VENTILATOR ASSOCIATED PNEUMONIA (VAP)/ VENTILATOR ASSOCIATED EVENTS (VAE) CHANGE PACKAGE - Preventing Harm from VAP/VAE - Hospital Quality Institute
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

VENTILATOR ASSOCIATED PNEUMONIA (VAP)/ VENTILATOR ASSOCIATED EVENTS (VAE) CHANGE PACKAGE Preventing Harm from VAP/VAE

Table of Contents
OVERVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 ORAL CARE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Secondary Driver: Perform regular oral care with an antiseptic solution,
Suggested AIM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 brush teeth, and perform oral and pharyngeal suctioning. . . . . . . . . . . . . . . . 9
Potential Measures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Change Ideas: Routine Oral Care Standardized . . . . . . . . . . . . . . . . . . . . . . 9
Key Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Secondary Driver: Educate the RN staff about the rationale
supporting good oral hygiene and its role in reducing
DRIVER DIAGRAM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 ventilator-associated pneumonia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
“Hardwiring” Oral Care in Improvement Plans . . . . . . . . . . . . . . . . . . . . . . . . . . 9
PREVENTION OF VENTILATOR-ASSOCIATED PNEUMONIA (VAP) . . . . . . 4
POTENTIAL BARRIERS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
SUGGESTED AIMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
TIPS FOR USING THE MODEL FOR IMPROVEMENT . . . . . . . . . . . . . . . . . . . 10
ELEVATE THE HEAD OF THE BED TO BETWEEN 30-45 DEGREES . . . . . . 5
Secondary Driver: Use visual cues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 APPENDIX I: EXAMPLE OF A VAP BUNDLE VISUAL CUE —
Change Ideas: Visual cues for HOB elevation to 30 to 45 degrees . . . . . 5 POSTED AT THE BEDSIDE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Secondary Driver: Identify one person to check for visual cues. . . . . . . . . . . 5
APPENDIX II: EXAMPLE OF A BRIGHT COLORED STRIPE ON
Change Ideas: Include HOB elevation in rounding. . . . . . . . . . . . . . . . . . . . 5 BED FRAME . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Secondary Driver: Include cues/reminders on order sets. . . . . . . . . . . . . . . . . 5
APPENDIX III: EXAMPLE OF A BEST PRACTICE CHECKLIST . . . . . . . . . . . 14
Change Ideas: Utilize reminder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Secondary Driver: Educate patients and their families . . . . . . . . . . . . . . . . . . . 5 APPENDIX IV: SAMPLE SBT/SAT PROTOCOL . . . . . . . . . . . . . . . . . . . . . . . . . 15
“Hardwiring” HOB Elevation in Improvement Plans. . . . . . . . . . . . . . . . . . . . . . 6
APPENDIX V: SAMPLE COMMUNICATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
PEPTIC ULCER DISEASE (PUD) PROPHYLAXIS . . . . . . . . . . . . . . . . . . . . . . . . 6
APPENDIX VI: SAMPLE DELIRIUM PREVENTION PROTOCOL . . . . . . . . . . 17
Secondary Driver: Use of Medications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Change Ideas: H2 Blockers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 APPENDIX VII: SAMPLE SEDATION PROTOCOL . . . . . . . . . . . . . . . . . . . . . . . 18
Secondary Driver: Include PUD on the ICU order sets . . . . . . . . . . . . . . . . . . . 6
APPENDIX VIII: CONFUSION/DELIRIUM ASSESSMENT . . . . . . . . . . . . . . . . 19
Secondary Driver: Engage pharmacy (redundancy, failure remediation). . . 6
Change Ideas: Multidisciplinary approach . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 APPENDIX IX: SAMPLE RASS WORKSHEET . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Secondary Driver: Include PUD Rx on daily checklist . . . . . . . . . . . . . . . . . . . . 6
APPENDIX X: SAMPLE EARLY PROGRESSIVE MOBILITY PROTOCOL . . . 21
Change Ideas: Make it a part of daily rounds . . . . . . . . . . . . . . . . . . . . . . . . 6
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
VENOUS THROMBOEMBOLISM (VTE) PROPHYLAXIS. . . . . . . . . . . . . . . . . . 6
Secondary Driver: Initiate VTE prophylaxis unless contraindicated. . . . . . . . 7
Change Ideas: Standardize with ICU Order Sets . . . . . . . . . . . . . . . . . . . . . 7
Secondary Driver: Interdisciplinary support. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Change Ideas: Team approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Secondary Driver: Include VTE Rx on daily checklist . . . . . . . . . . . . . . . . . . . . 7
“Hardwiring” VTE Prophylaxis in Improvement Plans . . . . . . . . . . . . . . . . . . . . 7
THE ABCDE BUNDLE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Secondary Driver: “A” & “B” — Spontaneous Awakening Trial (SAT)
and Spontaneous Breathing Trial (SBT) Protocols . . . . . . . . . . . . . . . . . . . . . . . 7
Change Ideas: Assess Daily for Readiness and Success with SAT/SBT. . 8
Secondary Driver: “C” — Coordinate SAT and SBT to maximize
weaning opportunities when patient sedation is minimal . . . . . . . . . . . . . . . . 8
Change Ideas: Coordinate and communicate . . . . . . . . . . . . . . . . . . . . . . . . 8
Secondary Driver: “D” — Sedation should be goal oriented . . . . . . . . . . . . . . 8
Change Ideas: Implement a sedation protocol . . . . . . . . . . . . . . . . . . . . . . . 8
Secondary Driver: “E” — Early progressive mobilization and ambulation . . 8
Change Ideas: Early implementation of a progressive mobility protocol . . . 9
“Hardwiring” ABCDE as part of improvement plan . . . . . . . . . . . . . . . . . . . . . . 9
The AHA/HRET HEN would like to acknowledge our partner, Cynosure Health, for their work in
developing the Ventilator Associated Pneumonia (VAP)/Ventilator Associated Events (VAE)
Change Package.
OVERVIEW
Background • The total annual direct medical costs for VAP in United States
• Patients on mechanical ventilation are at high risk for Ventilator hospitals is $1.03 billion to $1.50 billion.
Associated Pneumonia (VAP), with attributable mortality rates
up to 40%. Suggested AIM
• Decrease the rate of VAP to a median state of 0.0/1,000 ventilator
• VAP is the leading cause of death among hospital-acquired
days for at least 6 months by December 31, 2013.
infections, exceeding the death rate due to central line
infections, severe sepsis, and respiratory tract infections Potential Measures
in the non-intubated patient. Outcome: VAP rate (number of VAPs per 1,000 ventilator days)
• VAP also prolongs time spent on the ventilator, the length of ICU for ICU and high-risk nursery (HRN) patients.
stay, and the length of hospital stay after discharge from the ICU.
Process: Ventilator Bundle Compliance (individual bundle
• For 2010, NHSN facilities reported more than 3,525 VAPs; element compliance, all-or-none bundle element
the incidence for various types of hospital units ranged from
compliance)
0.0-5.8 per 1,000 ventilator days.
PRIMARY DRIVERS IDEAS TO TEST
Elevate the Head of • Use visual cues that make it easy to identify when the bed is in the proper position, e.g. a line on the wall that
the Bed to between can only be seen if the bed is below a 30-degree angle.
30-45 degrees. • Include clues on order sets for the initiation of and weaning from mechanical ventilation, for delivery of tube
feedings, and for provision of oral care.
