children of some studies suggest that in-
ing diabetes mellitus all ages (healthy contacts 2 through fluenza vaccination in pregnancy
Any condition that can compro- 49 years of age can receive either IIV may decrease the risk of preterm
mise respiratory function or han- or LAIV). birth and of giving birth to infants
dling of secretions or can increase Any woman who is pregnant or who are small for gestational age.
the risk of aspiration, such as neu- considering pregnancy (IIV only), Pregnant women can receive the
10 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
influenza vaccine safely during episode in the previous 12 months has an influenza illness for which
any trimester. because of the potential for in- antiviral agents are appropriate, the
Children and adolescents of Amer- creased wheezing after immuniza- antiviral agents should be given. Re-
ican Indian or Alaska Native heri- tion. In this age range, many immunization may be indicated be-
tage. children have a history of wheezing cause of the potential effects of
with respiratory tract illnesses and antiviral medications on LAIV rep-
HCP or health care volunteers. De-
are eventually diagnosed with lication and immunogenicity.
spite the AAP recommendation for
asthma. Therefore, when offering
mandatory influenza immunization
LAIV to children 24 through 59 Children for Whom IIV Is Preferred
for all HCP,2 many remain unvacci-
nated. As of November 2013, the
months of age, the pediatrician Children with chronic underlying
should screen them by asking the medical conditions, including meta-
CDC estimated that only 62.9% of
parent or guardian, “In the previous bolic disease, diabetes mellitus,
HCP received the seasonal influ-
12 months, has a health care pro- other chronic disorders of the pul-
enza vaccine. The AAP recommends
fessional ever told you that your monary or cardiovascular systems,
mandatory vaccination of HCP, be-
child had wheezing?” If a parent renal dysfunction, or hemoglobinop-
cause HCP frequently come into
answers “yes” to this question, LAIV athies. The safety of LAIV in these
contact with patients at high risk
is not recommended for the child. populations has not been estab-
of influenza illness in their clinical IIV would be recommended for the
settings. lished. These conditions are not
child to whom LAIV is not given. contraindications but are listed un-
Close contacts of immunosuppressed Children with the diagnosis of der the “Warnings and Precautions”
people. asthma. section of the LAIV package insert. A
Children with a history of egg allergy. precaution is a condition in a recip-
CONTRAINDICATIONS AND
PRECAUTIONS Children who have received other ient that might increase the risk or
live virus vaccines within the last 4 seriousness of an adverse reaction
Minor illnesses, with or without fever, weeks; however, other live virus or complicate making another diag-
are not contraindications to the use of vaccines can be given on the same nosis because of a possible vaccine-
influenza vaccines, particularly among day as LAIV. related reaction. A precaution also
children with mild upper respiratory may exist for conditions that might
Children who have known or sus-
infection symptoms or allergic rhinitis. compromise the ability of the vac-
pected immunodeficiency disease
cine to produce immunity. Vaccina-
or who are receiving immunosup-
Children Who Should Not Be tion may be recommended in the
pressive or immunomodulatory ther-
Vaccinated With IIV presence of a precaution if the ben-
apies.
Infants younger than 6 months. Children who are receiving aspirin
efit of protection from the vaccine
Children who have a moderate to or other salicylates.
outweighs any risk.
severe febrile illness, on the basis IIV is the vaccine of choice for anyone in
Any woman who is pregnant or close contact with a subset of severely
of clinical judgment of the clini-
considering pregnancy. immunocompromised people (ie, those
cian.
