WorkingPapers No. 16 SOCIUM SFB 1342 - Gabriela de Carvalho Alexander Polte Katharina Scherf Mai Mohamed Abdou Mahmoud Lorraine Frisina Doetter
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SOCIUM SFB 1342
•
WorkingPapers No.16
Gabriela de Carvalho
Alexander Polte
Katharina Scherf
Mai Mohamed Abdou Mahmoud
Lorraine Frisina Doetter
Trends in time:
Identifying health care
system introductions
worldwide
Gabriela de Carvalho, Alexander Polte, Katharina Scherf, Mai Mohamed Abdou Mahmoud , Lorraine Frisina Doetter Trends in time: Identifying health care system introductions worldwide SOCIUM SFB 1342 WorkingPapers, 16 Bremen: SOCIUM, SFB 1342, 2021 SOCIUM Forschungszentrum Ungleichheit und Sozialpolitik / Research Center on Inequality and Social Policy SFB 1342 Globale Entwicklungsdynamiken von Sozialpolitik / CRC 1342 Global Dynamics of Social Policy Postadresse / Postaddress: Postfach 33 04 40, D - 28334 Bremen Websites: https://www.socium.uni-bremen.de https://www.socialpolicydynamics.de [ISSN (Print) 2629-5733] [ISSN (Online) 2629-5741] Gefördert durch die Deutsche Forschungsgemeinschaft (DFG) Projektnummer 374666841 – SFB 1342
Gabriela de Carvalho
Alexander Polte
Katharina Scherf
Mai Mohamed Abdou Mahmoud
Lorraine Frisina Doetter
Trends in time:
Identifying health care
system introductions
worldwide
SOCIUM • SFB 1342
No. 16
Gabriela de Carvalho (decarvalho@uni-bremen.de),
Alexander Polte (alexander.polte@uni-bremen.de),
Katharina Scherf (s_cvpwv8@uni-bremen.de),
Mai Mohamed Abdou Mahmoud (abdoumai@uni-bremen.de),
Lorraine Frisina Doetter (frisina@uni-bremen.de)
Collaborative Research Centre 1342 and SOCIUM,
University of Bremen
Funded by the Deutsche Forschungsgemeinschaft (DFG,
German Research Foundation) – Projektnummer 374666841
– SFB 1342.
Abstract
The present research aims to identify the timing of health care system introductions
in countries across the globe, an event which represents the state’s assumption of
substantial responsibility in the health (care) of its people. In doing so, we espe-
cially look for trends in time, which refers to the clustering of system introductions
over a distinct period, whether marked by shared historical experiences or by sim-
ple virtue of their proximity in years. Our study is structured as follows: First, we
set out to identify the introduction date of each country’s system starting in 1883
with the creation of the first health care system in the world. We then proceed to
map out introduction dates for the entire period of observation and all countries
to explore whether trends emerge. Looking beyond domestic factors that are tra-
ditionally associated with the development of social policies, we explore the po-
tential impact of transnational events as drivers of social policy change, such as
de-colonization, membership in international organizations, and the introduction
of a health care system in a neighboring country. While the present paper does
not tease out the explanatory factors contributing to the rise of health care sys-
tems worldwide, by identifying trends in their timing, our study provides important
clues as to the potential influences of transnational interdependencies in driving
social policy, as well as points to future avenues for comparative research.
[ii]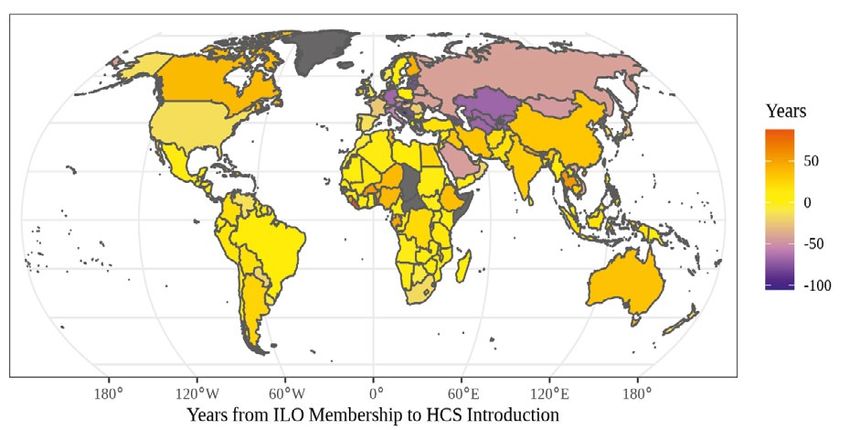
Zusammenfassung
Die Einführung eines Gesundheitssystems ist ein Ereignis, das die Übernahme
wesentlicher Verantwortung des Staates für die Gesundheitsversorgung seiner
Bevölkerung darstellt. Ziel der vorliegenden Untersuchung ist es, den Zeitpunkt
dieses Ereignisses für Länder auf der ganzen Welt zu identifizieren sowie an-
hand ähnlicher historischer Erfahrungen oder zeitlicher Nähe nach Trends zu
suchen, die sich auf die Häufung von Systemeinführungen über einen bestim-
mten Zeitraum beziehen. Die Studie ist wie folgt aufgebaut: Beginnend mit
dem Jahr 1883, als das erste Gesundheitssystem der Welt entstand, werden
zunächst die Einführungsdaten der Gesundheitssysteme in den einzelnen Län-
dern ermittelt. Anschließend werden die Einführungsdaten für den gesamten
Beobachtungszeitraum und alle Länder beschrieben und abgebildet, um zu un-
tersuchen, ob sich bestimmte Trends abzeichnen. Während inländische Faktoren
traditionell mit der Entwicklung von Sozialpolitik in Verbindung gebracht werden,
stehen darüber hinaus transnationale Ereignisse, wie z. B. Entkolonialisierung,
die Mitgliedschaft in internationalen Organisationen und die Einführung eines
Gesundheitssystems in einem Nachbarland, als Triebkräfte des sozialpolitischen
Wandels im Vordergrund dieser Untersuchung. Wenngleich in der vorliegenden
Arbeit keine erklärenden Faktoren, welche zum Aufstieg von Gesundheitssys-
temen weltweit beitragen, herausarbeitet werden, liefert die vorliegende Studie
durch die Identifizierung von Trends im zeitlichen Verlauf wichtige Hinweise auf
die potenziellen Einflüsse transnationaler Interdependenzen bei der Steuerung der
Sozialpolitik und weist auf zukünftige Wege für die vergleichende Forschung hin.
