Primary Care Informatics Response to Covid-19 Pandemic: Adaptation, Progress, and Lessons from Four Countries with High ICT Development
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Published online: 2021-04-21
44
© 2021 IMIA and Georg Thieme Verlag KG
Primary Care Informatics Response to
Covid-19 Pandemic: Adaptation, Progress,
and Lessons from Four Countries with High
ICT Development
Siaw-Teng Liaw1, Craig Kuziemsky2, Richard Schreiber3, Jitendra Jonnagaddala1, Harshana
Liyanage4, Aliasgar Chittalia5, Ravninder Bahniwal6, Jennifer W. He7, Bridget L. Ryan8,
Daniel J. Lizotte9, Jacqueline K. Kueper7, Amanda L. Terry8, Simon de Lusignan4
1
WHO Collaborating Centre on eHealth, UNSW Sydney, Australia
2
MacEwan University, Edmonton, Alberta, Canada
3
Penn State Health Holy Spirit Medical Center, Camp Hill, Pennsylvania, USA
4
Nuffield Department of Primary Care Health Sciences, University of Oxford, UK
5
Family Practice Center, Mountaintop, Pennsylvania, USA
6
Schulich Interfaculty Program in Public Health, Western University, London, Canada
7
Graduate Program in Epidemiology and Biostatistics, Western University, London, Canada
8
Centre for Studies in Family Medicine, Department of Family Medicine, Western University,
London, Canada
9
Department of Computer Science, Western University, London, Canada
Summary Results: All countries responded rapidly. Common themes change. However, the lack of coordinated national strategies and
Objective: Internationally, primary care practice had to transform included rapid reductions then transformation to virtual visits, regulation, assurance of financial viability, and working in silos
in response to the COVID pandemic. Informatics issues included pausing of non-COVID related informatics projects, all against a remained limitations. The potential for primary care informatics
access, privacy, and security, as well as patient concerns of background of non-standardized digital development and dispa- to transform current practice was highlighted. More research is
equity, safety, quality, and trust. This paper describes progress rate territory or state regulations and guidance. Common barriers needed to confirm preliminary observations and trends noted.
and lessons learned. in these four and in less-resourced countries included disparities
Methods: IMIA Primary Care Informatics Working Group mem- in internet access and availability including bandwidth limita- Keywords
bers from Australia, Canada, United Kingdom and United States tions when internet access was available, initial lack of coding Telemedicine, Primary Health Care, health policy, public health,
developed a standardised template for collection of information. standards, and fears of primary care clinicians that patients were severe acute respiratory syndrome coronavirus 2
The template guided a rapid literature review. We also included delaying care despite the availability of televisits.
experiential learning from primary care and public health Conclusions: Primary care clinicians were able to respond to the Yearb Med Inform 2021:44-55
perspectives. COVID crisis through telehealth and electronic record enabled http://dx.doi.org/10.1055/s-0041-1726489
1 Introduction nication technology (ICT) developments
and telehealth were “fast-forwarded” to
privacy and ethical issues, participants’ lit-
eracy, cost, reimbursement, and regulatory
Primary care informatics (PCI) is the sci- support the rapid and ongoing response to barriers [3]. Despite a lack of evidence for
ence that underpins digital health in the the COVID-19 pandemic [2]. the access, equity, utility, safety and qual-
community, empowering patients, carers, Primary care had to deal with managing ity of telehealth, it quickly became policy
citizens, health professionals and health or- personal protective equipment (PPE), pub- (Box 1) [4]. The scope to develop PCI
ganisations in the delivery of safe, effective, lic health guidelines such as hand hygiene and digital health to support primary care
and integrated patient-centred care. and social distancing, and contact tracing during COVID-19 cannot be separated from
Global progress towards digital health apps, and informatics issues including tech- policy, human resources and other system
maturity [1] was slow until the COVID-19 nical issues (network connectivity & user limitations [5, 6].
pandemic when information and commu- interfaces), limited physical examination,
IMIA Yearbook of Medical Informatics 2021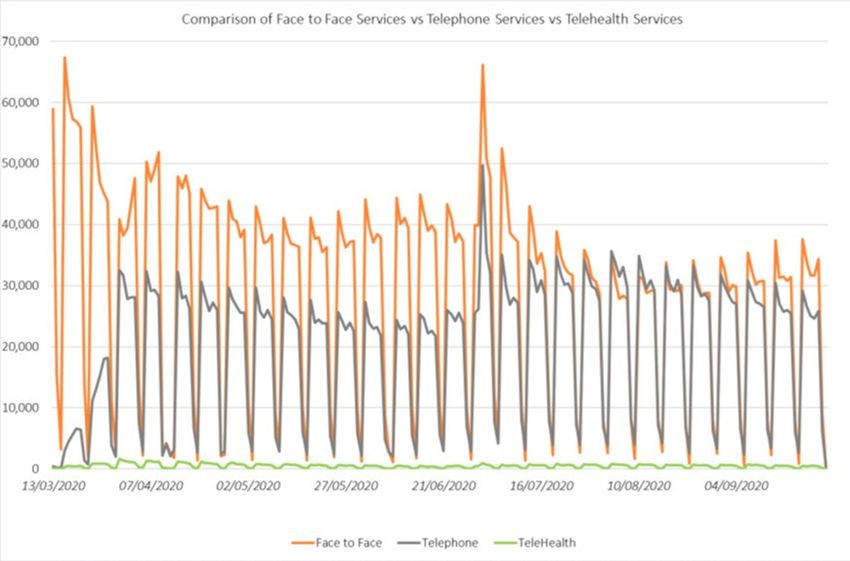
45
Primary Care Informatics Response to Covid-19 Pandemic: Adaptation, Progress, and Lessons from Four Countries with High ICT Development
countries (Australia, Canada, USA, UK) However, the Australian Nation-
“Our government’s response to the
ranked in the top 30 of 176 countries with al COVID-19 Primary Care Response
pandemic brought forward a 10-year
an International Telecommunication Union changed this and implemented expanded
plan on telehealth within 10 days.”
Australian Health Minister
ICT Development Index [7] and provided access to telehealth services, training of the
an international comparison with data from health workforce, 24-hour health advice,
India (ranked 134) and Pacific Islands (Kiri- dedicated community-based “respiratory”
“These investments will help provide
bati ranked 154). clinics, and enhanced protection for remote
Canadians with virtual health care
The concepts guided the limited scoping communities [9].
services that are safe and secure.”
Canadian Federal Minster or Health
literature review for each of the countries.
Search terms included: primary health care,
family medicine, general practice, popula- b COVID-19 Impacts on Primary Care
“GP tele-consultations should be
tion, health, medical, informatics, telemed- Delivery in Australia
default unless reason not to.” Temporary telehealth items introduced in
icine, telehealth, teleconsultation, virtual,
United Kingdom Health Secretary March 2020 for 6 months significantly acceler-
consultation, encounter, videoconference,
COVID-19, equity, disparities, health insur- ated a shift from physical “in-person” consulta-
“’Please don’t give up. Don’t despair, ance, health benefits, accessibility, privacy, tions to virtual face-to-face consultations [10].
the end is in sight,’ as opposed to: Telemedicine activities peaked in April, 2020
computer security, regulatory, regulations,
‘Hey, we are good to go, don’t worry at 38% of all ambulatory visits captured in the
risk, and various short forms with wildcards.
about anything.’ We are not good Australian Medicare program [11]. In the first
to go. We have got to continue to
We enhanced the literature review with
personal experiences with COVID-19 from 40 weeks of COVID-19, a significant initial
double down on public health mea-
the primary care and public health perspec- increase in phone consultations was maintained
sures.”
