The Preoperative Use of Gabapentin, Dexamethasone, and Their Combination in Varicocele Surgery: A Randomized Controlled Trial
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pain Medicine
Section Editor: Spencer S. Liu
The Preoperative Use of Gabapentin, Dexamethasone,
and Their Combination in Varicocele Surgery:
A Randomized Controlled Trial
Serhat Koç, MD* BACKGROUND: We investigated the effects of gabapentin and dexamethasone given
together or separately 1 h before the start of surgery on laryngoscopy, tracheal
Dilek Memis, MD* intubation, intraoperative hemodynamics, opioid consumption, and postoperative
pain in patients undergoing varicocele operations.
METHODS: Patients were randomly divided into four double-blind groups: group C
Necdet Sut, PhD† (control, n ⫽ 20) received placebo, group G (gabapentin, n ⫽ 20) received 800 mg
gabapentin, group D (dexamethasone, n ⫽ 20) received 8 mg dexamethasone,
group GD (gabapentin plus dexamethasone) received both 800 mg gabapentin and
8 mg dexamethasone IV 1 h before the start of surgery. Standard induction
and maintenance of anesthesia were accomplished and continued by propofol
and remifentanil infusion. Heart rate and arterial blood pressure were recorded
before induction and after intubation. Intraoperative total remifentanil consump-
tion was recorded. Hemodynamic variables and visual analog scale were recorded
for 24 h. Side effects were noted.
RESULTS: Hemodynamics at 1, 3, 5, and 10 min after tracheal intubation, total
remifentanil consumption during surgery, postoperative visual analog scale scores
at 30 min, 1, 2, 4, 6, and 12 h, and postoperative nausea and vomiting were found
to be significantly lower in group GD than in group G and group D (P ⬍ 0.05 for
both), and substantially lower when compared with group C (P ⬍ 0.001). All values
in group C were also higher than in groups G and D (P ⬍ 0.05).
CONCLUSION: Gabapentin and dexamethasone administered together an hour before
varicocele surgery results in less laryngeal and tracheal intubation response,
improves postoperative analgesia, and prevents postoperative nausea and vomit-
ing better than individual administration of each drug.
(Anesth Analg 2007;105:1137–42)
G abapentin and dexamethasone are two well toler-
ated and mechanistically diverse drugs that have each
(6 –10). Studies have shown synergism between gaba-
pentin and morphine for analgesic effects in animals
shown promise in the management of postoperative and in humans (11–13). Preoperative oral gabapentin
pain. Gabapentin, a structural analog of ␥-aminobutyric reduces opioid consumption in patients undergoing
acid, is used as an anticonvulsant drug. In addition, it surgery (14 –16). In a recent systematic review, peri-
has been shown to be effective in neuropathic pain (1), operative oral gabapentin was a useful adjunct for the
diabetic neuropathy (2), postherpetic neuralgia (3), management of postoperative pain that provided an-
and complex regional pain syndrome Type 1 (4). algesia through a different mechanism than opioids
Studies have demonstrated that mechanical hyperal- and other analgesic drugs and would make a reason-
gesia surrounding the wound in postoperative pa- able addition to a multimodal analgesic treatment
tients, and experimentally, heat-induced, secondary plan (17).
hyperalgesia, share a common mechanism, and that Glucocorticoids are well-known for their analgesic,
central neuronal sensitization contributes to postop- antiinflammatory, immune-modulating, and antiemetic
erative pain (5). Gabapentin has a selective effect on effects, although the mechanisms by which glucocorti-
the nociceptive process involving central sensitization coids exert their action are far from clarified (18). Several
randomized, clinical trials in many different major and
From the Departments of *Anaesthesiology and Reanimation, minor surgical procedures have been conducted to
and †Bioistatistic, Medical Faculty, Trakya University, Turkey.
examine the effects of a perioperative single-dose glu-
Accepted for publication June 13, 2007.
cocorticoid administration on surgical outcome (19). The
Address correspondence and reprint requests to Dilek Memis,
MD, Department of Anaesthesiology and Reanimation, Medical overall results on postoperative outcome have either
Faculty, Trakya University, 22030, Edirne, Turkey. Address e-mail been positive in favor of the glucocorticoid group or
to dilmemis@mynet.com. without differences between study groups, with postop-
Copyright © 2007 International Anesthesia Research Society erative nausea and vomiting and pain as outcome vari-
DOI: 10.1213/01.ane.0000278869.00918.b7
ables most significantly improved (17,19 –21).
