Restructure Consultation Paper - Executive and Senior Management Structure St George Hospital and Health Service
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
T21/23078
Restructure Consultation Paper
Executive and Senior Management Structure
St George Hospital and Health Service
May 2021
Comments or feedback on this proposal can be submitted in writing
to Maria Buric, A/Principal HR Advisor, St George Hospital
via email to:
Maria.Buric@health.nsw.gov.au
By 1 June 2021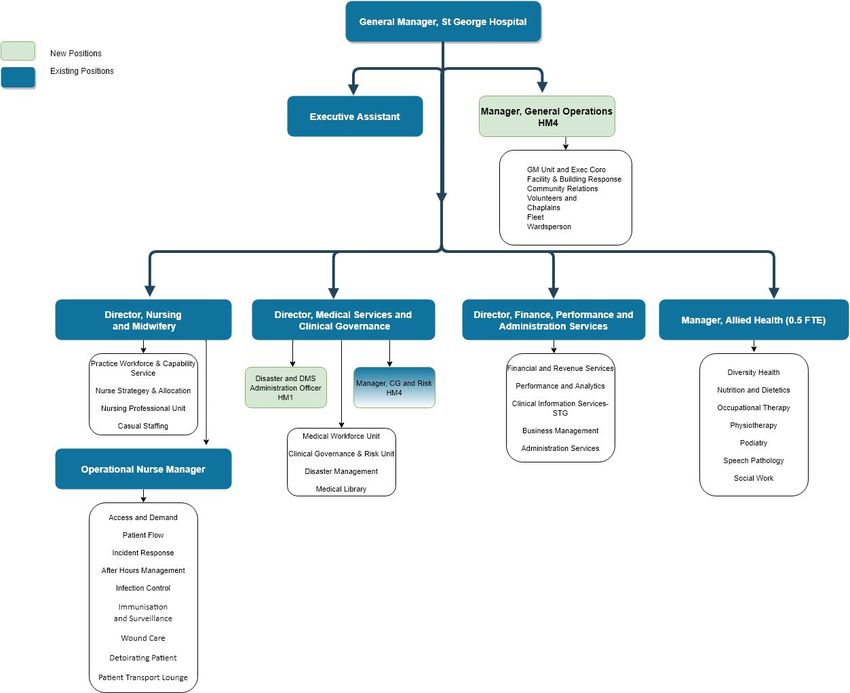
TABLE OF CONTENTS
1. Overview of St George Hospital & Health Service
1.1 Introduction
1.2 Current Organisational Structure
TAB A - Current Executive and Senior Management Structure
TAB B - Current Service Line Structure
TAB C - Current Structure of Nursing & Midwifery Services Across SGH
2. Case for Change
3. Proposed Executive & Senior Management Structure
3.1 TAB D - Proposed Organisation Chart
3.2 TAB E - Proposed Executive Organisation Chart
3.3 TAB F - Proposed Executive & Senior Management Organisation Chart
3.4 TAB G - Proposed Divisional Chart
3.5 TAB H - Proposed Structure of Nursing & Midwifery Services across
SGH
3.6 TAB I - Proposed Structure outlining LHD Service Alignment
4. Proposed Structure Detailed Explanation
4.1 The Co-Director Model
4.2 Business and Administrative Support
4.3 Clinical Governance & Risk Unit (formally known as, Clinical Practice
Improvement Unit)
4.4 Director of Nursing and Midwifery
4.5 Re-naming ‘Deputy Director of Nursing and Midwifery Services’ to
‘Operational Nurse Manager’
4.6 Casual Staffing Office, Nurse Manager
4.7 Allied Health Manager
4.8 Disaster and DMS & Clinical Governance Administration Officer
4.9 Manager, General Operations
5. Summary of all proposed changes
5.1 Current positions to be deleted
5.2 Proposed new positions
5.3 Proposed new reporting lines
6. Consultation
7. The recruitment and matching process
8. Employee Assistance Program
9. Restructure Timeframe
Appendix 1 Proposed Position Descriptions
Divisional Co- Director
Medical Co-Director
Clinical Services Manager
Divisional Administration Officer
Disaster and DMS & CG Administration Officer
Manager, General Operations
Page 2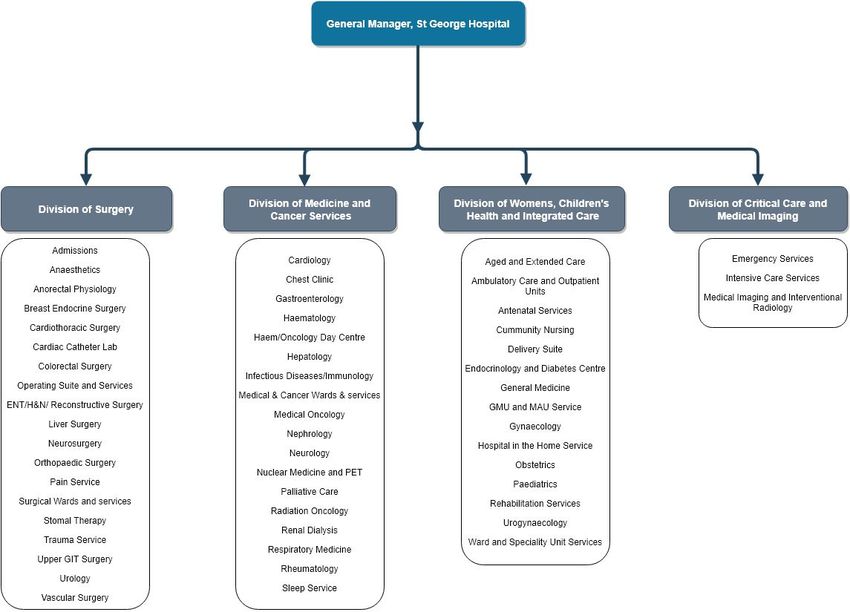
1. Overview of St George Hospital & Health Service
1.1 Introduction
St George Hospital and Health Service (SGH) is part of South Eastern Sydney Local
Health District (SESLHD) and is located in the southern suburb of Sydney, Kogarah.
The hospital employs approximately 4,000 staff across the full range of health care
and support service professions and has a bed base of 650.
The hospital is an A1 major teaching hospital affiliated with the University of NSW
and is a tertiary referral centre. SGH provides a comprehensive range of specialist
inpatient and community services, including but not limited to Critical Care, Surgery,
Cancer Care, Medical, Women’s and Children’s Health, Community Health, Medical
Imaging, Bone Marrow Transplant, Brachytherapy and Trauma.
The hospital services an area bounded by Botany Bay, Cooks River in the North,
Georges River in the South and Salt Pan Creek in the West. In addition, the hospital
has a number of well recognised centres of excellence providing State-wide services
to the population of NSW.
SGH is a Level 1 Trauma Centre and has one of the busiest Emergency
Departments in the State.
SGH began operation in November 1894, became a teaching hospital in 1964 and
was recognised as a world class tertiary teaching hospital in the late 1980s.
SGH proudly provides an opportunity for health and medical researchers to conduct
research that will directly service the needs of patients both locally and extending to
national and international populations.
In 2019, the hospital celebrated its 125th anniversary.
1.2 Current Organisational Structure
The current structure has all of the clinical services and departments at St George
Hospital split into two main service lines. They are:
- Surgery, Critical Care and Women’s and Children’s; as well as
- Medicine, Cancer and Aged and Extended Care
Each Service Line is managed by an Operational Manager (HM5) reporting to the
General Manager. In addition each of the individual clinical groups is managed by a
Nurse Manager (NM) (5x NM6 and 1x NM4), one per service. All of the NMs report
both operationally and professionally to the Director, Nursing and Midwifery.
