The Growing Threat of Qui Tam Litigation Against Healthcare Providers
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
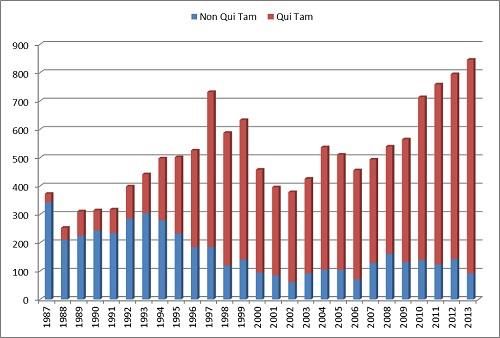
Winter 2015, Vol. 12 No. 1 The Growing Threat of Qui Tam Litigation Against Healthcare Providers By Amandeep S. Sidhu – December 9, 2014 Over the past few years, there have been steady changes in the regulatory, enforcement, and litigation environment that should worry every company providing goods or services to the United States. Hospitals and other healthcare providers, in particular, should be on guard. While providers have long-feared the False Claims Act (FCA), Stark law, and anti-kickback statute— and have often crafted compliance, education, and oversight in response—the 2009 Fraud Enforcement and Recovery Act (FERA) amendments to the FCA and the corresponding uptick in FCA actions and recoveries have resulted in a litigation climate today that is more troubling than ever. To provide some context, there has been a substantial increase in FCA recoveries over the past five years, and more and more of this money is coming from hospitals. Between 2009 and 2013, the United States recovered over $17 billion from FCA litigation. Of the $3.8 billion in FCA settlements and judgments secured by the U.S. Department of Justice (DOJ) in 2013, $2.6 billion came from healthcare providers and nearly $1 billion came from hospitals. See, e.g., Press Releases, U.S. Dep’t of Justice, Justice Department Recovers $3.8 Billion from False Claims Act Cases in Fiscal Year 2013 (Dec. 20, 2013). Often, the litigation and ultimate recoveries have little to do with the actual provision of care to patients. Rather, the cases involve issues related to a provider’s billing and coding or physician productivity and compensation. Many of the allegations do not even challenge the fact that medically necessary services were provided to patients or that the physicians were compensated based on services they personally performed for patients; rather, the suits challenge the “how” of billing and calculating incentives. It is “gotcha” litigation at its finest. Qui Tam Litigation Starting with the 1987 amendments to the FCA, the percentage of cases being brought by whistleblowers has steadily increased. Since 1995, the majority of FCA litigation has taken the form of qui tam actions, whereby a whistleblower is acting on behalf of the United States in seeking fraud recovery. In 2013, 753 of the 846 newly initiated cases were qui tam cases. See U.S. Dep’t of Justice, Fraud Statistics—Overview (Dec. 23, 2013). While the risk of qui tam litigation being brought by a whistleblower is nothing new, there has been a steady revolution in the way these cases are being handled over the past five years. Gone are the days when the United States’ decision not to intervene allowed a provider’s general counsel to breathe a sigh of relief and manage less aggressive litigation from the qui tam _________________________________________________________________________________________________________ © 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database or retrieval system without the express written consent of the American Bar Association.
Health Law Litigation Winter 2015, Vol. 12 No. 1 _________________________________________________________________________________________________________ plaintiffs’ bar. With the 2009 FERA amendments to the FCA, the success of relators in cases in which the United States declined to intervene has increased exponentially. Of the $342 million recovered by relators pursuing non-intervened claims since 1987, over half has been the result of settlements or judgments in the past four years. Qui Tam Litigation Statistics With the incentive of a potential 30 percent share on the non-intervened claims, whistleblowers and their lawyers are more motivated than ever to vigorously litigate a case on behalf of the government. The United States is often declining to make an intervention decision prior to the unsealing of a qui tam complaint at the outset; rather, DOJ lawyers sit on the sidelines while well-funded whistleblower lawyers increasingly able to expend significant resources begin litigating the case, watching closely to determine whether and when the expenditure of government resources could result in a significant recovery. Courts are hesitant to deny the United States the opportunity to intervene late in the game, provided the intervention does not significantly affect the existing case schedule. Also gone are the days when FCA litigation was derived from undisputed falsity—today providers are facing the gray areas that were once thought to be immune from FCA litigation. While the so-called “Lincoln Law” was enacted during the Civil War to combat undisputable false claims seeking payment for goods and services that were never rendered, the FCA is used today to combat a far broader swath of transactions. With over $35 billion in recoveries since the 1986 amendments, the FCA is the government’s principal weapon against fraud. _________________________________________________________________________________________________________ © 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database or retrieval system without the express written consent of the American Bar Association.
