BUILDING AN IMPROVED PRIMARY HEALTH CARE SYSTEM IN TURKEY THROUGH CARE INTEGRATION - BY SAFIR SUMER JOANNE SHEAR AHMET LEVENT YENER JULY 17, 2019
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
BUILDING AN IMPROVED PRIMARY
HEALTH CARE SYSTEM IN TURKEY
THROUGH CARE INTEGRATION
BY
SAFIR SUMER
JOANNE SHEAR
AHMET LEVENT YENER
JULY 17, 2019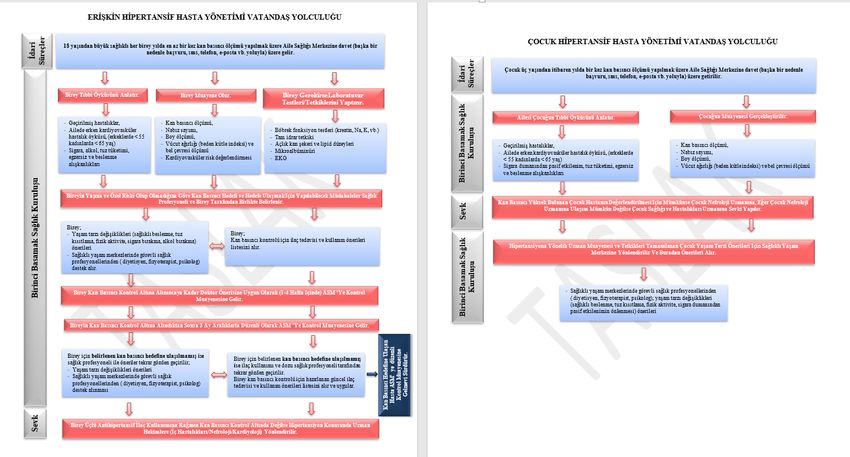
© 2019 The World Bank 1818 H Street NW, Washington DC 20433, USA. Telephone: 202-473-1000; Internet: www.worldbank.org. Some rights reserved The report entitled Building an Improved Primary Health Care System in Turkey through Care Integration has been produced under the grant received from the Japan Policy and Human Resources Development (PHRD) Technical Assistance Program which is financed by the Government of Japan. This work is a product of the staff and consultants of the World Bank. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of the Executive Directors of The World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. Rights and Permissions The material in this work is subject to copyright. Because The World Bank encourages dissemination of their knowledge, this work may be reproduced, in whole or in part, for noncommercial purposes as long as full attribution to this work is given. Attribution—Please cite the work as follows: “Sumer, Safir, Joanne Shear, and Ahmet Levent Yener. 2019. Building an Improved Primary Health Care System in Turkey through Care Integration. © World Bank.” All queries on rights and licenses, including subsidiary rights, should be addressed to World Bank Publications, The World Bank Group, 1818 H Street NW, Washington, DC 20433, USA; fax: 202-522-2625; e-mail: pubrights@worldbank.org.