There are also two Medical Leads for each of the current service lines. The Medical
Leads report to the Director, Medical Services and are Senior Staff Specialists.
Page 3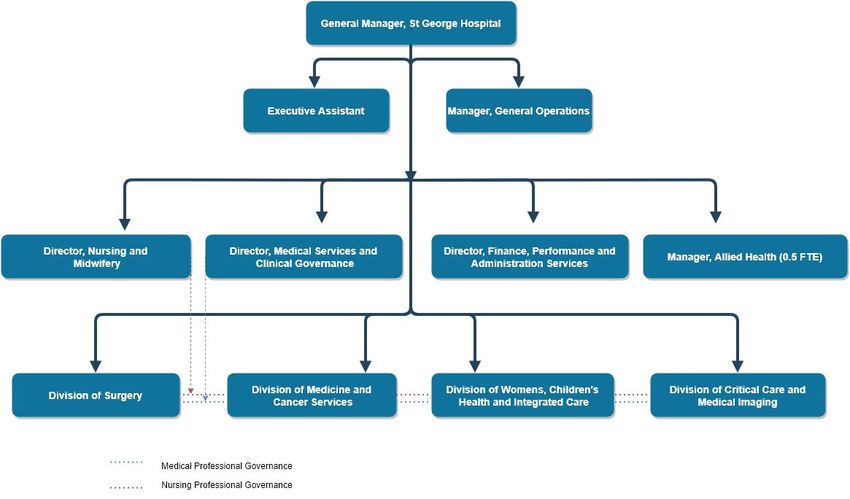
In addition, the part time Allied Health Manager (0.5FTE) reports to the General
Manager and has responsibility for the areas of Medical Imaging, Pharmacy, Clinical
Information, as well as Allied Health services of Physiotherapy, Occupational
Therapy, Social Work, Nutrition and Dietetics, Speech Pathology and Podiatry.
The Clinical Practice Improvement Unit (CPIU) is staffed with a team of Patient
Safety Manager’s, Quality Manager, Complaints Manager and Documents
Governance positions which report individually to the General Manager.
The structure has largely been in place since 2015, when the then, St George and
The Sutherland Hospital and Health Services Sector were separated to support
facility based management.
TAB A - Current Executive and Senior Management Structure
TAB B - Current Services Line Structure
TAB C - Current Structure of Nursing & Midwifery Services across SGH
Page 4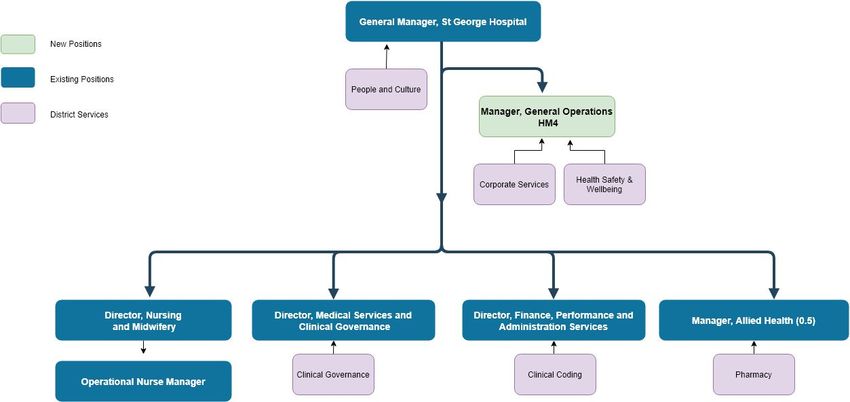
TAB A - Current Executive and Senior Management Structure
General Manager
St George Hospital & Health
Service
Senior Executive
Executive Assistant
Officer
HM1
HM3
Director, Medical Director, Nursing & Manager, Allied
Operations Manager Operations Manager Director, Finance
Services Midwifery Services Health CPIU
HM5 HM5 SnrSS HM5
NM9 0.4 FTE, AHP 7.3
Deputy Director, Complaints/Medico
Critical Care Medicine Medical Workforce Nursing & Midwifery Professor of Nursing Legal Manager
Nurse Managers Pharmacy
Unit Services Research
Surgery Cancer Financial Services Medical Imaging NM3/HM3/AHP
NM7 Surgery, Trauma, and
Women’s & Aged & Senior Medical Anaesthetics NM6 Revenue
Officers Clinical Information
Children’s Extended Care Hospital
Critical Care, NM6 Medical Library
Junior Medical Performance Patient Safety
Officers Women’s & Children’s Analytics Business Physiotherapy Managers
NM6 Management Speech Pathology 2.5 FTE HM3
Admin Supervisor Medicine, NM6
Business Manager Business Manager Social Work
2 FTE, AO6 Aged & Extended Care
1.4 FTE, HM3 1.5 FTE, HM 3 Nutrition &
NM6
Dietetics Quality Manager
Cancer, NM4
Orthotics 0.74 FTE HM3
Workforce, Strategy &
Allocation, NM5 Occupational
Admin Officer 1 Therapy
FTE, AO5 Executive Support,
NM3
Practice & Workforce
Capabilities, NM5 Business Manager
0.5 FTE, HM 3
Admin Officer
2.26 FTE, AO5
SGH Executive and Management Restructure Consultation Paper Page 5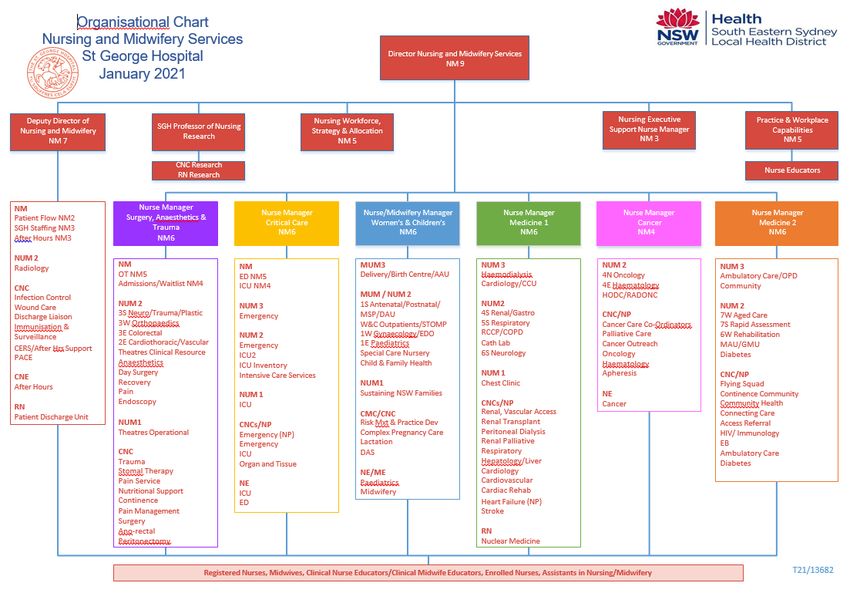
TAB B - Current Services Line Structure
SGH Executive and Management Restructure Consultation Paper Page 6
TAB C - Current Structure of Nursing & Midwifery Services across SGH
SGH Executive and Management Restructure Consultation Paper Page 7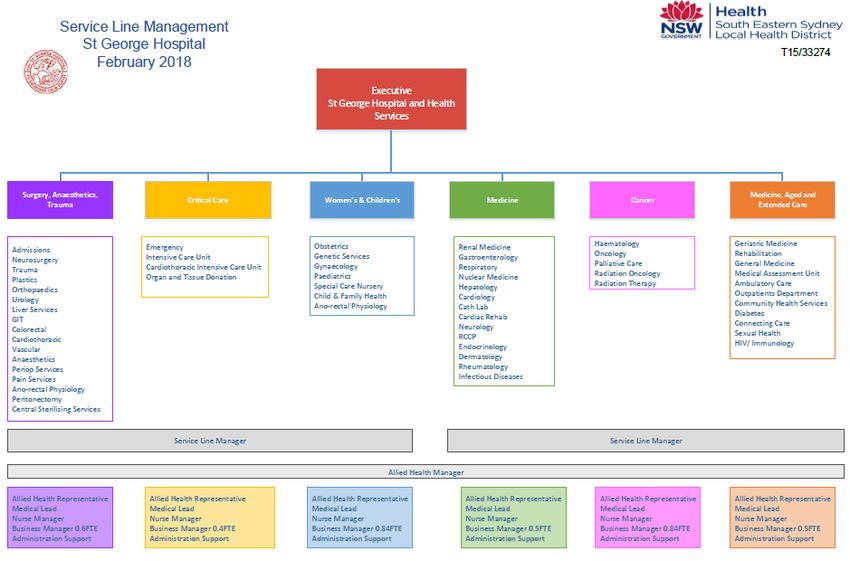
2. Case for change
The SESLHD Journey to Excellence Strategy 2018 - 2021 identifies that the
transformational journey will build local capacity and capability with a vision of improving
systems and support for value-based change and improvement to meet the growing
demands of the community and deliver safe, quality and compassionate patient care. It
proposes considerable changes for health service provision with more sustainable
options, preventative measures and earlier interventions within the community.