SOCIUM • SFB 1342 WorkingPapers No. 16 [iii]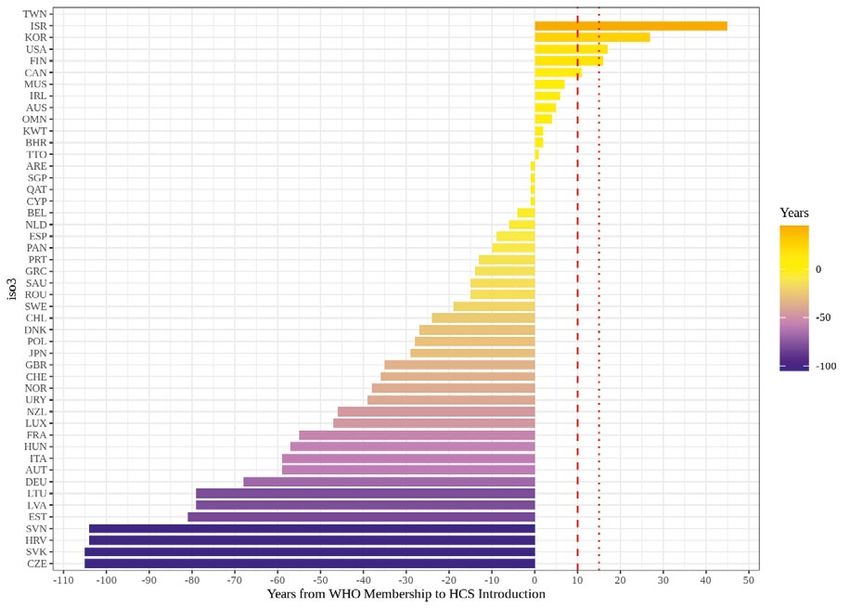

Contents
1. Introduction ................................................................................................. 1
2. Theoretical background: what drives health care system introductions? ....................2
2.1 Transnational interdependencies and health care system introductions .............4
3. Methods ..................................................................................................... 6
4. Results ........................................................................................................ 8
5. Discussion and conclusion ........................................................................... 17
References ......................................................................................................... 19
Appendix .......................................................................................................... 23
SOCIUM • SFB 1342 WorkingPapers No. 16 [v]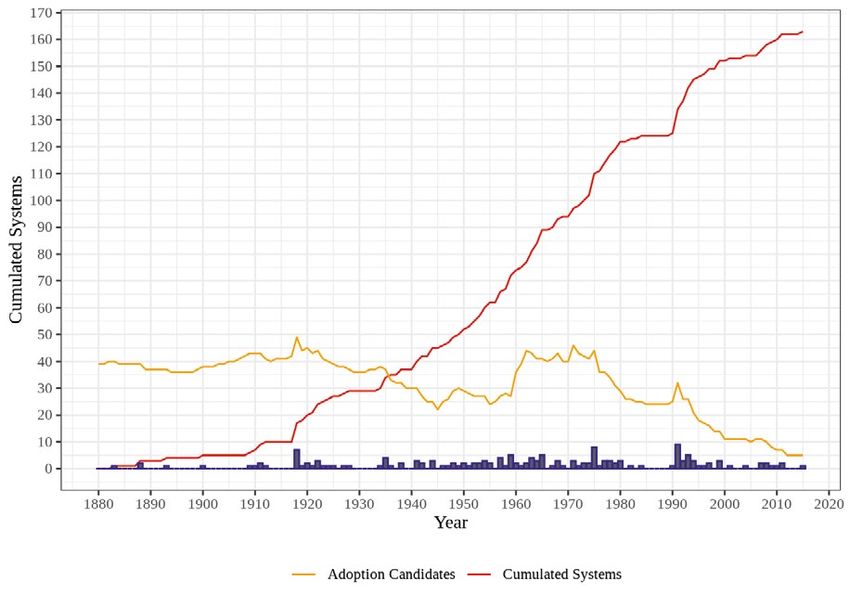
1. Introduction pursue a commitment – even if minimal – to
the health of its people.
In the present study, we set out to identi-
The aims of health care are both manifold fy this point in time for countries across the
and ambitious, spanning a wide range of ac- globe, asking the two-fold question: When
tivities to improve, maintain and prevent the do health care systems emerge and can pat-
deterioration of the health status of individu- terns be identified in the timing of system
als, as well as to mitigate the consequences introductions? To address the latter, we look
of ill-health through qualified health knowl- beyond established domestic factors associ-
edge (de Carvalho & Fischer, 2020). Given ated with welfare state developments, such
the breadth of this mission and its bearing as economic growth or the role of political
on people’s lives, the emergence of the parties, to explore the potential impact of
health care system under public responsibili- major transnational events as drivers of so-
ty (hereafter health care system) represents a cial policy change, indicating possible caus-
groundbreaking event in social policy history al explanations to be investigated in future
in a country – one in which the state takes research. More specifically, we examine
on responsibility for the financing, provision, whether the timing of health care system in-
and/or regulation of health care. troductions worldwide clusters around one or
Of all social policies, health care is said several of the following events: (1) political
to be the most controversial, constituting a independence following de-colonialization
“boundary issue” of the welfare state as it and leading to a period of nation building;
is not automatically accepted as part of the (2) membership in an international organi-
social protection package such as unem- zation (IO) concerned with health; and (3)
ployment insurance and pension plans (Der- the introduction of a health care system in
thick, 1980; Immergut, 1992). According to a neighboring country. Crucially, by focusing
Immergut (1992), the introduction of health on major transnational events we do not ar-
policies represents the division between lib- gue against the significance of domestic fac-
eralism/free market and socialism/planned tors rather we expand our analytical horizon
economy, and, therefore, is a highly politi- to include the space in which the domestic
cized issue that involve numerous societal meets the regional or global and becomes
players. In analyzing the timing of health transnational and interdependent.
care system introductions worldwide, we In what follows, we begin by discussing
may understand when political processes re- the main tenets of classical welfare state
sult in the extension of social rights across and comparative social policy theories, be-
the globe, which advances our understand- fore proceeding to more recent scholarship
ing about the politics of the welfare state in – the insights of which inform the present
general, and when health care in included study: global social policy theory and the
in the political agenda. Further, its timing re- transnational interdependencies’ framework
flects the moment in which the state no lon- (TIF) (CRC, 2018; Deacon, 2007; Kaasch,
ger relegates the totality of risk associated 2012; Obinger, et al. 2012; Nullmeier et
with illness and injury to the individual, fam- al., 2021). We then describe our research
ily, or societal actors. Put differently, the state design and methods, including our opera-
finally ‘steps up’ in a fundamental area of tionalization of key concepts. Following this,
social protection. While the degree of state we present our findings under each major
involvement in health care may vary wildly transnational event and discuss their impor-
over space and time, all system introductions tance for understanding the timing of system
share in the significance of this turning point introductions. We conclude by reflecting on
at which the state’s policy trajectory shifts to
SOCIUM • SFB 1342 WorkingPapers No. 16 [1]
the strength and limitations of our study, as health care system must be integrated, i.e.
well as with next steps for research. the existence of a (set) of institution(s) mainly
responsible for health care.
