The effect of Worklessness on Health and Wellbeing Professor Ewan B Macdonald OBE - Healthy Working Lives Group University of Glasgow - wwdpi
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The effect of Worklessness on
Health and Wellbeing
Professor Ewan B Macdonald OBE
Healthy Working Lives Group
University of Glasgow
What is Work? Oxford English dictionary – “Purposeful Activity” • Paid employment • Self Employment • Voluntary work • Carer • Homemaker • Child rearing • Full time/ part-time • Community activities, clubs, church • Etc ALL OF THESE ARE BENEFICIAL TO SOCIETY AND THE INDIVIDUAL PROVIDED THEY HAVE ENOUGH MONEY

Definition of
“Worklessness”
‘Worklessness’ is a fairly new term.
Is it just a different word for unemployment?
…….worklessness is not the same as unemployment
-several different definitions.
“Worklessness” includes people who are
unemployed and people who are economically inactive:
people who are sick or disabled, students, people looking
after the family and home, and retired people…...
Worklessness: not engaged in any form of work, which includes
but is broader than economic inactivity and unemployment.
What is Health? • WHO Definition – “a complete state of physical, mental and social wellbeing and not merely the absence of disease and infirmity” • Newer definitions - Healthy Working Lives - “being able to do as much as possible for as long as possible in your working and non working lives” (HWL, Macdonald 2004) • Health is about level of functioning, functional capacity or capability
Long Term Health
conditions
Examples of long term health conditions
• Congenital
• Chronic inflammatory joint disease e.g. Rheumatoid arthritis
• Other musculoskeletal conditions e.g. back pain
• Respiratory problems e.g. COPD
• Cardiac disease
• Hypertension
• Stroke
• Cancer
• Diabetes
• Obesity
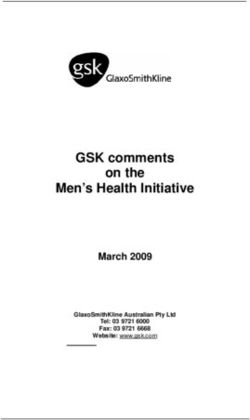
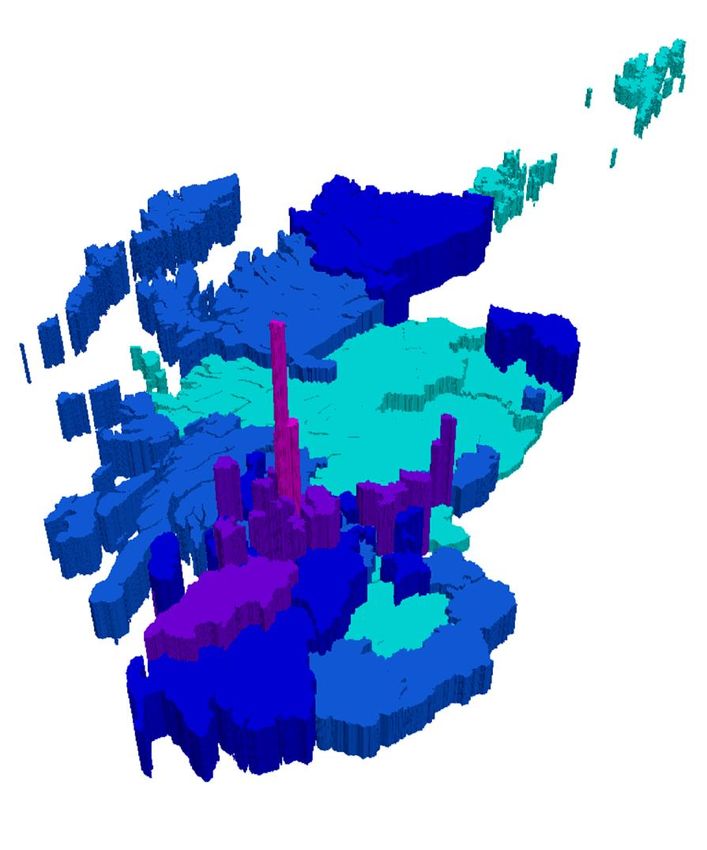
Rate of IB receipt by
MSP constituency 2008
Rate of IB receipt 2008
3.5% - 6.7%
6.8% - 8.6%
8.7% - 9.9%
10% - 14.7%
14.8% - 20.0%
.