Health Law Litigation
Winter 2015, Vol. 12 No. 1
_________________________________________________________________________________________________________
The False Claims Act
Generally, the types of false claims covered by the FCA are (1) factually false claims, (2) legally
false claims (false certification), and (3) reverse false claims. FCA litigation is typically focused
on two liability provisions: (1) the false claims provision under 31 U.S.C. § 3729(a)(1)(A),
which creates liability for knowingly presenting, or causing to be presented, a false or fraudulent
claim for payment to the United States; and (2) the false statement provision under 31 U.S.C.
§ 3729(a)(1)(B), which creates liability for knowingly making, using, or causing to be made or
used, a false record or statement material to a false or fraudulent claim.
False certification claims take the form of express certification or implied certification theories.
For providers, implied certification theories are largely derived from Medicare conditions of
participation and conditions of payment (discussed further below).
Implied certification theories have been accepted by the Second, Third, Sixth,
and Ninth Circuits where the certification is an express condition of payment.
Where the provision is an implied condition of payment, the First, Eighth, Tenth,
and D.C. Circuits have accepted implied certification theories. The Eleventh
Circuit has recognized implied certification theories but has not clearly articulated
a position on the express/implied condition of payment question.
Implied certification has not been adopted in the Fourth, Fifth, and Seventh
Circuits.
Leaving aside the wide split among the circuit courts, the threshold question that most courts are
asking is whether the certification is material to the provision of care. Generally, the closer the
regulation is to the government’s payment to the provider, the more likely it is a court will allow
implied certification claims to go forward.
The distinction between Medicare conditions of participation and conditions of payment is a hot-
button issue in FCA litigation today. Conditions of participation are standards that hospital
providers “must meet in order to begin and continue participating in the Medicare and Medicaid
programs.” See Ctrs. for Medicare & Medicaid Servs., Conditions for Coverage & Conditions of
Participations (June 17, 2014).
In stark contrast, conditions of payment are standards that providers must meet to be paid by the
Medicare program for items and services that they furnish. The Centers for Medicaid &
Medicare Services has determined that the conditions of participation, which govern most
aspects of hospital operations, are better enforced administratively—with specific administrative
remedies and penalties to address noncompliance—rather than through the blunt force of the
FCA. See 42 C.F.R. §§ 488.10, 488.24.
While relators have recently pursued theories that a provider’s noncompliance with a condition
of participation (e.g., the existence of a physician order for admission) establishes “falsity” and
“knowing” conduct, courts have consistently distinguished conditions of participation from
conditions of payment. See, e.g., United States ex rel. Williams v. Renal Care Grp., 696 F.3d
_________________________________________________________________________________________________________
© 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any
portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database
or retrieval system without the express written consent of the American Bar Association.Health Law Litigation
Winter 2015, Vol. 12 No. 1
_________________________________________________________________________________________________________
518, 532 (6th Cir. 2012); United States ex rel. Conner v. Salina Reg’l Health Ctr., Inc., 543 F.3d
1211, 1221 (10th Cir. 2008).
There are several key provisions of the FCA that should keep providers awake at night:
Treble damages. After the judge or jury determines single damages at trial, the
court must apply mandatory treble damages.
Civil penalties. The court must also impose mandatory civil penalties of $5,500 to
$11,000 per claim identified at trial.
Whistleblowers incentives. The relator gets up to 30 percent of the recovery on
non-intervened claims and up to 25 percent of the recovery on intervened claims.
Attorney fees. Relator’s counsel are entitled to recovery of reasonable fees,
which adds additional incentives to the lawyers.
To be clear, a jury’s single damages award is subject to mandatory post-verdict trebling by the
court and a minimum $5,500 penalty per claim. For their efforts, whistleblowers (and their
lawyers) receive sizable shares of the recovery, whether or not the United States intervened.
