The United States' Response to COVID-19: A Case Study of the First Year
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The United States’ Response to COVID-19: A Case Study of the First Year
CHAIR CASE STUDY COMMITTEE Ari Hoffman, MD
Associate Professor of Clinical
Jaime Sepúlveda, MD, MPH, Dean Jamison, PhD, MS
Medicine, Department of Medicine,
MSc, DrSc Edward A Clarkson Professor,
University of California, San
Executive Director, Institute for Emeritus, Institute for Global Health
Francisco; Affiliated Faculty, Philip
Global Health Sciences, University Sciences, University of California,
R. Lee Institute for Health Policy
of California, San Francisco; Haile San Francisco
Studies
T. Debas Distinguished Professor of
Global Health, Institute for Global Carlos del Rio, MD
Andrew Kim, MD, MPhil
Health Sciences, University of Distinguished Professor of
Resident Physician in Internal
California, San Francisco Medicine, Division of Infectious
Medicine, School of Medicine,
Diseases and Executive Associate
University of California, San
Dean at Grady Hospital, Emory
Francisco
University School of Medicine;
AUTHORS Professor of Epidemiology and Jane Fieldhouse, MS
Neelam Sekhri Feachem, MHA Global Health, Rollins School of Doctoral Student in Global Health,
Associate Professor, Institute for Public Health of Emory University Institute for Global Health Sciences,
Global Health Sciences, University University of California, San
Jeremy Alberga, MA
of California, San Francisco Francisco
Director of Program Development
Kelly Sanders, MD, MS and Strategy, Institute for Global Sarah Gallalee, MPH
Technical Lead, Pandemic Health Sciences, University of Doctoral Student in Global Health,
Response Initiative, Institute for California, San Francisco Institute for Global Health Sciences,
Global Health Sciences, University University of California, San
Katy Bradford Vosburg, MPH
of California, San Francisco; Clinical Francisco
Associate Director, Pandemic
Instructor, Lucile Packard Children’s
Response Initiative, Institute for
Hospital at Stanford University
Global Health Sciences, University
Forrest Barker of California, San Francisco
Master of Science Student in Global
Arian Hatefi, MD
Health, Institute for Global Health
Associate Professor, Department of
Sciences, University of California,
Medicine, University of California,
San Francisco
San Francisco
The United States’ Response to COVID-19: A Case Study |B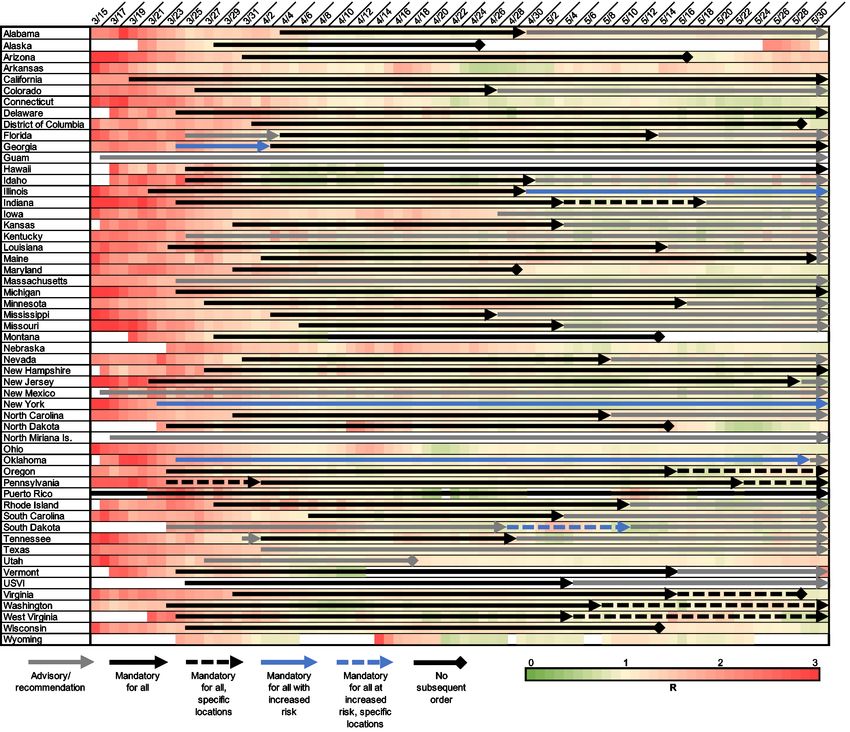
Contents
Abbreviations iii Chapter 7: Health System Resilience 38
Executive Summary 1 Hospital and Primary Care Capacity: Overflow 38
and Spillover Effects
Chapter 1: Introduction and Epidemiology 5 Human Resources for Health: Shortages, 41
The Context 5 Attrition & Mental Health Impact
This Report 6 Essential Supplies for the Healthcare System 43
How Did the U.S. Get Here? 6 Vaccine Deployment: an Operational Challenge 43
The Story in Numbers 6 Investing in Global Immunologic Equity 45
The Bottom Line 14 Chapter 8: Scientific Innovation 47
Chapter 2: Framework for Assessing the U.S. 15 Research and Development 47
Response Basic Science & Clinical Innovation 48
Domestic Leadership 16 Global Health Security Research 49
Global Leadership 18
Chapter 10: Conclusions and 50
Chapter 4: Economics and Finance 20 Recommendations
Economic Impact 20 Post-Script: The Biden-Harris National 55
Fragmented Health System Financing & Lack 24 Strategy
of Universal Health Coverage
References 56
Chapter 5: Public Health Measures 26
Appendix 74
Know the Enemy 26
The Blunt Instrument 28 Acknowledgements 77
Lockdown Replacement Package 28
Genomic Surveillance 32
The Importance of a One Health Approach 32
Chapter 6: Communications, Trust and 34
Engagement
Building and Maintaining Trust 34
Communicating Clearly 35
Empowering Communities 37
The United States’ Response to COVID-19: A Case Study | Contents |i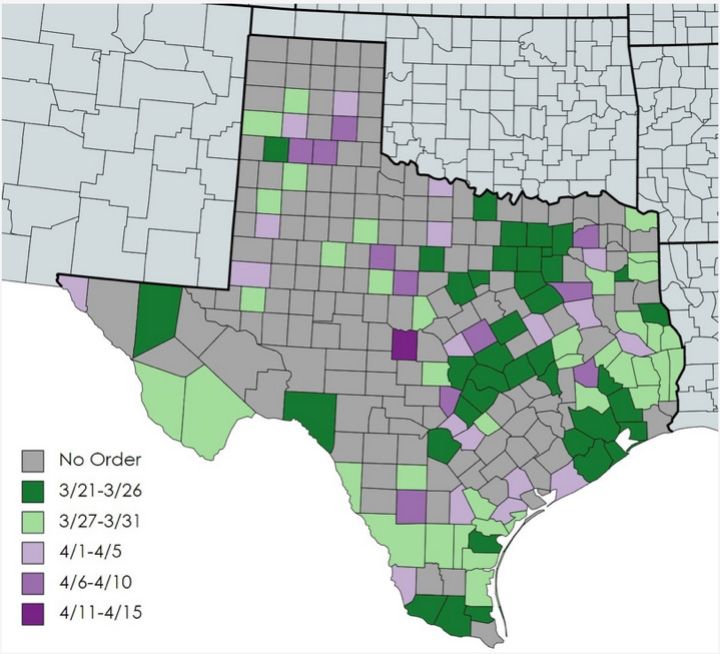
Preface
One year ago, the WHO declared COVID-19 a The second is good communication. This
pandemic. History will surely consider 2020 as means communication from leaders that is clear,
the most calamitous year in health since 1918, accurate and honest and builds trust between the
when influenza swept the globe. It will also be government and its people. The third lesson is
remembered as the worst economic crisis since that as a global community, we can trust science.
the Great Depression. The social consequences of With COVID-19, science has once again come
this pandemic will be felt for a long time to come. to the rescue, delivering innovative vaccines in
record time.