Scottish Observatory for Work and Health, University of Glasgow (Data source: DWP)
ESA and Incapacity Benefit

What do we know about
being out of work?
Unemployment is bad for you:
• Loss of Income¹
• Destructive on self-respect¹
• Risks of ill-health²
• The “psychosocial scar” persists³
• Trans-generational effects
1. Winkelmann and Winkelmann 1996; 2. Clark, Georgellis, Samfey 2001;
3. Clark and Oswald 1996; 4. Aylward 2006
The new Paradigm
Work is good for you
“Overall the beneficial effects of work outweigh the risks
of work, and are greater than the harmful effects of long-
term unemployment or prolonged sickness absence. Work
is generally good for health and well-being”
Waddell and Burton 2006
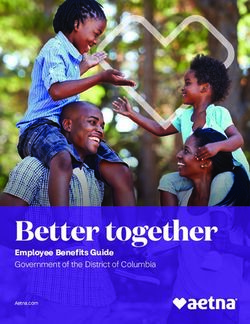
Self-Reported health from
the British Household Panel
Survey
Self-Reported Health by Economic Group in Scotland
.8
.6
.4
.2
0
Employed Workless Incapacity Benefit
Excellent/Good Less than Good
Scottish Observatory for Work and Health, University of Glasgow
(Data Source: BHPS)Proportion of deviation from perfect health by social class
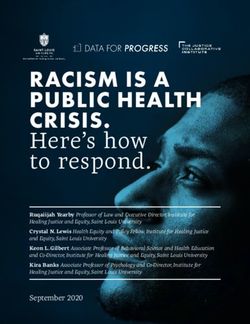
Changing Scotland: Estimated & Projected Age Structure
1901 – 2031 (GROS)
Scotland 1911 Scotland 1951
80 - 84 80 - 84
MALES FEMALES MALES FEMALES
70 - 74 70 - 74
60 - 64 60 - 64
50 - 54 50 - 54
Age
Age
40 - 44 40 - 44
30 - 34 30 - 34
20 - 24 20 - 24
10 - 14 10 - 14
0-4 0-4
-300,000 -200,000 -100,000 0 100,000 200,000 300,000 -300,000 -200,000 -100,000 0 100,000 200,000 300,000
Population Population
Scotland 2001 Scotland 2031
80 - 84 MALES FEMALES 80 - 84 FEMALES
MALES
70 - 74 70 - 74
60 - 64 60 - 64
50 - 54 50 - 54
Age
Age
40 - 44 40 - 44
30 - 34 30 - 34
20 - 24 20 - 24
10 - 14 10 - 14
0-4 0-4
-300,000 -200,000 -100,000 0 100,000 200,000 300,000 -300,000 -200,000 -100,000 0 100,000 200,000 300,000
Population PopulationPrevalence of chronic disease
ILO Projection for Workers Over 55
Europe 32
North America 30
%
Asia 21
Latin America 7
0 10 20 30 40Source: United Nations, Department of Economic and Social Affairs, Population Division
Over 60’s
• In 1999, 593 million persons were aged 60 or over
• In 2009, 737 million persons
• The UN Population Division - 2 billion in 2050
• Today - 1 :9 is 60 or over.
• 2050 - 1:5
Source: United Nations, Department of Economic and Social Affairs, Population DivisionOver 50’s • In the UK by 2020 – 47% of the population will be over 50 years of age. • They will 32% of the available workforce
Work, Health & Society
Society needs the maximum number of
productive years from as many people as
possible.
Childhood Working life Retirement
The future population will be composed of longer
survivors, many with several long-term health
conditions.Labour force participation
Is work good for
your health & well-being?
• Work meets important psychosocial needs in societies
where employment is the norm;
• Work is central to individual identity, social roles and
social status;
• Employment and socio-economic status are the main
drivers of social gradients in physical and mental health
and mortality;
• Various physical and psychosocial
aspects of work can also be hazards
and pose a risk to health.Unemployment
• Conversely, there is a strong association between
worklessness and poor health.
