The skin in psoriasis: assessment and challenges - Clinical ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The skin in psoriasis: assessment and challenges
V. Oji, T.A. Luger
Department of Dermatology, ABSTRACT tologist, who first diagnoses the skin
University Hospital Münster, Germany. The coexistence of psoriasis arthritis disease. Hence, both specialties play an
Vinzenz Oji, MD (PsA) and psoriasis vulgaris in about important role in early disease detec-
Thomas A. Luger, MD, Prof. 20% of patients with psoriasis leads to tion and determining the course regard-
Please address correspondence to: a need for rheumatologic-dermatologic ing further treatments of PsA as well as
Vinzenz Oji, MD, team work. We summarise the role of psoriasis.
Department of Dermatology, dermatologists in assessment of the skin This paper refers to the tasks of der-
University Hospital Münster
Von-Esmarch Straβe 58,
in psoriasis. matologists in assessment of the skin
48149 Münster, Germany. Chronic plaque psoriasis must be dif- in a patient with psoriasis and/or PsA.
E-mail: ojiv@uni-muenster.de ferentiated from other subtypes such as Clinically challenging aspects will be
Received and accepted on September 29, generalised pustular psoriasis (GPP) addressed to strengthen the collabora-
2015. or palmoplantar pustulosis (PPP). tion of dermatology, rheumatology, as
Clin Exp Rheumatol 2015; 33 (Suppl. 93): Therapeutic management is based on well as general medicine, to care for
S14-S19. the evaluation of the disease severity. patients with psoriasis. First of all the
© Copyright Clinical and Quantitative scoring of skin severity diagnosis of psoriasis must be identi-
Experimental Rheumatology 2015. includes calculation of the Psoriasis fied. The differential diagnoses includes
Area and Severity Index (PASI), body eczema or mycosis fungoides, and the
Key words: plaque psoriasis, surface area (BSA) as well as the Der- distinct type of skin psoriasis should
generalised pustular psoriasis, matology Life Quality Index (DLQI). be defined, i.e. psoriasis vulgaris (PV)
palmoplantar pustulosis, PASI, These scoring systems do not replace manifesting as chronic plaque psoriasis
DLQI, BSA, PGA, comorbidity the traditional dermatologic medical has to be distinguished from generalised
history and physical examination of the pustular psoriasis (GPP), palmoplantar
patient. The skin should be examined pustulosis (PPP), or acrodermatitis con-
for additional skin diseases; moreover, tinua suppurativa (6, 7). We focus on
patients should be monitored for co- PV and summarise the specific clinical
morbidity, most importantly PsA and tools which are commonly used for the
cardiovascular comorbidity. assessment of disease severity, and de-
scribe some challenges that may occur.
Introduction Assessment of the skin of patients with
Psoriasis is a chronic inflammatory PV or PsA is a component of a com-
skin disease affecting about 2% of the plete dermatological examination:
Caucasian population (1). About 20% thoroughly performed it takes into ac-
of the patients have psoriatic arthritis count important individual aspects of
(PsA) (2, 3). Many patients with pso- the skin status such as the number of
riasis are not aware of their PsA; and melanocytic nevi or the tendency to
the prevalence of undiagnosed PsA is skin dryness and atopy (Table I). Im-
still high as has been shown in a recent portantly, patients have to be moni-
systematic meta-analysis. Accordingly, tored for skin tumours or precancerous
up to 15.5% of patients with psoriasis lesions such as basal cell carcinoma,
had undiagnosed PsA (4). Dermatolo- squamous cell carcinoma or actinic
gists usually are the doctors consulted keratoses, respectively, taking into ac-
in cases of new-onset psoriasis (5). In count the often increased cumulative
collaboration with rheumatologists risk of carcinogenic sun exposure, UV
they should screen their patients with light treatment and/or immunosuppres-
psoriasis for PsA, as PsA is a progres- sive therapies (8).
