Symptom Magnification and Malingering in Occupational Health and Workers' Compensation - Matthew Barber, M.D.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Symptom Magnification and
Malingering in Occupational Health
and Workers’ Compensation
Matthew Barber, M.D.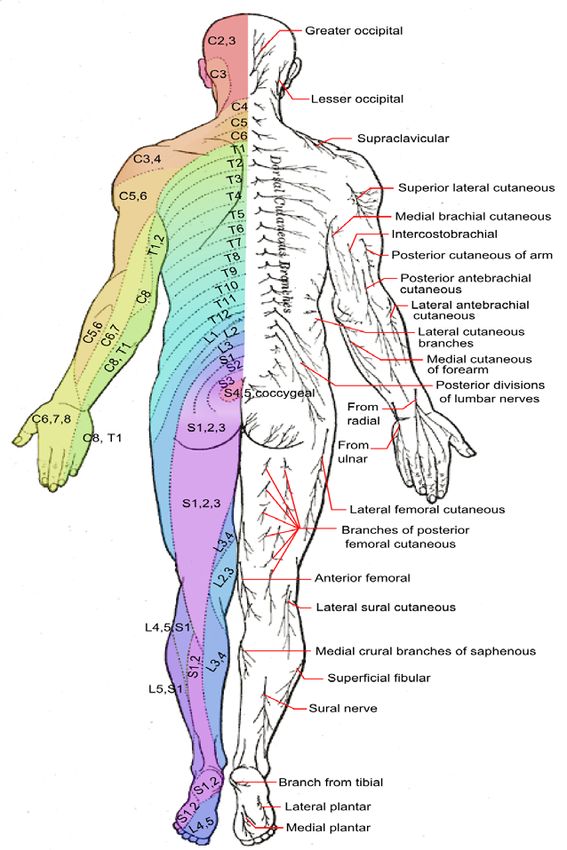
Symptom Magnification and Malingering
• Difficulties of the subject
• Definitions
• Possible ways to detect (exam,etc.)
• Testing (in a specialty setting)
• Improving Recovery Time and Return To Work
• Q&A
* Perspective of orthopaedic surgeon
Training “Treating health providers often do not consider malingering, even in cases of delayed recovery involving work injuries or other personal injuries, where there may be a significant incentive to feign or embellish symptoms or delay recovery” (Aronoff et al, 2007). “The term malingering, as a description of behavior or as a diagnosis, usually is considered highly pejorative and controversial. Clinicians may be reluctant to address this behavior directly, even if there is strong evidence, because they are afraid of the consequences (e.g., mislabeling someone, being threatened, or being sued) [Binder & Iverson, 2000].

Symptom Magnification • Symptom Magnification refers to the conscious or sub-conscious tendency of an individual to under-rate his or her abilities and/or over-state his or her limitations. Symptom magnification is measured through assessment of observed functional performance, as compared to a subjective reports of the limitations caused by his or her symptoms. It does not imply intent.
Malingering • Malingering is a medical term that refers to fabricating or exaggerating the symptoms of mental or physical disorders for a variety of "secondary gain" motives, which may include financial compensation (often tied to fraud); avoiding school, work or military service; obtaining drugs; getting lighter criminal sentences; or simply to attract attention or sympathy.
Detection of Malingering • Complaints grossly in excess of clinical findings • Bizarre, absurd, inconsistent symptoms • Atypical fluctuation in symptoms in response to external incentives • Unusual response to treatment that cannot be otherwise explained (e.g., paradoxical response to medication) • Markedly discrepant capacity for work vs. recreation • Substantial noncompliance with evaluation or treatment • Compliance only with passive versus active treatment • Refusal to undergo invasive testing or treatment, regardless of potential benefit • Special Signs/Tests

Non-organic Physical Signs
(“Waddell’s signs”)
• Non-anatomic weakness or sensory loss
• Non-anatomic superficial tenderness
• Simulation tests with axial loading and en
bloc rotation producing pain
• Distraction test or flip test in which pt has no
pain with full extension of knee while seated,
but the supine SLR is markedly positive
• Over-reaction verbally or exaggerated body
language
Waddell, et al. Spine 5(2):117-
125, 1980.
