Submission by the Irish Pharmacy Union on Budget 2019 - August 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Submission by the Irish Pharmacy
Union on Budget 2019
August 2018
Executive Summary
The Irish Pharmacy Union (IPU) is the representative and professional body for community
pharmacists. With over 2,300 members working in 1,761 pharmacies (95% of all community
pharmacies), which employ directly and indirectly 26,000 people, our mission is to promote
the professional and economic interests of our members.
Community pharmacists are highly trained healthcare professionals. Each year there are
nearly 78 million visits to community pharmacy outlets, or 17 visits per annum per man,
woman and child in the State. This provides an unprecedented level of access to the general
public, providing the pharmacy sector with an opportunity to significantly expand our role to
the benefit of both the patient and the State.
Government and HSE cutbacks and ongoing pressure on margins due to reference pricing,
combined with an onerous regulatory regime, increased competition, reduced consumer
spending and rising utility and staff costs, have all conspired to undermine the traditional
business model of pharmacies around the country. Since the introduction of the Financial
Emergency Measures in the Public Interest (FEMPI) Act in 2009, community pharmacy has,
directly and indirectly, contributed over €3.1 billion of savings to the Exchequer from cuts to
pharmacy payments.
Summary of Key Proposals
In summary, the following are the key proposals from the IPU for Budget 2019:
Immediately commence the unwinding of FEMPI measures which were applied to
community pharmacy contractors, with the immediate implementation of the State-
commissioned Dorgan Report;
Enhance primary healthcare services by expanding the role of the pharmacist to include
the introduction of pharmacy-based services available in other jurisdictions, including a
Minor Ailment Scheme, New Medicine Services, Chronic Disease Management,
2
Improved Access to Contraception and an expanded vaccination service, which have
been shown to offer cost-effective access to improved healthcare;
Legislate for the introduction of a comprehensive Biosimilar Medicines Policy, which
independent analysis shows could lead to savings of €370 million over a three-year
period;
Reinstate the 4.25% PRSI rate for lower paid workers from the current 8.5% rate. The
measure should be reintroduced for a further three-year period to assist in sustaining
and increasing employment in the sector;
Bring fees for registering both an individual pharmacist and a pharmacy business in
Ireland into line with those in other European countries especially the UK;
Introduce a properly funded nationwide DUMP (Disposal of Unused Medicines Properly)
Scheme to be operated by the HSE and all local authorities in order to promote safety
by encouraging the public to return their unused medication to pharmacies rather than
hoarding often dangerous medicines;
Commence the phasing out of the Medical Card Prescription Levy; at the very least,
especially vulnerable patients should immediately be exempted from paying it; and
Reinstate tax reliefs on trade union subscriptions to levels that were available in 2011.
These proposals are outlined in further detail below.
3
Introduction
Community pharmacies are largely family-owned businesses (89%) which are part of the
fabric of the local communities they serve, supporting over 26,000 employees in full, part-
time and induced employment, contributing over €2 billion to national GDP both directly
and indirectly.
There are 1.5 million visits to pharmacies every week; half the population lives within 1km
of a pharmacy, with 88% living within 5km. The accessibility of pharmacy in Ireland is among
the highest internationally when compared with other developed countries.
The network of over 1,800 community pharmacies provides an unparalleled opportunity to
meet Ireland’s future healthcare demands within existing healthcare infrastructure.
Community pharmacies are an integral part of the primary healthcare system. Every
pharmacy has a consultation room and most offer late night openings, and access to an
expansive list of services at short notice including at weekends and on public holidays.
Research shows a 96% public satisfaction with pharmacy services.
The Government commitment to reorienting the health service towards primary care has
led to an over-reliance on GP services that GPs say is unsustainable. Population changes in
the coming years will put further demands on an already overstretched health service.
Given the very high level of interaction between the general public and pharmacists every
day in every city, town and village in Ireland, local pharmacists are in a unique position to
expand their role as healthcare providers for the benefit of both patients and the State.
With an ever-increasing demand for healthcare as our growing population continues to age,
and with the ongoing constraints on the resources available to deliver healthcare, we simply
do not have the option of doing nothing. There is an urgent need for a fundamental shift in
health policy and the immediate implementation of change. The time is right to optimise
the delivery of primary care by providing appropriate, convenient, accessible and cost-
effective healthcare through pharmacies in communities throughout the country.
4
However, this cannot be done in isolation. In order to provide these key services, our
community pharmacies need to be adequately resourced to ensure that they can provide
the continuum of care which is urgently required in our communities and which patients are
demanding.
Economic advisors EY-DKM analysed the Irish community pharmacy sector and concluded
that there is an under-provision of certain services in pharmacies in rural and disadvantaged
areas, where demand for these services is higher. This deficit arises because there is less
opportunity in these areas for pharmacies to develop the retail business which is necessary
to subsidise the income from State schemes, upon which rural pharmacies are utterly
reliant. It is clear that the State urgently needs to invest in enhanced pharmacy-based
services which, internationally and domestically, have demonstrated real benefits in terms
of patient outcomes, reduced total care costs and, crucially, the additional capacity which
can be released in more complex healthcare settings such as General Practice and
Emergency Departments. Now is the time to deliver.
5
1. FEMPI – Unwinding
It is now nine years since the Financial Emergency Measures in the Public Interest (FEMPI)
Act was used to cut payment rates to pharmacists. Since then, the State through FEMPI and
other measures has extracted over €3.1 billion from the community pharmacy sector in
reduced medicine reimbursements and cuts to pharmacy fees and margins. The cuts
through FEMPI measures alone come to €1.386 billion. This comprises €527 million in cuts
to dispensing fees and mark-ups (see Table 1) and €859.5 million (Table 2) in cuts to the
wholesale margin/ingredient cost.