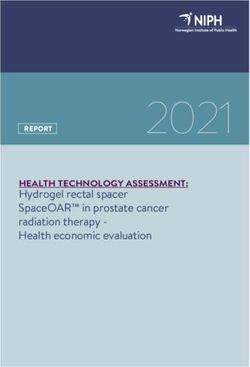
Dr. Anthony Fauci, COVID advisor tives in our respective countries. We also but the small initial increase in video consul-
to the President of the United States examined issues with data custodianship tations was not (Figure 1) [12]. Telehealth has
of America and stewardship of primary care data re- enabled 85% patients with COVID-19 to be
positories in the UK and Australia. We then managed in the community, including patients
summarised and synthesised the information suspected of SARS-CoV-2 (Severe Acute Re-
Box 1 Quotes from health system leaders about the shift towards to identify the impacts of COVID-19 on spiratory Syndrome Coronavirus 2) infection
digital health primary care, how PCI adapted, and how it and vulnerable elderly patients at increased
may evolve into the future and a new normal risk of complications [13]. At-risk older or
for primary care. quarantined GPs can continue consulting from
home, avoiding in-person consultations [14].
2 Objectives By September, 32% GP consultations
were by telehealth: 97% by phone and used
We examine the use of PCI and telehealth 4 Results: PCI response to more by women. Video was highest for the
across the COVID-19 pandemic across
countries with variable resources and levels
COVID-19 25-44 age group. About 20% specialists
billed MBS telehealth services; of these 16%
of digital health maturity. We report how 4.1 Australia were for video, compared with 3% for GPs
PCI supported the transformation of health [11]. While 16% is not great for nine years
systems focusing on virtual primary care en- a Healthcare system (from 2011), it suggests video services in
counters, documenting areas of accelerated The Australian federated health system general practice are likely to increase with
progress and lessons learned. is complex and fragmented, but evolving time, familiarity and better infrastructure,
towards an integrated, citizen-centred, ac- consistent with international literature [15].
countable and sustainable system. The My The MBS GP telehealth items have been
Health Record system addressed informa- extended to March 2021, restricted to vul-
3 Methods tion sharing and integrated care delivery.
There was little progress on foundational
nerable patients with an existing relationship
with the GP – defined as an in-person visit
Volunteer members of the IMIA Primary elements such as e-prescribing and com- in the past 12 months [16]. This restriction
Care Informatics Working Group developed puterised physician order entry (CPOE) has prevented some vulnerable groups from
a template to standardise the collection of in primary care. Whilst the Australian accessing telehealth services [14]. It also wor-
relevant PCI concepts and information. We Medicare Benefits Schedule (MBS) has ries many private general practices (60%) at
described the primary care system in each included specialist telehealth items since risk of non-viability as a result of COVID-19
country, then how PCI was used and adapted, 2011 there were no general practice (GP) [17]. An Australian private health insurer
extent of success, and lessons learnt from items, apparently because of risks of fraud/ (Medibank) has extended coverage indefinite-
each country. We present data from four over-servicing [8]. ly for allied health teleservices [18].
IMIA Yearbook of Medical Informatics 2021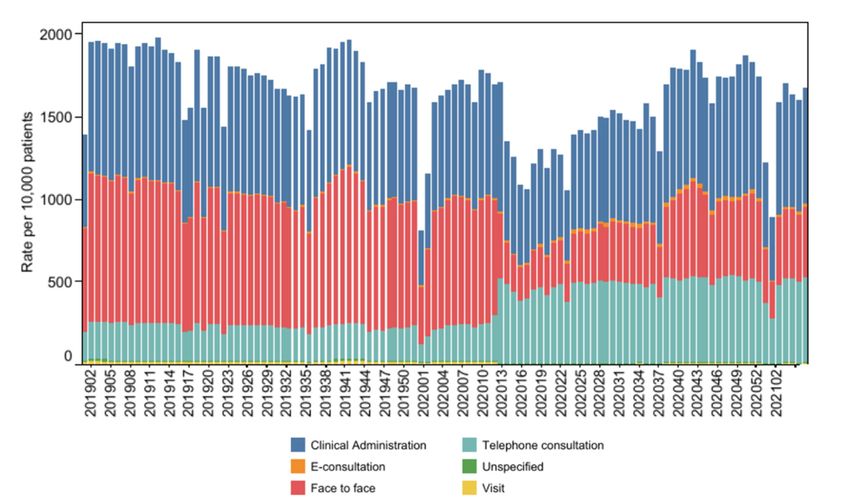
46
Liaw et al.
d Next steps: What has Australia learned
from COVID-19?
Primary care will need support to increase its
digital health capacity, including standards
for virtual health competencies, training,
implementing electronic referrals and CPOE
to enable the delivery of virtual care [24].
4.2 Canada
a Healthcare system
COVID-19 has accelerated the Canadian
health system to increase virtual care capacity
while respecting physical distancing [2]. The
challenges are significant for primary care
providers (PCP) as they need to deliver regu-
lar PC services and also manage COVID-19
screening and contact tracing. There was no
national eHealth strategy or system to support
the Canadian national COVID-19 response
Fig. 1 Daily charting of mode of consultations by GPs in South Eastern Australia. In person consultations declined and phone consultations because the separate Province and Territory
increased; both after the initial surge. The low levels of telehealth (videoconsultation) remained stable. Source: Pearce C et al. The GP Insights healthcare delivery systems developed their
Series no 7. 26 Oct 2020 (www.polargp.org.au) [12] own strategies and tools including telehealth
and virtual care [25], e-referral and intake
[26] and a hospital-at-home initiative [27].
c Implications for primary care informatics South Eastern Australia [12]. In the first 40 b COVID-19 impacts on primary care
Non-standardised development of digital weeks of COVID-19, POLAR data showed delivery in Canada
tools: Telemonitoring is increasingly being marked reduction in GP presentations for Canada was challenged by travel restriction
used for patients at high risk of readmission childhood infective illnesses (bronchiolitis, delays, insufficient testing, insufficient PPE
or who live in residential aged care settings gastroenteritis) and antibiotic prescriptions, supply, and difficulties with infection control
[19]. Current systems are being modified to with concomitant increases in anxiety, in long-term care settings [28]. PCPs started
address COVID-19, an example being the depression and eating disorder-related diag- working in new settings such as COVID-19
Total Cardiac Care (TCC+) system which noses. Other data sources showed contem- screening and assessment centres. PCPs
added oximetry to its range of sensor de- porary decreases in cancer biospecimens were encouraged to provide telemedicine
vices [20]. TCC+ is seeking registration as and pathology services [23]. A balanced and virtual care, with immediate uptake of
Software as a Medical Device with the Aus- approach for timely cancer diagnosis was a virtual-visit-first model. In-person consul-
tralian Therapeutic Goods Administration. recommended and indicates what PCI could tations were limited by deferring non-urgent
COVIDSafe, a contact tracing app, has been focus on [8, 23]. Mental healthcare support visits. Triaging protocols for virtual visits
superseded by electronic registration using for isolated elderly and young people needs were developed [29]. Consults were primar-
QR-based technologies at public venues. digital enhancement. ily by telephone, but also included email,
COVID-19 sped up electronic prescribing, Unintended consequences: An Adelaide video conferencing, and telemedicine ser-
allowing general practices to communicate, digital health firm sent patient details and vices (e.g., https://onmd.ca/). Patients were
using a token or an active script list, with COVID-19 test results to wrong people. generally satisfied and will continue using
local pharmacies to write and dispense an Australia’s current hybrid method of contact virtual care, citing reasons like increased
eScript [21]. tracing—manual and assisted by spread- safety, convenience, and accessibility [30].