The pandemic has affected everyone on the
planet, directly or indirectly. So far over 10% of Perhaps the most important lesson from this
the global population has been infected. With pandemic is that “no country will be safe until all
over 10,000 deaths per week, COVID-19 is now countries are safe.” Global immunologic equity
the third main cause of death globally; and an should not only be a humanitarian desire, but a
estimated 4 million deaths from this pathogen national security concern. To ensure the world is
are expected by July of this year. These numbers prepared for the next pandemic, we will require
are likely to be a significant underestimate of the more than just a plan; we will require global and
morbidity and mortality and caused during this national public health institutions to be well-funded
disease. with the authority and ability to move nimbly and
forcefully in the face of uncertainty. And it will
Not all regions of the world have been similarly mean that we must think about human health as
affected. Some countries have performed much part of a broader ecologic system that includes
better than others. Understanding what elements the health of our planet, and all the species that
made a difference and what lessons can be live on it.
derived is the object of our case study.
In our research of how the U.S. has responded to
this pandemic, we find that there are four areas of
particular importance. Each of these is highlighted
in detail in our report. Jaime Sepúlveda, MD, MPH, MSc, DrSc
Chair, Case Study Committee
First is good governance, which includes
institutional strength and effective leadership.
The United States’ Response to COVID-19: A Case Study | Preface | ii
Abbreviations ACA Affordable Care Act AI/AN American Indians and Alaska Natives BARDA Biomedical Advanced Research and Development Authority CARES Coronavirus Aid, Relief, and Economic Security Act CDC Centers for Disease Control and Prevention CMS Centers for Medicare and Medicaid EU European Union FDA Food and Drug Administration FEMA Federal Emergency Management Agency GDP Gross Domestic Product HHS Health and Human Services ICU Intensive Care Unit IHR International Health Regulations IHS Indian Health Services IPPR Independent Panel for Pandemic Preparedness and Response JHE Joint External Evaluation LTCF Long-term Care Facilities MERS Middle East Respiratory Syndrome mRNA Messenger Ribonucleic Acid NGO Non-governmental Organization NIH National Institutes for Health NPI Non-pharmaceutical Interventions NSC National Security Council OECD Organization for Economic Co-operation and Development OWS Operation Warp Speed PCR Polymerase Chain Reaction PPE Personal Protective Equipment RCEP14 Regional Comprehensive Economic Partnership 14 SARS Severe Acute Respiratory Syndrome SPAR Self-Assessment Annual Reporting U.K. United Kingdom U.S. United States USCIS U.S. Citizenship and Immigration Service WHO World Health Organization The United States’ Response to COVID-19: A Case Study | Abbreviations | iii
Executive Summary
The story of COVID-19 in the United States is one of and scientific capacity. Much like the patchwork U.S.
daunting scale. The U.S. epidemic dwarfs that of any health system – the most expensive on the planet – the
other country. At the time of writing,* the U.S. reports pandemic response has been fragmented and deeply
over 28 million cases and 500,000 deaths, accounting flawed. With new variants arising worldwide, bringing
for 25% of global cases and 20% of global deaths, the epidemic under control requires strong and capable
despite comprising only 4% of the world’s population. leadership, with competent execution of sound policies,
Life expectancy in the U.S. shrank by a full year in backed by significant investments.
2020. Had the U.S. responded with the swiftness and
effectiveness of East Asia, over 428,000 American lives The World Health Organization Independent Panel on
could have been saved. Pandemic Preparedness and Response (IPPR) invited
the University of California, San Francisco Institute for
The story is also one of great inequity. The pandemic Global Health Sciences to develop a case study on
has laid bare existing socioeconomic, health, and the US response to the COVID-19 pandemic. A multi-
healthcare access disparities, with Black and Latinx disciplinary team analyzed and synthesized the work
Americans dying at over 2.6 times the rate of of academics, journalists, non-profit organizations,
White Americans. In 2020, life expectancy for Black national, state and local government agencies, and
Americans is expected to have dropped by over two private industry, studying hundreds of academic and
years, with Latinx Americans suffering a drop of over media articles, government reports, press releases,
three years. While experiencing lower mortality rates blogs, and websites. The team also conducted 23
from the virus itself, the economic and social conse- key stakeholder interviews to ensure a diversity of
quences have been particularly severe for women, viewpoints.
notably women of color. Record numbers of women
have left the labor force since the pandemic began. This report assesses the U.S. experience one year into
Despite Congress providing over $3.7 trillion dollars the still unfolding epidemic, with the aim of supporting
in fiscal relief to support businesses and families, an a smarter, faster response to this pandemic, and to the
additional eight million Americans may have slipped next one, which will surely come.
into poverty in 2020.
The devastating impact of COVID-19 on all countries,
While this report focuses on an assessment of the and the universal commitment to never let this happen
national response to the virus, the story of COVID-19 is again, provides a shared purpose and agenda for
fundamentally about individuals, families and communi- transformational change in global collective action.
ties. The human impact of the pandemic must anchor The new U.S. administration has a once in a generation
the sea of staggering statistics. Individual stories of opportunity to seize this moment and work with other
lives taken, businesses shuttered, jobs lost, schools countries to create a new era of global health security.
closed, and dreams fractured must inform all our strat-
The table below highlights key conclusions and
egies for bringing this devastating crisis under control.
recommendations. More detail on each of these is
This catastrophe has unfolded despite the United provided in the body of the report.
States’ enormous wealth and unparalleled medical
*February 22, 2021
The United States’ Response to COVID-19: A Case Study | Executive Summary |1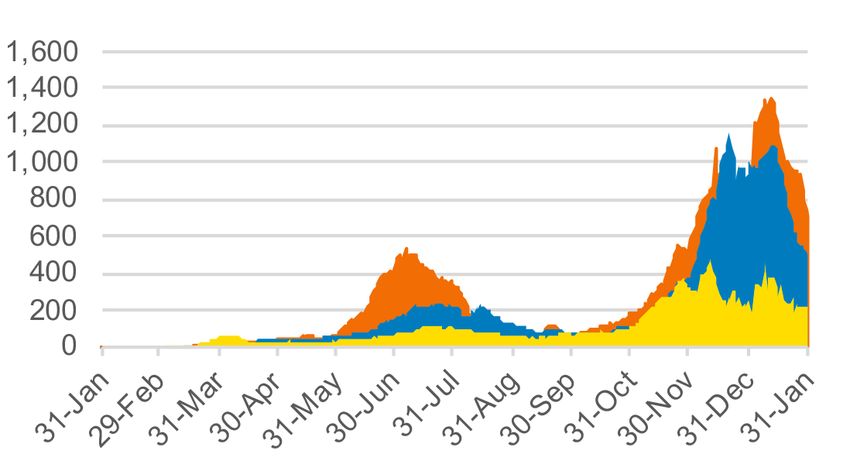
Recommendations
Response: For COVID-19 Preparedness: For the Next One
Conclusion #1 • Effective collaboration between • Legislation granting emergency
federal, state and local levels, powers and funding to mobilize
The United States lacked with clearly defined roles and a rapid, coordinated, federally-led
effective political leadership responsibilities. response during public health
• Fully staffed National Security emergencies.
in its COVID-19 response at
Council Directorate for Global • An apolitical architecture for key
the federal level. Leadership
Health Security and Biodefense. public health institutions such as
at sub-national levels was the Centers for Disease Control and
highly variable. Prevention and the Food and Drug
Administration. Consider Federal
Reserve model.