Vol. 105, No. 4, October 2007 1137In our literature search, we could not find any MAP, HR, and Spo2 were monitored through non-
study evaluation effect of gabapentin and dexameth- invasive continuous measurement. HR and MAP were
asone on tracheal intubation and intraoperative hemo- recorded at baseline (before induction of anesthesia),
dynamics and postoperative analgesia. For this which was the mean of the three resting measure-
reason, we investigated the effects of gabapentin and ments in the operating room before any instrumenta-
dexamethasone, given together or separately, 1 h tion, 1, 3, 5, 10, 15, 30, 40, and 60 min after tracheal
before the start of the surgery, on the responses to intubation. MAP and HR were maintained within 20%
laryngoscopy and intubation, intraoperative hemody- of baseline values using a predetermined decision
namics, opioid consumption, and postoperative pain algorithm for adjustment of the opioid and propofol.
in patients undergoing varicocele operations. The remifentanil infusion rate was first decreased by
25% in case of hypotension or bradycardia; if this was
METHODS insufficient to restore values to within 20% of baseline
After obtaining the approval of the Institutional Ethics after two adjustments, the propofol infusion was also
Committee (Trakya University, Edirne, Turkey) and adjusted upward or downward by 25%. Five minutes
written consent of the patients, 80 normotensive patients were allowed between each adjustment. The total
(ASA physical status I) undergoing elective varicocele remifentanil and propofol consumption by each pa-
surgery were randomly assigned to four groups of 20 tient was determined and noted. Ephedrine (3 mg
patients each. Exclusion criteria were cardiac disease, increments) was administered for hypotension (MAP
contraindications to anesthetics, asthma, renal insuffi- ⬍80 mm Hg, or a decrease of ⬎30% from baseline
ciency, predicted difficulty in intubation or airway values for ⬎60 s) and atropine, in 300 g increments,
maintenance, and pregnancy. The study design was for bradycardia (HR ⬍45 bpm/min).
randomized and double-blind; patients were randomly Immediately after the placement of the last skin
allocated according to computer-generated randomiza- suture, propofol, remifentanil, and N2O were discon-
tion. The control group (n ⫽ 20) received oral placebo ⫹ tinued. After patients were tracheally extubated, ven-
IV 2 mL saline (group C), group G (n ⫽ 20) received oral tilation was assisted until the recovery of spontaneous
800 mg of gabapentin (Neurontin, 400-mg capsule, breathing after the patients were extubated.
Pfizer, Goedecke GmbH, Germany) ⫹ IV 2 mL saline, After tracheal extubation, patients were transferred to
group D (n ⫽ 20) received oral placebo ⫹ IV 8 mg the postanesthesia care unit. Assessment of postopera-
dexamethasone (Dekort amp 4 mg/mL, Deva, Istanbul), tive pain was made with a visual analog scale score
and group GD (n ⫽ 20) received 800 mg of gabapentin ⫹ (VAS; 0 cm ⫽ no pain and 10 cm ⫽ worst pain
8 mg of dexamethasone 1 h before surgery in the imaginable). During the first 1 h in the postanesthesia
operating room. The study drugs were prepared by the care unit, then at 2, 4, 6, 12, and 24 h in the patient’s
pharmacy, and an appropriate code number was as- room, patients were evaluated for pain scores, HR, and
signed. The occurrence of any side effects, such as MAP by an anesthesiology resident not otherwise in-
nausea and vomiting, respiratory depression, dizziness, volved in the study. Additional analgesic requirements
somnolence, peripheral edema, or headache, was re- for each group within 24 h were determined according
corded. After the patients had been taken to the operat- to VAS; when VAS values were ⬎3, tenoxicam 20 mg IM
ing room, crystalloid infusion was started through a was administered and noted. The occurrence of any side
20-gauge IV cannula inserted in an appropriate antecu- effects, such as nausea and vomiting, constipation, respi-
bital vein, and the mean arterial blood pressure (MAP), ratory depression, dizziness, somnolence, peripheral
heart rate (HR), and peripheral oxygen saturation (Spo2) edema, diarrhea, headache, and pruritis were recorded.
