"The Commissioning Landscape" Peter Kay, National Clinical Director for MSK
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
1
“The Commissioning Landscape”
Peter Kay, National Clinical Director
for MSK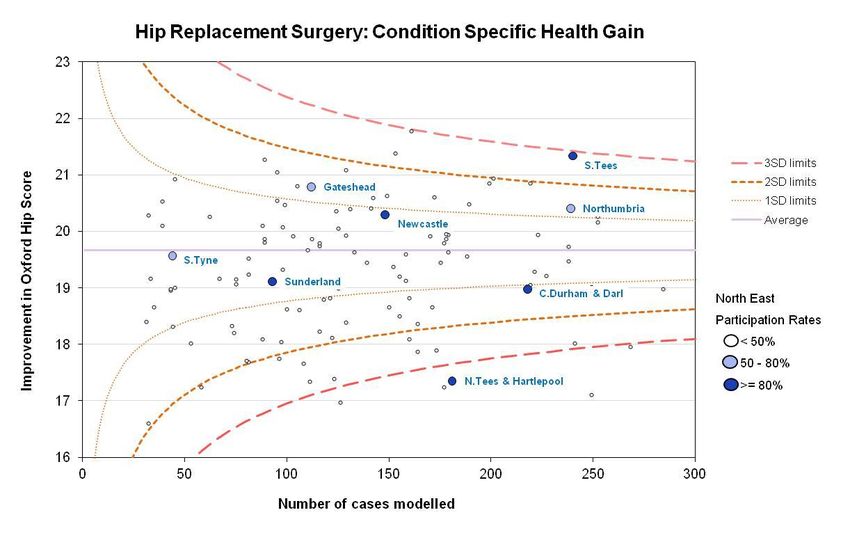
2
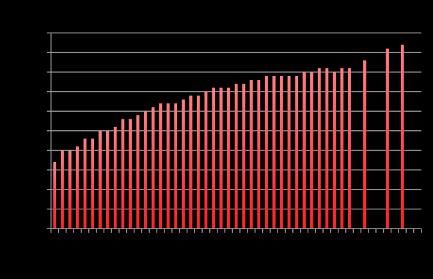
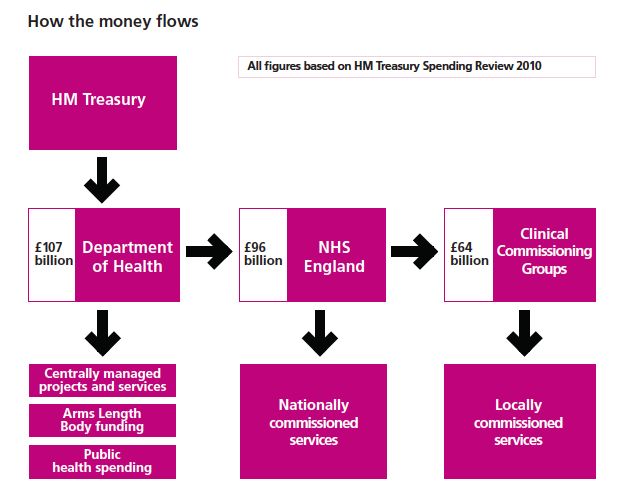
Money and Healthcare
• Commissioning History England
– 1948-91 unitary system all funded through AHA
– 1991 The split commissioners/providers
– 1991-94 GP fund holding / DHAs (192)
– 1997 Primary Care Groups 481
– 2002 Primary Care Trusts 303-152
– 2010 Clinical Commissioning Groups 211
Directly commissioned Services (Not via CCG) Orthopaedic CRG All Specialist services under review
MSK CRG issues
• Need to see specialist commissioning in the context of
pathways of care
• Drivers to get the right patient in the right place
– Facilitate Networks
– Integration not fragmentation
• The right amount of specialised commissioning
• 75+ CRGs realistically we reduce the number
• Excellent CRGs, Rheumatology, Orthopaedics
• Aspiration and work of the CRGs
• The wider strategy of NHS England
• Specialist Commissioning will become better supported
both clinically and financially with better outcomes
The Clinical Commissioning Group The Bolt on the Landscape? or the solution?
MSK in the NHS England (£7 -10bn)
4th largest area of spend
• More years lived with MSK disability than any other disease
• 2nd cause of disability
• More time off work
• 25% of all GP slots
• etc etc
• Not Kids, Cancer, Cardiac
• Is it a priority for payers?
