Sleep Basics & Insomnia Review - Alessandra M. Gearhart, MD Clinical Assistant Professor Pulmonary, Critical Care and Sleep Medicine Oklahoma ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sleep Basics & Insomnia Review Alessandra M. Gearhart, MD Clinical Assistant Professor Pulmonary, Critical Care and Sleep Medicine Oklahoma State University Center for Health Sciences
Disclosures No financial disclosures or conflicts of interest related to this presentation.
PART 1
Sleep Basics
Agenda
▫ What is sleep?
▫ Why do we sleep?
▫ Our current sleep crisis.
“ A good laugh and
a long sleep are the
two best cures for
anything.”
Irish Proverb
3
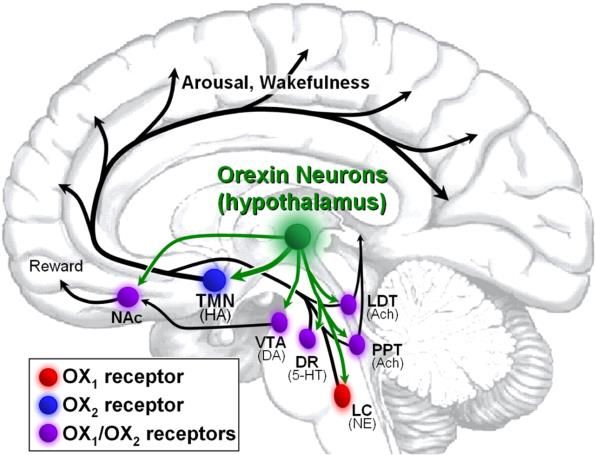
▫ It is not simply the absence of wakefulness What is Sleep?
▫ Complex, reversible state of diminished
responsiveness
▫ Generated and maintained by complex CNS
networks using specific neurotransmitters
located in specific areas of the brain
4
Sleep Architecture
▫ Cyclical pattern of sleep, as we alternate between
different sleep stages
5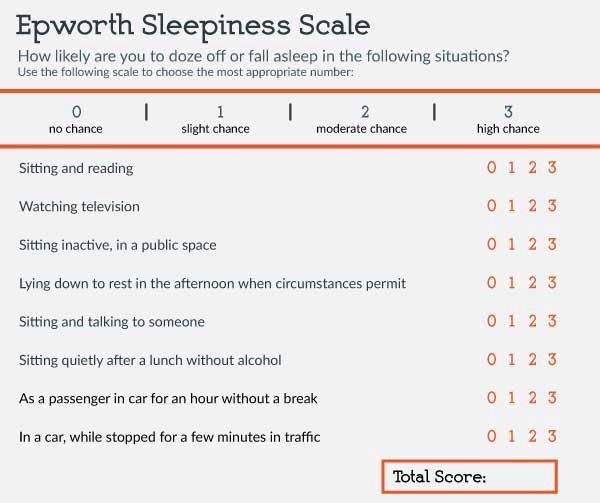
Sleep Stages
▫ Average adult: 7-9h of sleep per night
▫ NREM: 1>2>3, progressively “deeper” sleep.
Tissue repair, immune strength, memory
consolidation.
▫ REM (rapid eye movement): ~every 90 min,
progressively longer periods. Muscle paralysis,
intense dreaming. Processing of emotional
information. REM suppressors: sleep
deprivation, meds (MAOIs, SSRIs, TCAs)
▫ Durations are variable night by night and
patient by patient
6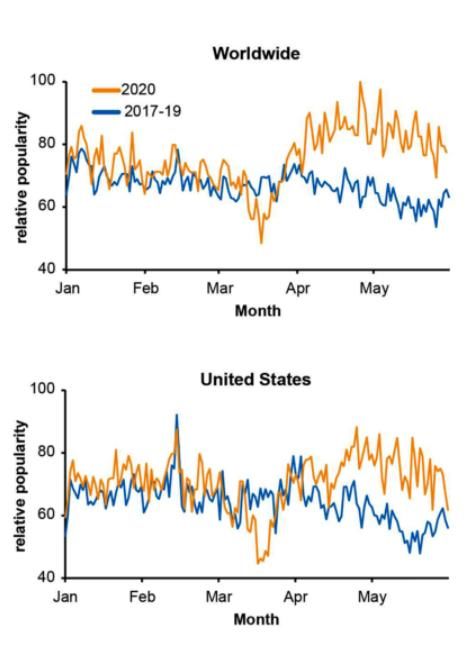
Sleep Trackers
▫ Measure activity or lack thereof, not sleep (EEG)
▫ “Light vs Deep sleep”, “Sleep quality/rating”
▪ Potential for anxiety and obsession about the perfect
sleep: orthosomnia
▫ Useful for some patients, can identify habits and patterns
▪ Bedtime routine
▪ Estimated sleep duration
▪ Week vs Weekend schedules
7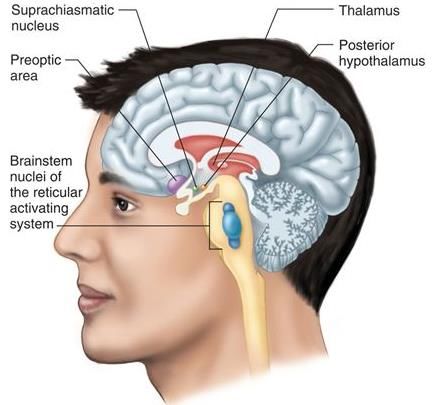
Why do we 1. Neural growth and information processing: brain
sleep? development, restoration, learning, and memory
consolidation. Critical in infants and older children.