Timely access to real-world data (RWD) sheets and generic customer relationships Each jurisdiction introduced similar
across the spectrum of care: Popula- management solutions—raises questions regulations such as adapting physician fee
tion-level data on telehealth are available about safety standards, security and schedules, updating practice guidelines, and
through Medicare [22]. The POLAR privacy, similar to those posed to the providing income stabilization [31]. Virtual
repository contains patient-level RWD head of UK National Health Service care billing codes were released in March
extracted from 1000 general practices in (NHS) Test-and-Trace. 2020 [32]; some provinces have since updated
IMIA Yearbook of Medical Informatics 2021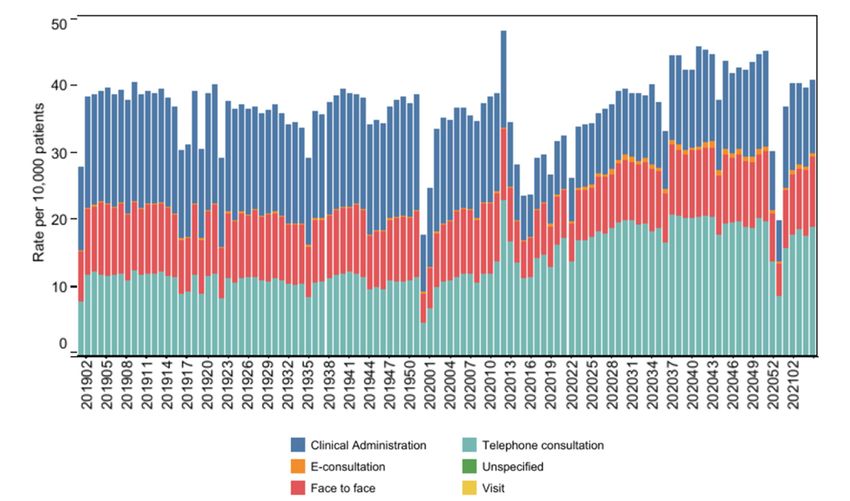
47
Primary Care Informatics Response to Covid-19 Pandemic: Adaptation, Progress, and Lessons from Four Countries with High ICT Development
these codes. Challenges with the new billing Virtual care can increase or decrease ineq- policy, with practices largely left to create
codes for virtual visits included delayed uitable access. For Canadians living in rural their own policies [46]. PPE other than
payments [15]. There were documented de- or remote regions, including First Nations face masks, plastic aprons and gloves were
creases in the use of PC services, likely due communities, and individuals facing barri- initially in short supply [47].
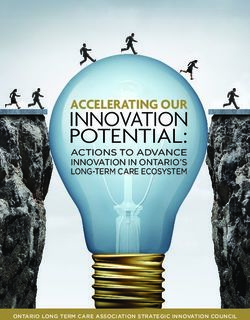
to patients self-isolating at home, worries ers related to mobility, travel costs and time There was initially a drop in the total num-
about overstressing the healthcare system and constraints, virtual care has been decidedly ber of consultations associated with a rise in
a perceived risk of COVID-19 exposure in beneficial [41]. In contrast, PCPs worry this non-face-to-face with a return to normal rates
healthcare settings [28]. Reductions in contact technology may perpetuate health disparities of consulting within 12 weeks (Fig. 2). There
with PC have reduced routine preventative among seniors, individuals with disabilities, was a move to more non-face-to-face con-
care, mental health care, and delayed immuni- populations with language barriers, and those sulting, overwhelmingly by telephone, though
zations. Many physicians are concerned about who cannot afford or use technology [42]. the latter included sharing of photographs by
long-term health impacts [33]. Decreased Just as expectations for the continued email, with only a small rise in e-consultations.
patient visits and delayed payments, coupled expansion and use of virtual care are in- In the week that lockdown was announced a
with the adoption of new digital workarounds creasing, so does a need for the appropriate record number of patients did not attend their
have resulted in financial challenges for many health education, clinician training, and peer consultations (Fig. 3). In a study of people 65
practices [33]. However, despite reduced networks [43]. years and older, it did not appear that the shift
practice hours, most family physicians have to non-face-to-face increased disparities [48].
not shut down their offices [34]. d Next steps: What has Canada learned
from COVID-19? c Implications for primary care informatics
c Implications for primary care informatics COVID-19 like any pandemic or public The service showed speed and adaptability.
These are positive and negative. While more health emergency, requires integration A national notice allowing data sharing
care could be offered virtually [30], it is across sectors of society. A strong primary over the COVID-19 pandemic has allowed
recognized this will not eliminate in-person care-public health interface is critical. Pa- innovations in data use including OpenSafely
visits for physical examinations and medical tient and PCP input is important in address- (opensafely.org).
procedures. The potential to increase produc- ing equity and access for vulnerable popula- Coding: At the start of the pandemic there
tivity is challenged by PCPs’ preoccupation tions. Standards for privacy and security of were no codes to record COVID-19 infection
with complexities such as figuring out what is virtual care are necessary. Medical/health in primary care CMR systems. CMR system
essential versus non-essential care, redirecting education and training is important to ensure medical directors created temporary codes
patients for tests and procedures, organizing a competent workforce. While COVID-19 within days, later replaced with substantive
schedules, sanitizing office space, and learning has highlighted the need for virtual care, SNOMED clinical terms, though the latter
new protocols and technologies [33]. There effective implementation and adoption is took two iterations [49]. Subsequently these
is no one-size-fits-all solution for informatics still a long way off [5, 44]. had to be developed into an ontology to
support as some tasks are better support- enable virologically confirmed, clinically
ed virtually than others. Guiding patients likely, possible and virologically negative
through physical exam tasks such as a hernia 4.3 United Kingdom cases to be differentiated in routine data [50].
diagnosis can be a challenge [35]. In contrast a Healthcare system Success of the linkage technology in
to diagnostic tasks such as cancer screening, NHS spine: The NHS spine includes a
The UK National Health Service (NHS) pro-
mental health care and ongoing management personal demographics service within the
vides a free service at point of care. Primary
of chronic conditions are areas where virtual secure NHS network. This lets data about
care is a registration-based system largely
care could be particularly impactful [36]. a patient to be linked and shared. This has
delivered through independent general prac-
Many areas of Canada had been working been particularly important for the large-
tices, and consultations have been recorded
on telehealth solutions prior to COVID-19 scale testing offered for COVID-19 enabling
into computerised medical record (CMR)
[37, 38]. However, with the need to deploy fast results to be filed into the relevant patient’s
systems for some years [45]. Each patient
and easy virtual care, PCPs were compelled primary care record, and early reporting of
is registered with a single general practice.
to decide on eHealth tools on their own and disparities in those with COVID-19 [50].
A unique personal identifier, NHS number,
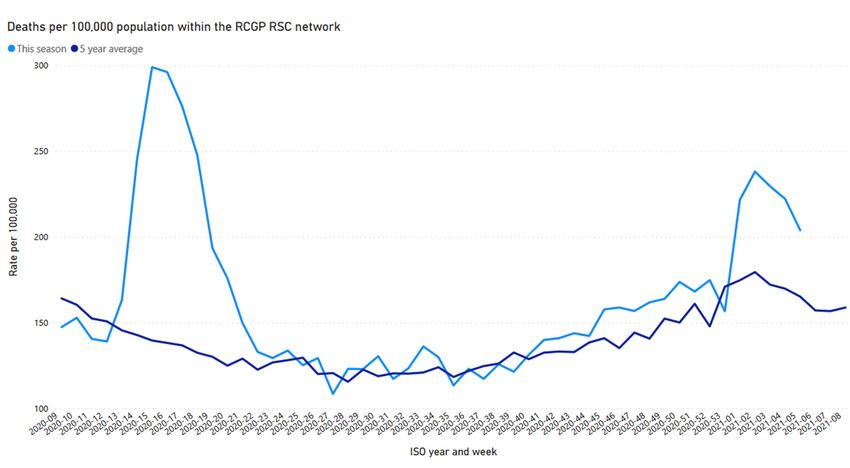
learn how to use them [35]. However, the Mortality data: Mortality data are also
links an individual’s records across the NHS.