were monitored. On patient request, or if nausea and vomiting occurred,
Oxygen was administered via an anesthetic breathing ondansetron 4 mg IV was given.
circuit and facemask. After 3 min of administration of Normality distribution of the variables was tested
oxygen, induction of anesthesia was achieved in all using the one sample Kolmogorov-Smirnov test. De-
patients with a continuous infusion of remifentanil 0.5 mographic characteristics were compared using one-
g 䡠 kg⫺1 䡠 min⫺1 followed by propofol 2 mg/kg. Then, way ANOVA test, differences from baseline within
0.5 mg/kg atracurium was given to facilitate tracheal groups were evaluated using repeated measures
intubation and to maintain neuromuscular blockade, ANOVA test for normally distributed data, and the
monitored by train-of-four stimulation with a peripheral Freidman ANOVA test for nonnormal distributed
nerve stimulator. Laryngoscopy and tracheal intubation data. Bonferroni post hoc tests were used to correct for
were then performed 3 min after loss of verbal contact by multiple comparisons. Categorical variables were an-
the same experienced anesthesiologist using a Mcintosh alyzed using the 2 test. Statistica 7.0 statistical soft-
three laryngoscope blade and 8.0 mm endotracheal tube. ware was used for statistical analysis. P ⬍ 0.05 was
After tracheal intubation, the lungs were ventilated with considered statistically significant.
50% N2O in oxygen, and end-tidal CO2 was maintained
at between 30 and 35 mm Hg. Remifentanil infusion was RESULTS
then reduced to 0.25 g 䡠 kg⫺1 䡠 min⫺1 in all patients after There were no significant differences among the
propofol infusion (4 mg 䡠 kg⫺1 䡠 h⫺1) was started. four groups with respect to, age, weight, duration of
1138 Gabapentin and Dexamethasone ANESTHESIA & ANALGESIATable 1. Demographic Characteristics
Group C Group G Group D Group GD
Variable (n ⫽ 20) (n ⫽ 20) (n ⫽ 20) (n ⫽ 20)
Age (yr) 41.10 ⫾ 20.85 39.45 ⫾ 19.27 38.35 ⫾ 17.43 35.25 ⫾ 18.01
Weight (kg) 72.65 ⫾ 12.28 74.55 ⫾ 10.02 72.70 ⫾ 12.85 76.25 ⫾ 11.29
Duration of anesthesia (min) 78.2 ⫾ 25.92 90.75 ⫾ 37.60 94.00 ⫾ 46.61 86.05 ⫾ 28.14
Duration of surgery (min) 67.35 ⫾ 22.85 79.25 ⫾ 36.50 79.15 ⫾ 41.94 73.55 ⫾ 27.47
Intraoperative remifentanil consumption (mg) 745.7 ⫾ 119.7 408.5 ⫾ 139.7* 409.2 ⫾ 136.6* 249.1 ⫾ ⫺85.7†‡
Values are shown as number (n) of patients or mean ⫾ SD.
*P ⬍ 0.05, when group C compared with group G and group D.
†P ⬍ 0.001, when group GD compared with group C.
‡P ⬍ 0.05, when group gabapentin (G) and dexamethasone (D) compared with group gabapentin and group dexamethasone (GD).