2. Restorative tissue growth and repair
3. Regulation of bodily functions: temperature, energy
conservation, toxin removal
4. Survival theory: protective and adaptive behavior
and immune defense
Sleep and
Immunity
▫ Amount of sleep and respect to circadian rhythms
associated with susceptibility to certain diseases and
antibody response to vaccines
9
Our Current Sleep Crisis
▫ Oct 2019
▫ Feb 2021▫ 2.77 million Google searches for
insomnia in US during the first five
months of 2020, 58% increase when
compared to the three previous years
▫ Queries peak at 3am
(Zitting, Holst et al. 2020)Caring for ourselves as we care for our patients
▫ 13 studies; >30,000 participants
▫ Insomnia ~ 35% - sleep quality correlated with level of social
support
▫ Anxiety and depression ~20-25%
▫ Moral injury and PTSD strongly linked to insomnia
(Pappa, Ntella et al. 2020)▫ Most common of all the 70
recognized sleep disorders
Public Health Impact ▫ Increasing burden on primary
care and amount of
Chronic Insomnia prescriptions
▫ Significant knowledge gap on
what is available versus what is
approved and has been
previously studied
13PART 2
Insomnia
Clinical Review Agenda
▫ Diagnosis
▫ Types of Chronic Insomnia
▫ Therapy
▪ Non-pharmacological
▪ Pharmacological
▫ Special populations
14Insomnia:
Diagnostic Criteria
▪ Difficulty initiating or maintaining; despite
adequate opportunity/circumstances
▪ Daytime impairment (fatigue, attention/memory/mood ,
sleepiness, etc)
Chronic Insomnia
▫ At least 3x/week for at least 3 months
▫ Not explained by another sleep disorder
▪ Polysomnogram or actigraphy not routinely indicated
15Common Types of Chronic Insomnia
▫ Psychophysiological: most common, heightened arousal,
excess focus on sleep, lack of daytime sleepiness
▫ Paradoxical: “sleep state misperception”
▫ Insomnia due to drug/substance: use or withdrawal
16✓ General medical/psychiatric
Work-up questionnaire
Important Tools
✓ Epworth Sleepiness Scale
✓ 2-week sleep log
▪ Latency, duration
▪ Naps
▪ Week vs Weekend
17Common Differential Diagnosis
Key Points on History Taking or Associations
▫ Onset vs maintenance + sleep-wake ▫ Insufficient sleep syndrome
schedule ▫ Circadian rhythm disorders: Delayed
or advanced sleep-wake phase
▫ Habits, environment, mental status
around bedtime (sleep hygiene) ▫ Inadequate sleep hygiene
▫ Snoring, gasping, leg movements ▫ Sleep apnea, restless legs syndrome
or periodic limb movement disorder
▫ Medications (including OTC), ETOH.
Identify origin of the complaint, life ▫ Depression, anxiety, PTSD, history of
stressors, events abuse
18Treatment
Acute/Adjustment Insomnia
▫ 1-3 months, often associated with a life event
▫ Discuss the impact of event on sleep
▫ If significant distress, consider short-term sedative
prescription:
▪ Benzodiazepine receptor agonists (BZRAs)
▪ Ramelteon
▪ Anxiolytics (Short-acting benzodiazepines)
▫ Short term f/u in 4 weeks
20Chronic Insomnia: Therapeutic Options
▫ Cognitive Behavioral Therapy for Insomnia (CBT-I): first line
▫ Pharmacotherapy
▪ Not first-line, should not be used a single therapy
▪ Not necessarily indicated for all patients
▪ If indicated, best to be appropriately treated and followed than abusing OTC
medications or ETOH as a hypnotic
▫ Combination of both is more successful▫ (Edinger, Arnedt et al. 2020)
Cognitive Behavioral Therapy for Insomnia (CBT-I)
▫ Large body of evidence showing
meaningful improvement in critical
outcomes with less side effects and more
durable effects.