need to develop telehealth systems that meet shared via the NHS spine, enabling rapid
standards for secure use, communication, and identification of the peak in mortality asso-
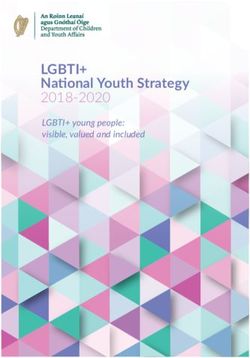
storage of digital health information may be b COVID-19 impacts on primary care ciated with the first COVID-19 peak (Fig.
compromised as patients and physicians turn delivery in UK 4). This has enabled contemporaneous data
to more user-friendly, but potentially insecure COVID-19 had a big impact on primary care to report rates of mortality [51], both those
video call platforms instead of tools endorsed delivery as there was uncertainty about what across the population [52] and those with
by health authorities [36, 39-41]. constituted an effective infection control known COVID-19 status [53].
IMIA Yearbook of Medical Informatics 2021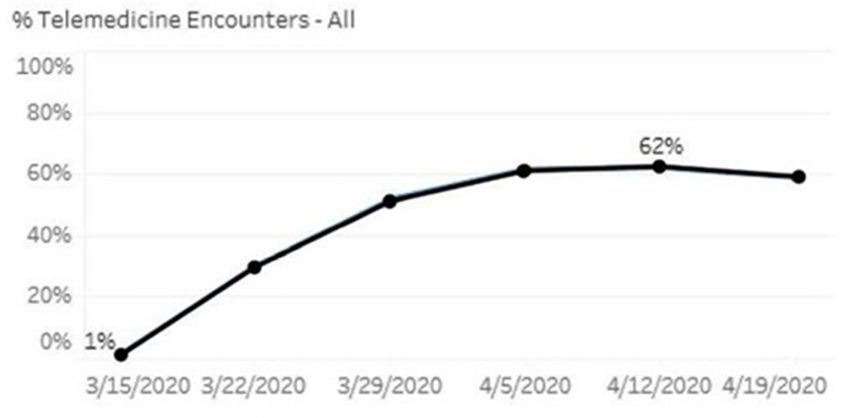
48 Liaw et al. Fig. 2 Weekly consultations by GPs in UK primary care, week 40 of 2018 to week 47 of 2020. In week 12 of 2020, (202012) lockdown was announced and there was a drop in overall consulting. Home visit rates and face to face in surgery declined, clinical administration (including text and email) and telephone consulting increased. Fig. 3 Rate of failed encounters / did not attend in UK primary care. Week 12 of 2020 was the highest ever recorded for not attending. The rates of non-attendance have not changed with lockdown. IMIA Yearbook of Medical Informatics 2021
49
Primary Care Informatics Response to Covid-19 Pandemic: Adaptation, Progress, and Lessons from Four Countries with High ICT Development
Fig. 4 Mortality in week 49 of 2019 (2019-48), to week 08 of 2021 (2021-08) in people 75 years old and older. The light blue line represents this year, with the peak coinciding with the first wave of COVID-19, the dark
blue line the 5-year mortality average.
d Next Steps: what has UK learned from had already increased by 154% compared sitioning care into larger clinics. Staff were
COVID-19? to 2019 [57]. One insurance plan reported redeployed to primary care offices. The elec-
The implementation of digital systems ac- a peak in televisits to nearly 18 visits per tronic health record (EHR) technical teams
celerated, and there has been a groundswell 1000 enrolees, but with wide geographic completed all configurations, templates and
of willingness of GPs to share data. The Ox- variation [58]. Some specialists, e.g., oph- phrases, billing and coding changes, and
ford-Royal College of General Practitioners thalmologists could not accommodate the technical set-up for televisits in a few weeks,
(RCGP) Research and Surveillance Centre need. By Spring many facilities reported similar to experiences elsewhere in USA
(RSC), one of Europe’s oldest sentinel sys- that c.75% of their ambulatory visits were [59-63]. Use of telehealth increased rapidly
tems, trebled its membership over the course virtual, including visits for patients with to a peak of c. 62% outpatient encounters
of the pandemic [54, 55], and created a range SARS-CoV-2. The US Centers for Medicare (Figure 5). Use depended on technical con-
of interactive observatories [56]. This will and Medicaid Services (CMS) authorized siderations and whether it was to manage
address the slowness of agencies involved in payment for both video and phone based chronic care patients, which was simpler
data linkage to actually share data, even for televisits during COVID-19. than managing acute problems that required
what have been designated high-priority pub- physical examinations.
lic health studies. The four nations that make The few reports regarding implemen-
b Case study: COVID-19 impacts on tation of telehealth systems in response to
up the UK have separate rules and policies. primary care delivery at Geisinger Health the COVID-19 pandemic come from large
System in Pennsylvania centers similar to Geisinger, including the
COVID-19 cases in central Pennsylvania University of California, San Diego [64], the
4.4 United States of America peaked initially in early May, then decreased Veterans Administration [59, 60], Boston’s
a Healthcare system until late fall into January 2021 when Children’s Hospital [65], and a few private
Telehealth in the USA prior to COVID-19 case numbers exceeded the spring peak. practices as part of larger academic medical
was largely the province of psychiatrists and Telehealth enabled Geisinger to continue centers [66]. However, it must be noted that
psychologists. As lockdowns occurred across operations during COVID-19 by decreasing the Geisinger experience may not represent
the nation, televisits increased exponentially all nonacute visits within primary care sites, the experience across the USA, even for
for all clinicians. By March 2020 televisits temporarily closing small clinics, and tran- similar sized integrated health systems.
IMIA Yearbook of Medical Informatics 202150
Liaw et al.
The COVID-19 pandemic revealed exten-
sive gaps in the ability of the US to respond
[75]. Lacking a coherent national COVID-19
response policy, it was left to each state and
indeed each hospital system and clinic to de-
velop its own operations [76]. Furthermore,
each state licenses its clinicians, and there
are no consistent regulations or cross-state
agreements for care of patients living close
to state borders [77].
d Next Steps: What has USA learned from
COVID-19?
A national not jurisdictional strategy is re-
quired to coordinate digital health laws and re-
Fig. 5 At its peak in the spring of 2020, telemedicine accounted for 62% of all outpatient encounters in the Geisinger Health System. imbursement. Foremost among the needs is a
national policy requiring cross-state privileges
to accommodate both clinicians and patients
who live close to a state border and provide
A telemedicine app integrated with the in-person physical exam beyond simply or seek services on both sides. Financial
Geisinger EHR system, enabled seamless observing the patient virtually. Further and political support for high-speed internet
encounter documentation through templated research of these areas is mandatory. everywhere is critical for sustained success
notes, shortcut phrases for routine documen- Sufficient bandwidth for both audio and of telehealth. Addressing the challenges and
tation, and appropriate phrases to document video connections depends on high-speed making these regulatory changes will funda-
specifics of televisits per legal and billing internet, not available in rural areas or afford- mentally alter primary care provision in the
requirements. Similar shortcuts were built able to the poor [69]. “Last mile” connec- United States [78, 79]. Telehealth appears to
to communicate test results to patients and tions are problematic, even in urban areas. be firmly established in primary care, and
work excuses to employers. People may have smartphones but cannot adequate resources made available to sustain
Prior to COVID-19, there was no co- afford Internet access, raising problems of it into the post-pandemic era, including man-
herent national policy, consistent national finding Wi-Fi hotspots that also offer privacy aging subsequent pandemics [80].