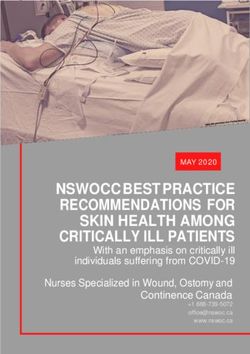
Figure 1. Intraoperative mean arterial blood
pressure data (mean ⫾ sd). The initial mean
arterial blood pressure was similar in all
groups. Mean arterial blood pressure val-
ues were statistically significantly lower in
the gabapentin– dexamethasone group at 1,
3, 5, and 10 min after tracheal intubation
than the dexamethasone group and gabap-
entin group (P ⬍ 0.05); when compared
with the control group, these values were
substantially lower (P ⬍ 0.001). The gabap-
entin group and dexamethasone group did
not differ statistically (P ⬎ 0.05), whereas
values were significantly lower in the gaba-
pentin group and dexamethasone group
compared with the control group (P ⬍
0.05).
surgery (Table 1). We did not observe any side effects, group G and group D were similar (Table 1). The
such as nausea and vomiting, respiratory depression, propofol infusion was kept constant.
dizziness, somnolence, peripheral edema, or headache Postoperative MAP and HR variables were similar
during the 1-h period before surgery. in the four groups at 30 min, 1, 2, 4, 6, 12, and 24 h after
Cardiovascular responses are shown in Figures 1 tracheal extubation (P ⬎ 0.05).
and 2. The initial hemodynamic variables were similar VAS scores were found to be significantly lower in
in all groups. HR and MAP values were significantly group GD at 30 min, 1, 2, 4, 6, and 12 h than in group
lower in group GD at 1, 3, 5, and 10 min after G and group D (P ⬍ 0.05 for both) and in group C (P ⬍
intubation than in group D and group G (P ⬍ 0.05) 0.001). Values in group C were also higher in group G
and in group C (P ⬍ 0.001). Hemodynamics was and D (P ⬍ 0.05). Group G and group D did not differ
similar in group G and group D, but lower than group significantly from each other (Fig. 3).
C (P ⬍ 0.05). One patient in group GD had transient Total tenoxicam consumption during the first 24 h
hypotension (MAP ⬍80 mm Hg for ⬍1 min), which postoperatively was significantly lower in group GD
did not require ephedrine. There were no bradycardia, (0 mg) than in group G (80 mg) and group D (80 mg)
tachycardia, or arrhythmias, ST segment alterations, or (P ⬍ 0.05 for both) and in group C (300 mg) (P ⬍
other echocardiographic changes observed during the 0.001). Each of these values in group C was higher
study. We did not use ephedrine or atropine. than group G and D (P ⬍ 0.05). Group G and group D
Intraoperative total remifentanil consumption was did not differ significantly from each other.
significantly lower in group GD (249.1 ⫾ 85.7 mg) Postoperative nausea and vomiting occurred in 15
than in group G (408.5 ⫾ 139.7 mg) and group D of 20 (75%) patients in group C, 8 of 20 (40%) patients
(409.2 ⫾ 136.6 mg) (P ⬍ 0.05 for both) and in group C in group G, 7 of 20 (35%) patients in group D, and 1 of
(745.7 ⫾ 119.7 mg) (P ⬍ 0.001). Values in group C were 20 (5%) patients in group GD. The incidence of post-
higher than in group G and D (P ⬍ 0.05), whereas operative nausea and vomiting was less frequent in
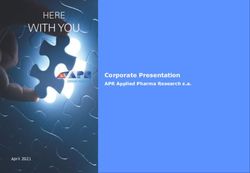
Vol. 105, No. 4, October 2007 © 2007 International Anesthesia Research Society 1139Figure 2. Intraoperative heart rate data
(mean ⫾ sd). The initial heart rate was
similar in all groups. Heart rate values
were statistically significantly lower in
the gabapentin– dexamethasone group at
1, 3, 5, and 10 min after intubation than
the dexamethasone group and gabapentin
group (P ⬍ 0.05); when compared with
the control group, these values were sub-
stantially lower (P ⬍ 0.001). The gabap-
entin group and dexamethasone group
did not differ statistically (P ⬎ 0.05),
whereas values were significantly lower
in the gabapentin group and dexametha-
sone group compared with the control
group (P ⬍ 0.05).
Figure 3. Postoperative visual analog score
(VAS) changes. Postoperative visual analog
scores were to be statistically significantly lower
in the gabapentin–dexamethasone group at 30
min 1, 2, 4, 6, and 12 h than in the gabapentin
group and dexamethasone group (P ⬍ 0.05),
and substantially lower when compared with
the control group (P ⬍ 0.001). These values
were also each found lower in gabapentin
group and dexamethasone group than in the
control group (P ⬍ 0.05). The gabapentin group
and dexamethasone group did not differ
significantly.