Conclusion #2 • Substantial additional federal • Public Health Infrastructure Fund
monies for pandemic control, to modernize information
The U.S. failed to act early including for widespread community technology infrastructure for
and decisively in combating surveillance, rapid antigen testing, coordinated operational response
supported isolation and quarantine, during public health emergencies.
the virus. Critical delays and
genomic surveillance, and vaccine • Investments in public health
poorly executed basic public roll-out. capacity to develop and deploy
health interventions, com- • Robust testing infrastructure to basic public health measures at
pounded by chronic under- scale-up public health surveillance. scale.
investment in public health, Consider public-private testing • Public messaging campaign to
were key contributors to the consortium modeled on Canada's prepare American people for the
staggering number of cases CDL Rapid Screening Consortium. next pandemic. Public education
• Expanded mask mandates and on need for emergency powers,
and deaths.
public education to promote potential loss of individual
The underinvestment in importance of mask wearing. freedoms, and importance of
• Investments in safe reopening of compliance during public health
public health continued emergencies.
schools and childcare facilities,
in 2020 with only 1.6% of including federal funding for
Congressional emergency infrastructure improvements, and
appropriations targeted to for rapid testing and priority
public health agencies for vaccination of teachers and staff.
epidemic control. • Investments in supported isolation
and quarantine programs, which
provide financial and social support
to those who are infected or have
been in contact with an infected
person. Include options for
conditional cash transfers, paid
institutional isolation, and direct
economic relief for workers lacking
employment protections.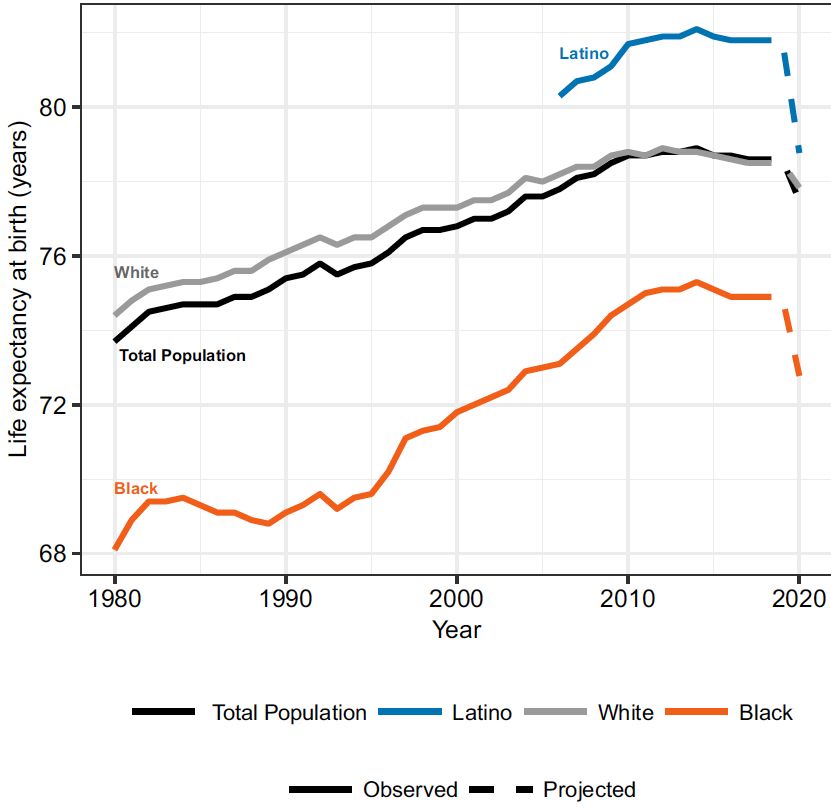
Recommendations
Response: For COVID-19 Preparedness: For the Next One
Conclusion #3 • Investments in targeted programs • Significant investments to flatten the
to protect hardest hit groups curve of racial and ethnic disparities
Immigrant, Black, Latinx, including communities of color, in health. This includes access to
American Indian/Alaska and low-income, incarcerated, testing facilities, healthcare coverage
institutionalized, homeless, and and access, worker protections and
Native populations, and
immigrant communities. sick leave benefits, and an expanded
those living in poverty, have social safety net for community
• Community partnerships for
suffered disproportionately culturally competent public health resilience.
from the COVID-19 messaging on testing, vaccination,
pandemic. and compliance with public health
orders such as mask wearing and
social distancing.
• Testing and Treatment Safe Havens
for undocumented workers. Free
testing, treatment, and vaccination
regardless of immigration status.
• Required state reporting of public
health interventions by racial and
ethnic group.
Conclusion #4 • Flexible rules for public coverage • Enhanced federal incentives for
of COVID-19 related interventions Medicaid expansion in the 12 states
The structure of the including testing, treatment, and that have not done so already, with
U.S. health system is short and long-term care for post- requirements to address chronic
COVID-19 disability. Guaranteed coverage gaps faced by millions.
fundamentally ill-suited
financial protection against medical • Commitment, funding and
to mounting an effective, impoverishment for those affected. action to ensure universal health
coordinated response to • Increased federal premium tax coverage for everyone.
a pandemic. credit or direct subsidies to ensure
continuity of health coverage for
unemployed or under-employed,
who are ineligible for Medicaid.
Conclusion #5 • Federal emergency subsidies for • Well stocked and expanded
federally qualified health centers Strategic National Stockpile to
Hospitals in the U.S. were and under-resourced hospitals in cope with outbreaks of novel
unprepared to cope with rural areas. pathogens.
the high influx of COVID-19 • Investments in strengthened
domestic supply chains for
patients.
critical products.
• Early use of Defense Production
Act during public health
emergencies.
• Disaster contingency planning
for worst-case novel pathogens
required for accreditation of
hospitals and health facilities.
The United States’ Response to COVID-19: A Case Study | Executive Summary |3Recommendations
Response: For COVID-19 Preparedness: For the Next One
Conclusion #6 • Coordinated and well-funded • Federal support of public-private
vaccine distribution program. partnerships to develop universal
U.S. commitment to vaccine • Investments in vaccine equity influenza and coronavirus vaccines
development has been a including health promotion and therapeutics.
defining success. Slow initial campaigns led by community • Re-engineered processes for faster
leaders to allay fears and overcome approval of new vaccines and
rollout and the absence of
high levels of vaccine hesitancy therapeutics while safeguarding
a coordinated national among some communities. the quality of approved products.
vaccination strategy has • Incentives to vaccine manufacturers
threatened to overshadow to develop improved, cheaper, and
this singular achievement. easier to administer vaccines for
COVID-19.
Conclusion #7 • Targeted relief for small businesses • Clear agenda and funding for
and those experiencing financial strengthened social safety net.
Record levels of federal hardship. • Reduced variability among states
spending to support families • Federal support to state and local and among ethnic groups in access
and businesses have been governments for continued to basic health and social services.
employment of teachers, public
effective in protecting many
health professionals, police,
Americans from serious corrections officers, and other state
economic shocks. However, and local government employees.
more must be done to
ensure continued recovery.