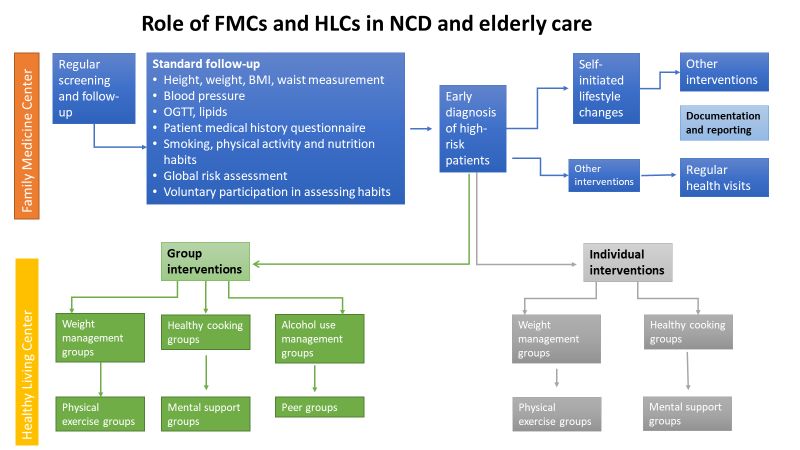
Table of Contents
List of Abbreviations ................................................................................................................................................................................ 3
Executive Summary .................................................................................................................................................................................. 5
1. Introduction ........................................................................................................................................................................................... 9
2. Background and Context for Integrated Care in Turkey ........................................................................................................ 11
2.1. Turkish PHC System (in a nutshell) ................................................................................................................................. 11
2.2. NCD Burden ....................................................................................................................................................................... 12
2.3. The Need for Change in Care Delivery Structures ................................................................................................... 15
2.4. Integrated Care at Higher Policy Level in Turkey .................................................................................................... 16
3. Essential Components of Integrated Care: Overview, Country Examples, Status of Turkey, and Recommendations 19
3.1. Fundamentals of Change .............................................................................................................................................. 21
3.1.1 Engaged Leadership and Shared Vision ......................................................................................................... 21
3.1.1.1 Overview and Country Examples ................................................................................................................. 21
3.1.1.2 Current State in Turkey ................................................................................................................................... 24
3.1.1.3 Recommendations on Integration within Primary Care Level ................................................................... 25
3.1.2 Patient Focus and Engagement .......................................................................................................................... 25
3.1.2.1 Overview and Country Examples ................................................................................................................. 25
3.1.2.2 Current State in Turkey .................................................................................................................................... 28
3.1.2.3 Recommendations on Integration within Primary Care Level ................................................................. 30
3.2. Organizational Change .................................................................................................................................................. 31
3.2.1 Regulatory Frameworks ....................................................................................................................................... 32
3.2.1.1 Overview and Country Examples ................................................................................................................. 32
3.2.1.2 Current State in Turkey ................................................................................................................................... 33
3.2.1.3 Recommendations on Integration within Primary Care Level ................................................................... 34
3.2.2 Creating an Enabling Environment .................................................................................................................... 34
3.2.2.1 Overview and Country Examples ................................................................................................................. 34
3.2.2.2 Current State in Turkey ................................................................................................................................... 36
3.2.2.3 Recommendations on Integration within Primary Care Level ................................................................. 37
3.2.3 Alignment of Financing and Incentives .............................................................................................................. 38
3.2.3.1 Overview and Country Examples ................................................................................................................. 38
3.2.3.2 Current State in Turkey ................................................................................................................................... 39
3.2.3.3 Recommendations on Integration within Primary Care Level ................................................................. 40
1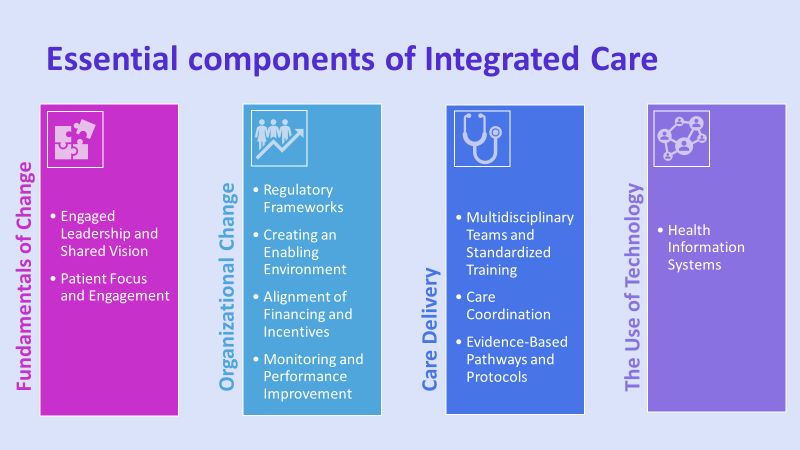
3.2.4 Monitoring and Performance Improvement ..................................................................................................... 40
3.2.4.1 Overview and Country Examples ................................................................................................................. 40
3.2.4.2 Current State in Turkey ................................................................................................................................... 44
3.2.4.3 Recommendations on Integration within Primary Care Level ................................................................. 44