Table 2. Adverse Effects
Postoperative nausea–vomiting
Treatment Dry mouth Vomiting Nausea Total Headache Pruritis
Control (n ⫽ 20) 4 (20) 14 (70) 1 (5) 15 (75) 6 (30) 2 (10)
Gabapentin (n ⫽ 20) 3 (15) 7 (35) 1 (5) 8 (40)* 7 (35) 0 (0)
Dexamethasone (n ⫽ 20) 3 (15) 7 (35) 0 (0) 7 (35)* 3 (15) 1 (5)
Combination (n ⫽ 20) 1 (5) 1 (5) 0 (0) 1 (5)†‡ 4 (20) 1 (5)
Values inside parentheses indicate percentages.
*P ⬍ 0.05, when group C compared with group G and group D.
†P ⬍ 0.001, when group GD compared with group C.
‡P ⬍ 0.05, when group gabapentin and dexamethasone compared with group gabapentin and group dexamethasone.
group GD compared with all other groups (P ⬍ 0.001). tracheal intubation response, better postoperative anal-
Nausea and vomiting in group G and group D were gesia, and less postoperative nausea and vomiting than
similar, but less than, in group C (P ⬍ 0.05). There the individual administration of each drug.
were no differences among the groups in other side In animal models of nociception, gabapentin reduces
effects (Table 2). hypersensitivity associated with nerve injury, inflamma-
tion, and pain after surgery (22,23). Mechanical hyperal-
DISCUSSION gesia surrounding the wound in postoperative patients
The above-mentioned results indicate that gabapentin and experimental, heat-induced secondary hyperalgesia
and dexamethasone, administered together an hour be- share a common mechanism; namely, central neuronal
fore varicocele operation, result in less laryngeal and sensitization that may contribute to some aspects of
1140 Gabapentin and Dexamethasone ANESTHESIA & ANALGESIApostoperative pain. Antihyperalgesic drugs such as min. Fassouloki et al. (36) demonstrated that 1600 mg gabapentin may have a role in postoperative pain, and gabapentin attenuated the pressor response, but not their combination with other antinociceptive drugs the tachycardia, associated with laryngoscopy and may produce synergistic analgesic effects (6). Gabap- tracheal intubation. In our literature search, we failed entin’s antihyperalgesic effects result from an action at to find any study evaluating the effect of dexamethasone the ␣2␦1 subunits of voltage-dependent Ca2⫹ channels or gabapentin– dexamethasone on intubation. The above (24), which are up-regulated in the dorsal root ganglia results indicate that a gabapentin– dexamethasone com- and spinal cord after peripheral injury (25). Gabapen- bination provides significant decreases in MAP and HR tin may also produce antihyperalgesia by decreasing values in the first 10 min after induction than the single glutaminergic transmission in the spinal cord (26). In drug gabapentin or dexamethasone. All three treatments addition, a study of gabapentin’s effect in rat hip- attenuated the pressor response. This reduction was pocampus and neocortex suggested that it selectively significantly greater with the combination than with inhibits Ca2⫹ influx by inhibiting voltage-operated either drug alone. Although observed changes in MAP Ca2⫹ channels in a subset of excitatory and inhibitory and HR at intubation were statistically significant, they presynaptic terminals, thereby attenuating synaptic were modest and clinically acceptable. There were no transmission (27). Although the molecular targets of incidences of bradycardia, tachycardia, arrhythmias, ST gabapentin remain unknown, the inhibition of Ca2⫹ segment, or other echocardiographic changes observed efflux from muscle cells, with a consequent inhibition during the study. of smooth muscle relaxation, might explain the effective- Postoperative nausea and vomiting are a multifac- ness of gabapentin in the relaxation of laryngoscopy. torial problem, and several anesthetic and nonanes- The analgesic