To meet the needs of the community both now and into the future, the existing structure
will be realigned to ensure improved congruency between craft groups and service
delivery models.
The goal of managing an organisation as a more refined portfolio of services is to devolve
management and ownership of service delivery models and operations to those subject
matter experts who have the capability, information and patient relationships to enable
the hospital to fulfil its overall objectives.
Successful transformation will require an integrated approach towards clinical, operational
and financial objectives and outcomes. It will provide clinicians with greater autonomy,
accountability and the ability to make their own decisions around how to improve service
delivery and performance and to implement changes that will best serve their patients,
their staff and the organisation as a whole.
To be able to achieve this at SGH, there needs to be both a realignment of the current
units to reflect synergy within clinical services, professional groups and overall
organisational business and strategic plans
See proposed Executive and Senior Management Structures:
TAB D - Proposed Organisation Chart
TAB E - Proposed Executive Organisation Chart
TAB F - Proposed Executive & Senior Management Organisation Chart
TAB G - Proposed Divisional Chart
TAB H - Proposed Structure of Nursing & Midwifery Services across SGH
In line with the Local Health District (LHD) business plan a major priority for the District is
to facilitate a district-wide approach to service delivery where there is an identification and
transition of services that can be appropriately managed across the entire LHD. As a
result, a number of site based services have been realigned to a centralised LHD run
model. Tab I outlines the proposed Executive Structure with a point of contact and
accountability for those LHD run services at SGH.
TAB I - Proposed Structure outlining LHD Service alignment
SGH Executive and Management Restructure Consultation Paper Page 83. Proposed Executive & Senior Management Structure
TAB D - Proposed Organisation Chart
SGH Executive and Management Restructure Consultation Paper Page 9TAB E- Proposed Executive Organisation Chart
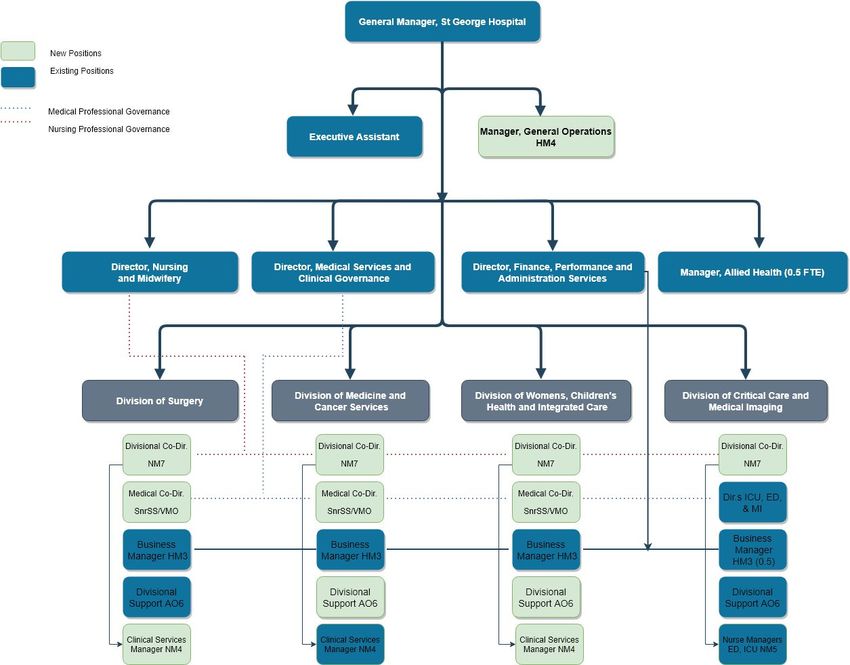
SGH Executive and Management Restructure Consultation Paper Page 10TAB F- Proposed Executive & Senior Management Organisation Chart
SGH Executive and Management Restructure Consultation Paper Page 11TAB G- Proposed Divisional Chart
SGH Executive and Management Restructure Consultation Paper Page 12TAB H- Proposed Structure of Nursing & Midwifery Services across SGH
St George Hospital: Director Nursing & Midwifery Executive Assistant
Nursing & Midwifery Structure (AO6)
(NM9)
Division of Medicine & Division of Womens , Division of Critical Care &
Division of Surgery
Cancer Services Children’s Health and Imaging
Divisional Co-Dir. (NM7) Integrated Care
Divisional Co-Dir. (NM7) Divisional Co-Dir. (NM7)
Divisional Co-Dir. (NM7)
NM
NM NM
Women & Children’s NM4 NM
OT NM5 Cancer NM4
Operational Nurse ED NM5
Admissions/Waitlist NM4
NUM/MUM 3 ICU NM4
Manager (NM7) NUM 3
Ambulatory Care/HITH
NUM 2 Cardiology/CCU NUM 3
Community/OPD
3S UGI/Plastic/ENT/BE HODC Emergency
3W Orthopaedics Birthing Services - Delivery/Birth
NM NM 2S Colorectal/Liver Centre/AAU
NUM2 NUM 2
Nursing Strategy & Access & Demand NM4 5S Cardiothoracic/Vascular 4S Renal/Gastro Emergency
Allocation Patient Flow NM2 5A Neuro/Trauma NUM 2
4W Dialysis ICU Inventory
Practice & Workforce After Hours Nurse Theatres Clinical Resource 7W Aged Care
5W Cardiology Intensive Care Services
Capability SGH/TSH Managers Anaesthetics 7S Aged Care
6B Respiratory
NESM Recovery 6A MAU/GMU Radiology
RCCP/COPD
Professor of Nursing CNC Day Surgery 6S Neurology 6W Rehab
Infection Control Recovery Diabetes Services SGH/TSH NUM 1
7A Oncology
Wound Care Pain 1S Antenatal/Postnatal/MSP ICU
NUM 2 7B Haematology/Rad Onc
Casual Staffing Office Patient Flow Endoscopy W&C Outpatients/STOMP
Immunisation & CCL 1W Gynaecology/EDO CNCs/NP
CNCs/NP/NE Emergency (NP)
Surveillance 1E Paediatrics
CNC Research Renal, Vascular Access Emergency
DPP NUM1 Special Care Nursery Child
SGH Nurse Educators Renal Transplant Peritoneal
Theatres Operational & Family Health ICU
Dialysis
RN/EN Organ and Tissue
Renal Palliative Respiratory
Patient Transit Lounge CNC/NP Hepatology/Liver Cardiology CNC/CMC/NP CERS
DPP Vascular Access Cardiovascular Cardiac Flying Squad
Trauma (CNS2) Rehab Continence NE
Stomal Therapy Heart Failure (NP) Community Health ICU
Pain Service Access Referral ED
Stroke
Nutritional Support HIV/ Immunology
Chest Clinic
Continence EB
Cancer Care Co-Coordinators
Pain Management Ambulatory Care
Palliative Care
Surgery Diabetes
Cancer Outreach
Key: Ano-rectal Physiology Oncology Risk Mxt & Practice Dev
Complex Pregnancy Care
Peritonectomy Haematology
Nursing & Midwifery Professional Reporting Line ERAS Lactation
Apheresis
Direct Reporting Line Cancer NE
NE NE/ME
OT Paediatrics
Midwifery
Clinical Nurse/Midwifery Educators, Registered Nurses, Midwives, Enrolled Nurses, Assistants in Nursing
SGH Executive and Management Restructure Consultation Paper Page 13TAB I - Proposed Structure outlining LHD Service alignment
SGH Executive and Management Restructure Consultation Paper Page 144. Proposed Structure Detailed Explanation
The current structure at SGH has been revised to ensure that the organisation is in a
position to meet the challenges associated with operating within a complex and fluid
environment. The proposed changes to the current Executive and Senior Management
structure are designed to improve the organisation’s effectiveness and management of
services for SGH for the benefit of patient care.