3.3. Care Delivery.................................................................................................................................................................... 46
3.3.1 Multidisciplinary Teams and Standardized Training ..................................................................................... 46
3.3.1.1 Overview and Country Examples ................................................................................................................. 46
3.3.1.2 Current State in Turkey ................................................................................................................................... 49
3.3.1.3 Recommendations on Integration within Primary Care Level ................................................................. 50
3.3.2 Care Coordination ................................................................................................................................................ 52
3.3.2.1 Overview and Country Examples ................................................................................................................. 52
3.3.2.2 Current State in Turkey ................................................................................................................................... 54
3.3.2.3 Recommendations on Integration within Primary Care Level ................................................................... 57
3.3.3 Evidence-Based Pathways and Protocols ........................................................................................................ 61
3.3.3.1 Overview and Country Examples ................................................................................................................. 61
3.3.3.2 Current State in Turkey ................................................................................................................................... 63
3.3.3.3 Recommendations on Integration within Primary Care Level ................................................................. 64
3.4. Use of Technology............................................................................................................................................................ 65
3.4.1 Health Information Systems ................................................................................................................................. 65
3.4.1.1 Overview and Country Examples ................................................................................................................. 65
3.4.1.2 Current State in Turkey .................................................................................................................................... 67
3.4.1.3 Recommendations on Integration within Primary Care Level ................................................................. 72
4. Suggested Roadmap for Integrated Care Efforts in Turkey .................................................................................................. 74
5. Conclusion ..................................................................................................................................................................................... 76
Bibliography .......................................................................................................................................................................................... 77
Annex 1 ER Visits for the Six Biggest Provinces of Turkey ....................................................................................................... 86
Annex 2 Role of Primary Care Providers in NCD and Elderly Care and Patient Pathways Developed by the MoH
for HT and CVD Risk Assessment ....................................................................................................................................................... 88
2
LIST OF ABBREVIATIONS
ACSC Ambulatory Care Sensitive Condition
AHBS Family Medicine Information System (Aile Hekimliği Bilgi Sistemi)
ARCHO Assessment of Readiness for Chronicity in Health Care Organizations
BI Business Intelligence
CHC Community Health Center
COPD Chronic Obstructive Pulmonary Disease
COSLA Confederation of Scottish Local Authorities
CPG Clinical Practice Guideline
CVD Cardiovascular Disease
DALY Disability Adjusted Life Year
DHBS Dental Health Information System
DM Diabetes Mellitus
DSS Decision Support System(s)
DYOB Dialysis Management Information System (Diyaliz Bilgi Yönetim Sistemi)
EBYS Electronic Document Management System
ED Emergency Department
EHR Electronic Health Record
ER Emergency Room
EU European Union
FM Family Medicine
FMC Family Medicine Center
FMP Family Medicine Physician
GDHIS General Directorate of Health Information System(s)
HbA1c Hemoglobin A1c
HBYS Hospital Information System (Hastane Bilgi Yönetim Sistemi)
HCP Health and Care Plan
HIS Health Information System(s)
HLC Healthy Living Center
3HSYS Public Health Information System (Halk Sağlığı Yönetim Sistemi)
HT Hypertension
HTP Health Transformation Program
HYP Disease Management Platform (Hastalık Yönetim Platformu)
ICD 10 International Statistical Classification of Diseases and Related Health Problems 10TH Revision
ICU Intensive Care Unit
IHI Institute for Healthcare Improvement
IRR Internal Rate of Return
ISBS Occupational Medicine Information System (İşyeri Hekimliği Bilgi Sistemi)
MBYS Medical Examination Information System (Muayene Bilgi Yönetim Sistemi)
MCH Maternal and Child Health
MoH Ministry of Health
MSSQL Microsoft SQL Server
NCD Noncommunicable Disease
NHS National Health Service
NPO Nonprofit Organization
PHC Primary Health Care
PHRD Japan Policy and Human Resources Development Fund