sive disease, and a subgroup of patients
develops progressive damage and loss Key features of skin psoriasis
of function in the first few years of the Psoriasis vulgaris (PV) is diagnosed
disease (4). On the other hand, in about by the characteristic psoriatic plaques
6 to 18% PsA may precede skin lesions consisting from salmon red sharply
Competing interests: none declared. (3, 4). Then it usually is the rheuma- bordered macules covered with silvery
S-14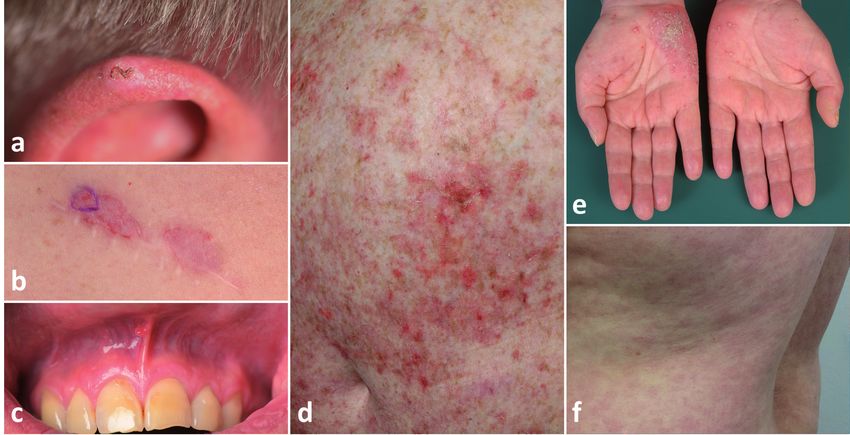
Dermatological assessment of psoriasis / V. Oji & T.A. Luger
Table I. Dermatological assessment of patients with psoriasis. teal cleft, groins, and retro-auricular ar-
eas have not been examined. Involve-
Definition of psoriasis type/s Concomitant skin disorders or history of these
Plaque psoriasis (Psoriasis vulgaris) Infections ment of the lips is possible; involve-
Palmoplantar pustulosis (PPP) Tumours ment of the mucous membrane would
Acrodermatitis continua suppurativa Eczemas be extremely unusual (1, 9). However,
Generalised pustular psoriasis (GPP) Lichen planus considering potential differential diag-
± Psoriasis arthritis (PsA) Vitiligo
Predilection sites of the skin Alopecia areata noses such as lichen planus or adverse
Scalp (retroauricular) Urticaria reactions of systemic therapies (Fig. 2)
Extensor sites Dermatitis herpetiformis Duhring inspection of the mouth should be per-
Nails Cutaneous lupus erythematodes
formed in all patients with psoriasis.
Flexural / genitals (gluteal cleft) Scars (after tumour excision)
General aspects of the skin Comorbidity / cardiovascular risk factors Nail psoriasis is extensively described
Pigmentation type Body Mass Index (BMI) elsewhere in this supplement. In short,
Number of nevi Hyperlipidaemia 15–50% of patients with psoriasis have
Skin dryness Hypertension
Mucous membrane (tonsils) Other diseases or history of these*
nail changes. This figure increases to
Teeth Rheumatologic / orthopaedic 85% in patients with psoriatic arthritis
Conjunctivae Gastrointestinal / hepatic / renal (10). Nail pitting, oil spots and onych-
Neurological / psychiatric olysis are highly diagnostic (11).
Cancer / haemolymphatic
Allergies
Distinct subtypes of psoriasis
*incl. screening for psychological distress, fatigue, smoking and alcohol consumption. Plaque psoriasis should be differenti-
ated from other psoriasis forms, which
scales. Knees, elbows, scalp and um- It presents with erythematous sharply are clinically distinct and have a differ-
bilicus are commonly affected (Fig. 1). demarcated areas, typically without sil- ent genetic background (1, 9, 12). GPP
Importantly, the diagnosis of inverse very scaling. Patients may not address is now regarded an autoinflammatory
psoriasis, in which only the flexural symptoms of inverse psoriasis. Hence, skin diseases (DIRA/DITRA, etc.) (13).
folds are affected, should not be missed. psoriasis cannot be excluded if the glu- It has a different, more rapid disease
Fig. 1. Clinical examples of distinct forms of psoriasis and special localisations of psoriasis vulgaris: severe chronic plaque psoriasis (PASI 21.6) (a), pal-
moplantar pustulosis in a female patient with Sapho syndrome (b), generalised pustular psoriasis in a patient with IL36 receptor mutations (c), acrodermatitis
continua suppurativa in a patient also suffering from psoriasis vulgaris (d), psoriasis capitis as most common location of psoriasis vulgaris (e), severe nail
psoriasis (f), inverse psoriasis first misdiagnosed as mycosis (g), isolated palmar psoriasis vulgaris (h), and psoriasis of the external ear canal and scalp (i).