To ensure the facility is best placed to not only meet these challenges but to identify,
develop, implement and sustain strategies to address these, the Service Lines have been
condensed from six independent clinical services in two service lines into four distinct and
inclusive Divisions, these include:
- Division of Surgery
- Division of Medicine & Cancer Services
- Division of Womens, Children’s Health & Integrated Care
- Division of Critical Care & Medical Imaging
It is proposed that each of the divisions are managed in a collaborative fashion using a Co-
Director model (Nursing & Medical). The changes associated with introducing the Nursing
Co-Director positions reporting directly to the General Manager, create a structure within
which clinicians can take the lead in service development and delivery. In addition, with the
implemementation of the Clinical Services Manager (CSM) NM4, the operational
responsibility primarily for inpatient areas will sit with this role, allowing the Divisional Co-
Director to focus on broader strategic service delivery and performance.
The proposed structure recognises that clinicians are best placed to identify the
opportunities in their specialist areas, to consider future goals and set objectives to realise
these goals. The end result being improved services, better healthcare and enhanced
patient experience.
The proposed structure establishes distinct operational units, centred around the patient,
that balance size and scale to allow for strategy development and implementation whilst also
maintaining clear line of sight and connection to frontline service delivery and clinical flow.
This structure and connection will foster the integration of clinical, operational and financial
performance across each division.
With the implementation of a Clinical Services Manager (NM4), the new structure resolves
the operational challenges in the current SGH operating model by improving clarity of
accountability and decision-making authority within the key positions. It also promotes
greater cohesiveness for decision-making and governance. This will be critical as the facility
works to progress the Stage 3 Redevelopment and implementation of various new models of
care and service delivery.
The team currently known as Clinical Practice Improvement Unit (CPIU), will be re-named
Clinical Governance and Risk Unit. A manager of Clinical Governance and Risk Unit has
been created and recruited to, and reports to the Director Medical Services. This position will
further support and enhance the existing safety culture with an emphasis achieving quality
outcomes with shared accountability and teamwork at the forefront. It is designed to promote
a streamlined, collaborative environment which draws on a culture of high performance and
the delivery of exceptional patient care.
SGH Executive and Management Restructure Consultation Paper Page 15The Division of Corporate Services is recognised as a district service, where the facility point
of contact is the Manager, General Operations.
4.1 The Co-Director Model
The following four divisions will be led by a Co-Director Model as summarised below:
Division of Surgery Division of Medicine & Division of Womens Division of Critical Care
Cancer Services Children’s Health & & Medical Imaging
Integrated Care
Director, ICU
Divisional Medical Divisional Medical Co- Divisional Medical Co- Divisional
Director, ED
Co-Director Co-Director Co-Director Director Co-Director Director Co-Director
Director, MI
The Divisional Co-Director position for each division will be a Nurse Manager Grade 7. The
Divisional Co-Director roles will work in partnership with the Medical Co-Director to provide
leadership as well as develop and deliver strategic service plans for the Division, inclusive of
implementing organisation-wide initiatives and local improvements.
Together, the leadership positions of each division will also jointly develop and implement
strategies, plans, systems and procedures to minimise risk exposure and improve
performance of the division. Both Co-Directors will be accountable for providing strategic
leadership and management to the division, and implementing high levels of clinical
expertise to provide high quality care to the patients of SGH. Review of all reporting lines,
where not reflected in the organisation charts nor position descriptions, will occur during the
implementation phase.
In conjunction with the Director Medical Services & Clinical Governance and Medical Heads
of Department, The Medical Co-Director will develop medical workforce planning strategies
to ensure that appropriate staffing and skill mix levels are sustainably maintained.
The Medical Co-Director will provide professional leadership and management of the
Medical Heads of Departments, for three of the four Divisions. They are Division of Surgery,
the Division of Medicine & Cancer Services and the Division of Integrated Care, Women’s
and Children’s Health. The fourth division, Division of Critical Care and Medical Imaging with
three specialities, will operate with the three Heads of Department providing the medical
leadship, with protected administration time to carry out this function.
The Medical Co-Directors, will be appointed to on merit based selection, and be
remunerated by Managerial Allowance. It is proposed that the Medical Co-Director role will
receive a level two managerial allowance in accordance with the award.
SGH Executive and Management Restructure Consultation Paper Page 164.2 Business and Administrative Support Structure
Each division will be supported by the following roles that will be embedded within the
divisions as indicated in the table below.
Division of Surgery Division of Medicine & Division of Womens Division of Critical Care
Cancer Services Children’s Health & & Medical Imaging
Integrated Care
Director, ICU
Divisional Medical Divisional Medical Divisional Medical Co- Divisional
Director, ED
Co-Director Co-Director Co-Director Co-Director Co-Director Director Co-Director
Director, MI
Business Manager Business Manager Business Manager Business Manager
(HM3, 1.0 FTE) (HM3, 1.0 FTE) (HM3, 1.0 FTE) (HM3, 0.5 FTE)
Divisional Administration Divisional Administration Divisional Administration Divisional Administration
Officer Officer Officer Officer
(AO6, 1.0 FTE) (AO6, 1.0 FTE) (AO6, 1.0 FTE) (AO6, 1.0 FTE)
The Business Managers (3.5 FTE) are existing positions that will be realigned in accordance
with the proposed changes. The Business Managers will retain a dual reporting line to the
Co-Directors and dotted line to Director, Finance & Performance & Administrative Services
to ensure operational and professional oversight.