Conclusion #8 • Investments and active participation • Active participation and investment
in global immunologic equity, to create a robust global health
The U.S. will not be safe including support of COVAX, and architecture for pandemic
until all countries are safe. other initiatives to develop and preparedness and response.
deploy new therapeutics and • Funding for a multi-disciplinary
Pandemics represent a
diagnostics for low and lower- One Health approach, including
global security threat that middle income countries. bio-surveillance at the human-
requires commitment to animal interface.
global immunologic equity.
To prevent the scale of
suffering inflicted by this
pandemic, the world needs
a strengthened global
architecture for pandemic
preparedness and response.
The United States’ Response to COVID-19: A Case Study | Executive Summary |4Chapter 1: Introduction
and Epidemiology
Sarah* called the urgent care pediatrician in including her three children, cousin, elderly par-
tears. Her two-year-old son, Eddie had been ents, and her sister’s family. Her cousin, aged 34,
diagnosed with COVID-19 during an emergency was now in the Intensive Care Unit with severe
department visit the previous day. She simply COVID-19 pneumonia. Her elderly mother with
couldn’t get his fever down and he wouldn’t heart disease had started coughing. She sobbed
drink. Sarah, a Latina waitress earning a questions over the phone: Would Eddie recover?
minimum wage, has no paid sick leave or Would her cousin live? Would her mother die
employment protections. She was exposed to from a virus she had brought home? Who would
COVID-19 by a coworker who could not afford bring them groceries or pick-up Eddie’s medicine
to isolate and came to work infected. Sarah also if she isolated? Her husband, the only person
became ill, along with many of her coworkers. in the household without symptoms, knew he
Unable to isolate from her large family, the virus should quarantine but couldn’t because they
spread rapidly through her household of eleven, needed his paycheck to survive.
The Context The story is also one of great inequity. The pandemic
has laid bare existing socioeconomic, health and
Sarah’s story is tragically common in the United States. access disparities, with Black, American Indians and
Despite being the wealthiest country in the world, the Alaska Natives,† and Latinx Americans dying at over
U.S. lacks a basic social safety net, compounding the 2.6 times the rate of White Americans‡,5,6 when adjust-
suffering reaped by the COVID-19 pandemic. While this ed for age.7 Projections show that in 2020, life expec-
report focuses on an assessment of the U.S. national tancy at birth for Black Americans will have dropped
response to the virus, the story of COVID-19 is funda- by over two years, while Latinx Americans will have
mentally about individuals, families and communities. suffered a drop of over three years.4 Life expectancy for
The human impact of the pandemic must anchor the Black males (74.9 years) was already a full 3.6 years
sea of staggering statistics. Individual stories of lives less than that of White males (78.5 years) in mid 2020.4
taken, businesses shuttered, jobs lost, schools closed, While experiencing lower mortality from the virus itself,
and dreams fractured must inform all our strategies for the economic and social consequences have also been
bringing this devastating crisis under control. particularly severe for women, notably for women of
color and immigrants like Sarah.8,9,10
The story of COVID-19 in the United States is one of
daunting scale. The U.S. epidemic dwarfs that of any This catastrophe has unfolded despite the United
other country. At the time of writing, the U.S. reports States’ unparalleled medical and scientific capacity.
over 28 million cases and 500,000 deaths, accounting Much like the patchwork U.S. health system – the most
for 25% of global cases and 20% of global deaths, expensive on the planet – the pandemic response has
despite comprising only 4% of the world’s popula- been fragmented and deeply flawed. And with new
tion.1,2,3 A recent study shows that average U.S. life variants arising worldwide and sluggish initial vaccine
expectancy at birth is expected to have dropped by a deployment, bringing the epidemic under control will
full year in 2020.4
*This is a true story with the names changed. ‡For the purposes of this report we have capitalized the term ‘White’
†This report uses the term American Indian and Alaska Native (AI/AN) in concordance with recommendations from the Center for the Study
in keeping with the conventions through which AI/AN communities of Social Policy and the National Association of Black Journalists.
refer to themselves.
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology |5require transformational leadership, with swift and seriousness of the virus, and to implement basic public
competent execution of sound policies, backed by health containment measures between January and
significant investments. March 2020. The consistent minimization of the unfold-
ing catastrophe, with false and misleading messages
from leaders, led to complacency and confusion, which
This Report allowed the virus to spread unchecked. A notable
This case study of the U.S. response to the COVID-19 success, however, was Operation Warp Speed, which
pandemic shines a light on lessons learned and led to the development of effective vaccines in record
provides recommendations for immediate action time. The key events in this timeline are discussed in
and longer-term preparedness to the World Health greater detail in the chapters of this report.
Organization Independent Panel on Pandemic
Preparedness and Response (IPPR). The Story in Numbers
The report analyzes and synthesizes the work of The U.S. epidemic is actually a composite of hundreds
academics, journalists, non-profit organizations, of different epidemics in towns, counties and cities
national, state and local government agencies, and throughout the United States. In this section we ex-
private industry. A multidisciplinary team, under the amine cases and deaths nationally and sub-nationally,
leadership of the University of California, San Francisco, covering the period of January 2020 to January 2021.
Institute for Global Health Sciences, has studied
hundreds of academic and media articles, government The U.S. Compared to Europe and East Asia
reports, press releases, blogs and websites. The team We compare U.S. cases and deaths to two major
also conducted 23 key stakeholder interviews to economic blocks using the University of Oxford data-
ensure a diversity of viewpoints. The conclusions and set: the European Union (EU)* and the Asian Regional
recommendations included in this report have been Comprehensive Economic Partnership minus China
reviewed by a group of external experts. (RCEP14).†3 By the end of January 2021, the United
The report’s aim is to provide an objective analysis States reported over 20 million cases, 79% higher than
and build a comprehensive narrative that can be used the EU when adjusted for population (Figure 1A).3 Due
to support a smarter, faster, more effective response, to limited testing availability, it is estimated that actual
both for this pandemic and the next one that will surely cases could be up to 20 times higher than those
come. reported.12 Strikingly, cumulative U.S. cases per million
people were almost 27 fold those in the RCEP14,
In this chapter, we lay a foundation for discussing the which has clearly been the world leader in containment
U.S. response to COVID-19 by highlighting key events of the virus.3
in the U.S. epidemic and providing an overview of its
epidemiology. Chapter 2 discusses our assessment By February 22, 2021, 500,000 Americans had died
framework. The main body of the report assesses the from COVID-19.13 In the month of January alone, one
U.S. response in the key domains of this framework; American was dying every 28 seconds.14
the final chapter provides conclusions and recommen- Higher case fatality ratios in certain European countries
dations; a Post Script at the end of the report highlights contributed to the EU and U.S. having similar peaks
key actions by the Biden Administration taken since in death rates in winter 2020–2021, but because of its
January 20, 2021. continuously high mortality rate throughout the year,
the U.S. (1354 deaths/million) had a cumulative mortality
How Did the U.S. Get Here? rate 28% higher than the EU (1058 deaths/million). The
cumulative U.S. mortality rate was a remarkable 22 fold
“There are instances in history where that of the RCEP14 (60 deaths/million) (Figure 1B).3
humanity has really moved mountains to
defeat infectious diseases. It’s appalling
that we in the U.S. have not summoned *European Union: Austria, Belgium, Bulgaria, Croatia, Cyprus, Czech
Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hun-
that energy around COVID-19.” gary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands,
Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, U.K.
– Caitlin Rivers, epidemiologist, Johns Hopkins (no longer part of the EU as of 12/31/2020)
Center for Health Security11 †Regional Comprehensive Economic Partnership: Australia, Brunei,
Cambodia, Indonesia, Japan, Korea, Laos, Malaysia, Myanmar,
As the timeline below shows, there were multiple lost New Zealand, Thailand, the Philippines, Singapore and Vietnam. We
opportunities for the U.S. to recognize the potential exclude China due to population size.