S-15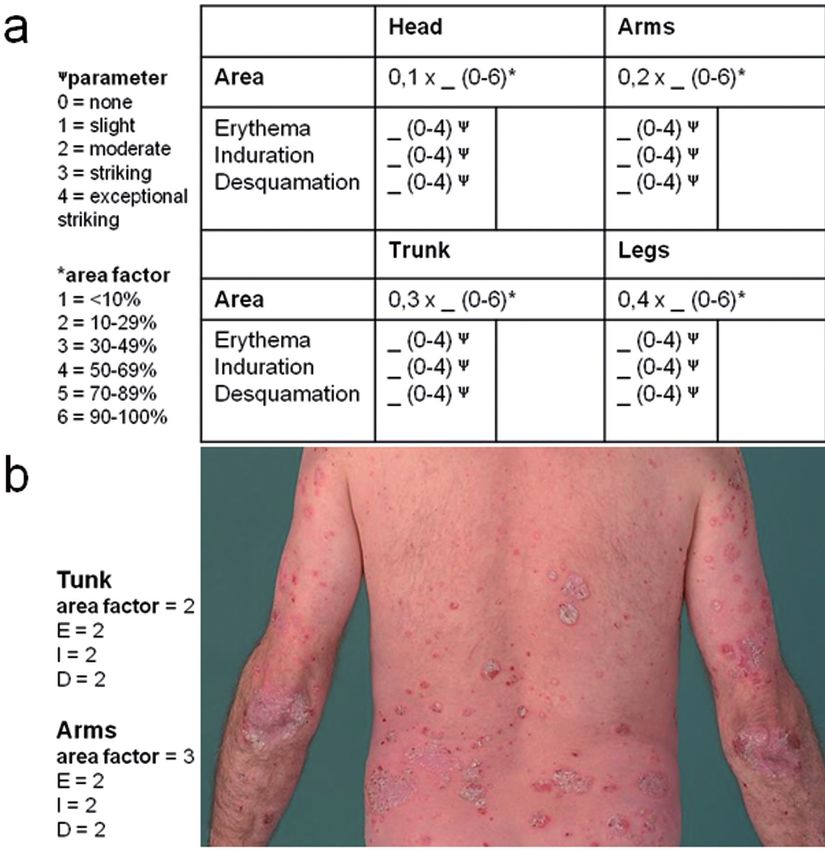
Dermatological assessment of psoriasis / V. Oji & T.A. Luger
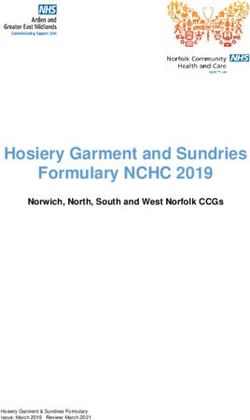
Fig. 2. Clinical examples of concomitant skin diseases in patients with psoriasis: squamous cell carcinoma in a patient, who regularly used sun bathing as
self-therapy (a), basal cell carcinoma origination from a scare in a patient suffering from psoriasis arthritis treated with methotrexate (b), mild lichen planus of
the gingiva in a patient under biologics (c), multiple actinic keratoses in a patient with plaque psoriasis, who had received a high cumulative dosage of UVB
light therapy (d), palmar pustulosis (e) and mild exanthema (f) in a female with nail psoriasis and psoriasis arthritis, who had received a TNF-alpha blocker.