effects of glucocorticoids are provided thetic factors must be controlled to obtain meaningful through inhibition of the phospholipase enzyme and results. Gabapentin has been reported to be effective subsequent blockage of both the cyclooxygenase and the in the treatment of emesis in patients receiving cyto- lipoxygenase pathways in the inflammatory chain reac- toxic drugs (37). The precise mechanism of gabapentin tion (18), as well as suppression of tissue levels of in the prevention of nausea and vomiting induced by bradykinin (28) and release of neuropeptides from nerve cytotoxic drugs is not known, but mitigation of tachy- endings (29). Both of these effects may enhance nocicep- kinin neurotransmitter activity has been postulated to tion in inflamed tissues and the surgical wound. In one be useful (38). There is evidence that tachykinins review (19) regarding the effects of perioperative single- activity is part of the pathogenesis of chemotherapy- dose glucocorticoid administration, randomized trials induced emesis in ferrets, and that a selective from several minor and major surgical procedures tachykinins-receptor antagonist improves nausea and were analyzed. The authors concluded that glucocor- emesis (39,40). ticoid administration in major abdominal surgery The mechanism by which glucocorticoids alleviate probably has no or limited analgesic effects, except nausea and vomiting is not fully understood, but the perhaps in minor surgical procedures such as hemor- effects are probably centrally mediated via inhibition of rhoidectomy, hallux valgus correction, thyroidectomy, prostaglandin synthesis or inhibition of the release of and dental surgery (19), and now also in our model. endogenous opioids (20). In a metaanalysis of 17 ran- Glucocorticoids suppress agonist-induced release of domized controlled trials, a single dose of dexametha- intracellular calcium in airway smooth muscle cells sone in combination with 5-HT3 receptor antagonists such as bradykinin (30). The suppressive effect of significantly reduced postoperative nausea and vomit- glucocorticoids on agonist-stimulated increases in in- ing when compared with placebo, but the optimal dose tracellular calcium concentration may involve down of this combination still needs to be identified (20). In our regulation of adenosine receptors, reduced adenosine study, all three treatments reduced nausea and vomiting receptor affinities, or reduction in adenylate cyclase postoperative periods. This reduction was significantly activity (31,32). This smooth muscle relaxation might greater with the combination than with either single also explain the effectiveness of dexamethasone in the drug. This study also demonstrated a decrease in the suppression of laryngoscopy. amount of remifentanil consumption in gabapentin– Surgical procedures, endotracheal intubation, and dexamethasone group more than in group gabapentin anesthesia are stressful to the patient and may induce or dexamethasone. This reduction in nausea and potentially harmful reactions, such as increases in HR vomiting may result from the lower opioid doses in and MAP (33). There is a clear relationship between group gabapentin– dexamethasone. surgical events producing intense sympathetic stimu- This trial provides empirical evidence to support lation and perioperative myocardial ischemic episodes the clinical utility of a gabapentin– dexamethasone and postoperative myocardial infarction (34). combination for postoperative pain. Future trials Memis et al. (35) found that 800 mg gabapentin, should further evaluate other analgesic combinations given 1 h before surgery blunted the MAP and HR to enhance symptomatic improvement and functional increase due to endotracheal intubation in the first 10 recovery after surgery. Vol. 105, No. 4, October 2007 © 2007 International Anesthesia Research Society 1141