ROI Return on Investment
SDGs Sustainable Development Goals
SINA Statistical and Causal Analysis in Health
SQL Structured Query Language
STEPS WHO STEPwise Approach to Adult Risk Factor Surveillance
TURKSTAT Turkish Statistical Institute
UHTS National Patient Tracking System (Ulusal Hastalık Takip Sistemi)
VHA Veterans Health Administration, United States
WHO World Health Organization
4EXECUTIVE SUMMARY
Turkey has realized a very successful health reform between 2003 and 2013. The Ministry of Health (MoH) has
developed strategic objectives and major transformation processes under the reform primarily focused on
people and gave priority to improve and reshape the primary care structure through the introduction of the
Family Medicine (FM) model. Universal health coverage has been established, and the MoH initiated various
programs to improve the service provision at all stages. While the overall transformation process includes
many aspects of a broader integration of care, an explicit ‘integrated care’ model has never been discussed in
Turkey. This report therefore aims to provide a picture of the Turkish health system from an integrated care
perspective while prioritizing noncommunicable diseases (NCDs) and to inform policy makers and
practitioners on the needs and opportunities to design a broader care integration model as well as to present
specific recommendations on how to improve integration among the primary health care (PHC) actors.
The scope of this report covers analysis and means for integration within the primary care levels as this seems
a good entry point for integrated care within the Turkish context. Discussions on the vertical integration
between preventive, primary, and secondary care as well as the financial models for integration are left to
future activities/efforts.
Key elements of integrated care, as elaborated in the report, can be grouped under four dimensional areas:
fundamentals of change, organizational change, care delivery, and the use of technology (Figure 1).
Figure 1
Engaged leadership necessitates charting the course for change and supporting efforts for transformation.
Engaged leaders provide direction and motivation and allocate resources through effective strategies. A shared
vision at all levels of the transformation process is also critical for successful change within a health care
system. Leadership is crucial for articulating a shared vision and conveying the message on the urgency and
importance of that vision to all stakeholders. Therefore, leaders need to provide a supportive organizational
culture by encouraging open and honest feedback from key stakeholders, which will facilitate transparent
monitoring and evaluation and shared decision making to foster public trust.
Patient focus, patient centeredness, and patient engagement and activation are not only essential
elements of integrated care models, but they also relate to a number of positive results such as improved health
outcomes, improved communication and interactions within the health care team, and patient satisfaction. The
concepts of self-care, co-ownership of health care delivery options, discussion on planned outcomes, and
informed expression of choice enhance the responsibility and accountability of health care seekers and
necessitate revisiting professional identity and scope of responsibilities of the health care workers. Population
5risk stratification based on care needs is another necessity to allocate resources and to plan personalized and
patient-centered care delivery.
A review of existing national health policies and regulatory frameworks is important for evaluating progress
toward integrated care. While the current approach to addressing chronic diseases is mostly hospital based
and has the potential to weaken links of NCDs with population health and wider determinants of health,
traditional approaches need to be revisited to shift the burden of care to lower levels of care. Therefore,
integrated care introduces new models of care delivery which facilitate this shift toward population health
management and proactive and preventive care.
An enabling environment should primarily bring together all involved stakeholders for a transformational
change. A cultural change in the clinical and management practices is needed to establish a shared vision and
ensure sustainability. To ensure alignment among all the processes and actors involved, top management’s
strong and visible support for the integrated care efforts and the existence of joint decision-making
mechanisms are important. Another enabler is the existence of clinical leadership to communicate a clear vision
on how integrated care can produce desired improvements. Lastly, the existence of shared accountability
through reliable information sharing is essential since integrated care delivery necessitates the existence and
acceptance of clearly defined shared values.1
Alignment of finances and incentives, either monetary or non-monetary, can be effective in promoting
change. Financing and incentives options are varied, including investments, making the business case, reward
schemes, pooled budget, shared risks and revenue/profits, bundled payments, capitated payments, long-term
contracts, and end-to-end managed care. While provider payments should generally be designed to encourage
performance improvement for providers to improve the experience of care, improve population health status,
and reduce costs, incentives and payment methods need to be aligned with broader system goals, to be
consistent across providers/payers and to address provider protection from unavoidable risk as well as
variation in patient morbidity.