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology |6Timeline of Key Events
12/31/19 World Health Organization is alerted to 2/26/20 Vice President Pence is appointed
reports of unusual cases of pneumonia to lead White House COVID-19 Task
linked to Huanan Seafood Wholesale Force. President Trump announces,
Market in Hubei Province and requests “This is a flu. This is like a flu.”26,27 CDC
verification from the Chinese govern- confirms community transmission in
ment of an emerging outbreak.15,16 It is U.S.28
suspected that undetected infections
2/27/20 White House takes control of all official
were circulating in Hubei, France, and
government press on COVID-19,
Italy as early as October, 2019.17
sidelining CDC and other public health
1/3/20 CDC China Director calls U.S. CDC agencies.29 CDC relaxes guidelines
Director for the first time about novel for testing and directs state public
viral outbreak.18 health labs to use test kits without
contaminated component.30
1/9/20 WHO reports the Chinese Government
has determined the outbreak is caused 2/29/20 President Trump begins leading press
by a novel coronavirus.19 briefings in which he minimizes threat
of the virus. He repeatedly praises the
1/11/20 Chinese authorities share genetic
U.S. response assuring the public that
sequence of SARS-CoV-2.19 First
“No, I’m not concerned at all. No, I’m
reported COVID-19 death occurs in
not. No, we’ve done a great job.”31
Wuhan.20
3/1/20 First case of COVID-19 is identified in
1/13/20 WHO publishes protocol for PCR assay
New York, starting a deadly surge on
developed by partner laboratory.19
the East Coast. Later studies show
1/21/20 Washington State confirms first case the virus has been circulating since
of novel coronavirus in traveler from January in the U.S., with first suspect-
China, who had arrived in the U.S. on ed cases of community transmission
January 15.16 dating from February.32,33
1/23/20 China issues lockdown of Hubei 3/11/20 WHO announces COVID-19 is officially
Province but virus is already a pandemic.19 U.S. issues travel ban
spreading worldwide.21 for expanded list of countries. All
travelers from these countries are
1/29/20 White House Coronavirus Task Force is
funneled to specific airports and
formed.22
screened on arrival.34
1/30/20 WHO announces a Public Health
3/13/20 President Trump declares a national
Emergency of International Concern.19
emergency.35
1/31/20 Trump administration announces travel
3/16/20 Trump administration announces 15
ban on non-U.S. citizens who have
day “Social Distancing” guidelines with
been to China in the past 14 days.23
non-essential business closures and
2/4/20 FDA grants emergency authorization stay-at-home orders (also called
of proprietary CDC test kits, which are lockdowns). This is later extended
not based on WHO published assay.24 to 45 days.36
2/5/20 CDC begins shipping test kits to state 3/17/20 COVID-19 is identified in all 50
public health departments. These kits states.37
are later found to be contaminated.24,25
3/26/20 1,000 U.S. Deaths Confirmed
2/6/20 First U.S. Death Confirmed
3/27/20 $2.2trn Coronavirus Aid, Relief, and
Economic Security Act (CARES) is
passed as stimulus relief for
businesses and families.38,39
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology |74/24/20 50,000 U.S. Deaths Confirmed 10/28/20 White house announces free future
COVID-19 vaccines for U.S. citizens.54
5/15/20 Operation Warp Speed is launched to
begin development of vaccines for 12/11/20 Emergency use authorization is granted
SARS-CoV-2.40 for Pfizer-BioNTech vaccine.55
5/27/20 100,000 U.S. Deaths Confirmed 12/14/20 300,000 U.S. Deaths Confirmed
7/9/20 WHO announces COVID-19 can be 12/27/20 Coronavirus Response and Relief
airborne after more than 200 scientists Supplemental Appropriations Act
sign a letter urging the organization to authorizing $900 billion in additional
revise its recommendations.41,42 funding, is passed to continue benefits
for those affected by lockdowns.56
7/15/20 The White House requires all hospitals
to bypass CDC and send COVID-19 12/30/20 B.1.1.7 variant from the U.K. is
data to Health and Human Services detected. Other variants are emerging
(HHS).43 in South Africa and Brazil.57
7/22/20 Advance purchase agreements are 1/19/21 400,000 U.S. Deaths Confirmed
signed with Pfizer and BioNTech for
1/20/21 Joe Biden is sworn in as 46th
large supplies of vaccines, contingent
President of the United States.
on successful Phase 3 trials.44,45
2/22/21 500,000 U.S. Deaths Confirmed
8/7/20 Large rally of motorcyclists in Sturgis,
North Dakota becomes “superspreader”
event.46
8/25/20 CDC issues guidelines recommending
exposed people who are asymptomatic
do not need testing. CDC's scientific
review process later reverses this
guidance.47,48
9/14/20 U.S. airports are instructed to stop
redirecting passengers from certain
‘hotspots’ and to stop screening
international travelers.49
9/22/20 200,000 U.S. Deaths Confirmed
9/26/20 White House Rose Garden gathering
for new Supreme Court justice
becomes a superspreader event.50
10/2/20 President Donald J. Trump tests
positive for COVID-19 and receives an
array of advanced treatments, includ-
ing monoclonal antibodies, remdesivir,
oxygen and steroids.51
10/5/20 President Trump is discharged from
the hospital. In subsequent days, he
reassures the American public saying,
“Don’t be afraid of COVID”, and “You
catch it, you get better, and you’re
immune.”52,53
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology |8Figure 1C shows the 7-day rolling average for incident dramatically worse than the RCEP14. This is remark-
cases in the three geographic regions. Following spring able given the extreme diversity of RCEP14 countries,
surges in both the U.S. and EU, the EU was able to from Laos to Japan, and Australia to the Philippines.
control transmission during the summer months, while As discussed in this report, these large differences do
the U.S. continued to experience high transmission not stem from the fundamental biology of the virus or
rates throughout the summer. While both regions its human victims, but from the critical nexus of
suffered major surges in the fall and winter, the U.S. leadership, policy, execution, and compliance.58 These
surge was much greater. By contrast, having contained differences in performance are not merely of scientific
community spread early in the pandemic, the RCEP14 interest – they translate into hundreds of thousands
had consistently low case incidence rates throughout of human lives saved or lost. If the U.S. had the same
the year.3 cumulative deaths/million as the RCEP14 over the last
year, a staggering 428,000 American lives would have
As Figures 1A–D illustrates, while the U.S. performed been saved by the end of January 2021.