• Create an environment in which respiratory therapists work collaboratively with nurses to maintain
head-of-the-bed elevation.
Peptic ulcer disease • Use medications: H2 blockers are preferred over sucralfate, and proton-pump inhibitors may be efficacious
(PUD) prophylaxis and an alternative to sucralfate or an H2 antagonist.
• Include PUD prophylaxis on the ICU admission and ventilator order sets.
• Incorporate review of PUD prophylaxis into daily multi-disciplinary rounds.
• Engage pharmacy in daily multi-disciplinary rounds to ensure ICU patients are given appropriate PUD and
VTE prophylaxis.
Venous • Initiate VTE prophylaxis on all mechanically-ventilated patients unless contraindicated.
Thromboembolism • Include VTE prophylaxis as part of the ICU admission and ventilator order sets.
(VTE) prophylaxis
ABCDE Bundle • Develop protocols, order sets, and standard work for Spontaneous Awakening Trials (SAT) and
Spontaneous Breathing Trials (SBT), Delirium, Sedation, and Early Progressive Mobility.
• Perform daily assessments of readiness to wean and extubate.
• Create an environment in which respiratory therapists work collaboratively with nurses to facilitate a
daily “sedative interruption” and potential “weaning trial.”
• Implement a protocol to lighten sedation daily to assess for readiness for extubation. Include precautions
to prevent self-extubation such as increased monitoring during the trial.
Oral Care • Perform regular oral care with an antiseptic solution, e.g. Chlorhexidine, in accordance with the
manufacturer’s product guidelines.
• Include daily oral care with Chlorhexidine as part of the ICU admission and ventilator order sets.
• Educate the RN staff about the rationale for supporting good oral hygiene and its potential benefit in
reducing ventilator-associated pneumonia.
Making Changes • CDC Guidelines for Preventing VAP. Retrieved at:
• This intervention is in the Collaborative with Reducing Infec- http://www.cdc.gov/mmwr/preview/mmwrhtml/00045365.htm
tions (Stay FIT Collaborative). National meetings, webinars, • Society of Hospital Medicine Guidelines for Preventing VAP.
monthly coaching calls, change packages and other tools will Retrieved at: http://www.hospitalmedicine.org/AM
augment state hospital association activities. • IDSA and SHEA Compendium on VAP. Retrieved at:
http://www.jstor.org/stable/10.1086/591062
Key Resources • IHI How to Guide Preventing VAP. Retrieved at:
• ABCDE Bundle Tools from AACN. Retrieved at: http://www.ihi.org/knowledge/Pages/Tools
http://www.aacn.org/dm/practice/aacnpearl.aspx?menu=practice
1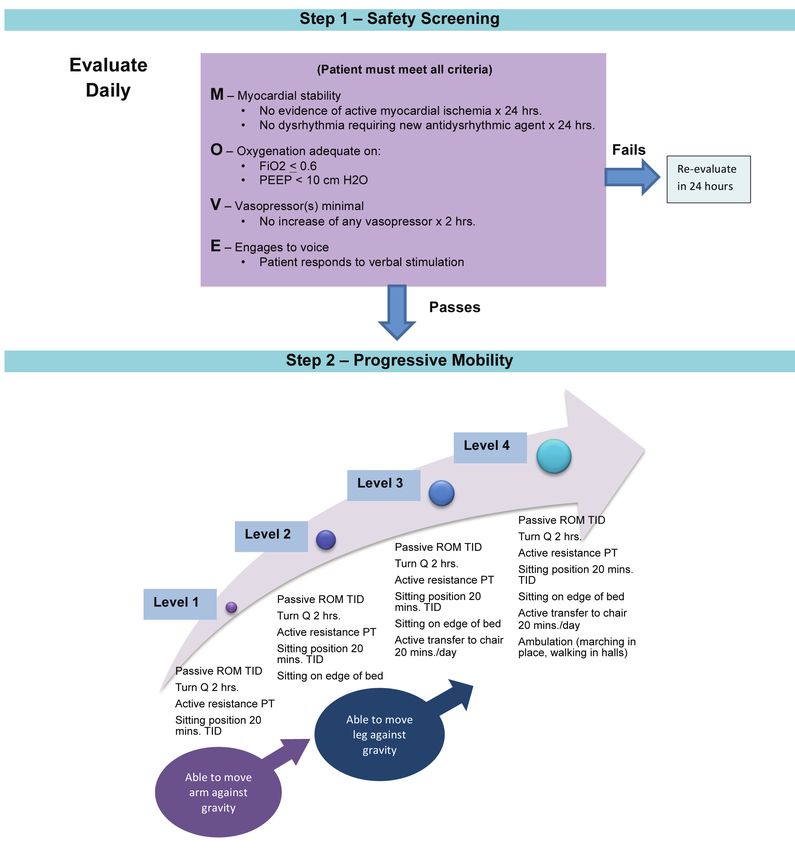
DRIVER DIAGRAM
AIM: Decrease the rate of VAP to a median state of 0.0/1,000 ventilator days for at least 6 months by December 31, 2013.
PRIMARY DRIVERS SECONDARY DRIVERS CHANGE IDEAS
Elevate the Head of • Use visual cues so that it is easy to identify • Use a line (red tape) on the wall that can only be seen
the Bed to between when the bed is in the proper position. if the bed is below a 30-degree angle.
30-45 degrees • Designate one person to check for visual • Assign respiratory therapy staff or a unit assistant to
cues every 1-2 hours in the entire unit. check visual cues every 1-2 hours.
• Include the cues on the order sets for • If using an electronic practice management system,
initiation of and weaning from mechanical institute computer-based pop-up reminders.
ventilation, for delivery of tube feedings, • Include the intervention on nursing flowsheets.
and for provision of oral care. • Discuss during multi-disciplinary rounds.
• Educate patients and their families on the • Include HOB elevation in charge nurse rounds; charge
importance of keeping the head of the nurse can provide just-in-time training.
bed elevated.
Peptic ulcer disease • Use appropriate medications. • H2 blockers are preferred over sucralfate. Proton-pump
(PUD) prophylaxis • Include PUD on the ICU admission and inhibitors may be efficacious, and an alternative to
ventilator order sets. sucralfate or an H2 antagonist.
• Engage pharmacy to ensure ICU patients • Discuss PUD prophylaxis during multi-disciplinary
have appropriate PUD prophylaxis rounds.
(redundancy, failure remediation). • Include PUD prophylaxis in charge nurse rounds; the
• Include PUD Rx on daily checklist. charge nurse can provide just-in-time training and assist
bedside nurses in obtaining orders for PUD prophylaxis.
Venous • Initiate VTE prophylaxis unless • Include VTE prophylaxis as part of your ICU admission
Thromboembolism contraindicated. and ventilator order sets.
(VTE) prophylaxis • Engage the pharmacy to ensure ICU • Include VTE prophylaxis in all ICU rounds; nurse leaders
patients are given appropriate VTE can provide just-in-time training and assist bedside
prophylaxis (redundancy, failure nurses in obtaining orders for VTE prophylaxis.
remediation).
• Include VTE prophylaxis on daily checklist.
ABCDE Bundle • “A & B” – Develop protocols, order sets, and • Perform daily assessments of readiness to wean and
standard work procedures for Spontaneous extubate.
Awakening Trials (SAT) and Spontaneous • Provide a daily reduction or removal of sedative
Breathing Trials (SBT). support.