Existing literature on health care system
2. Theoretical background: introductions often concentrates on specific
what drives health care system types of systems, such as social health insur-
introductions? ance, or programs, such as vaccination and
disease-related policies (e.g. Flora & Alber,
1982; Hu & Manning, 2010; Immergut,
To be able to understand what drives health 1992; Köhler & Zacher, 1981). Scholarship
care system introductions, it is first necessary dealing with the worldwide introduction of
to pause and consider what is meant by a distinct and integrated health care systems
health care system itself. Different defini- for which there is substantial involvement by
tions can be found in extant scholarship, as the state is lacking however. Further, litera-
health care systems are a ‘conceptual mov- ture that aims at explaining the emergence
ing target’ that reflect the researcher’s goals, and ongoing reform of health care systems
choices and interests (Frisina Doetter et al., traditionally tends to look no farther than the
2021). The present study defines healthcare boundaries of the nation-state. Health care,
system as “the sum of all formal arrange- as all other areas of social policy, is viewed
ments concerning financing, regulation and almost exclusively as a domestic policy issue,
provision of qualified health services within thus driven by developments from within. This
a society dealing specifically with healthcare line of thinking characterizes much classical
as an area of social protection” (de Carval- welfare state and comparative social policy
ho & Fischer, 2020, p. 12). As concerns the theories which put the onus of explanation
definition of health care system introductions, on factors such as modernization (related
here social scientific literature has not been to industrialization and urbanization) and
as abundant (de Carvalho & Fischer, 2020). conflicts and power resources in countries
The complexity of developing a concept that (e.g., Myles & Quadagno, 2002; Wilensky,
can capture the beginning of a health care 1975). As regards the former, moderniza-
scheme lies in the fact that they are a sum of tion processes are said to represent a dou-
processes and practices, and different ways ble-edged sword: on the hand, eroding tra-
to measure their introduction can be adopted ditional means of social protection through
(Frisina Doetter et al., 2018). As previously the family; on the other hand, affording the
mentioned, this research focuses on systems necessary economic growth for the establish-
in which there is involvement of the state in ment of health and other social protection
health care. Further, the initial involvement programs.
of the central state is a necessary condition The claims surrounding modernization as
for the introduction of a system, as observing a driver of social policy expansion mainly rely
regional variation within states is beyond the on large sample quantitative studies. By way
scope of this research. However, this does of example, research by Collier and Messick
not exclude non-state actors from having a (1975) and Usui (1994) involving countries
role in the system. In line with de Carvalho at varying stages of economic development
and Fischer (2020), we hold three conditions point to the correlation between per-capita
as necessary to identify the introduction of a GDP and the early adoption of social pro-
health care system. First, a first nation-wide tection schemes. In a similar vein, Schmitt et
legislation must be ratified. Second, entitle- al. (2015) identify a positive effect of GDP
ment to health care benefits must be enact- on the adoption of health insurance in 177
ed. And third and finally, the elements of the territories and independent states over the
[2]period of 1820 to 2013. Meanwhile, Kan- Crucially, classical welfare state and com-
gas (2012) attribute higher levels of indus- parative social policy theories are marked not
trialization with the increased likelihood of only by mixed findings, but also by systematic
health insurance introductions across 43 Af- shortsightedness. That is, scholarship tends
rican nations. The impact of modernization to concentrate on high-income countries to
as a driver of social policy would therefore the neglect of the Global South. Amongst
appear robust. At closer examination, par- other things, this means that the realities of
ticularly involving smaller samples of cases social policy making and health care system
or single case studies, however, this impact developments in poorly resourced states go
seems to wane. For instance, a look to the undetected (Deacon, 2007; Yeates, 2008).
work of Cutler and Johnson (2004), which As examples, Blake and Adolino (2001), Im-
covers 20 OECD and Latin American coun- mergut (1992), Köhler and Zacher (1981),
tries, points to contradictory evidence: higher Lin and Carroll (2006) study the introduc-
levels of GDP per capita are found to actually tion and evolution of social health insurance
slow down the implementation of a national only in Western European countries. In re-
health insurance defined as compulsory cov- cent decades, scholarship on health care
erage for a broad class of people. Based on systems of the Global South has expanded,
such mixed results, it is therefore difficult to however it still falls short in comparison to
conclude as to whether or when moderniza- studies focusing on advanced economies (de
tion drives health care system introductions Carvalho et al., 2020). Further, this growing
or rather hampers it. literature mainly focuses on in-depth coun-
Similar inconsistencies characterize a sec- try analysis (e.g. Coleman, 2011; He & Wu,
ond strand of theory which looks to conflict 2017; Tavecchi & Rebecchi, 2018), as well
and power resources within states as a source as regional comparisons of current systems
of explanation for social policy change. Such (e.g. Azevedo, 2017; Balabanova et al.,
approaches emphasize the role of political 2011; Mesa-Lago, 2007), resulting in a lack
regimes, particularly democratic representa- of systematic comparisons of health care
tion and the power of left-wing parties and system introductions worldwide. The limita-
unions, as drivers of social protection (Korpi, tions of such ‘theoretical nationalism’ do not
1983). Based on a sample of 76 cases, for only impact research on the Global South:
example, Cutright (1965) finds that countries social policy, including health care, in every
with more representative governments tend country is said to now face similar challeng-
to introduce social security programs earlier es that may require solutions beyond the na-
than elsewhere. This evidence is contradict- tion-state level (e.g., demographic changes,
ed, however, by the work of Flora and Alber growing inequality, global socioeconomic
(1982) and Mares and Carnes (2009) which crises) (Obinger et al., 2012; Kaasch, 2013).
points to monarchies or autocratic govern- Over the past few decades, newer strands
ments as early adopters of social policy. of research coming from global social poli-
Within the context of the latter, early imple- cy and, more recently, the TIF have emerged
mentation of social policy is undertaken as to address some of the theoretical and em-
a means to appease and control workers, to pirical shortcomings of classical approaches
acquire output legitimacy and stabilize re- by introducing a new focus on the transna-
gimes with weak or without democratic legit- tional context in which policy making un-
imacy. Taken together, the competing claims folds (CRC, 2018; Deacon, 2007; Kaasch,
found within this body of literature offer little 2012; Obinger et al., 2012; Yeates, 2008).
clarity as to the precise role played by po- The term ‘transnational’ is used here to cap-
litical regimes in contributing to health care ture the linkages between local, national, in-
system introductions. ternational, and/or supranational actors of
SOCIUM • SFB 1342 WorkingPapers No. 16 [3]all stripes and colors across the boundaries expected to play a role in driving health care
of the national. In the case of global social system introductions?
policy theory, an analytical focus is decidedly To answer this question, we build on the
placed more heavily on the side of interna- assumptions of the TIF (CRC, 2018) and
tional actors and processes – particularly in global health policy scholarship (Kaasch,
the form of aid and activities set in motion 2012) by exploring the role of three trans-
by international governmental and non-gov- national interdependencies: colonialism;
ernmental organizations (see e.g. Kaasch, membership in an international organiza-
2012; Yeates, 2008). The TIF, instead, fol- tion; and geographic proximity. More spe-
lows a more balanced approach in seeing cifically, these interdependencies can be said
social policy as the result of interdependen- to provide the context for specific processes1
cies arising between and across all levels to emerge – whether with the onset of the
from the local and national to the region- interdependency, at some point during, or
al and global (CRC, 2018; Obinger et al., at its suspension – that capture a set of re-
2012; Nullmeier et al., 2021). But what do lated happenings unfolding within a distinct
interdependencies consist of and how can period of time triggered by a major historical
they come to affect health care system intro- event: (1) post-colonial nation building pro-
ductions? cesses following political independence and
the conclusion of colonialism; (2) assimila-
tion processes within a country following the
2.1 Transnational interdependencies
event of joining an international organiza-
and health care system introduction tion concerned with health (i.e., the state of
maintaining membership taken as a transna-
In attempting to explore the realm of the tional interdependency); and (3) policy dif-
‘transnational’ and its significance for health fusion processes unfolding in countries that
care system introductions, particularly with neighbor with a (regional) early adopter of
a view to the assumptions of the TIF (CRC, a health care system (i.e., introduction of a
2018), the role of interdependency between health care system in a neighboring country
actors comes to the fore. That is, the ac- is a major historical event). In what follows,
knowledgement that the actions of one actor we present the theoretical assumptions un-
may impact another and vice versa. This may derlying each of these processes as they ap-
involve the willful actions of actors such as ply to health care system introductions.
the waging of a war. Or, it may involve invol-
untary actions and consequences – such as Post-colonial nation building processes
when the stock market crashes in one coun- following political independence
try causing ripple effects for other markets.