Finally, relator’s counsel who assumed the contingency-fee risk of taking on the whistleblower’s
case are entitled to reasonable attorney fees for their efforts.
Passage of the Patient Protection and Affordable Care Act (ACA) in 2010 also ushered in four
significant changes to the FCA that are favorable to relators and could add exposure risk to
providers. First, the public disclosure bar was amended to provide for the United States to have
the final say on whether a defendant can avail itself of what previously was a standard defense
against a qui tam lawsuit. See 31 U.S.C. § 3730(e)(4)(A) (“[T]he court shall dismiss an
action . . . unless opposed by the Government, if substantially the same allegations or
transactions as alleged in the action or claim were publicly disclosed.”).
Second, the ACA revised the original source requirement to provide relators with a lower
threshold of knowledge necessary to overcome the public disclosure bar. While relators were
previously required to have “direct and independent knowledge of the information on which the
allegations are based,” they now need only have “knowledge that is independent of and
materially adds to the publicly disclosed allegations or transactions.” See 31 U.S.C.
§ 3730(e)(4)(B).
Third, the ACA added a 60-day clock to the 2009 Fraud Enforcement and Recovery Act
amendments regarding the retention of overpayments, requiring providers to report and return
any overpayments within 60 days of discovery or be subjected to potential FCA liability. See 31
U.S.C. §§ 3729 et seq.; 42 U.S.C. § 1320a-7k (as added by the Patient Protection & Affordable
Care Act, Pub. L. 111-148, effective Mar. 23, 2010).
Finally, the ACA resolved a circuit split regarding whether claims submitted as a result of
violations of the anti-kickback statute constitute false claims for purposes of FCA liability.
Providers now face automatic statutory liability under the anti-kickback statute. See 42 U.S.C.
§ 1320a-7b(g), (h).
_________________________________________________________________________________________________________
© 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any
portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database
or retrieval system without the express written consent of the American Bar Association.Health Law Litigation
Winter 2015, Vol. 12 No. 1
_________________________________________________________________________________________________________
Recent Qui Tam Cases
In 2013, a South Carolina district court ordered over $39 million in damages and over $237
million in statutory penalties against Tuomey Healthcare Systems, Inc., for Stark-based FCA
allegations. United States ex rel. Drakeford v. Tuomey Healthcare Sys., Inc., 976 F. Supp. 2d 776
(D.S.C. 2013). As most readers know, Tuomey is not part of a large hospital system—at the time
of the litigation, it was a 242-bed community hospital with just over $200 million in annual
revenue. By all accounts, this was “bet the company” litigation for Tuomey.
After a procedural win in the Fourth Circuit for Tuomey, the case was sent back to the trial court
in the District of South Carolina for retrial, resulting in the ultimate $277 million judgment. The
Tuomey litigation was a wake-up call for all providers—and hospitals, in particular—that enter
into contractual arrangements with physicians. With FCA violations pinned to over 20,000
claims bootstrapped to Stark law violations involving 19 specialty physician contracts, the
Tuomey judgment is the sum of all fears for a provider’s general counsel, management, board,
and (in the for-profit world) shareholders.
A few other significant recent cases are summarized below.
United States ex rel. Ketroser v. Mayo Found., 729 F.3d 825 (8th Cir. 2013). FCA
allegations that the hospital fraudulently billed Medicare for certain surgical
pathology services related to the analysis of tissue samples because it failed to
prepare separate written reports of those services as required by Medicare
conditions of participation regulations. The Eighth Circuit held that the district
court properly dismissed the claim because the regulations do not specifically
require compliance as a condition of payment.
United States ex rel. Hobbs v. MedQuest, 711 F.3d 707 (6th Cir. 2013).
Allegations that MedQuest fraudulently billed Medicare for certain diagnostic
testing services because it (a) used physician-supervisors who were not
approved by the local Medicare carrier and (b) failed to properly re-register its
facility to reflect ownership changes or to enroll it in Medicare. The Sixth Circuit
held that the district court improperly granted summary judgment against
MedQuest because compliance with applicable regulations was not a condition of
payment from Medicare.