▫ Individual, group, digital (dCBT-I), video,
etc. Delivered by a trained professional:
psychologists, licensed therapists,
physicians.
▫ Generally 6-9 (1-hour) sessionsMulti-component CBT-I
• Cognitive: restructuring thoughts about sleep
• Prior insomnia experiences leading to worry, unrealistic expectations about sleep, worry
about daytime fatigue
• Behavioral: relaxation, stimulus control, sleep restriction, habits
• Reclaim the bedroom as a place for sleep, going to bed only when tired, consistent wake-up
time, sleep restriction/compression to consolidate sleep time
• Psychoeducational: understanding the connection between
thoughts/feelings/behaviors and sleep
https://www.sleepfoundation.org/insomnia/treatment/cognitive-behavioral-therapy-insomniaPatient’s path to CBT-I ▫ Primary Care -> Behavioral health, Psychology, Psychiatry ▫ Primary Care -> Sleep Physician -> Behavioral health, Psychology, Psychiatry
Brief Behavioral Therapies for Insomnia (BBT-I)
▫ Considering
▪ Barriers to referral to CBT-I, patient’s preference for shorter interventions
▪ 4 weekly sessions
❑ Sleep Restriction
• Reduce time in bed if not for sleep, change the association of bed with
wakefulness
❑ Stimulus Control
• Go to bed only when sleepy, get up if not asleep in 20-30 min, fixed
wake-up timeSleep Hygiene
▫ (Edinger, Arnedt et al. 2020)
▫ Sleep hygiene has not been shown to be an effective treatment for
chronic insomnia
▫ Used as the control group in clinical trialsSleep Hygiene
▫ Basic Practices
1. Maintain regular waking times
2. Limit caffeine consumption after noon (coffee, tea, sodas,
energy drinks)
3. Avoid stimulating activities (especially electronics and
exercise) within 2 hours of bedtime
4. Avoid nicotine and alcohol near to bedtime
5. Avoid excessive time in bed
6. Keep bedroom quiet and cool (65-69F)
28Pharmacological Therapies for Insomnia
Categories
1. Medications with regulatory approval
2. Off-label medications
3. Over-the-counter sleep aids
4. Dietary supplementsPharmacological Therapy for Insomnia – Basic Principles
▫ Associate with cognitive-behavioral interventions for better
treatment success
▫ Always warn patients and caregivers on side effects and the risk of
dependency
▫ CNS depression
▫ Abnormal thinking and behavioral changes
▫ Worsening depression/suicidal ideation
▫ Somnolence
▫ Generally avoiding benzodiazepines as first choiceMedications with regulatory approval
32Ramelteon • Melatonin receptor agonist, sleep-onset insomnia, non-controlled • Highly selective to the receptors M1 and M2, as opposed to exogenous melatonin • Side effects concerns: somnolence, no major CNS side effect concerns or withdrawal issues
Benzodiazepine receptor agonists
(BZRAs)
• Bind the BZ receptor
• Less tolerance, respiratory depression and rebound insomnia as benzodiazepines
• Zolpidem and zaleplon: minimal anxiolytic or muscle relaxing effects
• Eszopiclone: more anxiolytic effectsFDA
Warnings
▫ 2013: Lowered recommended dose for zolpidem, 10mg->5mg
▫ 2013: Patients taking controlled release form of zolpidem
should not drive the next day
▫ 2014: Lowered recommended dose for eszopiclone, 3mg->1mg
35FDA
Warnings
▫ 2019: Boxed warning: serious injuries and death caused
by sleepwalking/driving/other complex behaviors with
(BZRAs)
“ … overdoses, falls, burns, near drowning, exposure to
extreme cold temperatures leading to loss of limb,
carbon monoxide poisoning, drowning, hypothermia,
motor vehicle collisions with the patient driving, and
self-injuries such as gunshot wounds and apparent
suicide attempts. Patients usually did not remember
these events. The underlying mechanisms is unknown”
36Zolpidem
• BZRA, sleep-onset/maintenance, duration 6-8h
• Ideally for short-term use, 4-8 weeks
• Immediate release: 5mg; Extended release: 6.25mg taken immediately before bedtime
• Side effects concerns: complex sleep behaviors, next-day impairment, amnesia, difficult
tapering or discontinuation due to rebound insomnia
37Eszopiclone
• BZRA, onset/maintenance, half-life up to 9h in the elderly
• Ideally for short-term use, 4-8 weeks