• Possibly due to a health selection effect, but also
possibly a large extent cause and effect.
• There is strong evidence that unemployment is
generally harmful to health, including:
- higher mortality;
- poorer general health, long-standing illness, limiting
longstanding illness;
- poorer mental health, psychological distress, minor
psychological/psychiatric morbidity;
- higher medical consultation, medication consumption
and hospital admission rates.Re-employment
• There is strong evidence that re-
employment leads to improved
self-esteem, improved general
and mental health, and
reduced psychological distress
and minor psychiatric
morbidity.
• The magnitude of this
improvement is more or less
comparable to the adverse
effects of job loss.Do labour market status
transitions predict changes
in psychological well-being?
British Household Panel
Survey 1991-2007
• Positive effect of moving into
work not as large as the
negative effect of job loss.
Flint et Al Soc J Epid Com Health 2013Employment Status,
employment conditions
& limiting illness:
Prospective evidence from the
British Household Panel Survey 1991-2001
• Secure employment in favourable
working conditions greatly reduces
the risk of healthy people
developing limiting illness.
• Secure employment increases
the likelihood of recovery.
Flint et Al Soc J Epid Com Health 2013Health effects
of employment
A systematic review of prospective studies
• 33 Prospective studies
• 23 High Quality
• Strong evidence for
protective effect of
employment on
depression and
general mental health
Flint et Al Soc J Epid Com Health 2013Unemployment
and ill health
A connection through inflammation
• Increased inflammatory
markers more common
among the unemployed than
employed
• Five fold greater odds for
having an elevated
inflammatory status
Hintikka – BMC Public Health 2009Long term unemployment
- short telomeres
• Northern Finland Birth
cohort – 5620 men and
women
• Men: unemployment > 500
days associated with
having shorter leukocyte
telomere length (LTL)
• OR 2.61 (95% C1 1.16 -
5.85)
• No effect on women
Alla-Mursula - PLOS ONE 8 (11)Impact on Health of
Re-employment in
disability benefit recipients
• Compared to those who
remained on Benefits
• SF12 Mental Health
improvement 5.94 (CI
3.53-8.36)
• Physical Health
improvement 2.83 (CI
0.85-4.81u
Curnock et Al Soc sc and Med 162 (2016) 1-10Work for Sick and
Disabled People
Broad consensus across multiple
disciplines, e.g. disability groups,
employers, unions, insurers and all
political parties, based on extensive
clinical experience and on principles of
fairness and social justice. When their
health condition permits, sick and
disabled people (particularly those with
‘common health problems’) should be
encouraged and supported to remain in
or to (re)-enter work as soon as possibleWork for Sick and
Disabled People
because it:
• is therapeutic;
• helps to promote recovery and rehabilitation;
• leads to better health outcomes;
• minimises the harmful physical, mental and social effects
of long-term sickness absence;
• reduces the risk of long-term incapacity;
• promotes full participation in society, independence and
human rights;
• reduces poverty;
• improves quality of life and well-being.Work is generally
good for you
• Strong evidence base showing work is generally good
for physical and mental health and well-being.
• Worklessness is associated with poorer physical and
mental health and well-being.
• Work can be therapeutic and can reverse the adverse
health effects of unemployment.
• That is true for healthy people of working age, for
many disabled people, for most people with common
health problems and for social security beneficiaries.Work is generally
good for you
BUT….
• account must be taken of the nature and quality of
work and its social context;
• jobs should be safe and accommodating.
• Overall, the beneficial effects of work outweigh the
risks of work, and are greater than the harmful effects
of long-term unemployment or prolonged sickness
absence.