• “C” – Coordinate SAT and SBT to maximize • Designate one time of the day for the SAT and SBT to
weaning opportunities when patient be attempted.
sedation is minimal.
• Coordinate between nursing and respiratory therapy
• “D” – Sedation should be goal-oriented. to manage SAT and SBT. Use whiteboards, the EMR or
• “E” – Early progressive mobilization and other communication tools to enhance coordination.
ambulation. • Discuss the results of the SAT and SBT during daily
multi-disciplinary rounds.
• The SAT and SBT should be included in nurse-to-nurse
handoffs, nurse-to-charge nurse reports, and charge
nurse-to-charge nurse reports (if they occur).
• Administer sedation as ordered by the physician
according to a scale such as a RASS1 or Modified
Ramsey Score.
• Modify ICU orders to default activity level to
“as tolerated.”
• Implement an early progressive mobility protocol.
2
PRIMARY DRIVERS SECONDARY DRIVERS CHANGE IDEAS
Oral Care • Perform regular oral care with an antiseptic • Include teeth brushing twice a day in order sets for
solution, brush teeth, and perform oral and all ventilated patients.2,3
pharyngeal suctioning. • Include routine oral care every 2-4 hours with an
• Educate the RN staff about the rationale antiseptic mouthwash swab to clean the oral cavity
supporting good oral hygiene and its and teeth.
potential benefit in reducing ventilator- • Use Chlorhexidine 0.12% mouthwash at least daily
associated pneumonia. (many studies cite every 12 hours) as part of order
sets for all ventilated patients.4
• Create visual cues (e.g. empty holders of oral care
products) to indicate compliance with oral care.
• Include Respiratory Therapy in performing oral care,
make it a joint RN and RT function.
FOOTNOTES
1
Richmond Agitation Sedation Scale (RASS)
2
Munro CL, Grap MJ, Jones DI, McClish DK, Sessler CN. Chlorhexidine, tooth brushing and
preventing ventilator-associated pneumonia in critically ill adults. Am J Crit Care. 2009;
18(5):428-437.
3
Garcia R, Jendresky L, Colbert L, Bailey A, Zaman M, Majumder M. Reducing
ventilator-associated pneumonia through advanced oral-dental care: A 48-month study.
Am K Crit Care. 2009; 18(6):523-532.
4
Chan EY, Ruest A, O’Meade M, Cook DJ. Oral decontamination for prevention of
pneumonia in mechanically ventilated adults: Systematic review and meta-analysis.
Brit Med J. 2007; 10:1136.
3PREVENTION OF VENTILATOR-ASSOCIATED NOTE: The VAE algorithm is for use in surveillance, not as a
PNEUMONIA (VAP) clinical definition algorithm and is not intended for use in the
Mechanically ventilated patients are at high risk for complications clinical management of patients. The VAE algorithm is only
such as ventilator-associated pneumonia (VAP), peptic ulcer applicable to mechanically-ventilated patients > 18 years of age.
disease (PUD), gastrointestinal bleeding, aspiration, venous There are three definitions/tiers in the VAE algorithm:
thromboembolic events (VTE), and problems with secretion
1. Ventilator-Associated Condition (VAC);
management. Evidence-based interventions can reduce the risk
and incidence of these complications. For example, implementa- 2. Infection-Related Ventilator-Associated Complication
tion of the ventilator bundle has been shown to reduce VAP.1 (IVAC); and
The VAP prevention bundle includes: head of bed elevation to 3. Possible and Probable VAP.
30 to 45 degrees, oral care with Chlorhexidine 0.12%, peptic VAE ALGORITHM
ulcer prophylaxis, deep vein thrombosis (DVT) prophylaxis, and
spontaneous awakening trials and breathing trials. This guide
presents evidence-based practices to promote VAP reduction. Patient on mechanical ventilation > 2 days
Ventilator-Associated Events (VAE) Surveillance
Baseline period of stability or improvement,
Ventilator-associated pneumonia has been problematic to identify followed by sustained period w
eriod of worsening oxygenation
because commonly used definitions for VAP include subjective
criteria that are neither sensitive nor specific for VAP. The Ventilator-Associated
ated Co
Condition (VAC)
previous surveillance definition included: a combination of x-ray,
signs/symptoms and laboratory criteria. Three specific sets of General, objective evidence
nce of in
infection/inflammation
PNEU criteria are available for a PNEU to be counted as a VAP:
the endotracheal tube (ETT)/ventilator must have been in place
Infection-Related Ventilator-Associated
A i Complication (IVAC)
(1) at some time during the preceding 48 hours or (2) at the time
of the PNEU onset; and (3) there was no required amount of time
Positive results of laboratory/microbiological
ratory/m testing
that the ETT/ventilator must have been in place. Major limitations
of the former VAP definitions are:
• these VAP definitions rely on complex multiple and sometimes Possible or Probable
Probab VAP
subjective pathways;
• no valid, reliable definition for VAP exists; This algorithm takes into account research that to date has sug-
• the criteria that do exist are neither sensitive nor specific; and gested that most VACs are due to pneumonia, ARDS, atelectasis,
• they require radiographic findings of pneumonia whereas and pulmonary edema. These significant clinical conditions
evidence-based research suggests chest radiographic findings may be preventable. The definition of VAE states: “VAEs are
are not diagnostic for VAP. identified by using a combination of objective criteria: deteriora-
These limitations have implications for prevention. tion in respiratory status after a period of stability or improvement
In January 2013, the Centers for Disease Control (CDC) on the ventilator, evidence of infection or inflammation, and
released a new approach to surveillance for Ventilator-Associated laboratory evidence of respiratory infection.”2 The full document
Events (VAE) for the National Healthcare Safety Network can be retrieved at: http://www.cdc.gov/nhsn/PDFs/pscManual/
(NHSN). Surveillance has been limited to Ventilator-Associated 10-VAE_FINAL.pdf
Pneumonia to date. This new VAE Surveillance was designed to
SUGGESTED AIMS
address the limitations of the former VAP definitions including
An AIM statement for VAP reduction efforts could include one of
the NHSN PNEU.
the following:
The new VAE surveillance definition algorithm has been founded
• Decrease the rate of VAP to a median state of 0.0/1,000 ventilator
on objective, streamlined, and potentially automatable criteria. It
days (or mean state• Decrease the rate of VAP by 50% within 9 months and achieve and the charge nurse, is essential to ensure preventive measures
a rate of 0.0/1,000 ventilator days by December 31, 2013. such as elevated HOB are adhered to. (See Appendix III for an
• Decrease the rate of VAP by implementing all elements of the example of a Best Practices Checklist).
Ventilator Bundle for more than 95% of ventilator patients Change Ideas: Include HOB elevation in rounding
in the ICU by December 31, 2013. • Assign respiratory therapy staff or a unit assistant to look
ELEVATE THE HEAD OF THE BED TO BETWEEN out for visual cues every 1-2 hours.
30-45 DEGREES • If using an electronic practice management system, institute
Angling the head of the bed to between 30 to 45 degrees is a computer-based pop-up reminders.
simple nursing measure that has resulted in VAP reduction. • Include interventions on nursing flowsheets.
Keeping the head of the bed (HOB) elevated has been shown to
• Include HOB elevation in charge nurse rounds, if performed;
help prevent aspiration of gastric contents and secretions3,4,5,6
the charge nurse can provide just-in-time training as needed.