Table 1: Reductions in Fees and Mark-ups paid to Pharmacists by the State
Year Pharmacy No. of items Mark-up & Reduction State savings
fees & mark- dispensed fees per item per item
ups under State since 2009
schemes
2017* 76,312,934 €5.29 €0.92 €70,182,372
2016 €397,440,000 75,175,841 €5.29 €0.92 €69,136,626
2015 €389,740,000 73,542,223 €5.30 €0.91 €66,697,624
2014 €381,070,000 72,715,536 €5.24 €0.97 €70,236,816
2013 €393,930,000 74,378,504 €5.30 €0.91 €67,697,977
2012 €403,860,000 75,724,736 €5.33 €0.88 €66,123,326
2011 €386,630,000 72,023,261 €5.37 €0.84 €60,380,232
2010 €372,990,000 69,251,377 €5.39 €0.82 €56,816,616
2009 €420,960,000 67,825,991 €6.21
Total €527,271,589
(*estimate)
Source: PCRS Data and Fitzgerald Power
6
Table 2: Reductions in Medicine Reimbursements paid to Pharmacists by the State
Year PCRS payments No. of items Cost Reduction FEMPI State savings
for medicines dispensed per per item reductions
under State item since 2009
schemes
2017* 75,579,617* €84,500,000*
2016 €945,900,000 74,494,210 €12.70 €6.18 €84,492,157 €460,509,104
2015 €956,750,000 72,911,181 €13.12 €5.76 €85,461,329 €419,772,401
2014 €979,010,000 72,132,792 €13.57 €5.31 €87,449,695 €382,816,851
2013 €1,053,290,000 73,823,818 €14.27 €4.61 €94,084,728 €340,462,478
2012 €1,161,460,000 75,202,381 €15.44 €3.43 €103,746,972 €258,318,978
2011 €1,114,610,000 71,590,122 €15.57 €3.31 €99,562,113 €236,971,544
2010 €1,191,880,000 68,860539 €17.31 €1.57 €106,464,227 €108,168,541
2009 €1,273,770,000 67,468626 €18.88 €113,779,020
Total €859,540,240 €2,207,019,896
(*estimate)
Source: PCRS Data and Fitzgerald Power
By any measure, the cuts in the amounts and rates paid to community pharmacy
contractors under the 2009, 2011 and 2013 regulations have been exceptionally effective in
achieving savings for the State. Pharmacies were hit by statutory reimbursement reductions
in 2009, 2011 and 2013, which along with other measures have culminated in an average
medicine price reduction of 33% per item on State schemes. At the same time, average fees
per item have fallen from €5.97 to €5.03 – a drop of roughly 16% – while the number of
items being dispensed has risen by 11%, increasing the workload on pharmacists. The
average pharmacy relies on State schemes for two-thirds of its revenues, but a decade of
decline has seen the average turnover per pharmacy from State schemes decrease by a
third, with the average annual fees per pharmacy down by 17%.
7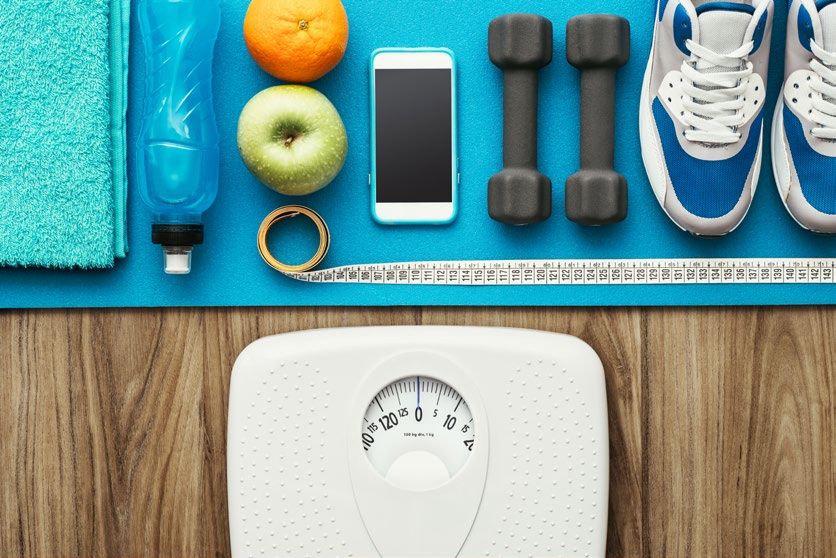
The first estimate of growth in the Irish economy for 2017 from the Central Statistics Office
suggests that there was growth in real terms in the Irish economy of 3.9% last year. In 2017,
Ireland’s debt to GDP ratio declined to 68.5% from 120% in 2013. Consumer spending on
goods and services increased by 1.9%, net Government expenditure expanded by 1.8%, and
net exports expanded by €40.7 billion. Having come through a very difficult period, the
economy is now recovering strongly, which is having a very positive impact on all fiscal
indicators and the international reputation of Ireland.
The economic growth background remains positive. The Department of Finance1 is now
forecasting GDP growth of 5.6% this year followed by an expansion of 4.0% next year, and
also GNP growth of 5.6% in 2018. The medium-term forecasts for the economy are also
projected to be strong. Between 2017 and 2021, real GDP growth is forecast to average
4.7% per annum and real GNP growth is forecast to average 4.3%. Employment is projected
to reach 2.389 million by 2021, and the unemployment rate is projected to average 5.4% in
2021. The General Government Balance (GGB) is forecast to move into modest surplus in
2020, with a surplus equivalent to 0.4% of GDP projected by 2021.
The ‘crisis’ situation that led to the introduction of the FEMPI legislation has passed, and the
future now looks considerably better. There has been a monumental change in the finances
of the State and the health of the economy, the disastrous condition of which were, of
course, the underlying rationale and justification for the cuts in the first instance.
According to analysis by economist Jim Power, FEMPI measures are estimated, in total, to
have resulted in over €2.2 billion in direct reductions in public service remuneration and
pensions. The Public Service Pay and Pensions Act 2017 commits in legislation to the
unwinding of the remaining FEMPI cuts for the public sector and the complete restoration of
their pay.
1
Stability Programme Update, Department of Finance, April 2018.
8
Under the FEMPI Act 2015, the process of reversing the cuts to public sector pay and
pensions has been put in train. The cost of the measures under FEMPI 2015 will be €844
million in the period to September 2018, which is equivalent to 38% of the €2.2 billion
savings made in the public pay bill under FEMPI. The €844 million contained under FEMPI
2015 represents the first phase of pay restoration; eventually most, if not all, of the cuts to
public service pay will be reversed. From 1 January 2018 the Public Service stability
agreement 2013 – 2018 was extended until December 2020, which the Government
estimates will cost €887 million over the three years.