When such relations between actors are sys- The colonial legacy in health is most often
tematic and cross-national borders, one can associated with imperial public health mea-
speak of a transnational interdependencies. sures to control contagious and parasitic
It is important to note that interdependency
does not necessarily imply symmetry, as ac-
1 In line with discussion by Vayda et al. (1991),
tors may wield different amounts of influence
we use the term ‘processes’ to refer to a set of
in a relation (e.g., in the case of international related events that occur within specific temporal
aid, the donor organization can be said to parameters and which collectively lead to a given
wield more power than the receiving coun- outcome. To establish the existence of a process
try that is dependent on financial assistance). entails going beyond loosely applied story telling
but necessitates strong evidence of a relationship
But what types of actions and actors can be
between events and between events and an out-
come.
[4]diseases in order to foster economic activity Assimilation processes following the joining
by keeping ‘bodies’ healthy enough to work of an international organization
(Lasker, 1977). This typically involved inva-
sive means of behavioral control applied to With the development of new strands of
indigenous populations, as well as the un- scholarship in global social policy and global
dermining of traditional healing practices. health, IOs have become one of the main
Colonial public health programs were often protagonists in the study of social policies
accompanied by a strong role for mission- (Yeates, 2008; Kaasch, 2015). Beyond the
ary hospitals, which eventually gave way obvious role of financing agents through
to training centers for midwives and nurses aid and loans, these actors are also sourc-
and, in some instances, some of the earliest es of ideas and normative standards, dis-
medical schools (Gros, 2016). In Africa, the seminators of models, promoters of policy
basic infrastructure set up during the colo- exchange, as well as advocators of rights
nial period, especially by non-state actors, (Kaasch, 2013; de Carvalho et al., 2020).
became the organizational bases for numer- Considering health care, two IOs been espe-
ous post-colonial developments in health cially active: The International Labor Organi-
care. This also applied to epistemic com- zation (ILO) founded in 1919 and the World
munities: the British Medical Association, for Health Organization (WHO) established in
example, had representation in Africa, while 1956 (Sirrs, 2020; Kaasch, 2021). Particu-
the political elite regularly received training larly for the countries of the Global South,
in imperial institutions of higher education. where limited capacity in terms of econom-
Accordingly, the colonial period was marked ic and technical resource mobilization is a
by a great deal of exposure to Western un- chronic issue, IOs play an important role
derstandings of the body, as well as the in- in financing, providing services, and even
strumentalization of that knowledge to keep regulating systems. These may result in an
labor supply abundant in the colonies. imbalance of power, making low-to-middle
With the advent of de-colonialization, po- income countries more prone to internation-
litical independence led to a period of na- al pressures and forces (Babb & Carruthers,
tionalization, particularly in Africa, in which 2008; Kaasch, 2013; de Carvalho et al.,
many newly formed governments took on 2020). Accordingly, we assume that mem-
health care and other social policy issues as bership in an IO concerned with health poli-
a means of gaining legitimacy and forging a cy quickens the introduction of a health care
new national identity (Gros, 2016). Often, system in a country by triggering assimilation
this translated to the government takeover processes – whether shaped by normative
of pre-existing colonial institutions in health. changes through exposure to new policy
Thus, the policy and infrastructure that had ideas and learning or through more forceful
been left behind by former imperial powers means such as conditionality – in health care
created a space for newly independent states in the new member state. We anticipate that
to occupy as part of their nation building pro- this will especially emerge in cases where
cess. In the language of the TIF, this suggests dependency on international aid is high, as
that colonialization – a transnational inter- characterizes many countries in the Global
dependency – once disrupted by the event South.
of political independence, may give way to a
process of nation building that led to accel- Policy diffusion processes following the
erated action in health and the introduction introduction of a health care system in a
of a health care system in a country. geographically proximate country (regional
neighborhood)
SOCIUM • SFB 1342 WorkingPapers No. 16 [5]Geographic proximity has been found are excluded from the analysis, even when
to play a role in social policy diffusion and they precede nation-wide schemes2. The sec-
transfer (Obinger et al., 2012). The main ar- ond condition refers to the establishment of
gument of this so-called neighborhood effect statutory rights to medical care as opposed
is that the closer the countries are located to to voluntary benefits or sick pay. At last, the
each other, the more likely they are in con- third condition allows us to distinguish health
tact, which may lead to the spread of ideas care systems from rudimentary and/or poli-
and normative standards, as well competi- cies or programs.
tion. Geographically close countries may in- We identify the introduction of health care
fluence each other as they have economic, systems under public responsibility through a
cultural, and linguistic similarities (Beck et five-step procedure: (1) the system must be
al., 2006). Further, spatial proximity inten- introduced by legal act; (2) this legislation
sifies communication between countries, as must be the first act of its kind ratified; (3)
the exchange of information between neigh- an institution or a set of institutions must be
bors is higher (Obinger et al., 2012). These made explicitly responsible for health care;
shared ties may lead to the establishment (4) the legal act must establish entitlements
of similar welfare state institutions (Maags, to health care; and (5) these entitlements
2020). For instance, Schmitt and Obinger must define the population group(s) that can
(2013) argue that policy examples from access benefits/services. Table 1 summa-
neighboring states are usually considered rizes our operationalization of system intro-
blueprints for domestic policies. In the pres- duction. The practical approach to pinpoint
ent study, however, we add a temporal ele- system beginnings starts with expert- judge-
ment to the neighborhood effect, assuming ment, particularly found in extant scholar-
that countries belonging to the same region ship, about when a healthcare system has
establish health care systems around the been introduced in order to map potential
same period, thereby suggesting a process starting dates. Second, we evaluate these
unfolding due to the major event of a system possible introduction points against second-
introduction within the area. ary literature, legal acts, and experts’ vali-
dation and based on the aforementioned
criteria for identifying health care system
3. Methods introductions. The earliest date at which all
necessary conditions are met is taken as the
introduction point. The introduction of the
In order to identify trends in the timing of Uruguayan health care system illustrates our
health care system introductions, this research practical procedure (Table 2)3.
descriptively shows when systems came into To pinpoint introduction dates, we exam-
being over time. In doing so, we focus on ine states with more than 500,000 inhabi-
systems in which there is substantial involve- tants in 2017, resulting in a pool of 167 cas-
ment of the state in health care. As previous-
ly state, systems under public responsibility
are introduced when (a) the first nation-wide 2 Even though we understand that the introduc-
tion of local systems may represent the first step
legislation is established; (b) entitlement to
towards establishing nation-wide schemes, for
health care benefits is enacted; and (c) the pragmatic purposes we limit our analysis to ar-
elements of the health care system are inte- rangements put in place by central governments,
grated. The first condition reflects the scope as legislations enacted by local governments are
of our research at the national level as the not easily found for 167 countries.