Children with any condition that in a protected environment). IIV is
Children Who Should Not Be can compromise respiratory func- preferred over LAIV for contacts of
Vaccinated With LAIV tion or handling of secretions or severely immunocompromised people
can increase the risk for aspira-
Children younger than 2 years. tion, such as neurodevelopmental
because of the theoretical risk of in-
fection attributable to LAIV strain in an
Children who have a moderate to disorders, spinal cord injuries, sei- immunocompromised contact of an
severe febrile illness. zure disorders, or neuromuscular LAIV-immunized person. Available data
Children with an amount of nasal abnormalities. indicate a very low risk of transmission
congestion that would notably im- Children taking an influenza antivi- of the virus in both children and adults
pede vaccine delivery. ral medication should not receive vaccinated with LAIV. HCP immunized
Children 2 through 4 years of age LAIV until 48 hours after stopping with LAIV may continue to work in most
with a history of recurrent wheezing the influenza antiviral therapy. If units of a hospital, including the NICU
or a medically attended wheezing a child recently received LAIV but and general oncology wards, using
PEDIATRICS Volume 134, Number 5, November 2014 11
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015standard infection control techniques. of this guideline in computer systems SF (sugar-free) by retail pharma-
As a precautionary measure, people and quality measurement efforts. This cies to a final concentration of 6
recently vaccinated with LAIV should document is available at www2.aap. mg/mL (Table 3).
restrict contact with severely immu- org/informatics/PPI.html. Continuous monitoring of the epi-
nocompromised patients for up to 28 demiology, change in severity, and
days after immunization, although USE OF ANTIVIRAL MEDICATIONS resistance patterns of influenza
there have been no reports of LAIV strains may lead to new guidance.
Oral oseltamivir remains the antiviral
transmission from a vaccinated person
drug of choice for the management of Treatment should be offered for:
to an immunocompromised person. In
the theoretical scenario in which
influenza infections. Inhaled zanamivir Any child hospitalized with pre-
is an equally acceptable alterna- sumed influenza or with severe,
symptomatic LAIV infection develops in
tive but is more difficult to admin- complicated, or progressive illness
an immunocompromised host, oselta-
ister. Antiviral resistance can emerge attributable to influenza, regardless
mivir or zanamivir could be prescribed,
quickly between seasons. If local or of influenza immunization status or
because LAIV strains are susceptible to
national influenza surveillance data whether onset of illness occurred
these antiviral medications.
indicate a predominance of a partic- >48 hours before admission.
ular influenza strain with a known
SURVEILLANCE Influenza infection of any severity in
antiviral susceptibility profile, then
children at high risk of complica-
Information about influenza surveil- empirical treatment can be directed
tions of influenza infection (Table 4),
lance is available through the CDC toward that strain. For example, all
such as children younger than 2
Voice Information System (influenza the influenza A (H3N2) and influenza B
years.
update, 888-232-3228) or at www.cdc. viruses tested since October 1, 2013
gov/flu/index.htm. Although current were sensitive to oseltamivir and Treatment should be considered for:
influenza season data on circulating zanamivir during the 2013–2014 in- Any otherwise healthy child with
strains do not necessarily predict fluenza season. Among the pH1N1 influenza infection for whom a de-
which and in what proportion strains viruses tested for resistance, only crease in duration of clinical symp-
will circulate in the subsequent sea- 1.2% were found to be resistant to toms is felt to be warranted by his
son, it is instructive to be aware of oseltamivir, and none were found to or her pediatrician. The greatest
2013–2014 influenza surveillance data be resistant to zanamivir. In contrast, impact on outcome will occur if
and use them as a guide to empirical high levels of resistance to amanta- treatment can be initiated within
therapy until current seasonal data dine and rimantadine exist, so these 48 hours of illness onset but still
are available from the CDC. Informa- drugs should not be used in the up- should be considered if later in the
tion is posted weekly on the CDC coming season unless resistance course of illness.