The 2016 FEMPI review, carried out by the Department of Health, concluded with a
recommendation to the Minister that changes to remuneration structures for community
pharmacy contractors must be linked to Government priorities for the health service which,
in the case of community pharmacy, included areas such as probity, piloting of a minor
ailment service, vaccination, expansion of interchangeable medicine use and reference
pricing. The IPU and community pharmacists have delivered on almost all of these, but no
reversal of cuts to pharmacies’ payments has yet been implemented, or even committed to.
The IPU has participated fully and constructively in all statutory consultation processes and
has worked collaboratively with the Department of Health and the HSE in developing
patient services and in improving financial accountability and probity. We have and will
continue to submit constructive proposals for enhancing the role of the community
pharmacist, thus helping the Government keep their commitment to expand the role of the
community pharmacist and improve access to primary care during their term of office.
Pharmacists expect a significant and immediate unwinding of FEMPI. There have been
consistent and repeated statements from various Ministers, including the Minister for
Health, Simon Harris T.D., regarding this. Following the publication of the then Public Service
Pay and Pensions Bill in 2017, Minister Harris, along with the Minister for Public Expenditure
and Reform, made it clear in several statements that they were committed to engaging with
health contractors on the revision of fees, as allowed under the new Act in 2018. Despite
this commitment, there has been no engagement yet with the IPU on behalf of community
9
pharmacy contractors, even though several requests have been made by the IPU seeking
meetings to discuss the issue.
We note that the process has already begun for solicitors, with the recent Financial
Emergency Measures in the Public Interest (Payments to State Solicitors) (Adjustment)
Regulations 2018 bringing about a partial reversal of FEMPI-related cuts to the fees paid to
the solicitors’ profession by the State.
Recommendations
Independent research and analysis has found that the current fee arrangement does not
adequately reimburse pharmacists for their cost of labour, overhead contribution and profit
margin. It is an uneconomic level of fee for the service that is provided by qualified
professionals with regulatory obligations and reporting requirements. Pharmacies have
delivered substantial productivity and efficiency gains, under a growing regulatory and
administrative burden and in the face of increased demand and greatly reduced fees. We
have played our part in the economic recovery of this country.
Implementation of Dorgan Report
It is ten years since the report of the Independent Body on Pharmacy Contract Pricing, which
was established by the then Minister for Health and Children in 2008 and chaired by Sean
Dorgan, to advise the Minister on the appropriate level of dispensing fee to be paid to
community pharmacists for existing services.
The process for the complete unwinding of FEMPI should see the implementation of the
recommendations of the Dorgan Report. Pharmacies have delivered excellent value for
money to the State in the face of massive cuts to fees. The Dorgan Report recommended a
tiered fee of:
€7.00 per item dispensed for the first 20,000 items;
€6.50 for the next 10,000 items; and
€6.00 for each other item dispensed per month.
10Recent independent analysis by EY-DKM Economic Consultants and Smith & Williamson
Accountants indicates that fees at this level, index linked to today and into the future, are
imperative for a sustainable pharmacy sector across the country. We estimate the cost of
implementing the Dorgan Report recommendation at approximately €161 million per
annum.
The Dorgan Report also noted their "strong view that a new contract is required urgently
and that the parties should move to achieve that". Ten years on, it is past time that the
Minister and the HSE engaged with the IPU in such discussions.
Any fee payment model and reversal of FEMPI must be viable and realistic, providing a
sustainable dispensing fee across all schemes, with appropriate professional and
administrative allowances to cover State-imposed costs, and supports for marginal
pharmacies in disadvantaged, rural or isolated communities. Unless dispensing fees are
increased to the levels recommended in the Dorgan Report of 2008 and indexed
accordingly, a significant number of non-urban pharmacies will ultimately close.
2. Expanding the Role of the Pharmacist
Healthcare policy shows a clear commitment to a decisive shift towards primary care, and
pharmacists have a key role to play in this. Sláintecare outlined the severe pressure on the
health service and the need for it to be reoriented towards primary care. Pharmacists are
ideally positioned to expand the services they offer, taking pressure off GPs, and ensuring
the public has access to professional, trustworthy and accessible healthcare in the
community.
There are a lot more services that can be provided in Irish community pharmacies. In
Canada and the UK, for example, pharmacies provide additional services like a pharmacy-
based Minor Ailment Scheme, New Medicine Service, extended vaccination services and
chronic disease management, which are shown to deliver significant benefits to both
patients and the State and to take pressure off other parts of the healthcare system,
11including GPs and hospitals (see Table 3).
Table 3: Examples of Community Pharmacy Services in other countries
Patients have clearly stated that they want more services from their community pharmacy.
Research by Behaviours & Attitudes confirms that 96% of patients want their pharmacists
to prescribe medicines for minor ailments, and 92% are in favour of pharmacists being able
to provide services to improve patient adherence to medicines. Pharmacists want to extend
the care and services they provide to patients and add even more value to the healthcare
system. The future of the healthcare system rests in the advancement of pharmacists’ roles
and the extension of the range of services that are provided.
Over the past number of years, the IPU has made several policy proposals to the
Department of Health, which offered pharmacy-based solutions to primary healthcare
deficits. These include:
2.1 Minor Ailment Scheme
A Minor Ailment Scheme is an internationally recognised extended pharmacy service, which
allows pharmacists to improve public health access, shape future services and broaden
pharmacy roles to deliver quality patient care and improve health outcomes. At present,
private patients who want to access non-prescription medicines for ailments such as hay
fever, migraine or skin conditions, consult with their local pharmacist on the best option for
them, and pay for their over-the-counter medication. Medical card patients with the same
ailments can only access the same medicines if they visit their GP and get a prescription. If a
Minor Ailment Scheme were introduced, public patients would no longer have to make and
wait for GP appointments, saving time for both the GP and patient.
12It has been reported that 18% of a GP’s workload is spent dealing with minor ailments. At a
time when GPs are already overworked and we face a self-reported GP manpower crisis, the
scheme could save nearly 950,000 GP consultations every year, freeing up the equivalent
of an additional 91 full time GPs and, in the process, keeping the focus on primary
healthcare in the community.
The IPU has already collaborated with the Department and the HSE on a pilot scheme, and
the final report was forwarded to the Department in June 2017. Full rollout of a Minor
Ailment Scheme is ready to go from the perspective of community pharmacists, and must
be rolled out to ensure equity and efficiency, and to ease pressure on the health service.