The Divisional Administration Officers will be 2.0 FTE from existing Administration Officer
Level 6 positions and 2.0 FTE from regraded Administration Officer Level 5 positions from
existing FTE. A Divisional Administration Officer will be aligned to each of the four Divisions,
reporting to the Divisional Co-Directors to support the divisions and functions as necessary.
4.3 Clinical Governance & Risk Unit (formally known as, Clinical Practice
Improvement Unit)
Within the Division of Medical Services & Clinical Governance, the new position of Manager,
Clinical Governance and Risk (1 FTE HM4) will provide enhanced oversight and support to
the Clinical Governance and Risk Unit, reporting through to the Director Medical Services
and Clinical Governance.
The role will provide management and leadership of the Clinical Governance and Risk Unit
and be responsible for governance and monitoring of key and quality safety areas including
but not limited to clinical incidents, healthcare acquired complications and overseeing the
work associated with Accreditation and safety and quality based programs e.g. Speaking up
for Safety and Clinical Excellence Commision initiatives.
The newly created position will also drive the development and implementation of risk
management systems and reporting frameworks extending across the site. The role will
serve to support and supplement the framework and processes currently in place to identify
and prevent circumstances that put patients at risk of harm. A focus for the role will also be
around ensuring key risk based learnings related to incidents are shared and mitigated for.
SGH Executive and Management Restructure Consultation Paper Page 17Under the current structure the Complaints/ Medico Legal Manager, Patient Safety
Managers and Quality Manager all report to the General Manager. This proposed change
will provide the Clinical Governance & Risk Unit staff a greater leadership presence with the
creation of a designated unit manager.
4.4 Director of Nursing and Midwifery (DONM)
The Director of Nursing and Midwifery will continue to work collaboratively with the General
Manager as a member of the St George Hospital Executive. The DONM will continue to
have professional responsibility for all nurses and midwives at St George Hospital.
In addition, the DONM will play a key role in supporting service delivery at a strategic level
inclusive of developing new models of care, providing strategic workforce and clinical advice
and support, and continuing to develop the workforce, vision and culture of nursing and
midwifery services.
The newly created Divisional Co-Directors will report directly through to the General
Manager (with the respective Medical Co-Director). This model encourages and promotes
integration and a cohesive and united approach to decision-making and governance.
Professional links to the Director of Nursing and Midwifery for Divisional Co-Directors will be
retained to ensure close links with professional and clinical service requirements.
The DONM will facilitate the transition of the Casual Staffing Office (CSO) governance to the
Nursing Strategy and Allocation Office. The CSO will remain operationally managed by the
Deputy DONM.
There will be no change with the remaining structure within Nurisng and Midwifery Services
including the Workforce Capability Services and the Professorial Research Unit.
4.5 Re-naming ‘Deputy Director of Nursing and Midwifery Services’ to ‘Operational
Nurse Manager’
The Deputy Director of Nursing and Midwifery will maintain its grade, and reporting line to
the Director of Nursing and Midwifery.
The intention in changing the title of the Deputy Director of Nursing & Midwifery to the
Operational Nurse Manager (ONM) is to better recognise the broader facility wide
operational responsibility of the position. The ONM is the central point of escalation for the
facility on matters relating to patient access and demand, critical incident and emergency
response and the executive lead on deteriorating patient models of care across all Divisions.
In addition, the position is responsible for the management of organisational services such
as Immunisation and Surveillance as well as facility based positions such as the After Hours
Nurse Managers and Infection Prevention and Control team.
SGH Executive and Management Restructure Consultation Paper Page 184.6 Casual Staffing Office, Nurse Manager
The St George Hospital Casual Staffing Office (CSO) is responsible for the daily central
coordination of clinical nursing and midwifery staff in all clinical areas across the facility. This
includes the management of over 430 casual nursing, midwifery and wardsperson staff as
well as the “Nurse Bank” workforce. In addition, the CSO has recently taken on the
management of the COVID Front Door Screeners (17.3 FTE).
The daily management of staff includes the allocation and coordination of clinical staff,
including the centralisation of sick leave calls, deployment and backfill. The CSO is
responsible for staffing clinical areas as per the Nursing Workload Tool (NWLT) and
industrial requirement of 6.0 NHPPD for those applicable areas. In addition the CSO also
manages unplanned staffing requirements including coordination of 1:1 specials, surge beds
and all overtime approvals via the ONM.
The CSO is staffed with 1 FTE Nurse Manager 3 and 1.42 FTE Nurse Unit Manager (NUM).
In the proposed structure the overarching governance of the Casual Staffing Office is to be
aligned to the Nursing Strategy and Allocation Office under the Nurse Manager 5. This will
facilitate enhanced coordination of recruitment strategies, vacancy management, the Nurse
Bank, as well as forward planning appropriate FTE management. The Nursing Strategy and
Allocation Office is the central point for recruitment, nursing/midwifery workforce and leave
matters with central oversight of the FTE status for all clinical areas, and as such will have
the ability to coordinate the permanent workforce with the addition of the casual workforce
with planned vacancies and unplanned leave.
The existing 1.42 FTE NUM2 within the service will continue to manage the operational
requirements and demands of the Casual Staffing Office in consultation with the ONM. The
existing workflow arrangements will remain unchanged.
It is proposed that the CSO Nurse Manager 3 position be deleted.
4.7 Allied Health Manager (0.5 FTE)
In the proposed structure, the Allied Health Manager position will have responsibility for the
Allied Health services of Physiotherapy, Occupational Therapy, Social Work, Nutrition and
Dietetics, Speech Pathology, Podiatry and Diversity Health.
Currently in the existing structure this position has responsibility for Medical Imaging,
Pharmacy and Clinical Information Service. Medical Imaging report professionally and
operationally to the Allied Health Manager with the exception of the Nursing staff who report
to the Deputy DONM.
In the proposed structure the management of Medical Imaging Services in its entirety will
report into the Division of Critical Care and Medical Imaging. Additionally, Clinical
Information Services will change reporting lines and move to the Director of Finance,
Performance and Administration Services portfolio. Pharmacy and Clinical Coding have
realigned to report directly into the LHD. This position will be the LHD point of contact for
Pharmacy Services.
SGH Executive and Management Restructure Consultation Paper Page 194.8 Disaster and DMS & CG Administration Officer (1.0 FTE)
St George Hospital has an Incident Controller and a Deputy Incident Controller as part of the
Disaster Control Plan. These positions have substantive roles, Director Medical Services &
Clinical Governance (DMS & CG) and Deputy Director of Nursing and Midwifery
respectively. Through the recent management of the pandemic, it became evident that a
dedicated position to support the management and administration of such an event is
required. The Disaster and DMS & CG Officer will oversee the management of central
communication, disaster response documentation and version control systems.
It is proposed that the current Administration Officer Level 6 position supporting the Director
Medical Services & Clinical Governance be reclassified to a Health Manager Level 1. This
reclassification will provide appropriate coverage of administrative matters related to the
disaster portfolio, as well as providing executive assistant support to the DMS & CG.
4.9 Manager, General Operations (1.0 FTE)
The Manager, General Operations will provide general operational support to St George
Hospital, and leadership on key projects and initiatives within the General Manager’s Unit.
The position will be directly responsible for autonomously managing a range of matters
within the General Manager’s Unit, such as projects, iniatives and a variety of resources,
including human, financial and physical.
An integral part of the role will be to act as the central point of contact for matters related to
Corporate Services. This position will be a point of escalation for matters relating to buildings
and facility infrastructure, including incidents relating to same. This includes the
responsibility to communicate the impact of these matters across the site. In addition, this
position will take on the management of Hospital Volunteers, Community Relations and
Wardspersons. The Manager will report to the General Manager and may also act as a
delegate for the General Manager in certain forums.