3 For a full account of the definition and operation-
locus of legislative action. Thus, health care
alization employed in this research, see de Car-
systems implemented only at the local level valho & Fischer, 2020.
[6]Table 1.
Operationalization criteria for the introduction of health care systems under public responsibility
Conditions Operationalization Criteria
Public responsibility Introduced by nation-wide legislation
Entitlements to benefits Definition of the population group for which is possible to receive benefits
Public responsibility AND entitlement to benefits Entitlements must be established by legislation
Temporal criterion First nation-wide legislation enacted
System integration Existence of an institution or set of institutions explicitly responsible for health care
Source: de Carvalho & Fischer, 2020, p. 14.
Table 2.
Operationalization of health care system introductions – Practical procedure
Procedure Potential Introduction Date I: 1910 Potential Introduction Date II: 1934
Expert judgement on system intro- Government of Uruguay, 1913; Muñoz et al., 2010; ISAGS, 2012; Government of Uru-
duction Puñales, 2002; Ferrari, 2010 guay, 2020
Has it been introduced through
Yes (Law No. 3724) Yes (Law No. 9202)
nation-wide legislation?
Yes (People suffering with diseases,
Do entitlements define the popula-
homeless, disabled and elderly, Yes (residents of the country)
tion group of beneficiaries?
pregnant women, and children)
Are entitlements established by a
Yes (Law No.3724) Yes (Law No. 9202)
legal act?
Is there an institution, or set of insti- Yes (Consejo de Salud Publica –
Yes (Ministry of Public Health)
tutions, responsible for healthcare? Public Health Council)
Is this the earliest date that meets
Yes No
the above criteria?
This is the beginning of the system? Yes No
Source: de Carvalho & Fischer, 2020, p.15.
es. Our period of observation starts in 1883 and Turkmenistan share the same introduc-
with the introduction of the first health care tion date, as the first health care system in
system in the world (Bärnighausen & Sauer- these territories was implemented by legis-
born, 2002; Busse et al., 2017; Light, 1985), lation in the Soviet Union. Since our focus is
and ends in 2015, when the last country es- on sovereign states legislations, we do not
tablished a system. Since the boundaries of take into account the regulations of colonial
states has changed over our period of ob- administrations to identify the emergence of
servation, we also look for legislation in the a healthcare system, as colonies were never
sovereign states preceding those currently in fully integrated into the colonizing state, but
existence. For nations which have been part an extra-territory where the rules applicable
of larger political unions or confederations to the colonial power did not automatical-
and separated over the course of the obser- ly apply. Thus, for former colonies, we only
vation period, as occurred particularly in Eu- consider systems introduced after indepen-
rope after the First World War and with the dence has been achieved4.
collapse of the Soviet Union, we trace back Drawing from global social policy theory
system beginnings to the first regulations ef- and the TIF framework, we observe whether
fective in the respective territory. This means
that, e.g., the Central Asian nations of Ka-
4 List with introduction dates and sources is avail-
zakhstan, Kyrgyzstan, Uzbekistan, Tajikistan, able on Appendix C.
SOCIUM • SFB 1342 WorkingPapers No. 16 [7]Table 3.
Operationalization criteria for the introduction of health care systems under public responsibility
Assumption Operationalization
» The analyzed countries are former British, French, Portuguese, and Spanish
colonies. We selected these colonial powers in line with Schmitt (2015, p. 332)
as “all other colonial powers had either only a very few colonies or maintained
their colonies for a much shorter duration”.
» When a country was colonized by more than one country, we consider it former
Political Independence colony of the last colonizer.
» Independence year is set in accordance with the Correlates of War (CoW, 2021)
» Countries that became independent before 1883 are excluded from the
analysis, as health care systems did not exist at the time and, therefore, could
not diffuse5.
» ILO membership date6.
» WHO membership date.
International Organizations » Countries of the Global South are operationalized according to the World Bank
income group classification (World Bank 2021). We consider the Global South
all countries that are not classified as high-income7.
» We consider ‘neighbors’ countries belonging to the same region according to
Neighborhood Effect
the UN geographical regions classification8.
Source: own presentation.
the timing of system beginnings overlap with b. IO Membership: Membership in an in-
selected transnational events in order to indi- ternational organization concerned with
cate avenues for future explanatory research. health policy accelerates the introduction
As we assume that, given the complexity of of a health care system in a country.
the phenomena at hand, a considerable
time-lag can arise between the event itself c. The Neighborhood Effect: The introduc-
and the introduction of a health care sys- tion of a health care system in a neighbo-
tem, we take a period of up to ten and/or 15 ring country accelerates the introduction
years as evidence of a potential relationship. of other systems within the region.
The burden of proof for the latter, however,
rests on future analysis. Bearing this mind,
the present research is guided by the follow- 4. Results
ing three assumptions: 78
a. Political Independence: Political indepen- This section presents the findings of our study.
dence leads to a period of nation buil- First, we elaborate on the temporal distribu-
ding which accelerates the introduction of tion of health care system introductions in
health care systems in former colonies. order to identify potential clusters in time.
Second, we examine whether the timing of
system beginnings overlaps with political in-
5 See Appendix B for independence dates and as- dependence, membership in international
signed colonizer. organizations, and geographical proximity
6 See Appendix A for ILO and WHO membership of a healthcare system introduction.
dates.
7 See Appendix A for complete list of countries and
World Bank income group classification.
8 See Appendix A for complete list of countries and
UN geographical region classification.
[8]Figure 1.
Temporal distribution of health care system introductions (health care system introductions
as percentage of existing countries)
Source: own presentation.
Temporal distribution of health care system in which the most countries adopted health
introductions care systems in relative terms. In 1888,
Austria and Italy established systems, which
Our results suggest that 164 out of 167 represents 5% of all existing countries at the
countries currently have a health care system time of introduction. Egypt, Ethiopia, Hon-
under public responsibility in place. Chad, duras, Morocco, and Syria created schemes,
Central African Republic, and Somalia are accounting for 5.3% of the extant countries
the only states with more than 500,000 in- in 1959. At last, in 1975 Angola, Congo,
habitants where the government does not Laos, Mali, Mauritius, Oman and Senegal
have a substantial role in the field (by Jan- put systems in place, making 1975 the year
uary 2021). The first health care system was in which more countries adopted health care
established in 1883 in Germany, while the systems in both relative and absolute terms.
last country to adopt a system was Burkina Interestingly, the 1959 and the 1975 spikes
Faso in 2015. Therefore, health care systems represent developments mainly in countries
have been introduced over a span of 132 of the Global South. Further, it is important
years. to highlight that the Austrian empire and Rus-
Figure 1 displays the temporal distribu- sia created their systems in 1888 and 1912,
tion of health care system introductions as respectively. In terms of current independent
a percentage of existing countries. It is pos- countries, these adoptions resulted in sys-
sible to observe several spikes in the graph, tems being put in place in Austria, Bosnia
but 1888, 1959 and 1975 were the years and Herzegovina, Croatia, Czech Republic,
SOCIUM • SFB 1342 WorkingPapers No. 16 [9]Figure 2.