reimbursement or incentives to establish and security. Many telehealth applications,
the informatics structure to support tele- especially those tethered to an EHR, require
health. This accelerated with the pressing encryption and/or compliance with the 4.5 An International Perspective
clinical, social and public health needs from Health Insurance Portability and Account-
COVID-19. Telehealth practice increased ability Act, which may not be compatible from Some Countries with Lower
exponentially across the USA [67]. Reser- with cell phone use. A risk of this inequity ICT Developments
vations about telehealth included fear that is that rural PCPs will be unduly burdened COVID-19 triggered many similar innova-
postponed elective surgeries or unmanaged with sicker patients [70]. tions in Indo-Pacific countries with high ICT
chronic diseases will result in more care Setting up televisits was easier for PCPs developments such as China, South Korea
requiring emergency attendances and hos- with mature EHRs, especially those with and Singapore. A comparison with countries
pitalizations [68]. available telehealth modules. The more agile with lower ICT developments , such as India
clinician offices with flexible scheduling suc- and Pacific Island Countries (PIC), will be
ceeded early, especially if they had institution- more meaningful.
c Implications for primary care informatics al support. The cessation of elective surgeries,
There are informatics, technical, and ed- decreased office visits, limited reimbursement
ucational challenges. Training for a new for telehealth, and patients not attending rou- a Pacific Island Countries
technology is difficult for both providers tine visits will reduce income and threaten the At the least developed end of the ICT devel-
and patients alike. There is little to no financial viability of small practices [71]. The opment scale [7] are the small and sparsely
empiric research supporting the efficacy CMS expanded telehealth payments for home populated PIC. Primary care is the centre of
or efficiency of telehealth, or the long-term health agencies [72], but payment for mental the health system. The digital health maturity
consequences. The literature is largely rap- health televisits will continue [73]. Some of PIC is generally low, as assessed by con-
id-cycle, non-peer reviewed articles. There insurance companies have already increased sidering four essential digital health foun-
are concerns about foregoing a regular telehealth costs to patients [74]. dations: ICT infrastructure, essential digital
IMIA Yearbook of Medical Informatics 202151
Primary Care Informatics Response to Covid-19 Pandemic: Adaptation, Progress, and Lessons from Four Countries with High ICT Development
health tools (e.g., Unique ID, EHRs and data raises privacy issues with telehealth. India cial telehealth systems need to be monitored
quality), readiness for information sharing and many low-and-middle-income-countries for compliance to technical, privacy and
(e.g., interoperability and enterprise archi- (LMICs) are also experiencing decreased use security standards.
tecture) and environment to support adoption of health services, especially for chronic dis- Countries where healthcare is decentral-
(e.g., capacity building, regulations) [1, 81]. ease management. A nationwide COVID-19 ized to individual provinces, territories, or
However, telecommunication is fairly well telephone helpline to complement telehealth states present different challenges than in
developed to support telemedicine with over- services and improve patient and work- countries where healthcare delivery is cen-
seas medical facilities. Most are developing force capability was not well received. The trally funded and delivered. The UK system
a national digital health strategy using the WHO-ITU collaboration to directly text the is centrally funded with autonomy devolved
World Health Organization (WHO) and In- public in LMICs with COVID-19 related to its four nations. The politics, funding,
ternational Telecommunication Union (ITU) information was not adopted or adapted to models of care, and governance of health and
framework [82]. Fortunately, COVID-19 has any significant extent [87]. social services are important determinants
not been prevalent in the PICT. Nevertheless, Data quality and interoperability remain of variations in the COVID-19 response.
local physical and digital arrangements, significant challenges to the development of Cross-country comparisons must also consid-
based on the WHO Early Warning, Alert and an integrated system to address pandemics er culture and contexts. For example, Israel’s
Response System [83], are in place to deal into the future. Data collection and manage- vaccine delivery model has been heralded as a
with disease outbreak in emergencies such ment systems are often a hybrid of paper and successful model to emulate [88], but Israel’s
as natural disaster or epidemics as well as digital, resulting in inefficiencies and data centralized healthcare delivery approach and
support the vaccine strategy. These arrange- security issues. relatively small geographic and population
ments will be well and truly tested with the There are many PCI tools readily avail- size (9M) can make comparisons inaccurate
recent COVID-19 outbreak in March 2021 able to address the data, information and and unfair, even with countries with similar
in Papua New Guinea. socio-technical aspects of COVID-19. How- ICT developments [89].
ever, despite technical guidance from WHO We report our findings in two sections:
to support digital health, countries like India the first describing how there has been
b India have yet to implement policies and regulations accelerated but patchy progress, the second
The Indian health system is a federated mod- at state and national levels. There is an emerg- addressing lessons for the future.
el with state and central governments having ing and encouraging shift to a co-creation
responsibility for various aspects of health. approach to digital health maturity assessment
There are significant urban-rural, socioeco- to guide national digital health strategy devel-
nomic and gender divides. India aspires to opment to address COVID-19 and its sequelae 5.1 Accelerated but Patchy Progress
a national digital health system to facilitate on service delivery [1]. Accelerated uptake of telehealth was experi-
the achievement of universal health coverage enced across all the countries, with important
and United Nations sustainable develop- variations in the strategies to protect vulner-
ment goals. State and central governments able and older people. All countries shared
implemented lockdowns early, introducing
targeted COVID-19 clinics and provided
5 Synthesis and Discussion the value inherent in maintaining quality
safeguards in health services [90].
PPE and infection control training to PCPs, Table 1 synthesizes the findings into a set Challenges were partly due to regulatory
focusing on early detection, controlling of seven themes, categorized into clinical differences between jurisdictions in digital
transmission and providing uninterrupted and public health and informatics and data health, information sharing and interopera-
essential primary care services [84]. science issues. Our analysis considered the bility [2]. Clinical effectiveness and safety
Telehealth initiatives in India have been ITU-ICT rankings of the six countries. The is important, but a successful response
struggling to gain momentum for many commonalities and variations in the PCI to COVID-19 requires a strong primary
years [85]. Despite high penetration, mobile response to COVID-19 emphasises that care-public health interface and standardised
phones are not frequently used for health ser- digital health maturity includes quantitative information exchange. COVID-19, as with
vices [81]. Reimbursement for telehealth and measures of ICT developments and other any public health emergency, requires a
telemonitoring services provided by PCPs sociotechnical determinants, including coordinated national multisectoral response.
remain ad hoc. Telemedicine Practice Guide- ensuring data quality, interoperability and Despite a strong national primary care and
lines for COVID-19 patients were issued on readiness for information sharing, and an digital health system, the UK has been
March 25, 2020 [86]. However, the general environment and culture to build capacity unable to limit the spread of COVID-19
fragmentation of the digital health system and support adoption [1, 81]. Health and because of delayed and inconsistent poli-
and tools, including between public and pri- digital literacy of healthcare professionals cy decisions on public health approaches
vate sectors, posed significant feasibility and and citizens are also important, as is previous based on social distancing and community
acceptability challenges. Low mobile phone experience with epidemics such as SARS in testing. It may also be due to the balance of
ownership especially among Indian women the COVID-19 context. Standalone commer- public and private providers in Australia and
IMIA Yearbook of Medical Informatics 202152
Liaw et al.
Table 1 Themes for PCI response for global pandemic
Theme International lessons
Clinical & public health
1 The COVID-19 pandemic onset was associated with an abrupt Lesson: Future pandemics contingency plans need to be made so that care usually delivered
fall in in-person consultations. face-to-face can switch to virtual. We need the technical, legislative, financing and
contractual frameworks to do this as standard.
2 The “new normal” will include increased non-face-to-face Lesson 1: We should keep the capability to step away from non-face-to-face care in future for
consultation. doctor, service or patient convenience.