• Process Measure: Daily audit of HOB elevation compliance, • Promote an environment in which respiratory therapists
and documentation of contraindications. work collaboratively with nursing staff to maintain head-of-
Secondary Driver: Use visual cues. the-bed elevation.
Visual cues are important to remind staff to elevate the HOB. • If HOB elevation is contraindicated, communicate and
A visual cue can also act as a guide to show staff how steep 30 to document the rationale.
45 degrees should be; staff often underestimate the angle of the Secondary Driver: Include cues/reminders on order sets
HOB. One research study found that HOB angle was perceived Research suggests that standardized order sets can be effective
correctly by only 50 to 86% of clinicians.7 in improving compliance with evidence-based practices such
Change Ideas: Visual cues for HOB elevation to 30 to as ventilator bundles for VAP reduction, improved stroke care,
45 degrees and sepsis. Standardized order sets have been shown to increase
Engage staff nurses to develop visual cues that work for their patient safety and improve outcomes for multiple patient
environment and work flow (See Appendix I for an example of a conditions.10,11,12,13
VAP Bundle Visual Cue). Standardizing the process of care has
Change Ideas: Utilize reminders
been shown to increase the number of patients who are placed
• If using an electronic practice management system, institute
in a semi-recumbent position.8 Examples of visual cues include:
computer-based pop-up reminders.
• Using a line (red tape) on the wall that can only be seen if the
• Discuss procedures during multi-disciplinary rounds to ensure
bed is below a 30-degree angle.
that all of the bundle components have been implemented.
• Cutting a piece of cardboard in the shape of a slice of pizza,
• Allow physicians to “opt-out” if the bundle or one of its elements
i.e. a 30 degree triangle.9
is contraindicated. Ask the physician to help improve bundle
• Placing a red stripe on the bedframe at a 30 degree angle.
by communicating and documenting the rationale for why the
When the HOB is at 30 degrees, the red stripe will appear
intervention is not appropriate for the patient.
to be parallel to the floor (See Appendix II for an example
of a Red Stripe on Bed Frame). Secondary Driver: Educate patients and their families
• Including the interventions on nursing flowsheets. Families can be invited to participate in care. Education of families
about the risks of VAP and how caregivers can mitigate those risks
• Incorporating HOB elevation into the standardized order set.
allow the family to feel involved and connected. Families can also
Secondary Driver: Identify one person to check for be asked to help keep the HOB elevated to 30 to 45 degrees, by,
visual cues.
for example, reminding staff to elevate the HOB after linen
The environment of an intensive care unit is a busy and stressful changes. Consumer groups are also encouraging patient’s families
one. Caregivers are confronted with multiple stimuli making to partner with hospital staff to keep their loved ones safe.14
demands for attention. Engagement of the entire team, including
bedside nurses, intensivists, nurse’s aides, respiratory therapists,
5“Hardwiring” HOB Elevation in Improvement Plans Secondary Driver: Engage pharmacy (redundancy,
Hardwiring for HOB includes routine reminders to help the failure remediation).
intervention to become part of daily care, such as: Asking the pharmacy to support your program will add a layer
• Including HOB elevation on the daily audit checklist. of redundancy to improve reliability and promote opportunities
for earlier detection of failure patterns. A pharmacist as part of
• Including the intervention on nursing and respiratory
interdisciplinary rounds is cost-effective and can improve safety.
care flowsheets.
Pharmacists can produce reports from the Pharmacy Information
• Incorporating HOB elevation into standardized order sets.
System that can positively affect care and can consult with physi-
• If using an electronic practice management system, instituting cians as medically appropriate.
computer-based pop-up reminders.
Change Ideas: Multidisciplinary approach
• Including HOB elevation in charge nurse rounds, so charge
nurse can provide just-in-time training. • Discuss procedures and interventions during multidisciplinary
rounds
• Promoting an environment where respiratory therapists work
• Consider producing a pharmacy exception report for
collaboratively with nursing staff to maintain HOB elevation.
PUD prophylaxis
PEPTIC ULCER DISEASE (PUD) PROPHYLAXIS
• Include a pharmacist on ICU multidisciplinary rounds
Critically ill patients requiring mechanical ventilation are at in-
creased risk for stress ulcers and subsequent gastrointestinal Secondary Driver: Include PUD Rx on daily checklist
bleeding. Additionally, bacterial colonization of the stomach Change Ideas: Make it a part of daily rounds
can lead to infection of the respiratory tract through aspiration • Include PUD prophylaxis in charge nurse rounds, if charge
of stomach secretions.16 nurses are utilized. A charge nurse can provide just-in-time
• Process Measure: Daily audit of PUD prophylaxis compliance training and assist bedside nurses in obtaining orders for
or documented contraindications. PUD prophylaxis.
“Hardwiring” PUD Prophylaxis into the Improvement Plan
Secondary Driver: Use of Medications.
To hardwire PUD prophylaxis, make the process of ordering PUD
To reduce PUD risk, mechanically-ventilated patients should
prophylactic medications as routine as possible. If such orders are
receive PUD prophylaxis.17
contraindicated, then the rationale should be communicated and
Change Ideas: H2 Blockers documented. Methods for hardwiring include:
• H2 blockers are preferred over sucralfate. Proton-pump • Including PUD prophylaxis in order sets.
inhibitors (PPI) may be efficacious, and serve as an • Including PUD prophylaxis on the daily audit checklist.
alternative to sucralfate or an H2 antagonist.18
• Reviewing the need for PUD prophylaxis during multi-
• Discuss interventions during multi-disciplinary rounds. disciplinary rounds.
• Include a clinical pharmacist on the care team to guide • Including as a standing item in nurse-to-nurse hand-off reports.
complex cases.
VENOUS THROMBOEMBOLISM (VTE) PROPHYLAXIS
Secondary Driver: Include PUD on the ICU order sets.
Mechanically-ventilated patients are at high risk for VTE. Risk
Requiring PUD prophylaxis on both ICU admission and ventilator
factors include immobility and a stress inflammatory response
order sets will standardize the treatment. However, allow physi-
resulting in hypercoagulation. Although there is no evidence to
cians to “opt-out” when clinically appropriate, and ask them to
suggest VTE prophylaxis reduces VAP risk, it is appropriate to
communicate and document the reasons for the “opt-out” to
include VTE prophylaxis in a bundle that promotes improved care
promote learning and understanding among the healthcare team.
of mechanically-ventilated patients due to their high risk for VTE.19
Audit how frequently physicians “opt-out” to observe if there are
any patterns (e.g. certain types of patients, specific physicians) • Process Measure: Daily audit of VTE prophylaxis compliance
that might suggest that a change to the order set or another or documentation of contraindications.
intervention is necessary.