course characterised by flares, continu- defined by pustular eruptions, initially Plaque psoriasis:
ous development of pustules, often with affecting the tip of the fingers and nails, assessment of disease severity
fever (1, 6, 13). PPP is a very chronic often affecting the bony structures of In psoriasis initiation of therapy and
disease of the feet and/or hands char- the distal phalanxes (1, 6) (Fig. 1). Co- monitoring of the therapeutic effective-
acterised by persisting sterile pustules existence of different types of psoriasis ness are based largely on evaluation of
with or without hyperkeratotic derma- may occur. PsA can be associated with the disease severity. Therefore, scoring
titis (1, 14). each of them, but frequency and type of skin severity is a necessity in psoria-
Several reports document that biologic of the arthritic component might differ, sis care. More than 44 different scoring
therapies with TNF-antagonists may e.g. PPP may be more often associated systems were used in 171 randomised
cause de novo occurrence or exacer- with SAPHO syndromic sternoclavicu- clinical trials of psoriasis therapies
bation of this form of psoriasis (15). lar and sternomanubrial tenderness and between 1997 and 2000 (17). Com-
Acrodermatitis continua suppurativa is pain (16). mon tools to score psoriasis include
determination of the area involved
Table II. Examples of relevant clinical severity scores for plaque psoriasis and their items. in relation to the whole body surface
(Body Surface Area, BSA) (18, 19),
Erythema Desqua- Infiltration BSA Psychosocial History of Calculated the Physician Global Assessment (19)
mation impact the illness by
and
and the Psoriasis Area and Severity In-
treatment dex (PASI), which was constructed by
Frederiksson and Pettersson (19, 20) in
PASI + + + + - - Physician order to assess the severity of PV. The
BSA - - - + - - Physician PASI score includes a number of well-
PGA + + + - - - Physician
defined dermatological parameters,
LS ⁄ PGA + + + + Physician
e.g. skin redness and infiltration cor-
SPI + + + + + + Physician
responding to the inflammatory com-
saSPI + + + + + + Patient
ponent of the disease, and allows for
proSPI + + + + + + Physician
scoring of skin area involvement (see
SAPASI + + + + - - Patient
below).
PASI: Psoriasis Area and Severity Index; BSA: Body Surface Area; PGA: Physicians Global Assessment; The Salford Psoriasis Index (SPI) is
LS: Laatice System Physician’s Global Assessment; SPI: Salford Psoriasis Index Simplified Psoriasis derived from combining a converted
Index; saSPI: self-assessment Simplified Psoriasis Index; proSPI: professional Simplified Psoriasis In-
dex; SAPASI: Self Administered Psoriasis Area Severity Index. [adapted from Puzenat et al. 2012 (24)].
figure of the PASI, a second score in-
dicating psychosocial disability, and a
S-16Dermatological assessment of psoriasis / V. Oji & T.A. Luger
third score based on historical informa-
tion (21). Chularojanamontri et al. re-
cently published a modified version of
the SPI renamed to Simplified Psoriasis
Index (22). However, no single instru-
ment captures all dimensions of psoria-
sis severity (23). Puzena et al. selected
six relevant clinical severity scores
(PASI, BSA, PGA, LS-PGA, SPI and
SAPASI) (Table II) and compared their
methodological validations and quality
(24). They conclude that the PASI is the
most thoroughly validated score and
can be recommended for quantitative
evaluation of clinical severity of pso-
riasis. This conclusion is in agreement
with the recommendations of current
consensus guidelines for the manage-
ment of psoriasis (8, 25).
The Psoriasis Area and Severity
Index (PASI):
everyday clinical practice
For calculation of the PASI four main
body areas are assessed: the head (h),
the trunk (t), the upper extremities (u)
and the lower extremities (l), corre-
sponding to 10, 20, 30 and 40% of the
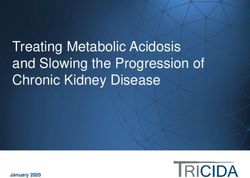
total body area, respectively (Fig. 3).
The area of psoriatic involvement of Fig. 3. Assessment of disease severity in psoriasis vulgaris: PASI scheme and calculation; the neck
these four main areas (Ah, At, Au and is assessed together with the heat; buttocks are assessed with the legs (a). Example of a patient with
plaque psoriasis (arms and trunk); the total sum of the PASI of this patient was 15.3 (b).