Web site (www.cdc.gov/flu/weekly/ patterns change significantly. Reviews of available studies by the
fluactivity.htm). Current treatment guidelines for CDC, the World Health Organization,
antiviral medications (Table 3) are and independent investigators have
VACCINE IMPLEMENTATION applicable to both infants and chil- consistently found that timely oselta-
These updated recommendations for dren with suspected influenza when mivir treatment can reduce the risks
prevention and control of influenza in known virus strains are circulating of complications, including those re-
children will have operational and in the community or when infants sulting in hospitalization and death.
fiscal effects on pediatric practice. or children are confirmed to have Although a 2012 Cochrane review of
Therefore, the AAP has developed seasonal influenza. studies primarily in outpatient settings
implementation guidance on supply, Oseltamivir is available in capsule suggested that oseltamivir may not be
payment, coding, and liability issues; and oral suspension formulations. effective in preventing complications
these documents can be found at The commercially manufactured liq- or hospitalizations from influenza, its
www.aapredbook.org/implementation. uid formulation has a concentration authors correctly pointed out that the
In addition, the AAP’s Partnership for of 6 mg/mL. If the commercially data reviewed were not always com-
Policy Implementation has developed manufactured oral suspension is plete, were analyzed in a variety of
a series of definitions using accepted not available, the capsule may be treated populations, and used a num-
health information technology stand- opened and the contents mixed ber of clinical trial designs. In addition,
ards to assist in the implementation with simple syrup or Oral-Sweet a recently revised 2014 Cochrane
12 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Downloaded from pediatrics.aappublications.org by guest on October 12, 2015FROM THE AMERICAN ACADEMY OF PEDIATRICS
review of NAIs for influenza further to assess the effect on severe out- been shown to provide some benefit
evaluated published and previously comes such as hospitalizations or and should be strongly considered. In
unpublished data from randomized deaths. previous years, the use of double-dose
clinical trials largely in healthy out- Importantly, treatment with oseltamivir oseltamivir, particularly for those hos-
patients with mild illness. Unlike other for children with presumed serious, pitalized with severe illness caused by
analyses of the efficacy of antiviral complicated, or progressive disease, pH1N1, was believed to provide better
drugs, this Cochrane analysis included irrespective of influenza immunization outcomes. However, recently published
both influenza virus–infected and status or even whether illness began data from a randomized, prospective
noninfected people with influenza-like greater than 48 hours before admis- trial with 75% of subjects younger than
illness. Given the specific antiviral sion, continues to be recommended by 15 years documented no benefit of
activity of NAIs against influenza viru- the AAP, CDC, and Infectious Diseases double-dose therapy over standard-
ses, this analytic approach under- Society of America (IDSA) (http://www. dose therapy.
estimates the treatment efficacy of idsociety.org/Influenza_Statement.aspx). Dosages for antiviral agents for both
NAIs and their valuable role in helping Earlier treatment provides better clini- treatment and chemoprophylaxis in
to lessen complications in those at cal responses. However, treatment after children can be found in Table 3 and
high risk for them, including hospi- 48 hours of symptoms in adults and on the CDC Web site (http://www.cdc.
talized patients. Furthermore, this re- children with moderate to severe dis- gov/flu/professionals/antivirals/index.
view of outpatients was not designed ease or with progressive disease has htm). Children younger than 2 years
TABLE 3 Recommended Dosage and Schedule of Influenza Antiviral Medications for Treatment and Chemoprophylaxis for the 2014–2015 Influenza
Season: United States
Medication Treatment (5 d) Chemoprophylaxis (10 d)
Oseltamivira
Adults 75 mg twice daily 75 mg once daily
Children ≥12 mo
Body wt
≤15 kg (≤33 lb) 30 mg twice daily 30 mg once daily
>15–23 kg (33–51 lb) 45 mg twice daily 45 mg once daily
>23–40 kg (>51–88 lb) 60 mg twice daily 60 mg once daily
>40 kg (>88 lb) 75 mg twice daily 75 mg once daily
Infants 9–11 mob 3.5 mg/kg per dose twice daily 3.5 mg/kg per dose once daily
Term infants 0–8 mob 3 mg/kg per dose twice daily 3 mg/kg per dose once daily for infants 3–8 mo; not
recommended for infantsYou can also read