Lesson 2: Where safe and convenient to patients, this as an opportunity to reset care.
However, both lessons need to be underpinned by research on how to do it safely.
3 Fears of primary care clinicians that patients were delaying care Lesson: We need robust international research as to whether this is real (likely is), what
despite the availability of televisits. exacerbated it, and what mitigated patients’ willingness to access primary care.
4 Coordinated national programs seem to have worked better to Lesson 1: We need empiric public health research to establish if national priorities, as
control spread of the disease opposed to local jurisdiction, leads to reduced spread of disease and lower mortality.
Lesson 2: The WHO, in coordination with other international agencies, needs to develop plans
acceptable to the world’s nations, to control pandemics on an international scale.
5 The digital divide in the pandemic was global. Lesson: We have a societal responsibility to correct uneven distribution of internet availability
for healthcare delivery. This should include equitable access to the internet and adequate
bandwidth for eHealth delivery; eHealth needs eAccess.
Informatics and data science
6 Inability to code SARS-COV-2 in the pandemic. There was an Lesson 1: The WHO working with others needs to have contingencies in place that work
international lack of clinical terms for coding standards. across terminologies (e.g., International Classification of Disease (ICD), SNOMED CT, and the
International Classification of Primary Care (ICPC)).
Lesson 2: We need to avoid frequent reclassification of pandemic diseases. There have been
three sequential reclassifications of COVID-19.
7 Variability across regions and jurisdictions in how they recorded, Lesson: Future preparedness needs to go beyond coding. There should be common data
coded, modelled, and managed key data during the pandemic, models created to facilitate sharing data about pandemic disease spread, testing (which may
making lessons harder to learn globally. be virological or serological), vaccine coverage, vaccine effectiveness and any adverse events
of interest.
Canada that has enabled its health system to The primary care data required to success- These obstacles need to be overcome if we
adapt with greater speed and agility than fully identify, manage and monitor pandem- are to ever offer truly integrated care services.
systems that are mainly publicly funded ics is most advanced in the UK. The use of Locally-based primary care organisa-
[24] or mainly privatised. real-world data from GP systems and record tions appear to have rapidly responded by
The equity issue and the general lack of linkage through the NHS spine is a model for adapting their services to ensure continued
evidence for safety and effectiveness of tele- other countries, recognising that the political equitable access by vulnerable populations
health compared to “in-person” encounters and policy environment needs to be support- to primary care services [42].
must be addressed. In addition to a rebalancing ive. Adopting international standards such as COVID-19 has embedded telehealth
of spending, lessons from COVID-19 to create SNOMED will make primary care data more more firmly in primary care. Virtual care
a more equitable and effective primary health compliant with FAIR (Findable, Accessible, will almost certainly find a stronger place
care system include: provide health services Interoperable, and Reusable) principles [92]. within health service models and is likely
where people are, e.g., expanding the network to have increased acceptance among both
of community health centres including those patients and health care providers. How-
in schools and housing complexes; improving ever, it is important to recognise that each
inter-racial communication and trust includ- 5.2 Lessons for the Future country is at a different level of digital
ing culturally competent health coaches; Timely access to quality data has been a health maturity and has different health
strengthen the caregiving workforce for older major PCI challenge. Though different health priorities [1, 81].
adults including staff in nursing homes and systems have billing and clinical diagnosis PCI is key to any digital health strategy,
home-based caregiving systems; and provide provisions for new services during pandem- and we must maintain the progress made
equitable or universal health insurance [91]. ics, provisions for data sharing are lacking. during COVID-19. Telehealth and EHR
IMIA Yearbook of Medical Informatics 202153
Primary Care Informatics Response to Covid-19 Pandemic: Adaptation, Progress, and Lessons from Four Countries with High ICT Development
systems underpinned the ability of primary Information Management 2019;49:343-54. from: https://apps.apple.com/au/app/total-cardi-
care to be flexible in-pandemic response. 6. Jonnagaddala J, Guo GN, Batongbacal S, Marcelo ac-care/id1437138162
A, Liaw S-T. Adoption of enterprise architecture 21. Australian Government Department of Health.
However, neither primary care nor PCI can for healthcare in AeHIN member countries. BMJ Electronic prescribing. Australian Government
be considered in isolation from the wider Health Care Inform 2020;27(1):e100136. Department of Health [Internet]; 2020. Updated
health system or health policy context. 7. International Telecommunication Union. Mea- 13 Nov 2020. [cited 2020 Nov 15]. Available from:
suring digital development. Facts and figures https://www.health.gov.au/initiatives-and-pro-
2020. Geneva: Internatiomal Telecommunication grams/electronic-prescribing
Union;2020. 22. The University of Queensland Centre for Online
Health. Telehealth and coronavirus: Medicare
8. Duckett S. What should primary care look like
6 Conclusion after the COVID-19 pandemic? Aust J Prim Health
2020;26(3):207-11.
Benefits Schedule (MBS) activity in Australia.
University of Queensland [Internet]; 2020 [cited
2020 Nov 14]. Available from: https://coh.centre.
We have conducted case studies in four 9. Desborough J, Dykgraaf SH, de Toca L, Davis S, uq.edu.au/telehealth-and-coronavirus-medi-
countries with well-developed ICT sys- Roberts L, Kelaher C, et al. Australia’s national care-benefits-schedule-mbs-activity-australia
tems and examined reported pandemic COVID‐19 primary care response. Med J Aust 23. Helsper CW, Campbell C, Emery J, Neal RD, Li L,
2020;213(3):104-106.e101. Rubin G, et al. Cancer has not gone away: A prima-
responses in two less-developed countries. 10. Snoswell CL, Caffery LJ, Haydon HM, Thomas ry care perspective to support a balanced approach
Response was accelerated but progress was EE, Smith AC. Telehealth uptake in general prac- for timely cancer diagnosis during COVID-19. Eur
patchy. Improved access to good quality tice as a result of the coronavirus (COVID-19) J Cancer Care (Engl) 2020;29(5):e13290.
data and a standardised approach to infor- pandemic. Aust Health Rev 2020;44(5):737-40. 24. Wright M, Versteeg R, Hall J. General practice’s
11. Snoswell C, Caffery L, Hobson G, Taylor ML, early response to the COVID-19 pandemic. Aust
mation-sharing and development of digital Haydon HM, Thomas E, et al. Telehealth and Health Rev 2020;44(5):733-6.
tools to support telehealth and virtual care coronavirus: Medicare Benefits Schedule (MBS) 25. Canadian Medical Association-Royal College
is foundational. Well-coordinated national activity in Australia. Centre for Online Health, of Physicians & Surgeons of Canada-College of
response and governance is essential, es- The University of Queensland; 2020. Updated Family Physicians of Canada. How to navigate a
May 19, 2020 [cited 2021 Feb 7]. Available from: virtual care visit: patient guide. Canadian Medical
pecially across the primary care and public https://coh.centre.uq.edu.au/telehealth-and-coro- Association [Internet]; 2020 [cited 2020 Nov 14].
health sectors. The informatics and digital navirus-medicare-benefits-schedule-mbs-activi- Available from: https://www.cma.ca/how-navi-
health responses to the COVID-19 pandemic ty-australia gate-virtual-care-visit-patient-guide
must not compromise privacy, security, data 12. Pearce C, McLeod A, Gardner K, Supple J, Epstein 26. Canadian Healthcare Technology. SK deploys
D, Buttery J. THE GP Insights Series no 7: Primary COVID-19 e-referral and intake system. Cana-
quality and interoperability standards and Care and SARS-CoV-2: The first 40 weeks of the dian Healthcare Technology [Internet); 2020.
other design issues. pandemic year. Melbourne: Outcome Health; 26 [cited 2020 Nov 14]. Available from: https://www.