2.2 New Medicine Service
A New Medicine Service can improve adherence to medicines for people who have been
newly prescribed medicines for certain long-term conditions or therapies such as asthma,
COPD, Type 2 diabetes, hypertension, antiplatelet/anticoagulant therapy, statin therapy and
chronic pain. The service would require a structured pharmacist-led intervention, delivered
within the community pharmacy setting, consisting of advice and support for patients
prescribed medicines for a specific chronic disease. The service has the potential to:
Ensure much more effective medicine-taking;
Improve patients’ health outcomes; and
Bring savings in the health budget.
Economic analysis of a similar service which has operated in the UK since 2011, has found
that it offers the NHS increased health gain at reduced overall cost, and provides short-term
savings of £75.4 million and long-term savings of £517.6 million. A successful pilot has been
completed here in Ireland, which identified a positive effect on patient adherence for a total
of 85% of all patients in the pilot; 77% of patients achieved a 9% improvement in adherence
and 8% were referred to their GP. A report has been submitted to the Department of
Health. The service is ready to be rolled-out and should be introduced without delay.
132.3 Chronic Disease Management
In Canada, pharmacists' scope of practice has been extended to include Chronic Disease
Management: monitoring patients with chronic illnesses, ordering lab tests where
appropriate, and renewing and adjusting their prescriptions to ensure tighter control of
their symptoms and delivering better treatment outcomes. The clinical benefits of pharmacy
involvement in chronic disease management are compelling, with a large evidence base
detailing that pharmacists have the most frequent contact with patients with chronic
diseases, due to their accessibility. Research in Canada has found that pharmacist care for
patients with hypertension would save their healthcare system more than CAD$15.7 billion
if the full scope pharmacist care were administered to the full eligible population. Analysis
commissioned by the IPU indicated that, in Ireland, approximately 71,600 cardiovascular
events could be avoided, delivering an estimated saving of €1.36 billion over 30 years.
2.4 Extended Vaccination Service
Making the flu vaccine available in pharmacies has significantly improved access to, and
promoted uptake of, this vital public health intervention. The existing flu vaccination service
has improved accessibility of vaccination for the public and achieved patient satisfaction
rates of 99% in a review carried out on behalf of the Pharmaceutical Society of Ireland (PSI).
Pharmacists currently provide 13% of all flu vaccinations. Since pharmacists first started
vaccinating in 2011, flu vaccine deliveries through the National Immunisation Office (NIO)
have increased overall by 29% and, within that, deliveries to GPs are up 8%, demonstrating
that when pharmacists vaccinate, public awareness increases, and vaccination rates
increase through all channels.
Pharmacists in other countries routinely offer a wider vaccination service. In most states of
the USA, in addition to influenza, pharmacists can offer vaccination of meningococcal
disease, tetanus and hepatitis A and B, as well as travel vaccines. We would like to see our
pharmacy vaccination services extended to include a similarly wide range of vaccines.
142.5 Improving Access to Contraception
Following the announcement in March of this year that the Government would consider
providing free contraception in the event that the Eighth Amendment was removed from
the Constitution, the IPU proposed a scheme to enable women to access contraception
directly from their community pharmacist without prescription and without charge,
regardless of eligibility.
Pharmacists have directly provided emergency contraception without the need for a
prescription since 2011, and most women now obtain emergency contraception from
pharmacies rather than from GPs. This reinforces findings from a 2010 HSE study on
contraception and crisis pregnancy, which found that convenience and accessibility are
important for the supply of contraception. The same study showed that nearly half of the
women surveyed (47%) reported that they would prefer to get their contraception from a
pharmacy. Similar prescription-free services are in place in several other countries
worldwide, including the USA where they have been supported by medical organisations
such as the American Academy of Family Physicians and the American College of
Obstetricians and Gynaecologists.
The IPU proposal would ensure equity and convenience for women seeking to access
contraception and would increase patient safety by ensuring women getting contraception
see a trained medical professional rather than relying on online resources.
An analysis of the costs and benefits of a number of the proposed pharmacy-based
services detailed above are included in a document at the back of this submission
2.6 VAT on Condoms
In line with Government policy to provide better access to contraception and make it more
affordable, we are calling on the Minister for Finance to immediately remove the current
Value Added Tax rate of 13.5% on condoms. This move would encourage more people,
particularly younger people, to protect themselves from sexually transmitted infections and
reduce the risk of unplanned pregnancies by making condoms more affordable.
15Removing the VAT on condoms, as is the case in many other European countries, would
send a clear signal to people that the Government is encouraging them not to have
unprotected sex, which risks sexually transmitted infections or an unplanned pregnancy.
Anything that promotes health and potentially reduces spread of infection is a positive for
society. It makes both economic and medical sense.
2.7 Biosimilars
Following the announcement in February 2017 that a National Biosimilar Medicines Policy
was to be introduced, the IPU commissioned research on the savings opportunity for the
State, which would result from successful adoption of biosimilar medicines. In response to
the Department’s consultation in September 2017, we proposed that a scheme be
introduced whereby community pharmacists would be enabled to supply biosimilars when a
biological reference medicine is first prescribed.
The Health (Pricing and Supply of Medical Goods) Act 2013 lays out the rules and regulations
for generic substitution of medicinal products, identified as interchangeable by the Health
Products Regulatory Authority (HPRA). Pharmacists have demonstrated that they have the
competence and capability to implement this legislation, resulting in a significant increase in
the usage of generic medicines in Ireland, from 11% by volume pre-2013 to 53% by 2016.
An amendment to this primary legislation is required to facilitate substitution by a
pharmacist from a biological reference product to a biosimilar.
Applied Strategic, a UK consultancy firm with expertise in biosimilar markets, conducted an
assessment of the savings opportunity presented by biosimilars in the Irish health system.
Using published PCRS data, they concluded that, in the absence of specific steps being taken
to improve biosimilar uptake, spending on biologics can be expected to reach €900 million
in 2020. Even though biosimilars can provide more cost-effective treatment, thus
broadening patient access to treatment for a given budget, uptake has been historically low
in Ireland, with biosimilars representing less than 10% market share, which is significantly
16lower than the EU average. Applied Strategic’s assessment of the Irish biologics and
biosimilar market identified a potential saving of €370 million over the next three years, and
up to €800 million over five years, with optimum biosimilar entry and penetration. Their
potential savings estimate of €370 million over the next three years is made up of €90
million in year one, €120 million in year two and €160 million in year three.