6Secondary Driver: Initiate VTE prophylaxis THE ABCDE BUNDLE
unless contraindicated. The ABCDE Bundle extends the original VAP Bundle and its HOB,
All high risk patients should have pharmacological VTE PUD prophylaxis, VTE prophylaxis, and oral care interventions.
prophylaxis unless it is contraindicated due to bleeding risk. The ABCDE Bundle was developed to improve the health of venti-
For patients with severe bleeding risk, mechanical prophylaxis lated patients by reducing their risk of oversedation, immobility,
is recommended unless contraindicated due to the patient’s and mental status changes.
condition. Intermittent pneumatic compression (IPC) is The bundle approach provides a means to incorporate evidence-
preferred for mechanical prophylaxis.20 The addition of based interventions into patient care. Bundles are not meant
mechanical prophylaxis to pharmacological prophylaxis has to be rigid recipes for the care of ventilated patients; providers
shown some benefits in VTE reduction.21 should assess which components of a bundle would be appropriate
Change Ideas: Standardize with ICU Order Sets for each individual patient. “The ABDCDE bundle includes
• Include VTE prophylaxis in the ICU admission order set and spontaneous awakening and breathing trial coordination, careful
the ventilator order set. sedation choice, delirium monitoring, and early progressive
• Allow physicians to “opt-out” with appropriate patients, and mobility and exercise. The intent of combining and coordinating
ask that the rationale for the “opt-out” be communicated and these individual strategies is to ‘(1) improve collaboration among
documented. clinical team members, (2) standardize care processes, and (3)
break the cycle of over sedation and prolonged ventilation, which
Secondary Driver: Interdisciplinary support.
appear causative to delirium and weakness.23,24
Engage pharmacists to ensure ICU patients have been given
ABCDE Bundle components include:
appropriate VTE prophylaxis and to review pharmacotherapy on
interdisciplinary rounds. A – Awakening trials for ventilated patients
B – Spontaneous Breathing trials
Change Ideas: Team approach
C – RN and respiratory therapist Coordination to perform
• Include VTE prophylaxis in ICU rounds; nurse leaders can
spontaneous breathing trials by reducing or stopping
provide just-in-time training and assist bedside nurses in
sedation so as to awaken the patient
obtaining orders for VTE prophylaxis.
D – Standard Delirium assessment program, including
• Consider creation of a pharmacy exception report to determine
treatment and prevention options
if appropriate VTE prophylaxis is being provided.
E – Early mobilization and ambulation of critically ill
Secondary Driver: Include VTE Rx on daily checklist patients.25,26,27
“Hardwiring” Standardize Interventions for Patients at Secondary Driver: “A” & “B” — Spontaneous Awakening
Risk for Falling in Improvement Plans Trial (SAT) and Spontaneous Breathing Trial (SBT)
Hardwiring strategies for VTE prophylaxis are similar to those for Protocols.
PUD prophylaxis. Making the process as routine as possible will Sedation in the mechanically ventilated patient may be necessary
assure that VTE prevention is addressed for every mechanically- to control anxiety, reduce pain, and control oxygenation needs.
ventilated patient. However, the use of sedation can prolong the duration of
• Include VTE prophylaxis in the ICU admission and ventilator mechanical ventilation. Patients receiving sedation should have
order sets. a neurological assessment daily, in which the patient’s sedation is
• Include VTE prophylaxis on the daily audit checklist. withheld until the patient is able to follow commands or until the
• Include VTE prophylaxis in multi-disciplinary rounds. patient becomes agitated. Daily screening of respiratory function
using trials of daily awakening and spontaneous breathing has
• Utilize the pharmacy to review all patients or to produce
been shown to reduce the duration of mechanical ventilation
exception reports to ensure adequate and appropriate
and the risk of VAP.28,29,30
prophylaxis.
• Include VTE prophylaxis as a standing item in nurse-to-nurse
hand-off reports.
7• Process Measure: Daily audit of SAT/SBT compliance Secondary Driver: “D” — Sedation should be goal
and documentation of rationale for non-compliance oriented.
(e.g. contraindications) Sedation typically assists in the pulmonary recovery of patients.
However, too little sedation can lead to increased anxiety,
The use of non-physician staff-driven protocols has been found increased work of breathing, a drop in blood and tissue oxygena-
to be very effective in assessing readiness to wean from the tion, and self extubation. Too much sedation can lead to decreased
ventilator--and have demonstrated a reduction in VAP.31 By respiratory muscle function, prolonged neurological depression,
developing staff-driven protocols and incorporating SAT and and the inability to wean from mechanical ventilation. The use
SBT into the daily care of the ventilator patient, patients will of a sedation algorithm or scale, such as the RASS, to monitor
experience fewer days on the ventilator and a shorter ICU stay.32,33 the level of sedation will help to reduce over-sedation, deliver
(See Appendix IV for a link to a suggested protocol). the most effective dose, and reduce mechanical-ventilation
Change Ideas: Assess Daily for Readiness and Success duration.34,35 (See Appendix VI for a sample Delirium Prevention
with SAT/SBT protocol and Appendix VII for a sample Sedation protocol).
• Determine if a patient meets the SAT criteria with
Change Ideas: Implement a sedation protocol
no contraindications.
• Assess patients at least daily for confusion/delirium.
• Decrease or stop sedation per the SAT protocol (nurse).
(See Appendix VIII for an assessment algorithm).
• Determine if patient meets SBT criteria with no
• Administer sedation as ordered by the physician, according to
contraindications.
a scale such as a RASS, SAS or Modified Ramsey Score. These
• Perform an SBT per the protocol (respiratory therapist).
scores help standardize communications, are more accurate, and
• Perform daily assessments of readiness to wean and extubate take less time than qualitative descriptions of level of sedation.
based on the SAT/SBT results. (See Appendix IX for a sample RASS worksheet).
Secondary Driver: “C” — Coordinate SAT and SBT to • Assess at least daily if the target RASS/Modified Ramsey/SAS
maximize weaning opportunities when patient sedation goal is met. If not, audit and analyze the reasons for missing
is minimal.
the target.
Nursing and Respiratory Therapy must work as a team to ensure
patient safety and to address the selected VAP prevention bundle Secondary Driver: “E” — Early progressive mobilization
interventions. SBTs will fail if the patient has too much sedation and ambulation.
to allow for “spontaneous” awakening or breathing. Many research studies have explored ICU-acquired weakness,
the acute onset of neuromuscular/functional impairment in the
Change Ideas: Coordinate and communicate critically ill for which there is no plausible cause other than
• Provide a daily reduction in or removal of sedative support. critical illness.36,37,38 This weakness impairs ventilator weaning
• Designate a time of the day that the SAT and SBT will be and functional mobility and can persist well after hospital dis-
attempted that allows for periods of patient rest. (See charge. Early progressive mobility can mitigate this neuromuscular/
Appendix V for a sample of Communication of Rest Period). functional impairment and reduce the inherent risks of immobility
• Determine how often SBTs have failed due to high levels such as VAP, hospital-acquired pneumonia, prolonged length-
of sedation. of-stay, skin breakdown, delirium incidence, and decreased
cardiovascular function.40,41 “Progressive mobility is defined
• Coordinate between nursing and respiratory therapy to
as a series of planned movements in a sequential manner
manage SAT and SBT. Use whiteboards, the EMR, or
beginning at a patient’s current mobility states/levels with a
other communication tools to enhance coordination.
goal of returning to his/her baseline.” 42 (See Appendix X for a
• Discuss the results of a patient’s SAT and SBT during
sample Mobility protocol).
daily multi-disciplinary rounds.
• The SAT and SBT results should be included in nurse-to-
nurse hand-offs, nurse-to-charge nurse reports, and charge
nurse-to-charge nurse reports.