• Under the Spot light
– Economy
• Expensive
– General Election
• Waiting times
– Work
• BenefitsOrthopaedics is part of MSK &
MSK is part of a wider NHS
We need to continually make the case
Advantage Effective interventions
Patient focused but population basedwww.england.nhs.uk/house-of-care
Organisational and Clinical Processes
• Guidelines, evidence and
• Information and technology
national audits
• Care Planning
• Care Delivery
• Safety and Experience
Informed and Health and Care
engaged patients Professionals
and carers committed to
partnership
Person centred- working
• Self management
• Information and coordinated care • Integration
Technology • Culture
• Group and peer • Workforce
support • Technology
• Care Planning • Care Co-ordination
• Carers • Care Planning
Commissioning
• Needs Assessment and Planning • Service User and Public Involvement • Care Planning
• Joint commissioning of services • Contracting and procurement • Tools and levers
• Metrics and EvaluationModels of Good Care Good care: • Transcends contractual arrangements that underpin it • Is not the preserve of primary or secondary care • Needs to be delivered by a wider team • Needs to be integrated – across providers, carers, local authorities and employers • Needs to be seamless in its delivery, user understanding it • Needs to be delivered in appropriate settings – Near home / specialist centre • Health Care Workers competent in delivering MSK care – Developing the MSK workforce • user-driven; by needs, preferences and outcomes • Prevention, public health, employment, social care.
Commisioning • Quote of 6 % of independently provided services • Disproportionate for MSK • Bedford, Sussex, Oldham • Big support for commissioning no support for tendering • AQP issues cherry picking, co-dependency of T&O • 5 to 6 year contracts • Nothing left
Prime vendor model • Holding the whole budget for MSK (usually not trauma) • Where this has worked it has ben an evolution • As service has developed more of the budget devolved • Integrated over time • The program budget does not define success • Giving the money over and expecting it to work • Cop out for some CCGs • Big conflicts of Interest
The ARMA Project:
Key findings so far (1)
• Why it’s important
• Key issues for MSK services:
– Inadequate understanding
– Under-referral for rheumatology, over and under referral
for orthopaedics?
– Right care, right place, right time. Effective triage
– Role of AHPs and nurses
• Good MSK services:
– Address urgent need
– Tailored to personal needs and wishes
– Improve quality of life