It is proposed that the current Senior Executive Officer Health Manager Level 3 position be
regraded to a Health Manager Level 4.
SGH Executive and Management Restructure Consultation Paper Page 205. Summary of proposed changes
5.1 Current positions to be deleted
Proposed
Current Position FTE Classification Grade
Action
Operations Manager - Critical 1.0 Delete Health Manager 5
Care, Trauma, Women’s &
Children’s Health
Temporarily filled
Operations Manager - Medicine, 1.0 Delete Health Manager 5
Cancer, Aged & Extended Care
Temporarily filled
Nurse Manager, Aged & 1.0 Delete Nurse Manager 6
Extended Care
Permanently filled
Nurse Manager, Critical Care 1.0 Delete Nurse Manager 6
Permanently filled
Nurse Manager, Surgery, 1.0 Delete Nurse Manager 6
Trauma and Anaesthetics
Permanently filled
Nurse Manager, Medicine 1.0 Delete Nurse Manager 6
Permanently filled
Nurse Manager, Women’s and 1.0 Delete Nurse Manager 6
Children’s Health
Permanently filled
Nurse Manager, Casual Staffing 1.0 Delete Nurse Manager 3
Office
Permanently filled
Senior Executive Officer 1.0 Delete Health Manager 3
Permanent encumbant on
secondment
Executive Assistant to Director 1.0 Delete Administration 6
Medical Services Officer
Permanently filled
Administration Officer Surgery 1.0 Delete Administration 6
Permanently filled Officer
Administration Officer Surgery, 1.26 Delete Administration 5
Critical Care and Women’s and Officer
Children’s Health
Permanently filled
Administration Officer Medicine 1.0 Delete Administration 5
Permanently filled Officer
Administration Officer Cancer 1.0 Delete Administration 5
and Aged and Extended Care Officer
Permanently filled
Administration Officer Women’s 1.0 Delete Administration 6
and Children’s Health Officer
Permanently filled
SGH Executive and Management Restructure Consultation Paper Page 215.2 Proposed new positions
New Position FTE Proposed Classification Grade
Action
Divisional Co-Director, Surgery 1.0 New Nurse 7
Manager
Divisional Co-Director, Medicine & 1.0 New Nurse 7
Cancer Services Manager
Divisional Co-Director, Integrated 1.0 New Nurse 7
Care, Women’s and Children’s Manager
Health
Divisional Co-Director, Critical Care 1.0 New Nurse 7
& Imaging Manager
Clinical Services Manager, Surgery 1.0 New Nurse 4
Manager
Clinical Services Manager, 1.0 New Nurse 4
Integrated Care, Women’s and Manager
Children’s Health
Medical Co-Director, Surgery 0.3 New Staff -
Existing staff specialist, merit based Specialist/
selection and managerial allowance VMO
Medical Co-Director, Medicine & 0.3 New Staff Specialist -
Cancer Services
Existing staff specialist, merit based
selection and managerial allowance
Medical Co-Director, Integrated 0.3 New Staff Specialist -
Care, Women’s and Children’s
Health
Existing staff specialist, merit based
selection and managerial allowance
Manager, General Operations 1.0 New Health 4
Manager
Divisional Administration Officer 2.0 New Administration 6
Officer
Divisional Administration Officer 2.0 New Administration 6
Matching of existing staff Officer
Disaster and DMS & CG Officer 1 New Health 1
Manager
Manager, Clinical Governance & 1.0 New Health 4
Risk Manager
Recruitment Completed
SGH Executive and Management Restructure Consultation Paper Page 225.3 Proposed new reporting lines
Department Current Reporting Line Proposed New Reporting
Line
CPIU General Manager Director of Medical Services
and Clinical Governance
Radiology Allied Health Manager Divisional Co-Director
Critical Care & Medical
Clinical Information Services Allied Health Manager Director of Finance and
Performance and
Administration Services
Community Relations General Manager Manager, General
Operations
Hospital Volunteers & General Manager Manager, General
Chaplains Operations
6. Consultation
This Restructure Consultation paper and the draft position descriptions will be released for
consultation for two weeks.
Staff that would be significantly impacted by the proposals set out in this document have
been contacted individually and advised of the proposed changes.
The General Manager, St George Hospital will consider feedback from all staff members.
Written feedback should be provided to Maria Buric, A/Principal HR Advisor via email
maria.buric@health.nsw.gov.au
The Health Services Union (HSU), the New South Wales Nurses’ and Midwives’ Association
(NSWNMA) and the Australian Salaried Medical Officers Federation (ASMOF) will be
notified of the proposal and provided with the Restructure Consultation Paper, as well as an
opportunity to comment on the proposal.
7. The recruitment and matching process
All changes will be managed as per NSW Health PD2012_021 Managing Excess
Staff of the NSW Health Service and SESLHD PD/180 Change Management.
Upon conclusion of the consultation period and provision of a response to feedback
including any changes as a result, all staff who will be affected by deletions,
realignment or change of reporting lines will be informed in writing that they are
affected.
Directly matched affected staff will be advised in writing of their new position.
Where matching cannot occur, positions will be advertised and a merit selection
recruitment process will be undertaken. Where staff are not matched or appointed
to a position, they will be declared excess.
Excess staff will have 14 days to accept or decline an offer of voluntary
redundancy. Staff who accept an offer of voluntary redundancy will leave SESLHD
within two weeks. Staff who decline the offer of voluntary redundancy will receive
case management and career assistance.
SGH Executive and Management Restructure Consultation Paper Page 238. Employee Assistance Program
Staff are reminded of the availability of the Employee Assistance Program through Converge
on 1300 687 327. This number is answered 24 hours per day, seven days per week, to
facilitate enquiries, booking requests and to provide assistance.
9. Restructure Timeframe
Timeframes
Task Documentation/Detail (indicative) Week
Commencing
Restructure Consultation
Consultation period with staff and
Paper and draft position 17 May 2021
unions commences
descriptions
Completion of consultation phase
1 June 2021
Restructure Consultation
Feedback reviewed and
Paper Feedback from 11 June 2021
considered
consultation
Final consultation document
Restructure Consultation
incorporating any changes
Paper (Final) 16 June 2021
identified during consultation
circulated
Written advice issued to affected Letters to advise staff of
22 June 2021
staff ‘affected status’
Process of direct matching of
Letter to advise of matching to
affected staff to positions in the 25 June 2021
position
new structure
Vacant positions advertised Through merit selection
25 June 2021
(either via EOI or ROB) recruitment process
Selection process for positions Assessment of applications
25 June 2021
commences and interviews
Written advice issued to staff Letter to advise of
23 July 2021
appointed to positions appointments
Letter to advise of ‘excess
Staff not matched or appointed to status’ and the option to
positions are declared excess choose a voluntary 23 July 2021
redundancy or seek
redeployment
Written advice to staff unable to be
Letter to advise of involuntary
placed in positions after three 3 months from
redundancy
months of case management to acceptance of
(CURRENTLY PAUSED IN
receive involuntary redundancy option to seek
RELATION TO ANY ACTION
(CURRENTLY PAUSED IN redeployment
OF INVOLUNTARY
RELATION TO ANY ACTION OF
REDUNDANCY)
INVOLUNTARY REDUNDANCY)
SGH Executive and Management Restructure Consultation Paper Page 24PROCESS MAP FOR ORGANISATIONAL RESTRUCTURES
Plan Developed for Restructuring
Unit/service/department
Proposed Structure and Position
Descriptions Developed and issued to
Union/Association for Consideration
Proposed Structure and Position Formal written advice
Descriptions Issued to Staff in issued to affected
Affected unit/service/department staff
Process of direct matching affected staff
to vacancies in the new Structure
Formal written advice
Direct matching of issued to staff
staff completed successfully matched
to new positions
Staff who are not directly matched to
positions able to submit an Expression of
Interest for remaining vacant positions.