United States ex rel. Sanchez-Smith v. Tulsa Reg’l Med. Ctr., 754 F. Supp. 2d
(N.D. Okla. 2010). Allegations that the hospital fraudulently billed the Oklahoma
Medicaid program for inpatient psychiatric services provided to children because
it failed to comply with “quality of care” regulations specifying hourly care per
week. Here, the hospital’s motion for summary judgment was denied because
the regulations at issue were directly tied to reimbursement and related to
objective and quantitative criteria.
A Robust Compliance Program Is a Provider’s Best Defense
Providers should recognize that compliance is complicated, and it is virtually impossible to be in
compliance with each regulation every minute of every day. A provider’s compliance function
_________________________________________________________________________________________________________
© 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any
portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database
or retrieval system without the express written consent of the American Bar Association.Health Law Litigation
Winter 2015, Vol. 12 No. 1
_________________________________________________________________________________________________________
has to be a team effort—part of the company’s culture and delegated where appropriate to ensure
that efforts are being made for compliance.
Providers should recognize that seemingly minor issues can give rise to large exposure.
Therefore, the lead compliance officer should be a senior executive with actual authority to take
action when compliance concerns are raised. The provider should have a robust compliance
program that is driven by the compliance officer and his or her team, but must have the buy-in of
everyone up and down the chain of command. Policies and procedures are not effective without
reinforcement from the chief executive officer on down, and implementation of the compliance
program does not work without buy-in from mid-level management.
The focus should be on key issue areas. A provider’s compliance program will be
more effective if issues are triaged and handled efficiently but comprehensively.
Given the government’s focus on Stark law and anti-kickback statute issues in
recent years, ensure that arrangements between providers and physicians are
reviewed to confirm compliance with the law. If relationships need to be
unwound, unwind them. Options for self-disclosure to regulatory agencies should
also be considered when the facts are appropriate.
When it comes to compliance, perfection is nearly impossible. The types of cases
dominating the FCA landscape are not black and white—they are largely in the
gray area. With the recent surge in compliance-driven FCA litigation, it is clear
that minor issues can generate large exposure. Recent cases have focused on
supervision, licensing, and fair-market-value analysis—all issues where the line
between “right” and “wrong” is incredibly thin.
Further complicating matters, today’s FCA cases are taking complex theories of liability to the
jury. Regardless of where the law is on the issue, the complexity of the issue is likely to be lost
on a jury. Have you ever tried to explain the difference between Medicare conditions of
participation and Medicare conditions of payment to your neighbor? Or even to a non–health-law
attorney? Now imagine your outside counsel trying to draw that distinction for a jury at trial.
While FCA litigation is incredibly complex, the task at trial continues to be explaining the issues
to the jury in plain English.
The Response to a Government Investigation Is Critical
While it can be a jarring experience to be on the receiving end of an Office of Inspector General
subpoena that appears to sweep broadly across an array of potential FCA violations, the internal
investigation that follows is the single most critical step in the process for a hospital provider.
What is learned from witness interviews and documents—and, more important, what is conveyed
to government officials—will shape how the litigation proceeds from that point forward.
A provider’s one shot to convince the United States not to intervene in a qui tam lawsuit comes
during this investigative phase of the case. This is critically important because 94 percent of
cases in which the United States declines to intervene are dismissed. And the vast majority of
recoveries continue to come from cases in which the United States has intervened. In 2013, $2.8
_________________________________________________________________________________________________________
© 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any
portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database
or retrieval system without the express written consent of the American Bar Association.Health Law Litigation
Winter 2015, Vol. 12 No. 1
_________________________________________________________________________________________________________
billion of the $2.9 billion recovered in qui tam litigation was from cases in which the United
States intervened or otherwise pursued the claims. See Fraud Statistics—Overview.
As the investigation unfolds and presentations are developed for Office of Inspector General
investigators and the DOJ trial attorneys, expect that the government knows more than the
provider. Remember, the DOJ lawyers are being spoon-fed whatever documents and company
secrets the whistleblower stole and handed over to his or her lawyers, so providers must make
every effort to get ahead of the curve and be aggressive out of the gate, gathering information to
fully understand the issues at hand. Part of this strategy will include determining when to
strategically invoke privilege to protect documents and when privilege should be waived to
establish a complete picture of the provider’s compliance and oversight regime.