Absolute and cumulative number of health care system introductions by the number of
adoption candidates
Source: own presentation.
Slovakia, Slovenia, Armenia, Azerbaijan, shows the cumulative number of health care
Belarus, Estonia, Georgia, Latvia, Lithuania, systems, and the orange line represents the
Moldova and Ukraine. total number of extant countries without a
The orange line, representing the cumu- health care system in place, or what we refer
lative number of health care system intro- to as adoption candidates. For instance, 40
ductions in percentage of existing countries, countries and one scheme existed in 1883;
shows consistent growth in the number of sys- therefore, there are 39 countries that can es-
tems being introduced throughout the entire tablish a system at this point in time. The blue
period of observation. Between 1918 and bars represent the number of systems intro-
1960 one can see a sharper increase in the duced in a year. As expected, the number
development of arrangements, which seems of health care system introductions and the
logical as the number of extant countries al- number of adoption candidates move in tan-
most doubles during the period, from 59 in dem, showing a direct relationship between
1918 to 108 in 1960. Even though there is these variables: The number of introductions
a slight reduction in the number of system increase when the number of countries with
introductions around the early 1960s, from no arrangement in place grows, and in the
1965 to 2015 there is a steady growth in the years in which less countries are at-risk of
establishment of health care schemes, when creating a system, there is a reduction in the
almost all existing countries put a system in number of systems being established.
place. We also attempt to verify the existence of
Figure 2 illustrates the total number of temporal cluster, delimited periods when a
health care system introductions by the num- great number of health care systems have
ber of candidates for adoption. The red line been introduced. However, both figures
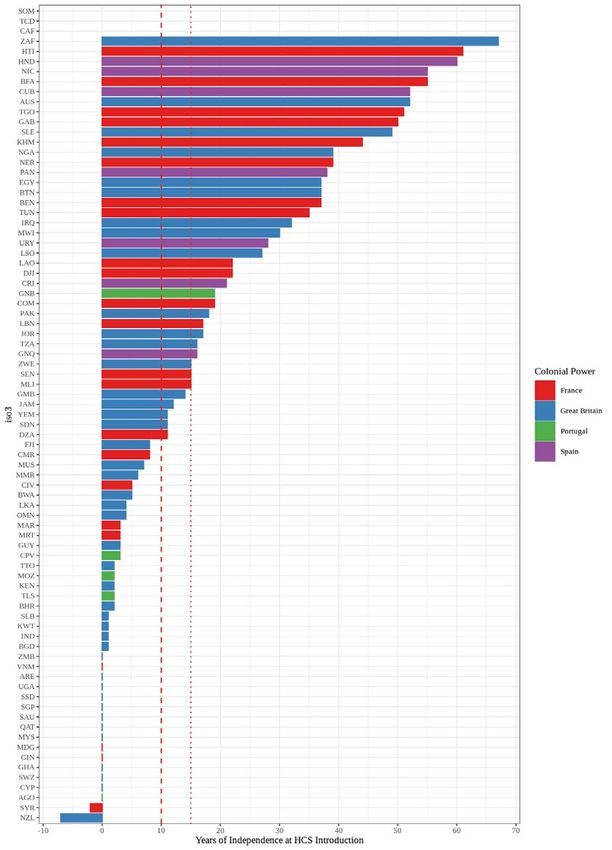
[10]Figure 3.
Health care system introduction in former colonies
Source: own presentation.
Assumption I: Political independence
seem to suggest that health care schemes
leads to a period of nation building which
have been introduced constantly and almost
accelerates the introduction of health care
evenly distributed throughout the whole pe-
systems in former colonies.
riod of observation, with no clusters being
identified. The period with most activity, how- Figure 3 displays the introduction of
ever, is from 1934 to 1980, when more than health care systems in former British, French,
half of all the existing health care systems Portuguese and Spanish colonies9. The X-ax-
were introduced (92 out of 164). is shows the difference in years between the
establishment of a system and the indepen-
Transnational interdependencies: dence, with zero/blue line representing the
Assumptions for potential relationships of year of independence. As previously stated,
health care system introductions we consider all countries colonized by the
former colonial powers that became inde-
This section examines the potential rele- pendent after 1883, when the first health
vance of three transnational events, identi- care system came into existence. Further, in
fied in the Global Social Policy and the TIF this case, we are interested in cases in which
scholarship, for trends in the timing of health the period between independence and the
care system introductions observed above.
9 Appendix D visually represents the relationship
between political independence and health care
system introduction by country.
SOCIUM • SFB 1342 WorkingPapers No. 16 [11]establishment of a system is smaller, here in- Assumption II: IO membership in an
dicated by the red lines. This may indicate international organization concerned with
that health care arrangements are part of the health policy accelerates the introduction of
nation building process. a health care system in a country.
The boxplots show that the median dif-
ference between both events is lowest for As previously discussed, at the core of
former Portuguese colonies (2) and highest the TIF and global social policy literature
for former Spanish colonies (38). The medi- are IOs and their impact on domestic social
an differences for former British and French policies. Based on this, we assume that be-
colonies are 4 and 17, respectively. In for- coming a member of an IO interested in the
mer British colonies, 26 out of 46 cases ad- field of health quickens the introduction of a
opted schemes within 10 years of political system due (but not limited) to recommen-
independence. Cyprus, Eswatini, Ghana, dations, pressure and knowledge sharing. In
Malaysia, New Zealand, Qatar, Saudi Ara- this research, we highlight the ILO and WHO
bia, Singapore, South Sudan, Uganda, Unit- as key IOs in the field of health care. Addi-
ed Arab Emirates and Zambia introduced tionally, we ask whether there is a triangular
health care system in the same year of be- relationship between membership, income
coming independent. If we expand this pe- level, and health care system introductions,
riod to 15-years, 67% of the cases created hypothesizing that low-to-middle income
system in the aftermath of the independence. countries are more likely to be influenced by
Considering former Portuguese countries, external pressures associated with IOs and
Angola, Cape Verde, East Timor and Mo- foreign aid. Figures 4 to 710 display health
zambique introduced systems within 3 years care system introduction in Global North
of political independence. For instance, An- and Global South countries after member-
gola became independent in November 11 ship in the ILO and WHO.