Al) is given a numerical value: 0 = no
involvement; 1 =Dermatological assessment of psoriasis / V. Oji & T.A. Luger
Dermatologic evaluation includes Table III. Internet resources for the assessment and management of skin psoriasis*.
assessment of health-related quality PASI
of life and comorbidity http://www.pasitraining.com/calculator/step_1.php
The assessment of psoriasis severity http://pasi.corti.li
should take into account its burden on http://www.dermnetnz.org/scaly/pasi.html
DLQI
health-related quality of life (HR-QoL) http://www.cardiff.ac.uk/dermatology/quality-of-life
(23). As mentioned above, the PASI is http://www.pasitraining.com/dlqi
insufficient to assess functional disabil- Dermatological guidelines for the management of patients with psoriasis
ity secondary to specific localisations of http://www.ncbi.nlm.nih.gov/pubmedhealth
http://www.awmf.org/leitlinien
skin lesions, e.g. on the face, hands or
nails. Moreover, patients with psoriasis *last accessed 6-9-2015.
often suffer from pruritus, cutaneous
pain, burning sensations, bleeding, and/ tologic diseases, neoplasm or allergy manifestations may have a substantial
or social-life impairment (23, 25). In (Table I). From epidemiologic studies impact on the dynamic or static Phy-
clinical practice evaluation of all these it has been well established that severe sician Global Assessment (PGA) (19),
symptoms might be perceived as cum- psoriasis is associated significantly which can alter the classification of
bersome; however, validated scales as- with a moderate increase of risk for dia- mild disease to moderate-to-severe dis-
sessing the burden of plaque psoriasis betes and obesity (5, 33). A recent pop- ease (23):
on HR-QoL are the Dermatology Life ulation-based Swedish register study • involvement of visible areas
Quality Index (DLQI) (28), the Short- showed that mild and severe psoriasis • involvement of major parts of the
Form 36 (SF-36) and the Skindex 29 are associated with increased mortality scalp
and Skindex 17 (23) that may be com- rates as patients with severe psoriasis • involvement of genitals
pleted by the patients in 3–15 minutes. die on average 2.6 years younger than • involvement of palms and/or soles
The DLQI consists of 10 questions con- age-, sex-, and residency-matched con- • onycholysis or onychodystrophy of
cerning symptoms and feelings, daily trol subjects. The increases in all-cause at least two fingernails
activities, leisure, work, and school, mortality observed were largely attrib- • pruritus leading to scratching
personal relationships and treatment. uted acutely to increased cardiovascu- • presence of single recalcitrant
All questions relate “to the last week”, lar mortality (34). For this reason, new plaques
and the score ranges from 0 (no impair- dermatological guidelines do not only
ment of life quality) to 30 (maximum refer to the skin, but also recommend to Definition of treatment effectiveness
impairment). The tool has been trans- determine the Body Mass Index (BMI) The reduction in PASI of ≥75% (Δ
lated into at least 21 different languag- (upper limit: 30 kg⁄m2) and/or waist cir- PASI ≥75) has been considered to in-
es. There is a children’s version of the cumference (upper limit: 94 cm in men, dicate treatment success after an antip-
DLQI (29), the Children’s Dermatology 80 cm in women) in patients with mod- soriatic treatment has been initiated (8,
Life Quality Index (CDLQI), and a text erate to severe psoriasis (23). 25). Clinical studies on the effectiveness
and cartoon version of this has been de- of systemic therapy in plaque psoriasis
scribed (30) (Table III). Combination of skin assessment may note that a certain proportion of
A definition of the different scores of tools and therapy algorithm patients experienced a 75% reduction
the DLQI and their impact on patients’ A recent consensus program for the in their PASI scores over a 3-months
life allows a reliable grading of the im- treatment of plaque psoriasis defined treatment period and report this as a
pact on quality of life (31). By using a number of important items related to percentage of people achieving “PASI
this definition in psoriasis, a DLQI 10 and DLQI >10 used in combination with the dynamic
chiatric, orthopaedic or other rheuma- The presence of the following disease PGA of the nails (11).
S-18Dermatological assessment of psoriasis / V. Oji & T.A. Luger
Conclusion ysis. J Am Acad Dermatol 2015; 73: 242-8. 21. KIRBY B, FORTUNE DG, BHUSHAN M, CHAL-
5. RADTKE MA, MROWIETZ U, FEUERHAHN MERS RJ, GRIFFITHS CE: The Salford Pso-
Assessment of the skin in patients with
J et al.: Early detection of comorbidity in riasis Index: an holistic measure of psoriasis
psoriasis is based on quantitative scor- psoriasis: recommendations of the National severity. Br J Dermatol 2000; 142: 728-32.