• Starting dose: 1 mg immediately before bedtime
• Side effects concerns: avoid in the elderly, CNS depression, complex sleep behaviors, next-day
impairment, amnesiaZaleplon • BZRA, sleep-onset insomnia, very rapid onset of action, half-life ~1 hour • Ideally used for limited period of time • Side effects concerns: complex sleep behaviors, daytime CNS depression
Benzodiazepines • Triazolam: sleep-onset insomnia, short half-life 2-5h • Temazepam: sleep-onset and maintenance, intermediate half-life 8-15h • Short-term with specific plan for weaning and discontinuation • Side effects concerns: caution in the elderly, impaired cognition, delirium, falls
DORAs Dual orexin receptor antagonists
Suvorexant
• Orexin receptor antagonist (wake promoting peptide), half-life ~12 hours (patients need to
allow enough time for sleep, at least 7 hours)
• Schedule IV
• Side effects concerns: daytime sleepiness, abnormal thinking, confusion, complex sleep
behaviors (sleep waking, eating, driving)Lemborexant • Recent FDA approval in 2019 • half-life ~17-19 hours (patients need to allow enough time for sleep, at least 7 hours) • Side effects concerns: Drowsiness, falls, sleep paralysis, sleep-related behaviors
Doxepin
▫ Histamine H1 receptor antagonist, sleep-maintenance insomnia
▫ Long half-life: 15 hours
▫ Side effects concerns: Suicidal thinking/behavior, anticholinergic effects, CNS depression,
QT prolongation , SIADH, sleep-related odd behaviors. Confusion and over sedation in the
elderly.
44Medications commonly prescribed off-label
▫ Trazodone: AASM recommends against, lack of evidence.
Cognitive/motor impairment, suicidal ideation in children and
younger adults, serotonin syndrome, QTc prolongation,
orthostatic hypotension.
▫ Alprazolam, clonazepam, lorazepam: not well studied for
insomnia, multiple safety concerns especially in the elderly
▫ Mirtazapine, amitriptyline: sedation, suicidal thinking/behavior,
anticholinergic effects, QT prolongation
45▫ Regulated by the US FDA
▫ Diphenhydramine, doxylamine
OTC Sleep Aids
▫ Easy access
▫ Side effect concerns: long-term
use, tolerance, potential for
abuse to reach sedating effects.
Anticholinergic effects:
confusion, delirium, dizziness
(especially in the elderly)
46Melatonin • Dietary supplement, not FDA regulated, concentration not assured • Lack of good quality evidence on improvement of sleep parameters • No significant safety concerns. Side effects: vivid dreams, daytime sleepiness, headache. • Important role as a chronobiotic in treatment of circadian rhythm disorders (delayed/advanced sleep phase, jet leg disorder, shift-work disorder)
Melatonin
▫ Canada, 2017
48❑ Combine pharmacotherapy with behavioral
strategies
❑ Discuss shared decision-making
Insomnia Medications
❑ Use the lowest dose possible
Safe Prescribing Checklist
❑ Discuss risks of combination with alcohol, opioids,
other sedatives
❑ Ensure enough time for sleep
❑ Set realistic expectations
❑ Discuss timeline for discontinuation/weaning and
schedule a f/u for this specific purpose
49▫ Elderly: avoid benzodiazepines, caution with any
sedative/hypnotic. CBT and sleep hygiene first.
Ramelteon or extended-release melatonin.
Special
populations
▫ Pregnancy and lactation: multiple factors, recognize
RLS, non-pharmacological strategies are best.
Doxylamine and diphenhydramine may be used. No
others medications proven safe.
▫ Substance abuse history: Ramelteon and low dose
doxepin have the lowest abuse potential.De-prescribing Insomnia Medications • Need to improve awareness about de-prescribing. • Rebound insomnia is common, especially with benzodiazepines and BZRAs • Evidence supports the role of CBT-I to facilitate taper/discontinuation • General guide: decrease by 25% every 2 weeks (consider 12.5% reduction near the end of the taper), with short-term f/u
Sleep Resources De-prescribing Resources
• aasm.org • deprescribingresearch.org
• sleepfoundation.org • deprescribingnetwork.ca
• sleepeducation.org
52“ Thank you
e-mail: alessandra.gearhart@okstate.edu
53You can also read

















