– Support people to remain active (eg in work) and
independentThe ARMA Project:
Key findings so far (2)
• Successful implementation of innovative MSK
services involved:
– links with CCG/ secondary care specialists
– pioneering and innovative clinician/ AHP; a
“champion”
– knowledge of change management
– prior specialist training in MSK
– persistence(!)A shared vision for
excellent MSK services
• Holistic patient-centred care
• Early intervention
• Improved clinical and personal outcomes
• Multidisciplinary with shared decision-making
• Co-ordinated care, empowering informed
patients
• Maximises community-based care closer to home
• Excellent communication channels
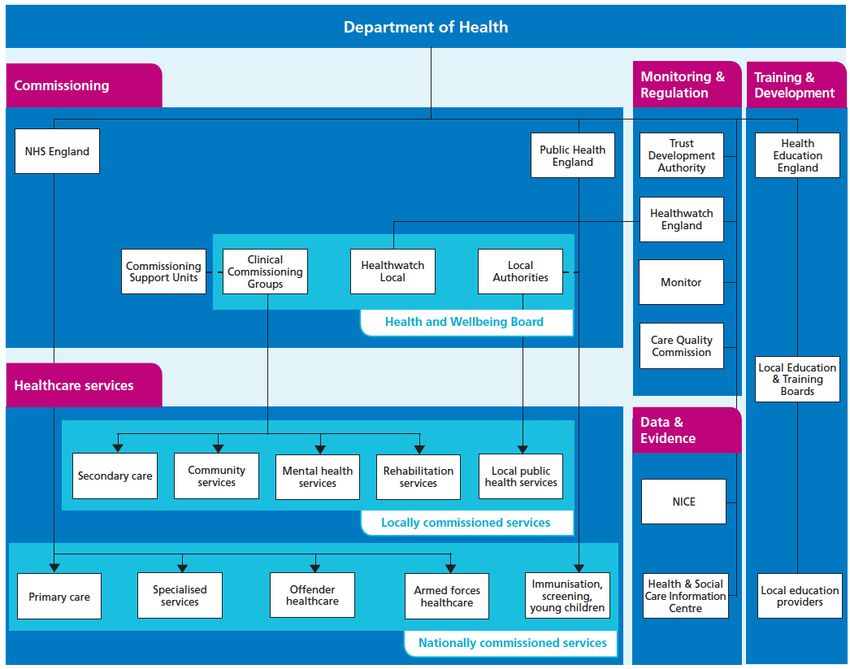
• Effective and accurate monitoring systemsThe “architecture” of
MSK clinical networks
Workforce: education Integrated, community- FLS (specific projects)
and training based care
Metrics / outcome measures
Patient involvement
Regional (SCN) level
Local (CCG) levelWorkforce: education and training
• Direct Assess to Physiotherapy (Scotland)
• Community Pharmacy
• The musculoskeletal Practitioner
• BSR, BOA, CSP, RCN, Keele University etc
• Physio, Nurse, OT, Radiographer
• Rheumatology nurse practitioner,
• Trauma co-ordinator
• Fragility Fracture Co-ordinator
• National Transferable rolesMetrics / outcome measures
• Making metrics part of the day job (ARUK)
• Should the NHS buy anything it does not measure
– Provide an estimate of disease burden
– Musculoskeletal Calculator
– Effectiveness of processes
• (Best practice tariff NOF)
• (Best practice tariff early rheumatoid)
– Pre treatment level of severity
– Outcomes after treatment
– Experience
• Finance
• Variation
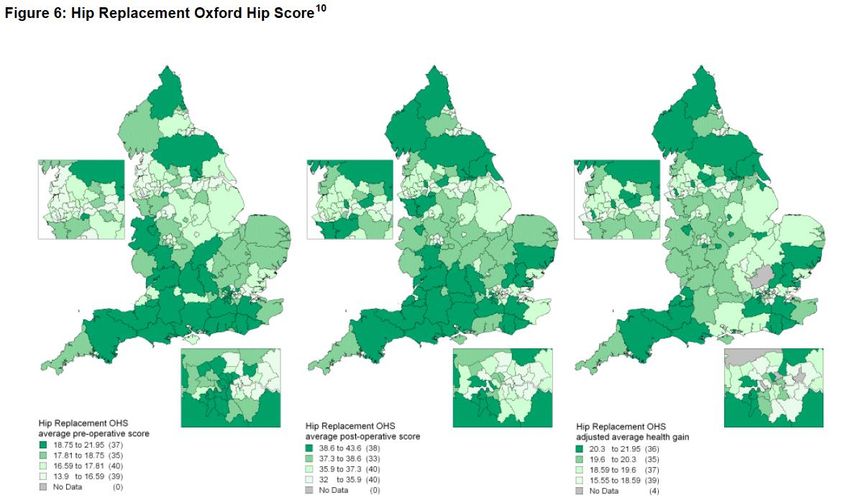
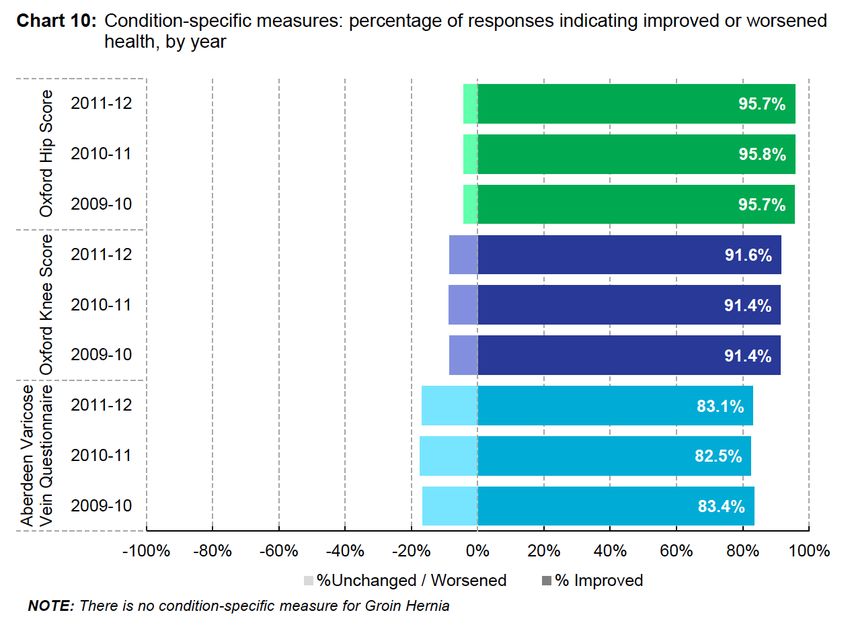
• CompetencePROMs – Hip Replacement Improvement in Oxford Hip Score
Outcome Relates to Pre-op Function*
Hip Replacement Knee Replacement
Pre Op Score Pre Op Score
Worse Better Worse Better
*from PROMs Data April 2010Commissioning • The Orthopaedic Profession needs to engage more with commissioners locally not just DH • The role for regional advisors BOA-RCS • Downward pressure on AQP private providers – Circle, Big Politics, CCG worries • Need to be proactive not just reactive • The election may be significant but…… • We still need to be working to define and design services not just do surgery
“When you are done changing, you're done.” Benjamin Franklin
We are not done MSK is a priority – The writing is on the wall Networks are the future in commissioning
You can also read

















