ing tools. The Psoriasis Area and Sever- Conference on Healthcare in Psoriasis. 22. CHULAROJANAMONTRI L, GRIFFITHS CE,
ity Index (PASI) is the best validated J Dtsch Dermatol Ges 2015; 13: 674-90. CHALMERS RJ: The Simplified Psoriasis In-
6. RAYCHAUDHURI SK, MAVERAKIS E, RAY- dex (SPI): a practical tool for assessing pso-
score for defining disease severity in CHAUDHURI SP: Diagnosis and classification riasis. J Invest Dermatol 2013; 133: 1956-62.
psoriasis vulgaris (23). New treatment of psoriasis. Autoimmun Rev 2014; 13: 490-5. 23. PAUL C, GOURRAUD PA, BRONSARD V et
goals are defined as Δ PASI 90 (90% 7. MENGESHA YM, BENNETT ML: Pustular skin al.: Evidence-based recommendations to as-
clearing of skin lesion) or Δ PASI 100 disorders: diagnosis and treatment. Am J Clin sess psoriasis severity: systematic literature
Dermatol 2002; 3: 389-400. review and expert opinion of a panel of der-
(disease free skin). According to the 8. NAST A, BOEHNCKE WH, MROWIETZ U et matologists. J Eur Acad Dermatol Venereol
current dermatological guidelines, cal- al.: German S3-guidelines on the treatment 2010; 24 (Suppl. 2): 2-9.
culation of PASI should be combined of psoriasis vulgaris (short version). Arch 24. PUZENAT E, BRONSARD V, PREY S et al.:
with the Body Surface Area (BSA), as Dermatol Res 2012; 304: 87-113. What are the best outcome measures for as-
9. GRIFFITHS CE, BARKER JN: Pathogenesis sessing psoriasis severity? A systematic re-
well as the Dermatology Life Quality and clinical features of psoriasis. Lancet view of the literature. J Eur Acad Dermatol
Index (DLQI) (25). The static or dy- 2007; 370: 263-71. Venereol 2010; 24 (Suppl. 2): 10-16.
namic Physician’s Global Assessment 10. BARAN R, SIGURGEIRSSON B: Psoriatic nail 25. MROWIETZ U, KRAGBALLE K, REICH K et
(PGA) should be estimated and may be disease, a predictor of psoriatic arthritis. Br J al.: Definition of treatment goals for moder-
Dermatol 2014; 171: 935-6. ate to severe psoriasis: a European consen-
highly important if special disease man- 11. KLAASSEN KM, van de KERKHOF PC, BAS- sus. Arch Dermatol Res 2011; 303: 1-10.
ifestations exist, e.g. nails are involved TIAENS MT et al.: Scoring nail psoriasis. 26. AUGUSTIN M, BLOME C, COSTANZO A et al.:
(11). However, these scoring systems J Am Acad Dermatol 2014; 70: 1061-6. Nail Assessment in Psoriasis and Psoriatic
12. TSOI LC, SPAIN SL, ELLINGHAUS E et al.: Arthritis (NAPPA): development and valida-
do not replace the dermatologic clinical
Enhanced meta-analysis and replication tion of a tool for assessment of nail psoriasis
examination and medical history of the studies identify five new psoriasis suscepti- outcomes. Br J Dermatol 2014; 170: 591-8.
patient, i.e. assessment of PASI, DLQI bility loci. Nat Commun 2015 5; 6: 7001. 27. RICH P, SCHER RK: Nail Psoriasis Severity
or PGA alone is not sufficient. The skin 13. ONOUFRIADIS A, SIMPSON MA, PINK AE et Index: a useful tool for evaluation of nail
al.: Mutations in IL36RN/IL1F5 are associ- psoriasis. J Am Acad Dermatol 2003; 49:
should be examined for additional skin ated with the severe episodic inflammatory 206-12.
diseases, which may occur in patients skin disease known as generalized pustular 28. FINLAY AY, KHAN GK: Dermatology Life
with psoriasis. Moreover, patients psoriasis. Am J Hum Genet 2011; 89: 432-37. Quality Index (DLQI)--a simple practical
should be monitored for comorbidity 14. MÖSSNER R, FRAMBACH Y, WILSMANN- measure for routine clinical use. Clin Exp
THEIS D et al.: Palmoplantar pustular pso- Dermatol 1994; 19: 210-6.
beyond the skin, most importantly PsA riasis is associated with missense variants 29. LEWIS-JONES MS, FINLAY AY: The Chil-
(4) and cardiovascular comorbidity (5). in CARD14, but not with loss-of-function dren’s Dermatology Life Quality Index
Since the coexistence of PsA and skin mutations in IL36RN in European Patients. (CDLQI): initial validation and practical use.
psoriasis is about 20–30%, an early di- J Invest Dermatol 2015; 135: 2538-41. Br J Dermatol 1995; 132: 942-9.