of 1975, and created its system in Decem- Figure 4 shows the timing of health
ber 10 of the same year (Hilhorst & Serrano, care system beginnings related to the year
2010; Tallio, 2017). Among the 26 former of membership in the ILO for four income
French colonies, 8 adopted a health care groups. The X-axis shows the difference in
system legislation within 10 years, and 11 number of years between membership and
within 15 years, which represents 30% and health care system adoption. While negative
42% of the cases. On the other hand, for values denote that systems have been intro-
former Spanish colonies, political indepen- duced before becoming part of the organi-
dence does not seem to be closely related zations, positive values represent the number
to the introduction of health care systems. As of years between ILO membership and health
Figure 3 clearly shows, none of the coun- care system creation. The boxplots suggest
tries introduced during the first 15 years of that the median time difference between
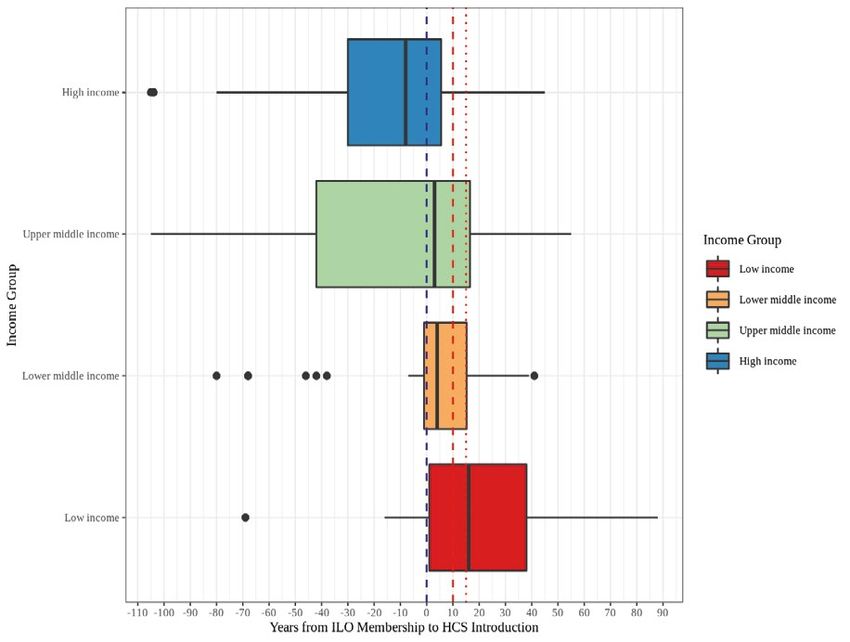
independence and the median gap between both events is lowest for high-income coun-
introduction year and independence is by far tries (-8) and highest in low-income coun-
the largest in this group. tries (16). For both lower- and upper-mid-
The graph shows a potential relationship dle-income countries the period is similar,
between political independence and the 3 and 4 respectively. The great majority of
adoption of a health care system, as 38 out high-income countries introduced their sys-
of 81 countries introduced a scheme within tems already before becoming affiliated with
10 years, and 46 in the first 15 years of po-
litical independence.
10 Appendix E visually represents the relationship
between ILO and WHO membership and health
care system introduction by country.
[12]Figure 4.
Health care system introductions in ILO country members by income groups
Source: own presentation.
Figure 5.
Health care system introductions in ILO country members
Source: own presentation.
SOCIUM • SFB 1342 WorkingPapers No. 16 [13]the ILO; therefore, the phenomenon under both events is lowest for high-incomers (-15)
study is not associated with membership in and highest in lower-incomers (15). The
this institution. great majority of high-income countries (35)
Differently, the great majority of the low- had health care arrangements in place be-
to-middle income countries introduced fore becoming a WHO member, as this insti-
health care arrangements after becoming an tution was created only in 1948 (Kott, 2019).
ILO member, as only 35 out of 119 coun- This also holds true fir upper-middle-income
tries had a system before membership. If countries. For this income group, the medi-
we split this larger group, we can observe an time difference between both events is -4.
that for low and lower-middle-income coun- Therefore, health care system introductions
tries about 75% of the observations created in richer countries are not associated with
health care systems following ILO member- WHO membership.
ship. It is also worth noting that almost 50% For low-middle- income and low-income
of lower-middle-income countries introduced countries the great majority introduced their
systems within 15 years after membership. If health care systems after becoming WHO
we only consider countries that are adoption members, representing about 75% and
candidates, out of the 33 lower-middle-in- more of the observations. The median time
come countries that are adoption candi- difference between events in low-middle-and
dates, around 64% adopted within 15 years low-income countries are 4 and 15, respec-
of association. Timing of introduction in this tively. It is important to note that 55,3% of
income group seems to have the highest po- the lower-middle-income countries that are
tential for being associated with ILO mem- candidates for adoption create a system
bership. within 15 years. In summary, the figures show
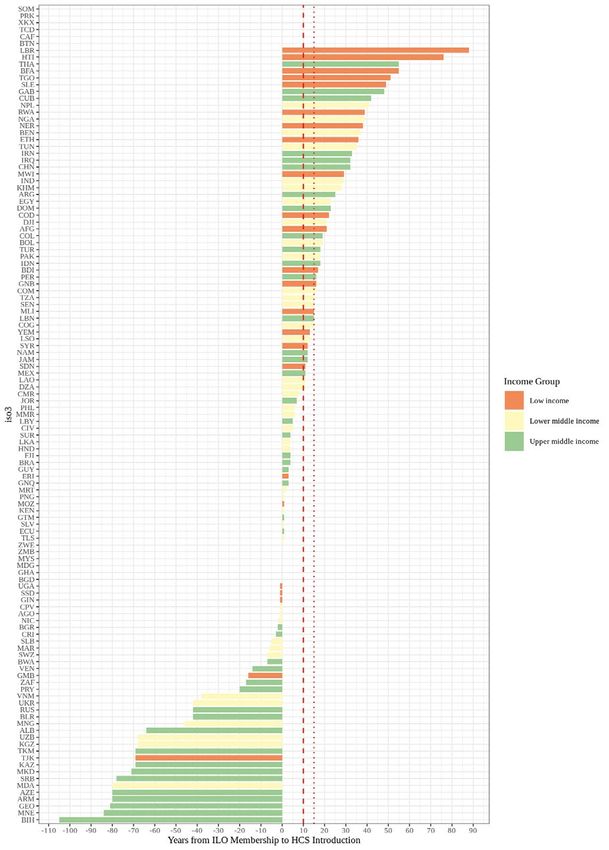
Figure 5 displays in a map the relation- a possible relationship between IO member-
ship between ILO membership and health ship and health care system introductions for
care system introduction. Shades of yellow low-middle and low-incomers.
to red, i.e. positive values, indicate that sys- Figure 7 shows the interval between ILO
tem adoptions happened after membership. membership and health care system intro-
Countries in grey are not members of the in- duction throughout the globe. Like the pre-
stitution or do not have a system in place. It vious map, shades of yellow and red indi-
is possible to observe that the great majori- cate that system adoptions happened after
ty of countries adopted health care systems membership, and shades of purple and blue
after becoming ILO member. In countries before membership. Countries in grey are
represented by different shades of yellow, the not members of the WHO or do not have a
period between membership and health care health care system in place. It is also possi-
system introduction is smaller. It is possible ble to observe that most countries in Africa,
to observe that the interval between mem- south east Asia, and North America adopted
bership and the adoption of health care ar- health care systems after becoming WHO
rangements seems to be smaller in several member, while most European, central and
African and Latin American nations, com- north Asian, as well as some south American
pared to Northern Asia and Europe, which countries adopted before.
introduced before their ILO membership, or Comparing the relationship between ILO
large countries in south and south-east Asia and the WHO memberships with health care
and Oceania, which adopted afterwards. system introductions, the boxplots present-
The relationship between WHO member- ed in this study have similar shapes. In both
ship and the introduction of health care sys- cases, the majority of high-incomers had sys-
tems is displayed in Figures 6 and 7. Figure tems in place before membership, and the
6 shows the median time difference between
[14]Figure 6.
Health care system introductions in WHO country members by income group
Source: own presentation.
Figure 7.
Health care system introductions in WHO country members
Source: own presentation.