October 2020. canhealth.com/2020/08/19/sk-deploys-covid-19-e-
Acknowledgements 13. Clark M, Brewster D, Jones L, Dhaliwal JS, Teng referral-and-intake-system/
J. Uncertainty and fear: aged care in a time of 27. Island Health. Hospital at Home - Victoria General
Patients and health providers who have al- COVID-19. MJA Insights+ 2020(44). Hospital Prototype. Island Health [Internet]; 2020.
lowed data sharing that enabled primary care 14. Baird A. Video communication for GPs and pa- [cited 2020 Nov 14]. Available from: https://www.
informatics organisations to contribute to the tients. MJA Insight+ 2020(32). islandhealth.ca/our-services/hospital-home-ser-
management of the COVID-19 pandemic. 15. Car J, Koh GC-H, Foong PS, Wang CJ. Video vices/hospital-home
consultations in primary and specialist care 28. Huston P, Campbell J, Russell G, Goodyear-Smith
during the covid-19 pandemic and beyond. BMJ F, Phillips Jr RL, van Weel C, et al. COVID-19
2020;371:m3945. and primary care in six countries. BJGP Open
References 16. Medicare Australia. Medicare Benefits Schedule 2020;4(4):bjgpopen20X101128.
29. Bhattacharyya O, Agarwal P. Adapting primary care
(MBS) Online. Medicare Australia [Internet];
1. Liaw S-T, Zhou R, Ansari S, Gao J. Digital Health 2020. [cited 2020 Nov 8]. Available from: http:// to respond to COVID-19. Can Fam Physician 2020.
Profile and Maturity Assessment Toolkit: co-cre- www.mbsonline.gov.au/internet/mbsonline/pub- 30. Canadian Medical Association. What Canadians
ation in the Pacific Islands. J Am Med Inform lishing.nsf/Content/Home think about virtual health care. Canadian Medical
Assoc 2020 Nov 29:ocaa255. Association [Internet]; 2020. [cited 2020 Nov 14].
17. The Royal Australian College of General Prac-
2. Webster P. Virtual health care in the era of Available from: https://www.cma.ca/sites/default/
titioners. General Practice: Health of the Nation
COVID-19. Lancet 2020;395(10231):1180-1. files/pdf/virtual-care/cma-virtual-care-public-poll-
2020. East Melbourne, Vic: RACGP;2020. june-2020-e.pdf
3. Maldonado JMSdV, Marques AB, Cruz A. Tele- 18. Meidibank Australia. Telehealth support. Look
medicine: challenges to dissemination in Brazil. 31. Canadian Institute for Health Information. Phy-
after your health from home with Telehealth. sician billing codes in response to COVID-19.
Cadernos de Saúde Pública [Internet]. 2016 [cited Medibank [Internet]; 2020 [cited 2020 Nov 14].
2021 Feb]; 32(Suppl2):e00155615. Available from: Canadian Institute for Health Information [Inter-
Available from: https://www.medibank.com. net]; 2020. [cited 2020 Nov 14]. Available from:
https://www.scielo.br/scielo.php?script=sci_art- au/health-support/hospital-assist/covid19/tele- https://www.cihi.ca/en/physician-billing-codes-in-
text&pid=S0102-311X2016001402005 health-services/ response-to-covid-19
4. Grönqvist H, Olsson EMG, Johansson B, Held 19. Celler B, Varnfield M, Nepal S, Sparks R, Li J, 32. Ontario Health Insurance Plan. Bulletin Number:
C, Sjöström J, Lindahl Norberg A, et al. Fifteen Jayasena R. Impact of At-Home Telemonitoring 4745: Keeping Health Care Providers informed
Challenges in Establishing a Multidisciplinary on Health Services Expenditure and Hospital of payment, policy or program changes. Ministry
Research Program on eHealth Research in a Uni- Admissions in Patients With Chronic Conditions: of Health [Internet]; 2020. Updated 2020 Mar
versity Setting: A Case Study. J Med Internet Res Before and After Control Intervention Analysis. 13. [cited 2021 Feb 7]. Available from: http://
2017;19(5):e173. JMIR Med Inform 2017;5(3):e29. www.health.gov.on.ca/en/pro/programs/ohip/
5. Champion C, Kuziemsky C, Affleck E, Alvarez 20. The University of New South Wales. Total Cardiac bulletins/4000/bul4745.aspx
GG. A systems approach for modeling health Care. UNSW Graduate School of Biomedical En- 33. Wong S, The Primary and Integrated Health Care
information complexity. International Journal of gineering [Internet]; 2020 [cited 2020]. Available Innovations Network. Quick COVID-19 Primary
IMIA Yearbook of Medical Informatics 202154
Liaw et al.
Care Survey of Clinicians: Summary of the a cross-sectional database study in the UK. Br J 61. Sinha S, Kern LM, Gingras LF, Reshetnyak E,
pan-Canadian survey of frontline primary care cli- Gen Pract 2020;70(697):e540. Tung J, Pelzman F, et al. Implementation of Video
nicians’ experience with COVID-19, series 6-11. In: 49. de Lusignan S, Williams J. To monitor the Visits During COVID-19: Lessons Learned From
Annals of Family Medicine, COVID-19 Collection. COVID-19 pandemic we need better quality a Primary Care Practice in New York City. Front
Deepblue: University of Michigan; 2020. primary care data. BJGP Open 2020;4(2):bjg- Public Health 2020;8:514-22.
34. Ontario College of Family Physicians. Family popen20X101070. 62. Srinivasan M, Asch S, Vilendrer S, Crandall
Doctors are Open and Here for Care, and More. 50. de Lusignan S, Dorward J, Correa A, et al. Risk Thomas S, Bajra R, Barman L, et al. Qualitative
Ontario College of Family Physicians [Internet]; factors for SARS-CoV-2 among patients in the Assessment of Rapid System Transformation to
2020. [cited 2020 Nov 14]. Available from: https:// Oxford Royal College of General Practitioners Primary Care Video Visits at an Academic Medical
www.ontariofamilyphysicians.ca/news-features/ Research and Surveillance Centre primary care Center. Ann Intern Med 2020;173(7):527-35.
family-medicine-news/~188-Family-Doctors-are- network: a cross-sectional study. Lancet Infect Dis 63. Smith WR, Atala AJ, Terlecki RP, Kelly EE,
Open-and-Here-for-Care-and-More 2020;20(9):1034-42. Matthews CA. Implementation Guide for Rapid
35. Glauser W. Virtual care is here to stay, but major chal- 51. Joy M, Hobbs FDR, McGagh D, Akinyemi O, de Integration of an Outpatient Telemedicine Program
lenges remain. CMAJ 2020;192(30):E868-E869. Lusignan S. Excess mortality from COVID-19 in During the COVID-19 Pandemic. J Am Coll Surg
36. Deloitte Centre for Health Solutions. COVID-19 an English sentinel network population. Lancet 2020;231(2): 216-222.e2
Virtual care is here to stay. Deloitte Canada; 2020. Infect Dis 2020 Aug 4;S1473-3099(20)30632-0. 64. Reeves JJ, Hollandsworth HM, Torriani FJ, Taplitz
37. Gagnon M-P, Julie D, Fortin J-P. A survey in 52. de Lusignan S, Joy M, Oke J, McGagh D, Nichol- R, Abeles S, Tai-Seale M, et al. Rapid Response to
Alberta and Quebec of the telehealth applica- son B, Sheppard J et al. Disparities in the excess COVID-19: Health Informatics Support for Out-
tions that physicians need. J Telemed Telecare risk of mortality in the first wave of COVID-19: break Management in an Academic Health System.