As the experience of generic substitution since 2013 has demonstrated, allowing community
pharmacists to substitute is the fastest and most effective way to ensure a rapid and
meaningful increase in the usage of biosimilars.
The case for increasing the uptake of biosimilars is quite straightforward. At a time when the
health service is being continuously stretched, it would produce substantial savings for the
State, whilst maintaining similar health outcomes for the patient.
2.8 Reclassification of Medicines
The IPU would like to see a greater role for pharmacists in supporting self care and for an
increase in the number of medicines available without prescription, in line with other
countries such as the UK and New Zealand. This will enable people to access treatments for
minor and self-limiting ailments, allowing GPs to focus on more complicated illnesses.
Pharmacists would utilise their clinical knowledge to help patients choose the appropriate
medication to deal with minor ailments. Medicines that could be reclassified include newer
anti-allergy medicines like fexofenadine and a wider range of analgesics, many of which are
already available without prescription in the UK and elsewhere.
3. Employment Costs
The cost of labour is one of the most significant drivers of business costs, particularly for
retailers. Wages in the Irish retail sector are 46.5% above the European average and
measured by Purchasing Power Parity (PPP), monthly retail wages in Ireland are the fourth
highest in the EU. Ireland’s minimum wage is now 7% higher than in 2015. Growth in
average hourly earnings has increased above the Consumer Price Index (CPI) in each of the
last four years and is now running at close to 3%. In the pharmacy, sector staff costs
17increased by over 4% in the 12-month period between 2016 and 2017. The average
pharmacy spends 20% of turnover on wages and salaries.
The reduction of the 8.5% employers’ PRSI rate to 4.25%, for those earning less than €356
per week, was announced as part of the 2011 jobs initiative and was in place until the end of
2013. This welcome support for job creation and sustainability was not renewed after that
date. Consequently, the ending of this measure had a significant impact on many retail
pharmacies, particularly those employing part-time staff. There is anecdotal evidence of
pharmacies having to reduce staff hours and, in some cases, let staff go, because of the
measure not being extended.
The current level of PRSI/Universal Social Charge on top of existing income tax rates is
rendering prohibitive the costs associated with employing additional staff members and is
also jeopardising the ongoing viability of the employment of existing levels of staff in many
pharmacies. Together with addressing the level of taxes imposed on employees to make
employment more attractive at the margins, it is also essential that employers’ PRSI rates
are addressed to incentivise pharmacy and other retail owners to sustain and increase
employment. A first step would be to reinstate the 4.25% PRSI rate for lower paid workers
from the current 8.5% rate, up to the threshold of €376. The measure should be
reintroduced for a three-year period to assist in sustaining and increasing employment in
the sector.
Employers’ PRSI is a direct tax on labour and should be reduced as a matter of urgency to
offset the substantial labour costs involved in hiring staff. Any possible further increase in
the National Minimum Wage must be offset by cuts to employers’ PRSI for low-income
workers at the very least.
4. Regulatory Costs
The fees charged to pharmacies for registration with the Pharmaceutical Society of Ireland
(PSI) are excessive and are far out of line with international comparisons. The annual
registration fee each pharmacy must pay is €2,135 (€3,325 on first registration). In the UK,
18the equivalent fees are £590 for a pharmacy premises (£831 on first registration), much less
than the cost of registration in Ireland.
The cost of registration with the PSI remains out of line with international comparisons. It is
no longer feasible for Irish pharmacists and pharmacy businesses to pay these fees. It is
unsustainable for one arm of the State, the HSE, to continually drive down unit payments to
the pharmacy profession (as has happened under the FEMPI Act and the Health [Pricing and
Supply of Medical Goods] Act) while, at the same time, another arm of the State, the PSI,
continues to levy the highest pharmacy registration fees in Europe, if not the world. These
costs need to be brought into line with those in other European countries, in particular,
those which apply in the UK.
5. Prescription Levy
The medical card prescription levy, currently €2.00 per item, has increased fourfold since it
was first introduced in June 2010 at €0.50 per item. Many patients, particularly those on
fixed incomes, just cannot afford to pay the levy. Instead, they gamble with their health
every day, either by reducing their medication, or by stopping it entirely. The ultimate
outcome is sicker patients with more complex medical needs needing advanced care in an
already extremely overburdened health system. The imposition of the levy is creating
increased future demand for a health service that is already struggling to cope.
The IPU would like to see a phasing-out of the levy and, at the very least, that it is not
applied to especially vulnerable patients, including those in residential care settings,
homeless patients, patients receiving treatment under the Methadone Treatment Scheme
in respect of other medication that they may require, patients with intellectual disabilities
and palliative care patients.
6. Waste Charges – Nationwide DUMP (Disposal of Unused
Medicines Properly) Scheme
Waste charges are an issue for all small businesses. For pharmacies, the costs are higher
than for other retail-type businesses due to the specialised collection and disposal services
19required for the disposal of medicines. There are significant public safety benefits to
encouraging people to dispose of their unused or out-of-date medicines at their local
pharmacies. However, this must be done without adding significant costs to the pharmacies
receiving the medicines.
The introduction of a nationwide DUMP (Disposal of Unused Medicines Properly) Scheme is
an important measure to prevent the problems associated with holding onto unused or out-
of-date medicines. We are all aware of the effects of uncontrolled disposal of medicines into
the environment and of the potential for accidental poisoning where there are excess
medicines stored in the home. By encouraging patients to return their unused medicines to
their local community pharmacy, thus restricting access to unused medicines, the
introduction of a DUMP Scheme can reduce the risk of suicide, deliberate self-harm and
accidental poisoning in children and help prevent environmental pollution.
Most community pharmacists accept unwanted medicines returned by patients to their
pharmacies and dispose of them at their own expense. However, this is no longer
sustainable as it is becoming an increasingly expensive burden at a time when pharmacies
are under unprecedented economic pressure.
To assist in alleviating these costs, a nationwide DUMP Scheme should be introduced by
the HSE and all local authorities that would encourage the public to return their unused
medicines to pharmacies, which would have significant health and public safety benefits
and, at the same time, alleviate the significant cost for pharmacies providing this service.