But even when the United States declines to intervene, whistleblowers are proceeding into
litigation with the resources to take defendants to task. Often they are joining forces with other
plaintiff-side firms to distribute the workload (and, more important, the cost) to pursue the
litigation without the DOJ’s backing. This allows for cost sharing and distribution of the
workload across several lawyers.
Providers must also have a media-response strategy. To the extent the relator’s counsel are still
in the picture, they will be going to the media at every opportunity to pressure the hospital into a
large settlement.
Defending Against Litigation
To describe qui tam litigation as multifaceted is an understatement. There can be a range of
potential plaintiffs bringing a range of potential claims.
Even before the qui tam complaint is unsealed—during the investigatory phase—providers
should be thinking about potential defenses. And when the complaint is unsealed, counsel should
be ready to attack the claims and incorporate arguments into a motion to dismiss the complaint.
Review the date range of the claims and determine whether there are any viable statute-of-
limitation defenses that should be raised. If the FCA suit has Stark law or anti-kickback-statute
claims bootstrapped into the FCA allegations, think about potential affirmative defenses such as
failure to plead fraud with sufficient particularity, the statute of limitations, regulatory ambiguity,
and the public disclosure bar and original source requirement (as augmented by the 2010 ACA
changes to the FCA).
Providers should also be thinking about mandatory FCA treble damages from the outset. While
your strategy is obviously to dismiss the claims altogether, you have to be constantly focused on
chipping away at the scope of damages that could go to the jury.
Relator cannot recover FCA penalties. If the relator is pursuing non-intervened
claims, consider filing a motion for judgment on the pleadings regarding the
relator’s inability to recover FCA penalties for lack of Article III standing. With a
circuit split and the issue likely to go to the Supreme Court in the next term, this
off-the-shelf brief can be filed with little additional cost and effort for an
_________________________________________________________________________________________________________
© 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any
portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database
or retrieval system without the express written consent of the American Bar Association.Health Law Litigation
Winter 2015, Vol. 12 No. 1
_________________________________________________________________________________________________________
experienced law firm. In short, long-established standing principles make it clear
that a private party has no standing to seek penalties to vindicate public rights.
Unlike FCA damages, FCA civil penalties vindicate public rights by redressing
the injury to the government’s sovereignty arising from violation of its laws.
Proper measure of damages includes offset. Starting with fact and expert
discovery, providers should be cognizant of the proper measure of potential
damages. As a general rule, the appropriate measure of damages under the FCA
is the government’s payment to the provider less the value of the goods or
services that were actually provided. See United States v. Bornstein, 423 U.S.
303, 317 (1976). Therefore, if the plaintiffs allege that the facility’s inpatient
admissions for certain procedures were not medically necessary, providers
should be thinking about strategically asserting that that damages must be
calculated to account for an outpatient or observation payment for the services
that were rendered.
Net trebling. As an extension of arguing that the proper measure of damages
includes an offset, courts are increasingly adopting “net trebling” provisions,
wherein the FCA multiplier of three is applied only after reducing the damages by
the value of the good or services that were provided to the government payer. In
United States v. Anchor Mortgage Corp., 711 F.3d 745, 751 (7th Cir. 2013), the
Seventh Circuit adopted the net trebling approach to calculating FCA damages,
holding that the multiplier can be applied only after offsetting the government’s
loss by the value of the goods or services received. As it happens, the Seventh
Circuit is a good place to be sued under the FCA as the courts have upheld
several defense-friendly positions.
Conclusion
In light of the recent trend in the FCA litigation landscape, providers should be taking stock of
their compliance and oversight functions and identifying weaknesses in the system that could
give rise to a whistleblower bringing a qui tam action. By establishing a proactive and reactive
strategy, providers can be prepared to combat the rising threat of qui tam litigation.
Keywords: litigation, health law, Affordable Care Act, ACA, False Claims Act, FCA, health
care
Amandeep S. Sidhu is a partner in McDermott Will & Emery LLP's Washington, D.C., office.
_________________________________________________________________________________________________________
© 2014 by the American Bar Association. Reproduced with permission. All rights reserved. This information or any
portion thereof may not be copied or disseminated in any form or by any means or stored in an electronic database
or retrieval system without the express written consent of the American Bar Association.You can also read