somewhat worse than the EU in 2020, it performed
Figure 1. Regional analysis United States, European Union, RCEP 143
A: Cumulative COVID-19 cases per million B: Cumulative COVID-19 deaths per million
90,000 1,600
80,000 1,400
70,000 1,200
60,000
1,000
50,000
800
40,000
30,000 600
20,000 400
10,000 200
0 0
31 ov
31 c
31 ov
31 c
29 an
31 n
an
29 an
31 n
an
31 ul
31 ul
30 ay
30 y
31 eb
30 ar
30 ug
31 p
31 b
30 ug
31 p
30 ar
30 c t
30 c t
31 pr
31 pr
e
e
a
u
u
e
e
e
-J
-J
-O
-O
-M
-M
-A
-A
-N
-D
-N
-D
-M
-M
-A
-S
-A
-S
-J
-J
-J
-J
-J
-J
-F
-F
31
31
C: Daily new COVID-19 cases per million, rolling 7-day D: Daily new COVID-19 deaths per million, rolling 7-day
average average
800 12
700 10
600
500 8
400 6
300 4
200
100 2
0 0
31 v
31 c
29 an
un
an
29 an
un
an
31 ul
31 ul
30 y
30 y
31 b
30 ar
30 g
31 p
31 b
30 r
30 c t
30 c t
31 pr
31 pr
31 v
31 c
30 g
31 p
a
o
e
a
a
e
u
e
e
o
e
u
e
-J
-J
-O
-O
-M
-M
-A
-A
-N
-D
-M
-M
-A
-S
-J
-J
-J
-J
-J
-J
-F
-F
-N
-D
-A
-S
31
31
31
31
United States European Union RCEP 14
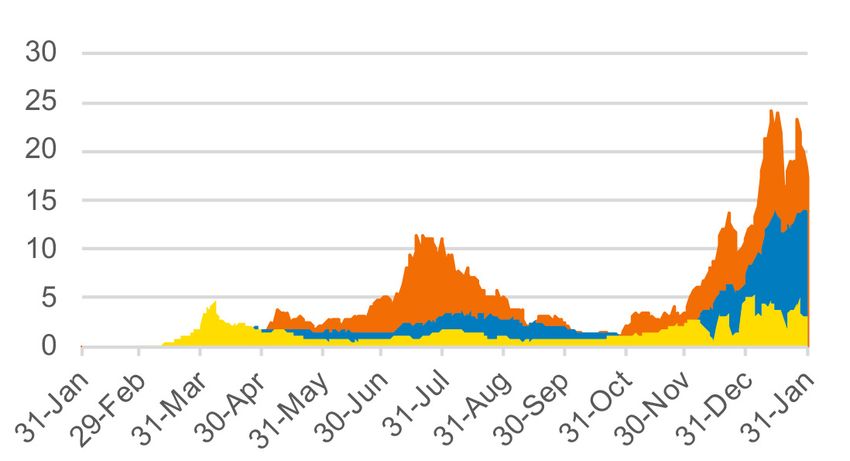
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology |9Testing in the United States Comparing States
Testing is important both to understand the scale of the There are significant variations among states in the
epidemic and to prevent community spread through U.S. in case and death rates. Without federal guidance,
isolation and quarantine. Testing roll-out did not states, counties, and cities pursued widely divergent
begin in earnest in the U.S. until mid-March, almost approaches, creating a patchwork of policies and
two months after the virus had arrived in the country. performance. Decisions on when and how to enact
public health interventions such as shelter-in-place
U.S. testing policy continues to prioritize symptomatic orders or “lockdowns,” as they were known, were left
patients over widespread community testing to identify to county public health departments, resulting in
and isolate asymptomatic cases. There are no federal haphazard implementation and differing orders, even
standards for reporting testing data, with each state within the same state.
determining which types of tests to report (PCR,
antigen etc.). States have also paused reporting at We use the Johns Hopkins University dataset to
various points. With these caveats, Figure 2 shows compare differences in case and death rates in three
the ramp-up of testing in the U.S., with rates growing states that are representative of a broad range of
slowly but steadily from March 2020 and notable peaks performance. Cases rates are impacted by testing
in December and January. policies in each state so interstate comparisons must
be viewed with caution. In addition, as with national
Figure 2. Daily COVID-19 tests per thousand data, real case numbers may be more than 10 times
people in the U.S., rolling 7-day average59 higher than reported. Figure 3A shows cumulative case
rates in Arizona, California, and Washington.1
5 Total cases/million people in Arizona, one of the worst
performing states were 2.5 times higher than those in
4
Tests/1000
U.S. tests Washington, one of the best performing states. The
performed cumulative death rate in Arizona was more than
3
triple that of Washington (Figure 3B). One cause of this
2 disparity may be the different racial and ethnic mix in
1
these two states. Whereas Arizona has a population
that is 42% Black, Latinx or American Indian, in
0 Washington State less than 20% of people fall into one
8-Mar 30-Apr 19-Jun 8-Aug 27-Sep 16-Nov 31-Jan of these racial or ethnic groups.60,61 Perhaps a fairer
2020 2020 2020 2020 2020 2020 2021 comparison would be between Arizona and California,
which have more similar racial and ethnic make-ups.62
Yet, Arizona’s mortality rate was 75% higher than that
Source: Daily COVID-19 Tests. Reprinted from Ourworldindata.org,
by M. Roser et al. 2021. Retreived from https://ourworldindata.org/
of California.1
coronavirus. Copyright 2021 by Our World In Data. Reprinted with
permission.
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology | 10Figure 3. State analysis for Arizona, California, and Washington1
A: Cumulative COVID-19 cases per million B: Cumulative COVID-19 deaths per million
C: Daily new COVID-19 cases per million, rolling 7-day D: Daily new COVID-19 deaths per million, rolling 7-day
average average
Arizona California Washington
While California and Washington managed to slow Total COVID-19 mortality rates between the best
transmission during the summer months, Arizona performing state, Hawaii, and the worst performing
experienced a summer peak followed by an even state, North Dakota, show more than a 6.5 fold
higher winter peak, which rose to more than 1300 difference. It is beyond the scope of this report to
cases/million per day (Figure 3C).1 analyze the causes of these differences.
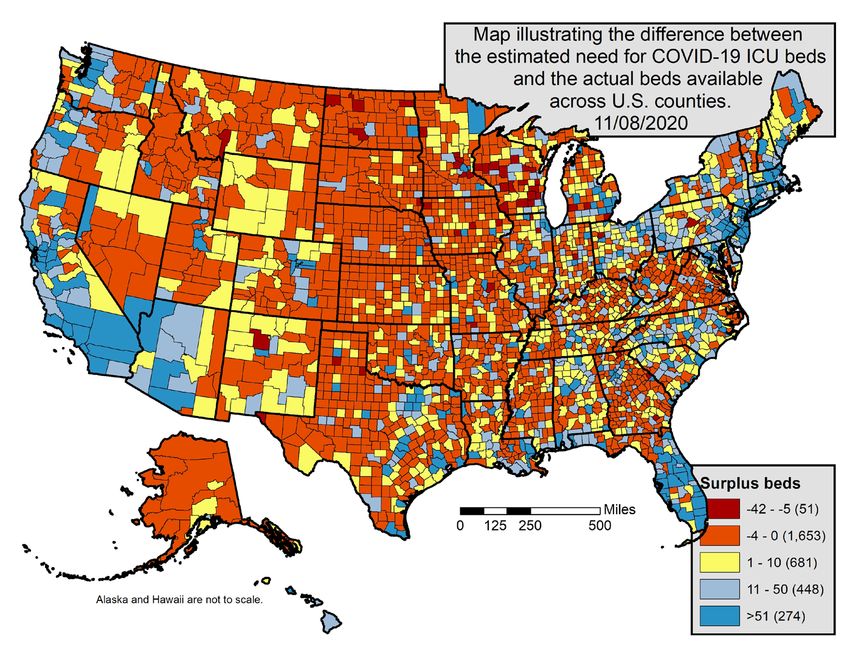
These patterns indicate starkly different outcomes Comparing Counties
between states by the end of 2020, translating into The differences among counties are even more notable.
many lives saved or lost, and pointing to major We compare two well-known counties in California, Los
differences in the performance of state governments Angeles and San Francisco (Figure 4).1 These counties
and agencies. are illustrative, rather than representative, of all U.S.
counties.