REFERENCES 22. Cheong JK, Pan HL, Eisenach JC. Antiallodynic effect of intra-
thecal gabapentin and its interaction with clonidine in a rat
1. Rosner H, Rubin L, Kestenbaum A. Gabapentin adjunctive model of postoperative pain. Anesthesiology 2000;92:1126 –31
therapy in neuropathic pain states. Clin J Pain 1996;12:56 – 8 23. Field MJ, Holloman EF, McCleary S, Hughes J, Singh L. Evalu-
2. Backonja M, Beydoun A, Edwards KR, Schwartz SL, Fonseca V, ation of gabapentin and S-(⫹)-3-isobutylgaba in a rat model of
Hes M, LaMoreaux L, Garofalo E. Gabapentin for the symptom- postoperative pain. J Pharmacol Exp Ther 1997;282:1242– 6
atic treatment of painful neuropathy in patients with diabetes 24. Gee NS, Brown JP, Dissanayake VU, Offord J, Thurlow R,
mellitus: a randomized controlled trial. JAMA 1998;280:1831– 6 Woodruff GN. The novel anticonvulsant drug, gabapentin,
3. Rowbotham M, Harden N, Stacey B, Bernstein P, Magnus-Miller binds to the alpha 2 delta subunit of a calcium channel. J Biol
L. Gabapentin for the treatment of postherpetic neuralgia: a Chem 1996;271:5768 –76
randomized controlled trial. JAMA 1998;280:1837– 42
25. Luo ZD, Chaplan SR, Higuera ES, Sorkin LS, Stauderman KA,
4. Mellick GA, Mellick LB. Reflex sympathetic dystrophy treated
Williams ME, Yaksh TL. Upregulation of dorsal root ganglion
with gabapentin. Arch Phys Med Rehabil 1997;78:98 –105
(alpha) 2 (delta) calcium channel subunit and its correlation
5. Mao J, Chen LL. Gabapentin in pain management. Anesth
with allodynia in spinal nerve injured rats. J Neurosci 2001;
Analg 2000;91:680 –7
6. Alden KJ, Garcia J. Differential effect of gabapentin on neuronal 21:1868 –75
and muscle calcium currents. J Pharmacol Exp Ther 2001;297: 26. Maneuf Y, Mcknight A. Block by gabapentin of the facilitation
727–35 of glutamate release from rat trigeminal nucleus following
7. Martin DJ, McClelland D, Herd MB, Sutton KG, Hall MD, Lee K, activation of protein kinase C or adenylyl cyclase. Br J Pharma-
Pinnock RD, Scott RH. Gabapentin-mediated inhibition of col 2001;134:237– 40
voltage-activated Ca2⫹ channel currents in cultured sensory 27. van Hooft JA, Dougherty JJ, Endeman D, Nichols RA, Wadman
neurones is dependent on culture conditions and channel WJ. Gabapentin inhibits presynaptic Ca(2⫹) influx and synaptic
subunit expression. Neuropharmacology 2002;42:353– 66 transmission in rat hippocampus and neocortex. Eur J Pharma-
8. Sarantopoulos C, McCallum B, Kwok WM, Hogan Q. Gabapen- col 2002;449:221– 8
tin decreases membrane calcium currents in injured as well as in 28. Hargreaves KM, Costello A. Glucocorticoids suppress levels of
control mammalian primary afferent neurons. Reg Anesth Pain immunoreactive bradykinin in inflamed tissue as evaluated by
Med 2002;27:47–57 microdialysis probes. Clin Pharmacol Ther 1990;48:168 –78
9. Shimoyama M, Shimoyama N, Hori Y. Gabapentin affects 29. Hong D, Byers MR, Oswald RJ. Dexamethasone treatment
glutamatergic excitatory neurotransmission in the rat dorsal reduces sensory neuropeptides and nerve sprouting reactions in
horn. Pain 2000;85:405–14 injured teeth. Pain 1993;55:171– 81
10. Patel MK, Gonzalez MI, Bramwell S, Pinnock RD, Lee K. 30. Tanaka H, Watanabe K, Tamura N, Yoshida M. Arachidonic
Gabapentin inhibits excitatory synaptic transmission in the acid metabolites and glucocorticoid regulatory mechanism in
hyperalgesic spinal cord. Br J Pharmacol 2000;130:1731– 4 cultured porcine tracheal smooth muscle cells. Lung 1995;
11. Shimoyama M, Shimoyama N, Inturrisi CE, Elliott KJ. Gabap- 173:347– 61