8Change Ideas: Early implementation of a progressive • Include routine oral care (at least every 2-4 hours) with an anti-
mobility protocol septic mouthwash swab to clean the oral cavity and teeth.48
• Modify standardized ICU admission orders to change the default • Order Chlorhexidine 0.12% mouthwash at least daily (many
activity level from “bed rest” to “as tolerated.” studies cite every 12 hours) for all ventilated patients.49,50,51
• Establish and disseminate simple guidelines for physical and oc- • Create visual cues (e.g. empty holders of oral care products;
cupational therapy consultations. by dating and timing products) to demonstrate compliance
• Incorporate the ABCDE bundle into standing orders as a default with oral care.
order making it a daily part of care; provide “opt-outs” for pa- • Engage Respiratory Therapy in the performance of oral care;
tients for whom the bundle or its individual elements are con- make it a joint RN and RT function.
traindicated. • Use a whiteboard to document the delivery of oral care;
“Hardwiring” ABCDE as part of improvement plan omissions make procedure failure obvious.
To hardwire SAT/SBT, incorporate the intervention into the daily Secondary Driver: Educate the RN staff about the ration-
workflow by: ale supporting good oral hygiene and its role in reducing
• Implementing protocols for non-physician staff for daily ventilator-associated pneumonia
SAT/SBT. Institution of the ventilator bundle does not by itself guarantee a
decrease in VAP. A decrease in VAP is more likely to occur when
• Including SAT and SBT protocols on order sets.
compliance with the bundle is audited and staff are provided with
• Including SAT and SBT protocols on daily audit checklists.
routine feedback and coaching.52,53
• Including SAT and SBT protocols on nursing and respiratory
care flowsheets. “Hardwiring” Oral Care in Improvement Plans
• Including SAT and SBT protocols as a standing item in nurse-to- Multi-focal options for “hardwiring” include:
nurse hand-off reports. • Incorporating oral care in order sets.
• Managing protocol implementation in smaller steps and antici- • Including oral care on nursing care flowsheets.
pating staff fears about patient self-extubation. Research litera- • Visibly documenting that oral care has been provided.
ture suggests that self-extubation is slightly higher with • Involving the patient’s family, if appropriate.
SAT/SBTs, but re-intubation rate is lower in the SBT/SAT group;
POTENTIAL BARRIERS
indicating that many patients were ready for extubation.43,44
• Clinicians may believe that they are complying with these
activities, especially if the VAP rate is low, but documentation
ORAL CARE
of bundle compliance is critical to ensure reliability of these
Oral care may seem simple, but can be challenging to implement.
interventions. Monitoring to confirm compliance includes:
Swabbing a patient’s mouth with an antiseptic mouthwash has
— Checking 5 ventilated patients to determine bundle
been recommended for comfort, but recent studies have demon-
compliance for each element.
strated that oral care with an antiseptic has also reduced the risk
for VAP. — Was the sedative infusion truly turned off and, if so, for
how long?
• Process Measure: Daily audit of oral care compliance. — Was the infusion restarted at the same dose or was the
Secondary Driver: Perform regular oral care with an dose lowered if possible?
antiseptic solution, brush teeth, and perform oral and — If an intermittent pneumatic compression device was
pharyngeal suctioning.
used for mechanical VTE prophylaxis, was it actually
Oral care is a basic task that can positively impact operating/functioning?
VAP prevention.45
— Was staff documentation of ordering and administering
Change Ideas: Routine Oral Care Standardized medications for PUD and VTE prophylaxis appropriate?
• Teeth brushing twice a day in order sets for all ventilated
patients.46,47
9• Recognize that many physicians will perceive these • Utilize respected senior physician as an “opinion leader” to trial
interventions as a change in their practice. these changes in his or her local unit, and then advocate for
— Traditionally, ventilation weaning and sedation were part of organization-wide adoption of successful best practices.
the physician’s role, not inter-dependent functions Don’t just change the practice, change the culture
implemented by non-physician staff. Select respected lead • Instituting the VAP bundle will require a change in culture,
physicians to serve on the improvement team and advocate particularly among physicians, who will be asked to trade their
as champions with physician colleagues to discuss and traditional approach of individualizing mechanical ventilation
implement these changes. Order sets and protocols are management for each patient for a standardized and more effec-
seen by some physicians as “cookbook” medicine. Reframe tive approach. Physicians may be concerned about the perceived
these interventions as “best recipe” medicine that uses loss of control and the risks of shared responsibility; encourage
research findings to suggest improved and individualized physicians to actively monitor the effectiveness of therapy and
patient care options to reduce the risk of VAP. the overall condition of the patient.
— Clinicians may define tasks as “ours” and “theirs.” Examples • Many physicians prefer to learn from peers rather than simply
include: oral care is a nursing task, medications are the to follow “expert advice.” Use lead physicians as peer educators
responsibility of the physician, and ventilators are managed to advocate for the adoption of improvements such as order sets.
by the respiratory therapist. Include key stakeholders such
• Nurses and respiratory therapists may be uncomfortable
as physicians, bedside nurses, and respiratory therapists on
implementing a staff-driven protocol independent of
improvement teams to collaborate in the development of
physicians, and have little experience collaborating with
protocols, workflows, and peer education programs.54,55
other health professionals. Educate staff about the expertise
• These processes may be new territory for many physicians, and roles of their colleagues and provide opportunities for
nurses, respiratory therapists, and pharmacists. Nurses and res- collaboration on the development of the new protocols.
piratory therapists, for example, may be concerned that they
• Begin the trial with a small test of change in one unit or area
may make a mistake and that patients may self extubate during a
and then disseminate successful results more widely across
SAT/SBT trial. They may fear confrontations or resistance from
the organizations. The ideal outcome is the development of
the medical staff. To mitigate these concerns:
team-based care wherein each member of the team (physician,
— Educate all healthcare providers about the proven nurse, respiratory therapist) contributes to improved patient
methodologies to reduce the risks and incidence of VAP. quality of care.
— Share evidence and experience from similar hospitals
TIPS ON USING THE MODEL FOR IMPROVEMENT
which demonstrate successful implementation of these
processes without complications such as self-extubations. • Implement the VAP Bundle one element at a time.
—Begin with a bundle element that will be easy to trial and
Use administrative leadership and sponsorship to help
remove or mitigate barriers
will likely be successful and have significant positive impact.
• Begin implementation with an early adopter physician who can For example, implementing HOB elevation is less complicated
lead and recruit other early adopter champions from among than implementing SAT/SBT protocols yet greatly reduces
specialty groups and intensivists. VAP risk.
• Enlist an executive sponsor who recognizes the value to the • Testing SAT/SBT protocols
organization and its patients of preventing VAP, and who can — Step One: Plan –
provide solutions and resources to address concerns about • Do not reinvent the wheel. Use a protocol that has been
the burdens of new processes for hospital staff. An executive successful at another hospital and adapt it your facility.
sponsor can help to staff see the “big picture” on how these • Test one step at a time. Do not plan to implement all of
changes may benefit the entire organization and advocate for the ABCDE recommendations at once. Concentrate first
necessary funding, staffing, and supplies, provide bridges over on the ABC, and then add the D and E.
implementation barriers, and educate relevant stakeholders
and the governing board.
10— Step Two: Do –
• Ask a receptive, early-adopter physician on your
improvement committee to trial these changes with her
next few patients on ventilation.
• Ask a receptive nurse and respiratory therapist on your
committee to trial the protocols as well.
• Test “small”: Coordinate with the physician champion to
trial the protocol on one patient, with one nurse and one
respiratory therapist.
— Step Three: Study –
• Debrief as soon as possible after the test with those
involved, asking:
• What happened?
• What went well?
• What didn’t?
• What do we need to revise for next time?
— Step Four: Act –
• Do not wait for the next committee meeting to make
changes. Revise and re-test with the same physician,
the same nurse, and the same respiratory therapist.