7. Tax Relief on Trade Union Subscriptions
Tax relief on trade union subscriptions was first introduced in 2001 by the then Minister for
Finance, Charlie McCreevy, to bring workers’ entitlements into line with people paying fees
to professional bodies who already received tax relief on such fees.
By 2008, the union subscription relief had risen to €350 at the standard rate of tax – the
equivalent of a €70 tax credit for employees with trade union membership.
20In 2011, as the economic crisis deteriorated, the Government of the day initially announced
that they were abolishing tax relief, not just on trade union subscriptions, but on fees to
professional bodies. Thankfully, however, the abolition of tax relief on fees to professional
bodies was not subsequently implemented.
In general, a tax deduction is allowed in relation to expenses incurred wholly, exclusively and
necessarily by an individual in the performance of the duties of his or her employment. The
traditional distinction between the tax treatment of the self-employed in comparison to PAYE
workers was that, for the PAYE worker to benefit for a tax exemption they had to show that
being a member of an organisation was ‘wholly, exclusively and necessarily’ for their
employment. In other words, being a member of that organisation was essentially necessary
for their ongoing employment.
IPU membership clearly passes not only the ‘wholly and exclusively’ tests, but also the
‘necessarily’ test because membership of the IPU provides pharmacists with access to IPU
Academy, an Education facility provided by the IPU, which allows them to do their mandatory
Continuing Professional Development (CPD) which is required for continued registration with
the Pharmaceutical Society of Ireland (PSI), the statutory regulator for pharmacists and
pharmacies. In the case of pharmacists who practise as locums, IPU membership provides
them a listing on the IPU locum panel, which supports them with vetting under the National
Vetting Bureau (Children and Vulnerable Persons) Act 2012, and assists with securing
employment. As a paid-up member of the IPU, employee members receive the British
National Formulary, a professional reference publication that provides essential information
on drug management, and monitoring, dispensing and administering medicines, a key
resource in the application of a pharmacist’s job, which allows them to practise safely.
Members also get access to vital information on pharmacy legislation and standards, essential
to them in carrying out their professional duties correctly and in compliance with regulatory
and legislative requirements. Specific training is provided to ensure that individual
pharmacists attain the necessary standards for them to carry out their day to day functions in
21a safe and compliant manner. In other words, the IPU does a lot more on behalf of our
membership than just representation. Many of these services are specific to the IPU and are
not available from other organisations.
While it is not obligatory for a pharmacist to be a member of the IPU, there is no doubt that
the benefits of membership enhance a pharmacist’s professional qualifications and
experience. It should also be noted that self-employed individuals can claim tax relief against
the subscription to a professional or representative organisation without the requirement of
the membership being mandatory on the individual.
The IPU supports the continuance of tax relief to the self-employed or those in membership of
professional bodies but believes that there is clearly no justification in denying tax relief for
subscriptions paid to our organisation by employee members when the self-employed and
members of some other professional bodies have this facility.
Other countries, including Germany, Belgium, Netherlands, Norway, Australia and Canada,
permit tax relief for trade union subscriptions. For example, in Belgium and Netherlands,
trade union members can get 50% of their union subscriptions back in tax relief.
The IPU is calling for the reintroduction of the tax relief that was available in 2011. What we
are seeking is fair play for employee pharmacists, and that the recognition and application of
reliefs that are available for those who are members of professional bodies and for the self-
employed, be extended to members of organisations like ours who pay their own annual
subscriptions.
Conclusion
It is imperative that the Government reviews and addresses the State-imposed and State-
controlled costs on small businesses, including pharmacies, to maximise sustainable
employment and to ensure the continuing provision of high-quality pharmacy services in local
communities. It is also essential that no further costs are imposed on pharmacies, which could
22have a detrimental impact on the survival of the pharmacy or threaten existing employment
levels.
There must be immediate action to commence the unwinding of FEMPI measures as they
apply to community pharmacy contractors, in recognition of the contribution they have made
to achieving significant savings for the State during the recent financial crisis.
Lastly, the IPU believes that developing the role of the pharmacist will deliver better patient
outcomes, as well as generating efficiencies and savings. The challenge now is to ensure that
community pharmacy is enabled to deliver more into the future, and this requires a new and
more strategic approach to be agreed for the delivery of community-based healthcare in the
context of overall healthcare reform. This year’s Budget can go some way to achieving this.
The IPU is available to discuss this submission in greater detail, if required.
23IRISH PHARMACY UNION Vision for community pharmacy in Ireland
Contents
Introduction 5
Executive Summary 6
1. Ireland’s ageing population and growing chronic disease problem 11
2. Capacity and Constraints in the Irish Health System 15
3. Medicine as the predominant intervention in Ireland 20
4. Pharmacy services as a solution to health sector constraints 21
5. Patient attitudes to new services in Irish pharmacies 22
6. New Pharmacy Services Propositions 28
Case Study 1: Treatment of Minor Ailments 28
Case Study 2: New Medicine Service 29
Case Study 3: Blood Pressure Management 32
Case Study 4: INR Testing 34
Case Study 5: Health Promotion and Smoking Cessation 35
Conclusion 37
Appendix: Case Study Calculations 38
3
Vision for community pharmacy in IrelandFigures
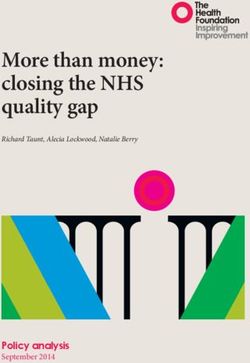
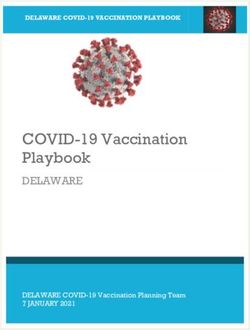
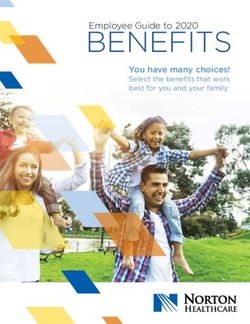
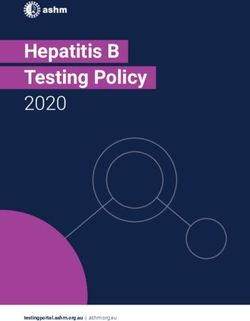
Figure 1: Projected shortfall of GPs in Ireland based on forecast demand and supply 6