• Work is generally good for health and well-beingJimmy
aged 45
• Contractor
• Minimal Health & Safety
• No eye protection/ear muffs
• Early noise induced hearing loss
• Vibration white finger
• Several Eye injuries in pastJimmy
aged 45
• Irritant dermatitis
• Back injury in past
• Osteoarthritis of spine, shoulders,
elbows and knees
• 6 visits to accident and emergency
• One hand fracture
• Getting a bit past itJimmy
• Old housing • Left school with no
qualifications
• Poor diet, not much fruit,
veg or fish • Jobs on building sites
• 4 pints of beer a night • Frequently does overtime
(occasional drink at • Sometimes in informal
lunchtime) economy
• 20 Cigarettes a day • Few of his employers have
occupational Health &
• No leisure exercise Safety resourceJimmy • Separated lives with partner and two stepchildren • Two children by ex wife • Financial problems • Child care issues • Has been on courses to use power tools • No other education • Reads paper occasionally • Has home computer - on internet
Jimmy • He has an accident - pipe rolled on leg fracture of right tibia and fibula • Taken to hospital –transferred to orthopaedics – surgery, plated, discharged on crutches after two days (superb treatment) • No record of job in the hospital notes • No physiotherapy • Attends GP given certificate (“Fit Note”) • No guidance about rehabilitation
Jimmy • Rests at home, watches TV (gets depressed) • Progresses to walking with a stick • Wasting of quadriceps (50%) and reduction in power both legs, pain at fracture site • After 2 months GP organises physio - once per week for six weeks • Pain and weakness still a problem, GP says job will be too much for him • Follow up hospital appointment- no discussion about work
If we treated our professional footballers and athletes the same way we treat our workers… there would be no sport any weekend
How does the system fail Jimmy?
Problems for Jimmy
• Lack of rehabilitation
• Lack of systematic health promotion
• Employer has no occupational Health & Safety advice
• No system to advise about planned career change and life
long learning
• Employee/medical staff do not know how to get vocational
advice
• Employee care and development is not holistic
• Employer not participating fully in process of return to work
• Culture of tolerance of absence
• All leading to long term incapacityJimmy - Options
Friendly with the
boss- given job
driving the dump Sacked – goes on to
truck benefits after 6
monthsWorking for a Healthier
Tomorrow: Conclusions
• Annual economic costs of sickness-absence and
worklessness associated with ill-health are over
£100bn, greater than the current NHS budget, an
unsustainable burden in a competitive global
economy.
• Left unchecked this will diminish quality of life in
Britain, undermine efforts to reach full
employment, and deny business the talent and
contributions of a potential workforce.
• It will condemn workless families to a cycle of
poverty and dependency that will widen
inequalities, perpetuate social injustice in our
most deprived communities, and obstruct efforts
to eradicate child poverty.
Black Review, 2008Factors that Influence
Work Participation
Disease
External PersonalReason on IB
Total IB/SDA claimants by main disabling condition (expressed as % of total claimants) in
Glasgow City
60.0
50.0
40.0
%
30.0
20.0
10.0
0.0
Mental & Diseases of the Diseases of the Diseases of the Injury, Poisoning Other
Behavioural Nervous System Circulatory or Musculoskeletal and certain other
Disorders Respiratory System System and consequences of
Connective Tissue external causes
Main disabling condition
June 99 - August 99 Dec 05 - Feb 06Age standardised mortality
(Men) per 100,000Relationship between mortality (age/sex standardised rates per 100,000 population and deprivation (as measured by the Scottish Index of Multiple Deprivation-SIMD) )
So…what were the consequences of Jimmy’s
“expert” Medical treatment?Worklessness is the single most important cause
of health inequality, social exclusion, deprivation,
and mortalityImpact on the next
generation
Working for a healthier tomorrow, 2008
There is evidence that :
• Families with no-one working are more likely to suffer persistent
low income and poverty
• Lower parental income correlates with
poor health in children
• Child deaths from injury correlate with
low employment status and worklessness
• Behavioural and conduct disorders
are more likely where no parent is working
• Children of workless households are
more likely to experience worklessness
themselves when adult.Long-term worklessness
……is one of the greatest known risks to public health
• Health Risk = smoking 10 packs of cigarettes per day (Ross
1995)
• Suicide in young men > 6 months out of work is increased
40 x (Wessely, 2004)
• Suicide rate in general increased 6x in longer-term
worklessness (Bartley et al, 2005)
• Health risk and life expectancy greater than many “killer
diseases” (Waddell & Aylward, 2005)
• Greater risk than most dangerous jobs
(construction/Fishing)The Process of
becoming Workless
• Failure of the Education and Skill development sector
• Lifestyle factors not addressed systematically
• Lack of Occupational Health & Safety
• NHS doesn’t bother about return to work
- GP:“its not my job to get people back to work”
- Surgeon: “we are far too busy to take that on as well”
• The NHS does not have maximisation of functional capacity as
a treatment outcome measureBiopsychosocial Model Biopsychosocial model recognises that biological, psychological and social factors all affect human response to disease or illness. Indeed, health is best understood in terms of a combination of biological, psychological, and social factors rather than purely in biological terms (Engel 1977)
Ageing is a process
An “accumulation of deficits taking place in different individuals
in different ways, with a variety of rates for
different organ systems”
• Ageing is not solely a passive
degenerative process.