Tests / Waddell’s Signs
• Waddell’s Light Pinch
– Non-anatomical tenderness to light pinch.
• Waddell’s Axial Vertical Loading
– Vertical loading on a standing patients skull produces
low back pain.
• Waddell’s Simulated Rotation
– Passive rotation of shoulders and pelvis in the same
plane causes low back pain.
• Distraction
– Discrepancy between findings on sitting and supine
straight leg raising tests.
• Overreaction
– Disproportionate facial expression, verbalization or
tremor during examination.
Waddell’s Light Pinch
Detection • Non-anatomic weakness or sensory loss
Bowlus and Currier Test
Waddell’s Axial Vertical Loading
Waddell’s Simulated Rotation
Distraction
Overreaction
Hoover Test • Helps to determine whether pt is malingering • Should be performed in conjunction with SLR • When pt is genuinely attempting to raise leg, he exerts pressure on opposite heel to gain leverage
Hip Adductor Test
Observation • Gait • Movements • Particularly when not being “examined”
Window Test
Surveillance
• Resource-intensive
• Not practical in every
caseFCE • Inconsistencies • Excess of “self-limiting” behaviors
Index of Suspicion • Must be on the lookout • Variation from clinical experience • Other information sources
Diagnostic Testing • Sometimes early • Sometimes late • Careful interpretation
Improving Recovery Time and
Return To Work
• Acknowledge that this can be an issue (M.D.)
• Be alert to signs
• Set expectations with the patient
– Active participant
– You WILL get well
• Use exam and diagnostic tests
• Confirm ( FCE ?, Second Opinion ?)Thank You
Waddell’s Inappropriate
Symptoms Questionnaire
• In 1980 Dr. Waddell and his colleagues wanted
to distinguish and standardize "non-organic"
physical signs that sometimes accompany low
back pain.
• Pain descriptions usually approximate
anatomical and pathological patterns of disease,
however, sometimes these descriptions do not
follow general clinical experience.
• Inappropriate symptoms are usually attributed to
psychological features and are vague, not well
localized and lack the normal relationships to
time, activity and anatomy.Purpose • This is a test to determine whether the clients symptoms are appropriate or inappropriate with respect to low back pain. • Should be noted that these symptoms may in fact occur in other pathologies such as hip pathology and therefore, the pathology should be confirmed as emanating from the low back before utilizing the test.
Administration • Provide the client with the questionnaire asking 5 simple questions requiring either a “yes” or a “no” answer. • There are two additional questions which may be utilized, they are gathered in the routine history which doesn’t appear on the patients questionnaire. • A “yes” answer to either of these additional questions constitutes an inappropriate response.
Instructions
• Answer the 5 questions by circling either
“Yes” or “No” to each question.
– 1. Do you get pain at the tip of your tail bone?
– 2. Does your whole leg ever become painful?
– 3. Does your whole leg ever go numb?
– 4. Does your whole leg ever give way?
– 5. In the past year, have you had any spells
with very little pain?Instructions Con’t
• Additional questions:
– 6. Do you have an intolerance of or reactions
to treatment?
– 7. Have you ever had emergency admission
to hospital with low back pain?
– These are the added questions that can be
utilized in the routine history and they do not
appear on the clients questionnaire.Scoring • A “yes” answer to questions 1 to 4 are inappropriate. • A “no” answer to question 5 is inappropriate. • A total of 2 or more inappropriate scores is indicative of inappropriate illness behavior. • Most symptom magnifiers usually score more than 2 inappropriate answers in the first 5 questions and it is therefore unnecessary to score questions 6 and 7.
Non-organic Physical Signs
(“Waddell’s signs”)
• Non-anatomic weakness or sensory loss
• Non-anatomic superficial tenderness
• Simulation tests with axial loading and en
bloc rotation producing pain
• Distraction test or flip test in which pt has no
pain with full extension of knee while seated,
but the supine SLR is markedly positive
• Over-reaction verbally or exaggerated body
language
Waddell, et al. Spine 5(2):117-
125, 1980.You can also read