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology | 11Figure 4. County analysis for San Francisco and Los Angeles, California1
A: Cumulative COVID-19 cases per million B: Cumulative COVID-19 deaths per million
120,000 1,800
1,600
100,000 1,400
80,000 1,200
1,000
60,000 800
40,000 600
400
20,000 200
0 0
31 ul
30 y
31 b
30 ar
30 c t
31 pr
31 ov
31 c
29 an
31 n
an
30 ug
31 p
31 ov
31 c
an
29 an
31 n
31 ul
30 ay
31 eb
30 ar
30 ug
31 p
30 c t
a
31 pr
e
e
u
e
-J
-O
e
-M
-A
u
e
-M
-F
-N
-D
-J
-A
-S
-J
-J
-J
-O
-M
-A
-N
-D
-M
-A
-S
-J
-J
-J
-F
31
31
C: Daily new COVID-19 cases per million, rolling 7-day D: Daily new COVID-19 deaths per million, rolling 7-day
average average
1,800 30
1,600
1,400 25
1,200 20
1,000
800 15
600 10
400
200 5
0 0
31 b
30 ar
30 c t
31 pr
31 ov
31 c
29 an
31 n
an
31 ul
30 y
30 ug
31 p
31 v
31 c
29 an
un
an
31 ul
30 y
31 b
30 ar
30 g
31 p
30 c t
e
31 pr
e
a
u
e
-O
-M
-A
o
e
-J
a
e
u
e
-F
-N
-D
-M
-A
-S
-J
-J
-J
-J
-O
-M
-A
-N
-D
-M
-A
-S
-J
-J
-J
-F
31
31
31
Los Angeles San Francisco
Despite identical state public health orders, compliance, Latinx in Los Angeles compared to 15% in San
enforcement and local policies differed markedly in Francisco.63,64 It is beyond the scope of this report
these two counties. San Francisco managed to control to analyze the causes of these differences.
its epidemic, with a cumulative case rate of approx-
imately 36,000/million and a low death rate of 368/ Inequities in Cases and Deaths
million (Figure 4A). By contrast, case and death rates in “We in California have to face the fact that
Los Angeles were 3.1 and 4.5 times higher, respectively,
at the end of January 2021 (Figure 4A & B). our Latino communities, overrepresented
among frontline workers, have never seen
These large differences are also clearly reflected in daily a decline in cases and deaths the way
case and death rates (Figure 4C & D). Daily case rates
in Los Angeles first peaked in June and then exploded other groups have. That means there has
in the winter months, despite warmer weather always been a rip-roaring brush fire in
conditions. Daily death rates in San Francisco were those communities.”65
consistently and dramatically lower than those in Los
Angeles, reflecting a combination of lower transmission – Dr. Kirsten Bibbins-Domingo, Director,
and lower case fatality ratios. Some of this variation Epidemiology and Biostatistics, University of
may be explained by differences in racial and ethnic California, San Francisco
demographics, with a population that is almost 50%
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology | 12COVID-19 has exploited existing disparities in health Table 1. Age adjusted COVID-19 cases,
outcomes in people of color, immigrants and low-in- hospitalizations, and deaths, by race/ethnicity,
come individuals. These historical disparities are January 20217
multifactorial and rooted in systemic racism, including
lower education attainment, fewer employment Rate ratios American Hispanic Black or
opportunities, and unequal access to health coverage compared Indian or or Latino African
and medical care.66,67,68 Almost a quarter of Black to White, Alaska American,
and Latinx Americans live in multigenerational homes Non-Hispanic Native, Non-
with crowded conditions efficiently fueling viral trans- persons Non- Hispanic
mission.69 Poverty and occupational hazards are also Hispanic
more pronounced in these communities, with many Cases 1.8 x 1.7 x 1.4 x
employed at low paying essential jobs, such as factory Hospitalizations 4x 4.1 x 3.7 x
work or grocery stores, placing them at higher risk of
Death 2.6 x 2.8 x 2.8 x
infection. Lacking employment benefits and protections,
isolating and quarantining is often financially infeasible. Source: Hospitalizations and Death by Race/Ethnicity. Adapted
For example, only 46% of Latinx workers have from CDC.gov by the Centers for Disease Control and Prevention.
Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/covid-
employer paid sick leave, compared to 67% of White data/investigations-discovery/hospitalization-death-by-race-ethnicity.
workers.70,71 In addition, disadvantaged communities html. Copyright 2021 by the CDC. Reprinted with permission.
experience higher rates of comorbidities, placing them
at additional risk for severe COVID-19.72,73 Modeling suggests that the long-term consequences
of this epidemic will be devastating for disadvantaged
Despite higher demand for testing in minority communi- communities, widening gaps in life expectancy.4,76 A re-
ties due to higher infection rates, one study found that cent study estimates that reductions in life expectancy
these communities tended to live in “testing deserts.”74 in 2020 in Black and Latinx populations are likely up to
Zip codes where the population is 75% or more White, four times those in White populations (Figure 5).4
had an average of one test site per 14,500 people;
whereas zip codes with 75% of residents who are
Figure 5. Projected trends in life expectancy by
people of color, had one test site per 23,300 people.74
population4
When adjusted for age, differences in outcomes for
Black, Latinx, and American Indian and Alaska Native
communities are pronounced (Table 1). Members of
these communities were 3.7 to 4.1 times as likely to
be hospitalized as White Americans, and between 2.6
to 2.8 times more likely to die from COVID-19.75 With
a history of disenfranchisement, American Indian and
Alaska Native communities in particular have
experienced poor outcomes (Box 1).75
Source: Projected trends in life expectancy by population. Reprinted
from Reductions in 2020 US life expectancy due to COVID-19 and
the disproportionate impact on the Black and Latino populations by T
Andrasfay, 2021, Proceedings of the National Academy of Sciences
of the United States of America, 118 (5) e2014746118. Copyright
2021 by PNAS. Reprinted with permission.
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology | 13Box 1: COVID-19 in American Indian and Alaska Native Communities
American Indians and Alaska Natives (AI/AN) have Figure 6. Public health expenditures per capita,
suffered greatly in this pandemic.77 Though leadership 201784
of many tribal communities was strong and proactive,
baseline disparities in healthcare embedded in histories 14,000
of neglect, erasure, under counting, and structural
racism, have contributed to poor outcomes.78,79,80 12,000
American Indians and Alaska Natives, like many his-
torically disadvantaged groups, often work in essential
jobs, and live in shared housing, placing them at high 10,000
U.S. Dollars per capita
risk for infection.81,82 Some American Indian reservations
lack basic necessities like running water, particularly 8,000
shocking in the wealthiest country in the world.83
National data also likely undercount AI/AN cases due
to limited availability of testing, and exclusion or 6,000
misclassification of ethnicity in national data reporting.82
4,000
Healthcare in tribal territories is provided by the Indian
Health Service (IHS), a branch of the U.S. government.
The IHS, which runs its own hospitals and clinics, 2,000
receives only 38% of the per capita funding as the
Veterans Affairs Administration, which also operates its
0
own health facilities (Figure 6).84 Indian Veterans Medicaid Medicare
Health Administration
Service
Federal program
Source: Public Health Expenditures per capita. Reprinted from
Spending Levels and Characteristics of IHS and Three Other Federal
Health Care Programs by the Indian Health Services, 2020, retrieved
from https://www.gao.gov/products/gao-19-74r. Copyright 2020 by
the Government Accountability Office. Reprinted with permission.
The Bottom Line deaths/million), and at the same level as some of the
best performing European countries.