15. IBIS N, HOCAOGLU S, CEBICCI MA, SUT- 30. LEWIS V, FINLAY AY: 10 years experience of
agnosis of a progressive PsA is needed. BEYAZ ST, CALIS HT: Palmoplantar pustular the Dermatology Life Quality Index (DLQI). J
Management of the patient with pso- psoriasis induced by adalimumab: a case re- Investig Dermatol Symp Proc 2004; 9: 169-80.
riasis clearly is the crystallising point port and literature review. Immunotherapy 31. KATUGAMPOLA RP, HONGBO Y, FINLAY AY:
of a rheumatologic-dermatologic team 2015; 7: 1-4. Clinical management decisions are related to
16. ALJUHANI F, TOURNADRE A, TATAR Z et al.: the impact of psoriasis on patient-rated qual-
work. The SAPHO syndrome: a single-center study ity of life. Br J Dermatol 2005; 152: 1256-
of 41 adultpatients. J Rheumatol 2015; 42: 62.
References 329-34. 32. FINLAY AY: Current severe psoriasis and the
1. CHRISTOPHERS E, MROWIETZ U: Psoriasis. 17. NALDI L, SVENSSON A, DIEPGEN T et al.: rule of tens. Br J Dermatol 2005; 152: 861-7.
In: BURGDORF W, PLEWIG G, WOLFF HH, European Dermato-Epidemiology Network. 33. PREY S, PAUL C, BRONSARD V et al.: Cardio-
LANDTHALER M (Eds.): Braun-Falco’s Der- Randomized clinical trials for psoriasis vascular risk factors in patients with plaque
matology. Springer-Verlag Berlin Heidelberg 1977-2000: the EDEN survey. J Invest Der- psoriasis: a systematic review of epidemio-
2009: 506-27. matol 2003; 120: 738-41. logical studies. J Eur Acad Dermatol Venere-
2. PREY S, PAUL C, BRONSARD V et al.: Assess- 18. RAMSAY B, LAWRENCE CM: Measurement ol 2010; 24 (Suppl. 2): 23-30.
ment of risk of psoriatic arthritis in patients of involved surface area in patients with pso- 34. SVEDBOM A, DALÉN J, MAMOLO C et al.:
with plaque psoriasis: a systematic review of riasis. Br J Dermatol 1991; 124: 565-70. Increased cause-specific mortality in patients
the literature. J Eur Acad Dermatol Venereol 19. SPULS PI, LECLUSE LLA, POULSEN M-L N F, with mild and severe psoriasis: a population-
2010; 24 (Suppl. 2): 31-5. BOS J D, STERN R S & NIJSTEN T: How Good based Swedish Register Study. Acta Derm
3. NOSSENT JC, GRAN JT: Epidemiological and Are Clinical Severity and Outcome Meas- Venereol 2015 Mar 13 [Epub ahead of print].
clinical characteristics of psoriatic arthritis in ures for Psoriasis?: Quantitative Evaluation 35. THAÇI D, BLAUVELT A, REICH K et al.:
northern Norway. Scand J Rheumatol 2009; in a Systematic Review. J Invest Dermatol Secukinumab is superior to ustekinumab in
38: 251-5. 2010; 130: 933-43. clearing skin of subjects with moderate to se-
4. ROUZAUD M, SEVRAIN M et al.: Prevalence of 20. FREDRIKSSON T, PETTERSSON U: Severe vere plaque psoriasis: CLEAR, a randomized
undiagnosed psoriatic arthritis among psoria- psoriasis--oral therapy with a new retinoid. controlled trial. J Am Acad Dermatol 2015;
sis patients: Systematic review and meta-anal- Dermatologica 1978; 157: 238-44. 73: 400-9.
S-19You can also read