• Actively regulated by genetic pathways.
• Understanding the molecular basis of
ageing is a necessary step for
therapeutic manipulation of these
pathways to combat age-related
disorders such as cancer and CKD.
• Essential for good health in old ageComplex variations in health and functional status are not fully understood, highlighting the need for translational age- related research With respect to ageing and health: How are different organ systems interlinked? How does this relate to the whole organism? How do these play out through the life course? How are these influenced by socioeconomic status, psychological, nutritional and lifestyle factors?
Ageing across
the life course
Antagonistic Pleiotropy
Positive effects Negative effects
Shiels PG, Ritzau-Reid K. Curr Aging Sci. 2015;8(2):123-
30.Homeostasis implies that an organism remains
within a certain range of physiological parameters
to maintain stable function.
Telomere attrition
Deficient response to DNA damage
Epigenetic changes
Metabolic shift
Allostasis implies that an organism constantly Mitochondrial dysfunction
Defective ER stress responses
varies and adjusts physiological parameters
Decline in autophagy
to maintain stable function. Defective proteostasis
Decline in regenerative capacities
Stem cell exhaustion
Accounts for environmental stimuli SASP (Low grade chronic inflammation)
Cellular senescence
Accumulation of damaged cells
Damage to nuclear envelope (lamina)
Decline in renal function
Impaired immune defence
Low Klotho expression
Age Calciprotein particle (CPP) toxicity
Shiels PG, Ritzau-Reid K. Curr Aging Sci. 2015;8(2):123-30.
Shiels PG et al Nature Rev.Neph. 2017Re-employment, job quality,
health and allostatic load
bio-markers
Prospective evidence from UK Longitudinal study
• Allostatic load measured
by bio-markers
• Allostatic load increased:
Unemployed → poor
quality job
Chandola & Zhang, Int J of Epid 47:1:47-574 major elements to
premature Ageing in disease
General increase in the allostatic load
Oxidative stress
Persistent inflammation
Sympathicovagal imbalance
Disturbances in circadian rhythm
Activation of the ‘stress resistance response’
due to unfavorable conditions in the internal
environment,
Inactivation of anabolic pathways
Activation of catabolic pathways.
Disease-specific age-promoting mechanisms
Hyperphosphatemia
Hyperhomocysteinemia
Gut dysbiosis
Impaired activity of anti-aging defense
mechanisms (e.g. Klotho)
Koomans, Kotanko, Schols, Shiels and Stenvinkel.
Nat Rev Nephrol. 2014, 10(12):732-42.Glasgow • Scotland is ‘sick man’ of Europe • Glasgow is ‘sick man’ of Scotland • Why? - Ill health tied to steep SE gradient - May impact upon age related health
Extremes of ageing
in Glasgow
East endRelation Between Longevity
and Serum Phosphate
in MammalsThe Method of Dealing
With Workers with
Multiple Chronic
Diseases
Social reinforcers
Psychological
distress
Attitudes and
beliefs
Disability
Biopsychosocial model of disabilityIOSH / IOM
study 2015
Reviewed evidence on:
• Ageing and physical changes
• Psychological and mental well-being
• Work organisation factors
• Accidents and ill health
• Intervention studiesFactors explored in relation to age – physical,
psychological, sensory and organisational
Source: IOSHAgeing and
Physical Changes
• Reduced aerobic capacity,
increased body weight
• Muscle strength generally reduces
with age (1% per annum over age
35 years)
• Self-reported musculoskeletal
disorders increases with age
• Limited evidence that chronic neck
and shoulder pain increases with
age
• Moderate evidence that need for
recovery is greater in older workers
Source: IOSHAgeing & psychological
or mental well-being factors
• Reactions Slower –but offset by experience
• Regular intellectual stimulation and
cognitive exercise, maintain and
improvement ability.