SOCIUM • SFB 1342 WorkingPapers No. 16 [15]greatest part of low-middle- and low-incom- Considering African sub-regions12, it is also
ers did not have any arrangement in place difficult to notice temporal clusters. Northern
before becoming associated with these or- Africa is the sub-region where we can find
ganizations. The great difference seems to the smallest interval between first and last in-
be found in upper-middle-incomers, as the troduction (25 years).
majority of the countries adopted systems For the other regions, the interval be-
after ILO and before WHO memberships. tween first and last adoption is even larger;
Therefore, it seems that membership and however, it is possible to notice periods with
health care system creation have a stronger more intense activity, particularly in Asia. In
impact on poorer countries, both lower-mid- this continent, it is possible to notice some
dle and low-incomers. clusters of health care system introduction. In
the 30- years-period, from 1948 and 1978,
30 systems were created, which may suggest
Assumption III: The introduction of a health a snow-balling effect. Japan and Mongolia
care system in a neighboring country were the first Asian countries to establish a
accelerates the introduction of other systems health care system under public responsibil-
within the region. ity, and Bhutan the last. In the Americas, the
period with most intense activity is from 1935
The neighborhood effect implies that and 1980, but it is not possible to identify
geographical proximity is a driver of social temporal clusters. However, accounting only
policy diffusion and transfer. If this assump- for subregions, there is a shorter adoption
tion holds true, countries belonging to the interval in Central America, where all seven
same geographic region adopt health care countries created systems within 14 years,
systems around the same period. Figure 8 and Northern America, as Canada and the
displays the total number health care system US established systems in 1957 and 1965
introductions throughout our entire period respectively. In South America and the Ca-
of observation within geographical regions ribbean, the number of introductions was
according to the United Nations’ classifica- more spread. Uruguay was the first country
tion11. In Africa, health care systems were of this region to create a system: In 1910,
introduced between 1957 and 2015. Gha- the Uruguayan government provided medi-
na and Libya were the early- adopters, and cal care to vulnerable groups, such as home-
Burkina-Faso the laggard. Africa was the less people, children, and pregnant women
last continent to start the introduction of the (Government of Uruguay, 1913). Haiti was
schemes, and is the only continent where the last country of the region to put a system
we find countries without any arrangement in place only in 1995.
(Chad, Central African Republic, and So- It is also difficult to identify clusters of
malia). In comparison to Europe, when Af- health care system introductions in Europe,
rica introduced its first system, all European as countries adopted arrangements through-
states had a scheme in place except for Fin- out an 80-years period. It is possible to no-
land (1963). Considering all regions, Africa tice, nonetheless, that Europe was the first
is the continent with the smallest difference region to start and to finish the implemen-
between the first and the last adopter, even tation of health systems. At last, three out
though this is spread over a 58 years-period. of five countries adopted schemes between
1977 and 1979 in Oceania (Papua New
Guinea, Fiji and Solomon Island). Australia
11 North Korea and Kosovo are not part of the anal-
ysis as these countries are not classified in any 12 See Appendix A for sub-region division according
region by the UN classification. to the UN classification (2021).
[16]Figure 8.
Health care system introductions by geographical region
Source: own presentation.
passed a health care system legislation cre- the Collaborative Research Center 1342:
ating a system in 1953, and New Zealand Global Dynamics of Social Policy, based at
was the first country outside Europe to put the University of Bremen, Germany. A sec-
an arrangement in place yet in 1900. Based ondary goal of this paper is to explore the
on these, the introduction of a health care relationship between the timing of health
scheme in a neighboring country does not care system introductions and three events:
seem to have a great impact on the adoption political independence of a former colony,
of such policy in countries belonging to the IO membership, and the introduction of a
same region. healthcare system in a neighboring country.
Each event represents a punctuated moment
in time underlined by a complex set of in-
5. Discussion and conclusion terdependencies both between countries and
between countries and IOs.
Our study of healthcare system introduc-
The main goals of the present study were tions led us to a number of important obser-
to describe the timing of health care sys- vations: By analyzing all countries with more
tem introductions and to present the data than 500,000 inhabitants in 2017, we iden-
collected within the research project Glob- tified the existence of systems under public
al developments in health care systems and responsibility in 164 out of 167 countries.
long-term care as a new social risk, part of Health care systems have been introduced
SOCIUM • SFB 1342 WorkingPapers No. 16 [17]over a 132-year span, Germany being the only created later. Considering low- and
first adopter in 1883, and Burkina Faso the lower-middle-incomers, the great majority
last adopter in 2015. Regarding trends, we did not have health arrangements in place
observed that the establishment of systems before membership in both the ILO and the
was constant throughout the whole period of WHO. Our findings show a potential stron-
observation; however, it is possible to identify ger relationship between affiliation to the
years 1934 to 1980 as the period in which organizations and health care system intro-
the great majority of systems were adopted in ductions: In both cases, about 75% of the
both relative and absolute terms. We could observations established health care systems
also verify that the three largest spikes in our following membership. In upper-middle-in-
data (1888, 1959 and 1975) represent the come countries, however, it seems that there
creation of systems in countries with simi- is a potential relationship between WHO
lar economic levels. In 1888, high-income association and the creation of health care
countries introduced systems; and in 1959 schemes, but this correlation cannot be ob-
and 1975, only countries of the Global served when considering ILO membership.
South established arrangements. In terms of In summary, our observation suggests a po-
geographical distribution, we observed that tential relationship between ILO and WHO
European countries were the early adopters membership for low and lower-middle-in-
of health care systems, and Africa was the comers, and upper-middle-incomers in the
last region to start implementing arrange- case of the WHO. For high-income coun-
ments. tries, the relationship seems to be inexistent.
As previously mentioned, the secondary This confirms our assumption that member-
goal of the study was to explore whether the ship in an IO quickens the introduction of
introduction of health care schemes over- a health care system in a country, especially
lapped with transnational events selected in cases where dependency on international
in accordance with scholarship on global aid is high, as characterizes many countries
social policy and TIF. We reiterate that this in the Global South.
paper does not intend to establish causal We also attempted to observe a possible
explanations, but to point to potential re- connection between geographical proximity
lationships between the establishment of and health care system introductions. Based
health care systems and important historical on the data presented in this research, geo-
events on the basis of their temporal proxim- graphical proximity added to temporal distri-
ity. With respect to political independence, bution did show regional differences in tim-
our results point to a potential relationship ing of introduction, Europe being an early
between independence and the creation of adopter and Africa a laggard.
health schemes, mainly in former British and Despite a set of promising observations,
Portuguese colonies, where approximately the present study is not without limitations.
67% of the countries adopted systems within With regard to health care system introduc-
15 years of independence. tions’ data, we identify possible introduc-
Our second assumption dealt with the po- tion dates through experts’ judgement only,
tential relationship between membership in mainly found in English-language secondary
IOs concerned with health and health care literature. This means that potential system
system introductions, i.e. ILO and WHO. We introductions not represented in this literature
observed that most high-income countries were not included in our analysis. Second, as
adopted systems before becoming mem- our understanding of a system begins with
bers of both institutions. A possible expla- the enactment of the first health care legisla-
nation for this is that richer countries were tion that meets our pre-established criteria,
early-adopters and these institutions were we may identify as starting points legislation
[18]You can also read