2007;13(7):352-6. Cross sectional study of the English sentinel net- J Am Med Inform Assoc 2020 Jun 1;27(6):853-9.
38. O’Gorman LD, Hogenbirk JC, Warry W. Clinical work. J Infect 2020;81(5):785-92. 65. Hron JD, Parsons CR, Williams LA, Harper MB,
Telemedicine Utilization in Ontario over the On- 53. Joy M, Hobbs FDR, Bernal JL, Sherlock J, Amir- Bourgeois FC. Rapid Implementation of an Inpa-
tario Telemedicine Network. Telemed J E Health thalingam G, McGagh D et al. Excess mortality tient Telehealth Program during the COVID-19
2015;22(6):473-9. in the first COVID pandemic peak: cross-sectional Pandemic. Appl Clin Inform 2020;11(3):452-9.
39. Bhatia RS, Falk W, Jamieson T, Piovesan C, Shaw analyses of the impact of age, sex, ethnicity, house- 66. Sinha S, Kern LM, Gingras LF, Tung J, Pelzman
J. Virtual health care is having its moment. Rules hold size, and long-term conditions in people of F, et al. Implementation of Video Visits During
will be needed. Healthydebate [Internet]; 2020. known SARS-Cov-2 status in England. Br J Gen COVID-19: Lessons Learned From a Primary Care
[cited 2020 Nov 14]. Available from: https:// Pract 2020:bjgp20X713393. Practice in New York City. Front Public Health
healthydebate.ca/opinions/virtual-health-care- 54. de Lusignan S, Lopez Bernal J, Zambon M, 2020;8:514.
rules-covid Akinyemi O, Amirthalingam G, Andrews N, et al. 67. Ranney ML, Griffeth V, Jha AK. Critical Supply
40. Appia V. What does the future of telemedicine look Emergence of a Novel Coronavirus (COVID-19): Shortages — The Need for Ventilators and Per-
like in Ontario after COVID-19? Toronto.com [In- Protocol for Extending Surveillance Used by sonal Protective Equipment during the Covid-19
ternet]; 2020. [cited 2020 Nov 14]. Available from: the Royal College of General Practitioners Pandemic. N Engl J Med 2020;382(18):e41.
https://www.toronto.com/news-story/9966360- Research and Surveillance Centre and Public 68. Brodwin E. With covid-19 delaying routine care
what-does-the-future-of-telemedicine-look-like- Health England. JMIR Public Health Surveill chronic disease startups brace for a slew of com-
in-ontario-after-covid-19-/ 2020;6(2):e18606. plications. Health Tech 2020 Apr 14 [cited 2020
41. MacLeod M. Virtual health care is ‘not the answer 55. de Lusignan S, Bernal J, Byford R, Amirthalingam Nov 14]. Available from: https://www.statnews.
for everything,’ critics warn. CTV News. Coronavi- G. Seasonal influenza surveillance and vaccine ef- com/2020/04/14/with-covid-19-delaying-routine-
rus updates Web site [Internet]; 2020. [cited 2020 fectiveness at a time of co-circulating COVID-19: care-chronic-disease-startups-brace-for-a-slew-of-
Nov 14]. Available from: https://www.ctvnews.ca/ Oxford-Royal College of General Practitioners complications/
health/coronavirus/virtual-health-care-is-not-the- (RCGP) Research and Surveillance Centre (RSC) 69. Jaffe DH, Lee L, Huynh S, Haskell TP. Health
answer-for-everything-critics-warn-1.4939283 and Public Health England (PHE) protocol for Inequalities in the Use of Telehealth in the United
42. Bhatti S, Commisso E, Rayner J. A Rapid Primary winter 2020/21 (Preprint). 2020. States in the Lens of COVID-19. Popul Health
Healthcare Response to COVID-19: An Equi- 56. University of Oxford CIHORG. RCGP RSC Manag 2020;23(5):368-77.
ty-Based and Systems- Thinking Approach to Care COVID-19 Observatory and Coding Guidelines. 70. Summers-Gabr NM. Rural–urban mental health
Ensuring that No One Is Left Behind. Healthc Q University of Oxford [Internet]; 2021. [cited 2021 disparities in the United States during COVID-19.
2020;23(3):29-33. Feb 13]. Available from: https://orchid.phc.ox.ac. Psychol Trauma 2020;12(S1):S222-S224.
43. Bhyat R. Canada’s ‘new normal’ must include virtu- uk/index.php/cov-19/ 71. Basu S, Phillips RS, Phillips R, Peterson LE,
al care. Healthydebate [Internet]; 2020. [cited 2020 57. Koonin LM, Hoots B, Tsang CA, Leroy Z, Farris Landon BE. Primary Care Practice Finances In
Nov 14]. Available from: https://healthydebate.ca/ K, Jolly T, et al. Trends in the Use of Telehealth The United States Amid The COVID-19 Pandemic.
opinions/new-normal-include-virtual-care During the Emergence of the COVID-19 Pandemic Health Aff (Millwood) 2020;39(9):1605-14.
44. Mosnaim GS, Stempel H, Van Sickle D, Stempel — United States, January–March 2020. MMWR 72. United States Centers for Medicare and Medicaid
DA. The Adoption and Implementation of Digital Morb Mortal Wkly Rep 2020 Oct 30;69(43):1595-9. Services (CMS). Home health agencies: CMS flex-
Health Care in the Post–COVID-19 Era. J Allergy 58. Patel S, Mehrotra A, Huskamp H, Uscher-Pines L, ibilities to fight Covid-19. Washington DC: Centers
Clin Immunol Pract 2020;8(8):2484-6. Ganguli I, Barnett ML. Trends in outpatient care for Medicare and Medicaid Services; 2020.
45. Schade CP, Sullivan FM, de Lusignan S, Madeley delivery and telemedicine during the COVID-19 73. US Centers for Medicare & Medicaid Services.
J. e-Prescribing, Efficiency, Quality: Lessons from pandemic in the US. JAMA Intern Med 2021 Mar Medicare telemedicine health care provider fact
the Computerization of UK Family Practice. J Am 1;181(3):388-91. sheet [Internet] 2020. Updated 2020 March 17
Med Inform Assoc 2006;13(5):470-5. 59. Reddy A, Gunnink E, Deeds SA, Hagan SL, Hey- [cited 2021 Feb 6]. Available from: https://www.
46. de Lusignan S, Carlyon T, Lalvani A. Removing worth L, Mattras TF, et al. A rapid mobilization cms.gov/newsroom/fact-sheets/medicare-telemed-
the handle of the Broad Street pump: measures to of ‘virtual’ primary care services in response to icine-health-care-provider-fact-sheet
slow the spread of covid-19 in primary care teams. COVID-19 at Veterans Health Administration. 74. Robbins R, Brodwin E. As insurers move this
BMJ 2020;369:m1841. Healthc (Amst) 2020;8(4):100464-100464. week to stop waiving telehealth copays, patients
47. Dyer C. Covid-19: Doctors make bid for public 60. Spelman JF, Brienza R, Walsh RF, Drost P, may have to pay more for virtual care. STAT+.
inquiry into lack of PPE for frontline workers. Schwartz AR, Kravetz JD, et al. A Model for Rapid Health Tech Web site [Internet]; 2020. [cited 2020
BMJ 2020;369:m1905. Transition to Virtual Care, VA Connecticut Primary Nov 14]. Available from: https://www.statnews.
48. Joy M, McGagh D, Jones N, et al. Reorganisation Care Response to COVID-19. J Gen Intern Med com/2020/09/29/united-healthcare-anthem-tele-
of primary care for older adults during COVID-19: 2020;35(10):3073-6. medicine-coverage-insurers/
IMIA Yearbook of Medical Informatics 2021You can also read