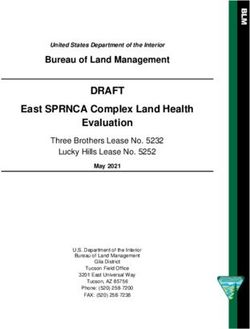
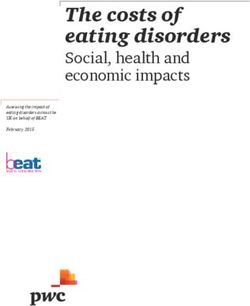
Figure 2: Overview of proposed enhanced pharmacy services 8
Figure 3: Overview of the Vision for Community Pharmacy 10
Figure 4: Medical interactions and the central role of the pharmacist 10
Figure 5: Cumulative growth in population by age category in Ireland 2016 - 2032 11
Figure 6: Relative per capita public health expenditure by age group in Ireland 12
Figure 7: Chronic disease statistics 12
Figure 8: Growing chronic diseases, 12
Figure 9: Ireland’s weight problem 14
Figure 10: Indicative Illustration of complexity of care and its cost 15
Figure 11: In-patient bed days for persons over 65 vs rest of the population 16
Figure 12: Primary Care facts and figures 17
Figure 13: Trends in out of hours payment fees after the introduction of free under six healthcare 17
Figure 14: Development of the age profile of Irish GPs, 1992 - 2015 18
Figure 15: Projected deficit of GP headcount, 2015 - 2025 19
Figure 16: Medication adherence rates for selected illnesses 20
Figure 17: No of GPs and pharmacists in Ireland 21
Figure 18: Growing healthcare demand and the shift to lower complexity settings 22
Figure 19: Making every contact count 22
Figure 20: Frequency of visits to pharmacies and GPs 23
Figure 21: Patient perception of pharmacy 23
Figure 22: Patient views on healthcare professionals 24
Figure 23: Non-dispensing services offered in Irish pharmacies, 2016 25
Figure 24: Irish public attitude to new services in pharmacies vs. global comparison 26
Figure 25: Examples of community pharmacy services in other countries 27
Figure 26: Pharmacy of the Future 30
Figure 27: Prevalence of smoking in Ireland, 2016 31
Figure 28: Minor Ailment Scheme 33
Figure 29: Pharmacist led treatment of Blood Pressure Management 35
Figure 30: Avoided cardiovascular events from pharmacist intervention 36
4
IRISH PHARMACY UNIONIntroduction
This report has been commissioned by the Irish There is a need for change in how community
Pharmacy Union (IPU) to emphasise the benefit pharmacists are utilised, which is determined by:
community pharmacy can deliver to the patient • The changing patient and population needs
and to the wider health system in Ireland. It builds for healthcare, in particular the demands of
upon recent reports in relation to the pharmacy an ageing population with multiple long term
profession and Irish health policy: conditions;
• In June 2016, the Dáil established the • Emerging models of pharmaceutical care
‘Committee on the Future of Healthcare’ with provision from the UK and further afield1;
the goal of achieving cross-party, political
• The need to improve value through integration
agreement on the future direction of the health
of pharmacy and clinical pharmaceutical skills
service, and devising a ten-year plan for
into primary healthcare;
reform. In May 2017, the committee published
its report, Sláintecare. The report outlined the • The need for service redesign in all aspects
severe pressures on the Irish health service of care for a financially sustainable health
and the requirement for health services to be service.
reoriented towards primary care.
In September 2017, the Department of Health
• In November 2016, the Pharmaceutical undertook a public consultation as part of a
Society of Ireland published a report; ‘Future review of health service capacity to the year
Pharmacy Practice in Ireland Meeting 2030, which took into account factors such as
Patients’ Needs’, which outlined the future current utilisation, unmet demand, demographic
role pharmacists could play as part of an and non-demographic factors and future policy.
integrated health system. The review will attempt to quantify the scale of
the shortfall of healthcare professionals given the
This report will outline the rationale for the funding
projected requirement2. There is great untapped
of enhanced pharmacy-based services. It is
potential to bridge this gap in capacity and to
based on successful international and domestic
improve care through the better use of the skills of
implementation of these services, demonstrating
the community pharmacy team.
the benefits in terms of patient outcomes, reduced
total care costs and, crucially, the additional
capacity which can be released in more complex
healthcare settings such as General Practice and
Emergency Departments.
1N
HS, Community Pharmacy Contractual Framework,
Advanced and Locally Commissioned Services
2E
SRI: Projections of demand for healthcare in Ireland,
2015-2030: First report from the Hippocrates
Model
5
Vision for community pharmacy in IrelandExecutive Summary
Irish people, as with populations in most developed Department of Health and Government policy
countries, are living longer, with an average approaches to tackling the rising demand for
lifespan of 81.4 years.3 This phenomenon radically healthcare have determined that Ireland’s current
affects the demographic profile of the population reliance on acute hospital services to treat such
with 88% growth in the 80+ years age category conditions is neither in patients’ best interests nor
forecast over the next 15 years. This will have a financially sustainable in the medium term.4 In
profound impact on the demand for healthcare response to this, successive government policies
services, with the average cost of care for older have indicated that a radical change is needed
persons being two to three times that of the in our approach to healthcare, with greater
average Irish person. collaboration amongst a multi-disciplinary team
of healthcare professionals practising to the top
These growing health needs will be exacerbated of their licence,5 and with the vast majority of
by the high and growing prevalence of chronic this care delivered in the community. If these
diseases such as Cardiovascular Disease, policies are to be implemented, primary care
Hypertension and Diabetes. By 2020, it is will require significant expansion in the coming
expected that 40% of the entire population will years. Currently, GP services are undergoing
be diagnosed with one or more chronic diseases. significant strain largely caused by two key factors:
Currently, management of chronic diseases 1) demand increases following the expansion of
accounts for 80% of all GP consultations and 75% access to free GP care and 2) capacity constraints
of hospital bed days. This continued growth in their within the profession, caused by an ageing
prevalence has ultimately resulted in a number of workforce profile.
high profile crises in the public health service, and
comes at a time when pressured public finances
cannot sustain indefinite capacity increases.