Successful
Selection process undertaken for
candidates
vacant positions
appointed
Staff member exits
the organisation
within a 2 week
Staff unsuccessful in the matching and
period Formal written advice
EOI process are declared Excess
provided to staff
successful in the
EOI process
Voluntary Offers of Voluntary Redundancy
redundancy made to excess staff, including
accepted calculations of redundancy payment Voluntary
Redundancy
declined
Staff member made Staff member issued Staff member Commencement of 3
forcibly redundant further written notice provided with Case month Retention
and exits the 2 weeks prior to the Management and Period for staff
organisation at end of expiry date of the Career Transition member to seek
the Retention Period Retention Period Assistance redeployment
Staff member
successfully
redeployed
SGH Executive and Management Restructure Consultation Paper Page 25Appendix 1 Proposed new Position Descriptions
1. Co-Director, Division, NM7
POSITION DESCRIPTION
Position Details
Position Number: TBA
Co-Director, Division
Position Title:
Cost Centre: TBA (Cost) Percentage:
Organisation: South Eastern Sydney Local Health District
Location: Kogarah
Facility: St.George Hospital
Are multiple Awards
relevant to this No
position?
NSW Public Hospital
Nurse Manager
Award: Nurses & Midwives Classification:
Grade 7
(State) Award
Registration and
Licence NSW Public Hospital Nurses (State) Award
requirements:
Specialty Code:
Vaccination
A
Category:
Operationally – General Manager
Responsible to:
Professionally – Director of Nursing of Nursing and Midwifery
Responsible for
FTE’s as per Division
(staff):
Position Description
March 2021
Approved/Reviewed :
Primary Purpose of the Position
South Eastern Sydney Local Health District (SESLHD) is committed to improving the care provided
to our patients in line with our vision of Working together to improve the health and wellbeing of
our community.
The Divisional Co-Director is responsible and accountable for the daily operational activities within
the program and for the delivery of clinical services within allocated resources, ensuring that service
activity and care delivery is consistent with organisation performance targets and clinical safety
standards.
The Divisional Co-Director will work closely with the Medical Co-Director, and will actively contribute
to the overall leadership and management within the Division. The position will be responsible for
the strategic development and delivery of the Divisional business plan, inclusive of implementing
organisation-wide initiatives and delivering local improvements and projects that improve
performance, workplace culture and organisational reputation
SGH Executive and Management Restructure Consultation Paper Page 26The Divisional Co-Director will be responsible for the professional development, education and
research of staff within the Division, and in driving professional strategy/initiatives in line with
Professional Plans at both the facility and South Eastern Sydney Local Health District level
(SESLHD).
Key Accountabilities
Executive Accountabilities:
• Develop, lead and implement systems and processes to ensure the delivery of service plans
and strategies, in alignment with SESLHD strategies and incorporating improvement, research,
analysis and high quality reporting.
• Contribute towards the strategic/planning processes within nursing locally and within the South
Eastern Sydney Local Health District.
• Lead and facilitate meetings, promoting effective collaboration for patient focused solution
development in areas such as patient safety and quality.
• Lead and participate in the implementation of key organisational and Programme initiatives that
contribute to the systems and business processes, reflecting improvement strategies in
meeting organisation performance indicators and goals.
• Evaluate achievements and outcomes through quality control audits in the area of mitigating
patient harm, using the patient safety program and other programs identified in achieving quality
patient safety within the Programme.
• Oversee financial management of the Programme using systems, budgets and reporting tools
that integrate with the organisations financial data systems.
• Evaluate and report on identification, escalation and mitigation of clinical risks within the
Programme in alignment with National Standards, Clinical and Patient Safety programs and
organisation data collection systems.
• Monitor and utilise person centred care principles, in addition to collected data and feedback,
to inform managers within the Programme, of deficits requiring timely action, ensuring
appropriate resources are in place.
• Monitor staffing strategies to ensure adequate requirement and retention, including
development, succession and capability building planning.
• Develop workforce plans for strategic use of human resources in achieving workforce priorities
and addressing models of care for the Programme.
• Develop, implement and monitor staffing strategies to ensure adequate recruitment and
retention including succession and capacity building planning for nursing and support services.
• Develop a culture within the Divisonwhich is open to critical reflection and change
• Identify, evaluate and incorporate where appropriate emerging trends with the nursing
discipline.
• Ability to represent nursing services in a range of forums internally and externally to the facility
and SESLHD.
Operational Accountabilities:
• Facilitate the engagement and collaboration of nursing and support staff colleagues in the
development, monitoring and achievement of key organisational and Division
initiatives/indicators.
• Manage senior nursing leadership teams through the use of performance management tools
and effective communication, including promotion of professional accountability, strategic
direction and operational goals of the service line.
• Develop workforce planning strategies in line with facility based nursing strategy, ensuring
appropriate staffing levels in line with NHPPD and other associated staffing models to enable
and maintain appropriate staffing and skill mix levels within the selected models of care.
• Participate in activities to assist meet requirements for National Accreditation Standards.
• Collaborate with Divisional NUM/NMs to ensure activity and care delivery is in line with the key
areas of cost centre management and reporting, human resource initiatives and risk
management
• Provide leadership and support to NUM’s to ensure an effective management of nurses through
the use of the organisations performance management frameworks and tools.
• Evaluate and report on local patient flow management within the Division.
SGH Executive and Management Restructure Consultation Paper Page 27• Escalation and management of operational issues to the Operational Nurse Manager & Director
of Medical Services as appropriate
• Escalation and management of issues to GM as appropriate
• Lead and coordinate regular executive Divisional management meetings with the Medical Lead,
Patient Safety Manager, Workforce Consultant and Allied Health Representative.
• Represent the service peak committees at local and district level (where appropriate)
• Contribute to the annual review and negotiation of the budget build up.
• Monitor compliance with approved budget and initiate timely and appropriate corrective action
in collaboration with cost centre Managers, .
• Model the highest standards of ethical behaviour and interaction that promote a culture and
supporting practices that reflect the organisations values at all times.
• Maintain responsibility for personal and professional development by participating in evidence
based practice activities, professional development and training/education, and performance
reviews/appraisals in order to continuously improve leadership and management within the
service.
Key Challenges and Influences
Challenges/Problem Solving:
Major challenges for the Divisional Co-Directorinclude:
• Balancing limited resources to meet competing patient/client needs and expectations and
dealing with high volume workloads while at the same time managing to achieve positive
outcomes
• Managing time and prioritising issues given the diverse range of issues encountered
simultaneously and work demands flowing from a number of sources
• Participating in ongoing consultations with internal and external stakeholders as considered
appropriate where there are competing needs/objectives
Communication:
• Internally, the Divisional Co-Director is required to communicate regularly with service line
executive and management, nursing staff, medical staff, and other health care members of
multi-disciplinary teams on issues related to patient care and team functioning
• Externally, the Divisional Co-Director will develop and maintain effective relationships with
relatives, patients, Ministry of Health, other health organisations, NGO’s
Decision Making/Influence:
The Divisional Co-Director:
• Makes decisions using advanced reasoning skills and independent judgement and work
autonomously in relation to day-to-day operations and clinical care of patients/clients within
scope of practice
• Has substantial autonomy in the management of staff and other resources of the Service Line
including managing the performance of others to achieve work objectives
• Exercises independent professional knowledge and judgement to solve problems of a
complex nature
Selection Criteria:
• Registered Nurse who holds current registration with the Nursing and Midwifery Board of
Australia (AHPRA).