• Majority of workers over the age of 65 show
no sign of cognitive impairment. (increases
over 70)
• Limited research on mental wellbeing in
older workers
• Older workers want to maintain and update
their skills and have access to training, just
as workers in general do.
Source: IOSHAgeing and work
organisation factors
• Limited evidence to show that working excessive overtime in
physically demanding jobs has an adverse effect on older
workers.
• Limited evidence that work ability reduced sooner in female
healthcare workers carrying out shiftwork than in male
healthcare workers
Source: IOSHAgeing and accidents
and ill health
• Older male workers were less of an accident risk but
females over 55 were found to have the highest estimated
incident rate.
• The risk of non-fatal serious injury was lowest in the older
worker group but the injuries sustained were more severe
and recovery took longer.
• There is an increased risk of developing chronic diseases
with age, but this doesn’t necessarily mean that work
shouldn’t be allowed.
• Short-term non-certified absence is the largest recorded
category of sickness absence. Workers over 55 take more
days off through self-reported ill health relating to work.
Source: IOSHIntervention studies
• No interventions found relating specifically to safety and
older workers
• OH interventions, e.g. health checks, rehabilitation and
mental health support, are viewed positively
• Action plans involving various professionals working
together can reduce the likelihood of sickness absence and
early retirement for health reasons
• Improvements to health promotion activities,
1.encouraging workers of all ages,
2.allowing time to attend during the working day,
3.consider the views of older workers on age-specific interventions.
Source: IOSHOccupational
Health Role
• Health checks useful
• Influence medical management
• Vocational rehabilitation - maximise function
• Physiotherapy
• Counselling
• Assessment of functional ability
• Career advice
• Recommend work adjustments
• Health surveillance of older workers
• Workplace health promotion programmes
Source: IOSHPredicting job loss
in those off sick
• 1. Patient’s prediction of likelihood of return to work
• after current sick leave –
Do you think you will be able to return to work after your current sick
• leave?
• 2. Patient’s prediction of ability to do current job in 6
• months’ time –
• Do you believe that from the standpoint of your health you will be able to do
• your current job in 6 months’ time?
3. The number of weeks off sick in the past year.
• 4. Whether they were waiting for a consultation or treatment
• for their health condition.
• 5. Age (more likely to return to work if younger in univariate
• model).
• (C-index 0.90)
Wilford , Macdonald Occup Med 2008;58:99–106The process for maintaining the workability of the ageing worker with
multiple diseases
(developed from Juhani E Ilmarinen Occup Environ Med 2001;58:546)
Health Education Psychosocial Work Organisation
Maintaining & improving New skills Adaptations Adaptations
WORKABILITYInterventions
• Political – sick note to a fit note in the UK- Fit for
work Service
• Denmark intervention Project
1. RTW coordinator
2. Multidisciplinary support to sick leave cases
1. Better coordination between employer , Health Care,
Social system
3. Early and regular content with employees during
sickness absenceAdapting work and
work environment
worker perspective
• Job design and rotation
• More frequent short breaks
• Improved organisation of shift work eg fast forward
rotation (2-3 days)
• Good lighting and noise control
• Imprved ergonomics and human factorsWorkability • Health and functional capability • Values attitudes and motivation • Work environment and community • Content, demands and organisation of work • Workability Index
Practical approach • Health improvement programmes specifically designed for older workers • Specific risk assessments • Job adaptation and adjustments • Reduced hours and regular breaks • Targeted Health checks and FCE • Case management of the older worker with health problems • Older worker apprenticeships and retraining
What to do about the
growth of NCD and
workers’ health
• It is not normal to be normal
• Implement the process for maintaining workability
• Use the biopsychosocial approach
• Maximise functional abilityYou can also read