Figure 1: Projected shortfall of GPs in Ireland based on forecast demand and supply
3,000
and
Dem
Increase in GP headcount
2,500
2,000 Deficit of 1,121 GPs
ly
Supp
1,500
1,000
500
0
2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Note: the figure aboveshows the shortage that is expected if the expansion of free GP care is extended to the under
6’s and over 70’s by 2025, with no emigration of staff
Source: HSE, Medical Workforce Planning, Future Demand for Medical Practitioners, 2015 – 2025, PwC Analysis
4 HSE, Planning for Health, 2017
5 Houses of the Oireachtas, Committee on the Future of
3 OECD Life Expectancy, 2015 Healthcare, Sláintecare Report, May 2017
6
IRISH PHARMACY UNIONA solution to this system-wide demand growth and Such potential enhancements of the pharmacy
constrained supply lies in the under-utilised network service would include:
of Irish community pharmacies. The network of
over 1,900 (PSI Annual Report 2016) community 1. Improving equality of access to care;
pharmacies provides an unparalleled opportunity 2. Treating GMS patients for common ailments with
to meet Ireland’s future healthcare demands within non-prescription medication;
existing healthcare capacity and infrastructure.
Pharmacists are highly trained, strictly regulated 3. Supporting better use of medicines for those
healthcare professionals who are trusted by the Irish newly starting a medicine for a long-term
public and have demonstrated success in providing condition;
new services such as the flu vaccination among 4. Supporting people with long-term conditions,
other initiatives.6 They are experts in medicines, the such as cardiovascular disease or asthma;
most common healthcare intervention throughout
the health system. 5. Improving the public’s health through helping
to deliver screening programmes as part of a
Modest investment in pharmacy-based services national health promotion strategy;
carried out in collaboration with GPs and within the
6. Provision of ‘stop smoking’ services.
professional scope of the pharmacist would free up
crucial capacity in GP surgeries and achieve cost- Outlined below are five summaries of proposed
efficient treatment across the continuum of care. services which could be implemented in Irish
pharmacies. Evidence from domestic pilot
projects and international case studies has been
used to indicate the estimated cost of national
implementation, outline the patient benefits and
6 Behaviours and Attitudes Survey, Irish Pharmacy Union,
demonstrate the cost savings across the health
2017 system.
7
Vision for community pharmacy in IrelandFigure 2: Overview of proposed enhanced pharmacy services
Summary of proposed service Patient benefits of service Health system benefits
This service would allow identical • Equitable access to An estimated
1.Treatment of Minor Ailments
access to medication for minor healthcare for both public total of 947,806
ailments as is currently enjoyed by and privately funded GP consultations
private patients for forty different patients; (approximately 91
conditions such as headache, • Saves patients’ time GP WTE) are saved
indigestion, constipation, because they do not have throughout the health
diarrhoea and hayfever. to attend surgeries which system as well as
take them more time (e.g. significant unnecessary
Patients would pay the standard ED attendances.
GPs, GP out of hours
existing €2.00 levy, without the
(OOHs), walk-in-centres or
need for a GP consultation.
A&E departments);
• Leads to a faster recovery
and improved quality
of life if they avoid
having to wait for a GP
appointment.
A new medicine service is • Significant increase in the Net saving of over
2. New Medicine Service
a structured pharmacist-led probability of adherence to €500,000 per year.
intervention, delivered within the the medication regime and
community pharmacy setting, thus better disease control Estimated savings over a
consisting of advice and support throughout the population. five year period amount
on medicine taking for a newly to €2.5m.
• Improved quality of life,
prescribed medicine for a specific and longer life expectancy. Further HSE cost
chjronic disease state, delivered
• Decreased adverse events savings could be
within two weeks of commencing
and hospitalisations. achieved as a result of
the medicine. Patients would be
• Reduction of medicines the service identifying
referred to the service by a GP or
wastage. ineffective prescribed
Pharmacist.
medicines, decreased
• Improvement in quality of
There is an initial consultation and hospitalisations due
life.
follow up 7-14 days after where to adverse events and
the patient can discuss medicine reducing medicine
related issues, side effects and wastage.
other queries. Patients are referred
back to the prescribing GP where
issues are observed.
This service is initially for
conditions with a high rate of
avoidable hospitalisation, such as
asthma, COPD, Type 2 diabetes,
hypertension, antiplatelet/
anticoagulant therapy and statin
therapy. The service can be further
expanded to other conditions
where non-adherence is an issue.
8
IRISH PHARMACY UNIONSummary of proposed service Patient benefits of service Health system benefits
3. Blood Pressure Management A pharmacist led blood pressure • Reduction of systolic blood An estimated 71,600
(BP) monitoring service is initiated pressure by up to 18.3 cardiovascular events
by a GP and involves the mmHg. avoided in Irish
pharmacists monitoring the patient • Lower systolic blood population and an
up to six times a year over a 12 pressure ensuring lower risk estimated saving of
month period. of cardiovascular event. €1.36 billion over a 30
year period.
The pharmacist assesses the • Reduction in admissions
patient; counsels on CV risk; to hospital for a variety
monitors BP; reviews medication of issues arising from
and adjusts dosage where hypertension.
necessary. • More frequent contact with
a healthcare professional
to monitor wider health
issues.
System-wide drug cost reduction • Large, immediate cost Saving to health system
4. INR Testing
is achieved by supporting and reduction due to patients by switching all patients
managing new patients using currently being on warfarin to Warfarin from
warfarin, rather than a reliance on compared to DOACs. DOAC is €23.1m per
high cost DOACs. • Less invasive than venous year including costs of
blood test. providing service.
New and existing patients
prescribed warfarin would attend • Limits any increased
a clinic in their local pharmacy for burden on already
testing and monitoring rather than overcrowded hospitals.
in a hospital outpatient setting. • Convenient and flexible
access to testing in
pharmacy.
Pharmacists would provide • Equitable access to Over 35,780 GP hours
5. Health Promotion and
Smoking Cessation
structured national health healthcare for both public saved per year. Which
monitoring and awareness and privately funded represents 17 GP WTEs.
campaigns. A specific patients
implementation case is that Significant long term
• Ensures greater capacity
of smoking cessation services savings due to the
utilisation of GP time
available for both private and elimination of smoking
• NRT with structured related illness.
public patients.
behavioural support is
10-25% more likely to
increase the chance of
success.
9
Vision for community pharmacy in IrelandYou can also read