• Holds tertiary management qualifications or equivalent work experience relevant to the role
and demonstrated evidence of recent professional development to further enhance leadership
and management competencies.
• Demonstrated experience and competencies in organizational change management and
achievements of measurable outcomes.
SGH Executive and Management Restructure Consultation Paper Page 28• Demonstrated broad clinical, operational and strategic experience at a senior level within a
complex health care environment, with an ability to function as part of a senior management
team working successfully with other professional and disciplines in the management of
health care services.
• Demonstrated high level verbal, written and negotiation skills with an aptitude to utilize
relevant information technology platforms and ability to provide clear and concise business
plans and reports.
• Demonstrated extensive experience in human resources and financial management within a
complex health care service.
• Demonstrated in depth knowledge of current clinical practice, its delivery and models of care
and the ability to motivate, inspire, and lead staff to achieve service and clinical outcomes.
Focus Capabilities
The focus capabilities for the role are the capabilities in which applicants must demonstrate
immediate competence. The behavioural indiactors provide examples of the type of behaviours that
would be expected at that level and should be reviewed in conjunction with the role’s key
accountabilities.
NSW Public Sector Capability Framework
Group & Capability Level Behavioural Indicators
Personal Attributes Highly Create a climate which encourages and
Advanced supports openness, persistence and genuine
DISPLAY RESILIENCE AND
debate around critical issues.
COURAGE
Provide sound exposition and argument for
agreed positions while remaining open to
valid suggestions for change.
Raise critical issues and make tough
decisions.
Respond to significant, complex and novel
challenges with a high level of resilience and
persistence.
Consistently use a range of strategies to
keep control of own emotions and act as a
stablilising influence even in the most
challenging situations.
Relationships
COMMUNICATE Highly Present with credibility, engage varied
EFFECTIVELY Advanced audiences and test levels of understanding.
Translate technical and complex information
concisely for diverse audiences.
Create opportunitnies for others to contribute
to discussion and debate.
Actively listen and encourage others to
contribute inputs.
SGH Executive and Management Restructure Consultation Paper Page 29Adjust style and approach to optimise
outcomes.
Write fluently and persuasively in a range of
styles and formats.
WORK COLLABORATIVELY
Highly
Encourage a culture of recognising the value
Advances
of collaboration.
Build co-operation and overcome barriers to
information sharing and communication
across teams/units.
Share lessons learned across teams/units.
Identify opportunities to work collaboratively
with other teams/units to solve issues and
develop better processes and approaches to
work.
Results
DELIVER RESULTS Highly Take responsibility for delivering on intended
Advanced outcomes.
Make sure team/unit staff understand
expected goals and acknowledge success.
Identify resource needs and ensure goals are
achieved within budget and deadlines.
Identify changed priorities and ensure
allocation of resources meets new business
needs.
Ensure finanical implications of changed
priorities are explicit and budgeted for.
Use own expertise and seek others’ expertise
to achieve work outcomes.
THINK AND SOLVE Undertake objective, critical anyalysis to draw
PROBLEMS Highly accurate conclusions that recognise and
Advanced manage contextual issues.
Work through issues, weigh up alternatives
and identify the most effective solutions.
Take account of the wider business context
when considering options to resolve issues.
Explore a range of possibilities and creative
alternative to contribute systems, process
and business improvements.
Implement systems and processes that
underpin high quality research and analysis.
Business Enablers
FINANCE Advance Understand core financial terminology,
policies and processes and display a
knowledge of relevant recurrent and capital
financial measures.
Understand impacts of funding allocations on
business planning and budgets, including
SGH Executive and Management Restructure Consultation Paper Page 30value for money, choice between direct
provision and purchase of services, and
financial implications of decisions.
Understand and apply financial audit,
reporting and compliance obligations.
Identify discrepancies or variances in
financial and budget reports, and take
corrective action where appropriate.
Seek specialist advice and support where
required.
Make decisions and prepare business cases
paying due regard to financial considerations.
People Management
MANAGE AND DEVELOP Advanced Refine roles and responsibilities over time to
PEOPLE achieve better business outcomes.
Recognise talent, develop team capability
and undertake succession planning.
Coach and mentor staff and encourage
professional development and continous
learning.
Provide timely, constructive ad objective
feedback to staff.
Address and resolve team and individual
performance issues, including serious
unsatisfactory performance, in a timely and
effective way.
Implement performance development
frameworks to aligh workforce capability with
the organisation’s current and future priorities
and objectives.
Employment Screening Checks:
National Criminal Record Check
National Criminal Record Check (Aged Care)
X Working with Children Check
Select one from the above options
Position Dimensions
Staffing
No. of staff reporting directly
No. of staff reporting indirectly
Total no. of staff reporting to position
Budget
SGH Executive and Management Restructure Consultation Paper Page 31Recurrent Expenditure $
Staff management $
Capital $
Revenues $
Total $
1. Certification
2.
Chief Executive or delegate: Associate Director/Manager/Supervisor
Date: ___/___/___
Date: ___/___/___
Position Holder:
Date: ___/___/___
SGH Executive and Management Restructure Consultation Paper Page 32JOB DEMANDS CHECKLIST
Definitions: *Denotes a critical requirement of the job
Frequency
Infrequent – intermittent activity exists for a Constant – activity exists for more than 2/3 of
I C
short time on a very infrequent basis the time when performing the job
Occasional - activity exists up to 1/3 of the Repetitive – activity involves repetitive
O time when performing the job R movements
Frequent – activity exists between 1/3 and Not applicable – activity is not required to
F 2/3 of the time when performing the job N/A perform the job
PHYSICAL DEMANDS - DESCRIPTION (comment) FREQUENCY
CRITICAL
I O F C R N/
A
Sitting Remaining in a seated position to perform tasks x
Standing Remaining standing without moving about to perform tasks x
Walking Floor type: even/uneven/slippery, indoors/outdoors, slopes x
Running Floor type: even/uneven/slippery, indoors/outdoors, slopes x
Bend/ Lean Forward from Waist Forward bending from the waist to x
perform tasks
Trunk Twisting Turning from the waist while sitting or standing to x
perform tasks
Kneeling Remaining in a kneeling posture to perform tasks x
Squatting/ Crouching Adopting a squatting or crouching posture to x
perform tasks
Leg/ Foot Movement Use of leg and or foot to operate machinery x
Climbing (stairs/ladders) Ascend/ descend stairs, ladders, steps, x
scaffolding
Lifting/ Carrying x
Light lifting & carrying – 0 – 9kg
Moderate lifting & carrying – 10 – 15kg x
Heavy lifting & carrying – 16kg and above x
Reaching Arms fully extended forward or raised above shoulder x
Pushing/ Pulling/ Restraining Using force to hold/restrain or move x
objects toward or away from body
Head/ Neck Postures Holding head in a position other than neutral x
(facing forward)
Hand & Arm Movements Repetitive movements of hands & arms x
Grasping/ Fine Manipulation Gripping, holding, clasping with fingers x
or hands
Work at Heights Using ladders, footstools, scaffolding, or other objects x
to perform work
Driving Operating any motor powered vehicle x
FREQUENCY
RI
C
SGH Executive and Management Restructure Consultation Paper Page 33You can also read