entin enhances the antinociceptive effects of spinal morphine in 31. Davies AO, Lefkowitz RJ. Regulation of -adrenergic receptors
the rat tail-flick test. Pain 1997;72:375– 82 by steroid hormones. Annu Rev Physiol 1984;46:119 –30
12. Eckhardt K, Ammon S, Hofmann U, Riebe A, Gugeler N, Mikus 32. Gerwins P, Freedholm BB. Glucocorticoid receptor activation
G. Gabapentin enhances the analgesic effect of morphine in leads to up-regulation of adenosine A1 receptors and down-
healthy volunteers. Anesth Analg 2000;91:185–91 regulation of adenosine A2 receptors in DDT1 MF-2 smooth
13. Caraceni A, Zecca E, Martini C, De Conno F. Gabapentin as an muscle cells. Mol Pharmacol 1991;40:149 –55
adjunctant to opioid analgesia for neuropathic cancer pain. 33. Derbyshire DR, Smith G. Sympatoadrenal responses to anesthe-
J Pain Symptom Manage 1999;17:441–5 sia and surgery. Br J Anaesth 1984;56:725–39
14. Turan A, Karamanlioglu B, Memis D, Hamamcioglu MK, 34. Slogoff S, Keats AS. Does perioperative myocardial ischemia
Tukenmez B, Pamukcu Z, Kurt I. Analgesic effect of gabap- lead to postoperative myocardial infarction. Anesthesiology
entin after spinal surgery. Anesthesiology 2004;100:935– 8 1985;62:107–14
15. Turan A, Karamanlioglu B, Memis D, Usar P, Pamukcu Z, Ture 35. Memis D, Turan A, Karamanlioglu B, Seker S, Ture M. Gabap-
M. The analgesic effects of gabapentin after total abdominal
entin reduces cardiovascular responses to laryngoscopy and
hysterectomy. Anesth Analg 2004;98:1370 –3
tracheal intubation. Eur J Anaesthesiol 2006;23:686 –90
16. Turan A, Memis D, Karamanlioglu B, Yagiz R, Pamukcu Z,
36. Fassoulaki A, Melemeni A, Paraskeva A, Petropoulos G. Gaba-
Yavuz E. Analgesic effects of gabapentin in ear-nose-throat
pentin attenuates the pressor response to direct laryngoscopy
surgery. Anesth Analg 2004;99:375– 8
17. Hurley RW, Cohen SP, Williams KA, Rowlingson AJ, Wu CL. and tracheal intubation. Br J Anaesth 2006;96:769 –73
The analgesic effects of perioperative gabapentin on postopera- 37. Guttuso T Jr, Roscoe J, Griggs J. Effect of gabapentin on nausea
tive pain: A Meta-Analysis. Reg Anesth Pain Med 2006;31: induced by chemotherapy in patients with breast cancer. Lancet
237– 47 2003;361:1703–5
18. Sapolsky RM, Romero LM, Munck AU. How do glucocorticoids 38. Guttuso T Jr, Kurlan R, McDermott MP, Kieburtz K. Gabapen-
influence stress responses. Integrating permissive, suppressive, tin’s effects on hot flushes in postmenopausal women: a ran-
stimulatory, and preparative actions. Endocr Rev 2000;21:55– 89 domized controlled trial. Obstet Gynecol 2003;101:337– 45
19. Holte K, Kehlet H. Perioperative single dose glucocorticoid 39. Navari RM, Reinhardt RR, Gralla RJ, Kris MG, Hesketh PJ,
administration: pathophysiological effects and clinical implica- Khojasteh A, Kindler H, Grote TH, Pendergrass K, Grunberg
tions. J Am Coll Surg 2002;195:694 –712 SM, Carides AD, Gertz BJ. Reduction of cisplastin-induced
20. Henzi I, Walder B, Tramer MR. Dexamethasone for the preven- emesis by selective neurokinin-1-receptor antagonist. L-754,030
tion of postoperative nausea and vomiting: a quantitative Antiemetic trials group. N Engl J Med 1999;340:190 –5
systematic review. Anesth Analg 2000;90:186 –94 40. Pandey CK, Priye S, Ambesh SP, Singh S, Singh U, Singh PK.
21. Fujii Y, Saitoh Y, Tanaka H, Toyooka H. Granisetron/ Prophylactic gabapentin for prevention of postoperative nausea
dexamethasone combination for the prevention of postoperative and vomiting in patients undergoing laparoscopic cholecystec-
nausea and vomiting after laparoscopic cholecystectomy. Eur J tomy: A randomized, double-blind, placebo-controlled study.
Anaesthesiol 2000;17:64 –7 J Postgrad Med 2006;52:97–100
1142 Gabapentin and Dexamethasone ANESTHESIA & ANALGESIAYou can also read