11APPENDIX I: Example of a VAP Bundle Visual Cue – Posted at the Bedside
ICU BEST PRACTICE for VENTILATED PATIENTS
Head of bed up to 30-45 degrees
Enteral feeding and q 2 hour oral care
Air mattress and turn q 2 hour
DVT prophylaxis
Sedation vacation
Ulcer prophylaxis
Pain control
12Appendix II: Example of a Bright-Colored Stripe on Bed Frame
13Appendix III: Example of a Best Practice Checklist
ICU BEST PRACTICE AUDIT/REPORT
Date:
IF INTUBATED OR TRACHED
BED NOT Patient # Central Pediatrician Hypothermia BGM over Sepsis Sepsis Meets CVS Patient INTUBATED TF/TPN HOB m Oral Care Chlorhexidine
ICU MR # Lines Notified & Temperature goal 200 write Meets CVS Fluid Goal Intake & 30"– 45" Yes q 2h Oral Rinse q
Status (include Documented reached within 30 note below Goal >8 1.5 – 2.5L Output goal circle shift, 12H
PICCs) minutes and maintained for follow up initial achieved No X out shift
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
Y N Y N Y N N D E Y N Y N
14Appendix IV: Sample SBT/SAT Protocol
The “Wake Up and Breathe” protocol pioneered by Vanderbilt University can be found at:
http://www.mc.vanderbilt.edu/icudelirium/docs/WakeUpAndBreathe.pdf
15Appendix V: Sample Communication
I AM GETTING MY
ZZZZZZZZZZZ
SLEEP CYCLE IN PROGRESS
DO NOT DISTURB
PLEASE CHECK WITH NURSE BEFORE ENTERING
16Appendix VI: Sample Delirium Prevention Protocol
DELIRIUM PREVENTION PROTOCOL
DAYTIME NIGHTTIME
a. Provide visual and hearing aids during daytime.
PM Care — begin between 2100-2200
b. Encourage communication and reorient the patient
a. Ask the patient if toileting is needed (bedpan,
frequently.
bathroom, bedside commode, etc.).
i. Ensure the room calendar is up-to-date.
b. Perform oral care (toothbrush, mouth moisture, with
ii. Introduce oneself with each encounter, providing assistance or independently); assist the patient in
the current date and time and explaining what will washing his face and hands; perform back care or
be done, and giving the patient choices regarding massage with warmed lotion); offer earplugs.
his or her care whenever possible.
c. Ask “Do you take or do anything at home to help
c. Have the family bring in a few familiar objects from you sleep? Do you sleep with white noise (fan, TV,
home to display in the patient’s room. music)?”
d. Ask the patient/family if they watch television, and, d. Ensure the call light is within reach and the bed is in
if so, what shows they prefer. Provide the patient with the low position; close the shades, dim the lights,
these choices, as well as with daily news on TV close the door (except in the MICU), put the bedside
or radio. charts outside of the room, and put the “sleep cycle
in progress” sign on the door.
e. Provide non-verbal music or opt for the patient’s
preference. e. Minimize noise inside and outside of the room.
f. Open shades and keep lights on during the day. f. Allow for minimum of 2 hours of uninterrupted sleep,
allowing for a full 90-minute sleep cycle; remove the
g. Provide an uninterrupted rest period in the afternoons
automatic BP cuff; enter the room with a flashlight
between 1-3pm.
or low lighting to perform necessary activities.
h. Minimize use of physical restraints (including lines
i. If patient has been hemodynamically stable in
and tubes).
the previous 24 hours, explore extending the
i. Provide early and progressive mobility. uninterrupted sleep period to 4 hours (but only
for patients who are unrestrained and can turn
themselves)
17Appendix VII: Sample Sedation Protocol
18Appendix VIII: Confusion/Delirium Assessment
CONFUSION ASSESSMENT METHOD IN THE ICU
19Appendix IX: Sample RASS Worksheet
RASS WORKSHEET
20Appendix X: Sample Early Progressive Mobility Protocol
EARLY PROGRESSIVE MOBILITY PROTOCOL
Website. Retrieved at: http://www.aacn.org/wd/nti/nti2012/docs/pearl/early%20exercise%20and%20progressive%20mobility/
early-progressive-mobility-protocol.pdf
21REFERENCES
1 30
Bird D, Zambuto A, O’Donnell C, et al. Adherence to ventilator-associated pneumonia Brook AD, Ahrens TS, Schaiff R, et al. Effect of a nursing-implemented sedation
bundle and incidence of ventilator associated pneumonia in the surgical intensive care protocol on the duration of mechanical ventilation. Crit Care Med 1999; 27(12):2824-2825.
unit. Arch Surg. 2010;145(5):465-470. 31
Dries DJ, McGonigal M, Malian MS, Bor B, Sullivan C. Protocol driven ventilator weaning
2 reduces use of mechanical ventilation, rate of early reintubation, and ventilator-associated
Center for Disease Control Device-associated Events: VAE. Retrieved at:
http://www.cdc.gov/nhsn/PDFs/pscManual/10-VAE_FINAL.pdf pneumonia. J Trauma-Inf Crit Care. 2004;56(5):943-952.
3 32
AACN practice alert: ventilator-associated pneumonia. AACN Clin Issues. 2005;16(1): Ely W, Meade MO, Haponik EF, et al. Mechanical ventilator weaning protocols driven
105–109. by nonphysician health-care professions: Evidence-based clinical practice guideline.
4 Chest 2001; 120(6)454S-463S.
Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body
33
position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: Brook AD, Aherns TS, Schaiff R, et al. Effect of a nursing-implemented sedation
a randomized trial. Lancet. 1999; 354(9193):1851-1858. protocol on the duration of mechanical ventilation. Crit Care Med 1999;27(12):2824-2825.
5 34
Collard HR, Saint S, Matthay MA. Prevention of ventilator-associated pneumonia: DeJonghe B, Bastuji-Garin S, Fangio P, et al. Sedation algorithm in critically ill patients
an evidence-based systematic review. Ann Intern Med. 2003;138(6):494–501. without brain injury. Crit Care Med. 2005;33(1):120-127.
6 35
Torres A, Serra-Batilles J, et al. Pulmonary aspiration of gastric contents in patients Quenot JP, Ladoire S, Devoucoux F, et al. Effect of a nurse-implemented sedation
receiving mechanical ventilation: the effect of body position. Ann Intern Med. 1992; protocol on the incidence of ventilator-associated pneumonia. Crit Care Med.
116(7):540-543. 2007;35(9):2031-2036.
7 36
Hiner, C, Kasuya T, Cottingham C, Whitney J. Clinicians’ perception of head-of-bed E-Early Exercise and Progressive Mobility. Session Notes from NTI 2012 (ABCDE
elevation. Am J Crit Care. 2010;19(2):164-167. Bundle). Accessed October 30, 2012. Retrieved at: http://www.aacn.org/wd/nti/
8 nti2012/docs/pearl/early%20exercise%20and%20progressive%20mobility/
Helman DC Jr, Sherner JH 3rd, Fitzpatrick TM, Callendar ME, Shorr AF. Effect of
early-mobility-nti-session-notes.pdf
standardized orders and provider education on head-of-bed positioning in
37
mechanically ventilated patients. Crit Care Med. 2003;31(9):2285-2290. Stevens RD, Marshall SA, Cornblath DR, et al. A framework for diagnosing and
9 classifying intensive care unit acquired weakness. Crit Care Med.