On the international stage, the U.S. has performed
poorly in comparison to the European Union, and The U.S. has failed its most vulnerable populations.
disastrously compared to East Asia and Australasia. Without exception, communities of color and historically
Within the U.S., some states and counties have per- disadvantaged people have suffered a far greater
formed notably better than others, indicating that poor burden of sickness, death, and economic and social
national performance was not inevitable. If all states hardship. On many fronts, the vulnerabilities and
and counties had been as effective at containing the inequities in U.S. society have been exposed. Perhaps
pandemic as Washington (563 deaths/million) or San this will be a wake-up call for the country to address
Francisco (368 deaths/million), the U.S. would have these long-standing disparities.
performed much better than the EU average (1058
The United States’ Response to COVID-19: A Case Study | Chapter 1: Introduction and Epidemiology | 14Chapter 2: Framework for
Assessing the U.S. Response
Historically, epidemic and pandemic preparedness and Table 2. A systems framework for assessment of
response frameworks have aimed to provide nations the United States COVID-19 response
with opportunities to evaluate response readiness.
These measurement tools assess national and global Category Description
health security capacity to minimize health shocks from
biological threats when they occur. Pandemic influenza Leadership Political leadership at all levels.
has been a central focus of many global assessment Attributes assessed: decision-making;
efforts; though recent infectious diseases, such as accountability; and constructive influ-
ence on public opinion and behavior.
SARS (2002), MERS (2012), Ebola virus disease (2014,
2018), and Zika virus (2015), have prompted revisions Economics Economic impact and special appro-
to these frameworks. and Financing priations for income support and virus
control, equitable and strategic distri-
The main global instrument for measuring pandemic bution of funds. Attributes assessed:
preparedness is the International Health Regulations resources for COVID-19; federal allo-
(IHR) 2005.85 The IHR provides a legal framework that cations; and safety net mechanisms.
defines responsibilities and obligations of State Parties
during public health events. It also includes a Moni- Public Health Activities to decrease viral transmis-
toring and Evaluation Framework that consists of two Measures sion and safeguard health. Attributes
assessed: testing strategy and imple-
measurement tools: State Parties Self-Assessment
mentation; contact tracing, masking,
Annual Reporting (SPAR) and Joint External Evalu-
quarantine, and isolation; stay-at-
ations.86,87 While the IHR is used by 196 countries,
home orders or sectoral closures and
numerous other frameworks exist, including the Global bans on large gatherings; surveillance
Health Security Agenda 2024 Framework, and the systems; and border control.
Global Health Security Index.88,89
Commu- Activities to build confidence in the
Multiple high-level reviews by independent panels and nication, integrity and reliability of institutions.
commissions have followed recent epidemics. Notable Trust and Attributes assessed: public trust in
examples, each with their own assessment methodolo- Engagement leaders and government agencies;
gies, include the WHO Ebola Interim Assessment communication accuracy, clarity,
Panel,90,91 the Harvard-LSHTM Independent Panel on reliability, consistency, transparency,
the Global Response to Ebola,92 the National Academy empathy; community engagement.
of Medicine Commission on a Global Health Risk
Health Health services delivery. Attributes
Framework for the Future,93 the UN Secretary-General System assessed: hospital and primary care
High-Level Panel on the Global Response to Health Resilience capacity; access to COVID-19 and
Crises,94 and the Global Preparedness Monitoring core health services; resources of
Board 2020 assessment.95,96 healthcare system; equity; and
vaccine deployment.
Our case study framework blends criteria from the
above assessment frameworks to assess the U.S. Scientific Innovation to develop new knowledge
response to COVID-19 (Table 2). To provide depth to Innovation & and technologies, expand existing
our analyses, we have conducted extensive interviews Research knowledge and technologies.
with 23 external experts. We have also reviewed IPPR Attributes assessed: vaccine develop-
documents and press releases, and addressed topics ment; drug development and clinical
specifically suggested by the IPPR. A group of trials; diagnostic test development;
independent reviewers provided comments on our scientific collaboration and innovation;
main conclusions and recommendations. clinical protocol development and
training; and pandemic related global
health research.
The United States’ Response to COVID-19: A Case Study | Chapter 2: Framework for Assessing the U.S. Response | 15Chapter 3: Leadership
Countries that successfully controlled cases and Threats and Biological Incidents (Pandemic Playbook).
deaths due to SARS-CoV-2 responded swiftly, acted Unfortunately, this playbook was not effectively utilized
decisively, created workable strategies, and executed for COVID-19, and the office that housed it, the NSC
well on these strategies.97,98,99,100,101 They did this in an Global Health Unit, had been disbanded in 2018.104
environment of considerable uncertainty where little
was known about this novel pathogen. These countries In mid-2019, the Department of Health and Human
adopted approaches that assumed the worst-case Services (HHS) partnered with key federal and state
scenario: that the virus had already been spreading agencies in a simulation exercise based on a novel
in their countries undetected; that transmission from respiratory pathogen originating in China. Dubbed
asymptomatic and pre-symptomatic cases would be Crimson Contagion, the simulation raised concerns
significant; and that the virus would cause greater mor- about the ability of the U.S. to respond to a pandemic.
bidity and mortality than initially apparent. Successful It unearthed large gaps in coordination across agencies
leaders appreciated that, as in most emergencies, the and problems with domestic capacity to manufacture
risk of doing too little is considerably greater than the necessary vaccines, therapeutics, and personal
risk of doing too much. Rapid, bold and decisive ac- protective equipment (PPE). An After-Action report
tion, even if based on imperfect evidence, is crucial to highlighted the steps needed to respond effectively to
effectively respond to an emerging public health crisis. a future pandemic.105 As of January 2020, when the
virus was first detected in the U.S., none of these
COVID-19 presented a national security threat which steps had been taken.106
successful leaders communicated clearly to their
people, seeking the public’s support for measures that A national response requires coordination of resources,
could cause considerable disruption to millions of lives personnel, expertise, and operational capabilities
and livelihoods. They recognized that to overstate the across multiple government agencies. In the U.S. these
threat, and later be of accused of being alarmist, is agencies rely on different data streams and information
preferable to the opposite. Leadership was an essential systems, and function under the leadership of ever-
element for success in managing the COVID-19 changing political appointees.107 Unlike permanent
pandemic – arguably the most important element – and secretaries in parliamentary democracies who are
one that was glaringly absent in the U.S. response. members of the civil service, leaders of the key
agencies involved in pandemic response are part of the
In this chapter we examine U.S. leadership in two roughly 4,000 political appointments filled by each new
arenas: domestic leadership, and the U.S. role in administration.108 What happened at the national level
global leadership. in this pandemic reflects the decisions of these leaders,
and actions or inactions of their agencies.
Domestic Leadership Slow, Flawed and Political
Structures and Safeguards “No, I’m not concerned at all. No, I’m not.
By some measures the United States was well pre- No, we’ve done a great job.”31
pared to respond to a global pandemic. It ranked first
for pandemic preparedness in the Global Health Se- – President Donald J. Trump, March 7, 2020
curity Index in 2019 and scored highly on International
With immense resources at its disposal, the U.S. did
Health Regulation (IHR) readiness assessments.102,103
not lack qualified or experienced people who knew how
Recognizing the threat posed by emerging infections, to swiftly respond to public health emergencies. What it
previous U.S. administrations had created a playbook did lack was an effective and apolitical body that could
for national public health emergencies: the National rapidly coordinate U.S. government agencies to focus
Security Council (NSC) Playbook for Early Response on the overarching goal of protecting the American
to High Consequence Emerging Infectious Disease public.
The United States’ Response to COVID-19: A Case Study | Chapter 3: Leadership | 16You can also read