Landor N, Charrvat P. VAP: It’s the little things that count. PSQH 2010 Nov – Dec.
2009;37(10)(suppl):S299-S308.
10
Panella M, Marchisio S, Di Stanislao F. Reducing clinical variations with clinical 38
Bolton CF, Gilbert JJ, Han AF, Sibbald WJ. Polyneuropathy in critical ill patients.
pathways: Do pathways work? Int J Qual Health Care. 2003;15:509–521
J Neurol Neurosurg Psychiatry. 1984;47(11):1223-1231.
11
Abbot CA, Dremsa T, Stewart DW, Mark DD, Swift CC. Adoption of a ventilator- 39
Bercker S, Weber-Carstens S, Deja M, et al. Intensive insulin therapy in the critical ill
associated pneumonia clinical practice guideline. Worldviews on Evidence-Based Nursing.
patients. N Engl J Med. 2001;345(19)1359-1367.
2006;4(3)139-152.
40
12 Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational
California Acute Stroke Pilot Registry Investigators. The impact of standardized stroke
therapy in mechanically ventilated, critically ill patients: a randomized controlled trial.
orders on adherence to best practices. Neurology. 2005;65:360–365
Lance. 2009;373(9678):1874-1882.
13
Micek ST, Roubinian N, Heuring T, et al. Before-after study of a standardized hospital 41
Morris PE, Goad A, Thompson C, et al Early intensive care unit mobility therapy in the
order set for the management of septic shock. Crit Care Med. 2006;34:2707–2713.
treatment of acute respiratory failure. Crit Care Med.2008;36(8):2238-2243.
14
Help prevent pneumonia from a ventilator (Breathing machine). 42
Vollman K. Progressive mobility in the critical ill. Crit Care Nurse. 2010;30(2):S3-S5.
Retrieved at: www.campaignzero.org/safety-checklists/prevent-pneumonia/
43
15 Guard TD, Kress JP, et al. Efficacy and safety of a paired sedation and ventilator waning
Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically
protocol for mechanically ventilated patients in intensive care (awaking and breathing
ill patients. Canadian Critical Care Trials Group. N Engl J Med. 1994;330(6): 377–381.
controlled trial): a randomized controlled trial. Lancet. 2008;371(9607):126-134.
16
Collard HR, Saint S, Matthay MA. Prevention of ventilator-associated pneumonia: 44
Kress JP, O’Connor MF, Pohlmarn AS, et al. Sedation of critically ill patients during
an evidence-based systematic review. Ann Intern Med. 2003;138(6):494–501.
mechanical ventilation: a comparison of propofol and midazolam. Am J Respir Crit Care
17
Darlong V, Jayalakhsmi TS, Kaul GH, Tandon R. Stress ulcer prophylaxis in patients on Med. 1996;153(3):1012-1018.
ventilator. Trop Gastoenterology. 2003;23(3):124-128. 45
Garcia R, Jendresky L, Colbert L, Bailey A, Zaman M, Majumder M. Reducing
18
Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for ventilator-associated pneumonia through advanced oral-dental care: A 48-month study.
management of severe sepsis and septic shock. Crit Care Med. Mar 2004;32(3):858-873. Am K Crit Care. 2009; 18(6):523-532.
19 46
Greerts Q, Selby R. Prevention of venous thromboembolism in the ICU. Chest. 2003; Munro CL, Grap MJ, Jones DI, McClish DK, Sessler CN. Chlorhexidine, tooth brushing
124(6 Suppl):357S-363S. and preventing ventilator-associated pneumonia in critically ill adults. Am J Crit Care.
20
Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schunemann. Executive summary: 2009; 18(5):428-437.
Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of 47
Garcia R, Jendresky L, Colbert L, Bailey A, Zaman M, Majumder M. Reducing
Chest Physicians evidence-based clinical practice guidelines. Chest 2012; 141;7S-47S. ventilator-associated pneumonia through advanced oral-dental care: A 48-month study.
21
Roderick P, et al. Towards evidence-based guidelines for the prevention of venous Am K Crit Care. 2009; 18(6):523-532.
thromboembolis: Systematic reviews of mechanical methods, oral anticoagulation, 48
Culter J, Davis N. Improving oral care in patients receiving mechanical ventilation.
dextran and regional anesthesia as thromboprohylaxis. Health Technol Assess 2005;9(49). Am J Crit Care. 2005;14(5):389-394.
22 49
ABC-Awaking and Breathing Trial Coordination. Session Notes from NTI 2012 Chan EY, Ruest A, O’Meade M, Cook DJ. Oral decontamination for prevention of
(ABCDE Bundle). Accessed October 30, 2012. Retrieved at: http://www.aacn.org/wd/nti/ pneumonia in mechanically ventilated adults: Systematic review and meta-analysis.
nti2012/ docs/pearl/awakening%20and%20breathing%20trial%20coordination/ Brit Med J. 2007; 10:1136.
abc-nti-session-notes.pdf 50
Genuit T, Bochicchio G, Napolitano LM, McCarter RJ, Roghman MC. Prophylactic
23
Vasilevskis EE, Ely EW, Speroff T, Pun B, Boehme L, Dittus R. Reducing iatrogenic risks. chlorhexidine oral rinse decreases ventilator-associated pneumonia in surgical
ICU-acquired delirium and weakness—crossing the quality chasm. Chest. 2010;138(5): ICU patients. Surg Infect. 2001 Spring;2(1):5-18.
1224-1233. 51
Houston S, Hougland P, Anderson JJ, et al. Effectiveness of 0.12% chlorhexidine
24
AACN Practice Alert: Delirium assessment and management. Issued Nov 2011. gluconate oral rinse in reducing prevalence of nosocomial pneumonia in patients
Accessed March 15, 2012. Retrieved at: www.aacn.org/WD/practice/docs/ undergoing heart surgery. An J Crit Care 2002;11:567-570.
practice alerts/delirium-practice-alert-2011.pdf 52
Cocanour CS, Peninger M, Domonoske BD, et al. Decreasing ventilator-associated
25
ABCDE Bundle: Collaboration to improve outcomes for ventilated patients. pneumonia in trauma ICU. J Trauma. 2006;61:122-130.
Bold Voices. 2012;4(10):13. 53
Quenot JP, Ladoire S, Devoucoux F, et al. Effect of a nurse-implemented sedation
26
AACN Practice Alert: Delirium assessment and management. Issued Nov 2011. protocol on the incidence of ventilator-associated pneumonia. Crit Care Med.
Accessed March 15, 2012. Retrieved at: http://www.aacn.org/WD/practice/docs/ 2007;35(9):2031-2036.
practicealerts/delirium-practice-alert-2011.pdf 54
McDonald S, Tullai-McGuinness S, Madigan E, Shiverly M. Relationship between staff
27
ABCDEs of Prevention and Safety. Accessed March 15, 2012. nurse involvement in organizational structures and perception of empowerment. Crt Care
Retrieved at: www.ICUdelirium.org Nurs Q. 2010;33(2):148-162.
28 55
Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in Brody, AA. Barnes K, Ruble C, Sakowski J. Evidence-based practice councils: Potential
critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342: 1471–1477. path to staff nurse empowerment and leadership growth. JONA. 2012;42(1):28-33.
29
Bingaman M, Rahman O. Decreasing ICU LOS,VAP rate, and mechanical ventilator days
using an electronic standardized wean screen tool by the respiratory therapist. Chest 2011,
140(4)404A.
22You can also read