Monitoring and performance improvement through quantitative and qualitative data against baseline is
critical in implementing integrated care. Performance indicators should include measurement in clinical
quality, patient experience, staff experience, staff satisfaction, and cost effectiveness.
The need for multidisciplinary teams emerges with the transformation of health care systems where new
roles need to be created and new skills need to be developed. Additionally, health care demand also changes
over time and this calls for retraining the skills and talent and expanding experience through novel practices
of care as well as improving the systems to become ‘learning systems’ that would continuously improve
productivity and increase success. As PHC provides the basis for a stable, cost-effective, and efficient health
care delivery system, building effective health care teams for an assigned group of patients to provide
preventive, chronic, and acute care would mean good PHC practice. Shifting care from hospitals to primary care
needs careful planning and execution to ensure that PHC services have the capacity and capabilities to meet
the demand. A team-based care approach requires that team members are trained and supported to function
effectively, and they are provided with the tools and guidance to effectively deliver care.
Care coordination is the organization of health care delivery activities between multiple providers and the
patient to facilitate appropriate health care. Care coordination involves the mobilization of personnel and other
resources needed for all required patient care activities and managed by the exchange of information among
different providers and the patient. Effective care coordination requires building relationships between PHC
1 Maruthappu, Hasan, and Zeltner 2015.
6teams, key specialist groups, hospitals, and community service agencies through tools such as referral and
transition protocols and systems to support information transfer.
Evidence-based pathways and protocols contribute to the advancement of evidence-based health care and
practice with a number of emerging factors such as cost pressures, technological achievements, changing public
expectations, value-for-money movement, political consensus, professional accountability, and changing
demographic profile. The use of evidence-based pathways and protocols is currently considered a value-added
approach to improve patient outcomes and bring efficiency to multidisciplinary work for standardized care
and work processes.
Health information systems (HIS) are critical for efficient collection of health system and patient data and for
the best use of these data to establish/improve the coordination of patient-provider and intra-provider clinical
activities. HIS also concentrate on the use of data for research, planning, and management decisions about
integrated care. Health care providers continuously need patient/beneficiary information in terms of their
wants and needs and other providers’ care details to adjust or to complement the ongoing patient care scheme,
and achieving efficient integrated care is possible only with effective communication and information.
Therefore, HIS have a critical role in care quality improvement, cost reduction, and establishing of innovative
integrated care models.2
In light of the essential elements and good country practices of integrated care, a quick look at the Turkish
health system reveals several challenges such as the lack of concretely defined objectives for integrated care,
limitations to access patient data at all levels of care to plan for integrated care, and lack of adequate health
care personnel at the primary care level to address the working modality change that would come with
integrated care. In addition, there is lack of financial models/mechanisms to deal with NCDs at the primary care
and prominent changes in the MoH upper management level during the last few years, which make long-term
program planning and implementation difficult as there is discontinuous top-level engagement to commit and
engage for possible integrated care initiatives.
Nevertheless, there are a number of good practices at both the central and local levels on differing scales, as
the report points out. To name a few, prevailing practices include the existence of well-advanced and flexible
HIS, small-scale care coordination efforts for a number of diseases, and initial local attempts to draft/reshape
care coordination processes as well as regular integrated care data collection procedures.
To support both the good country practices and efforts toward integrated care, this report provides a set of
recommendations for integrated care in Turkey based on the essential elements discussed above (Figures 2, 3,
4, and 5).
These recommendations, together with the country-specific good practice examples, can inspire and leverage
the future design efforts of integrated care and if successful, can lead the way to scale up integrated care efforts
throughout the health system.
2 Øvretveit 2017.
7Figure 2 Figure 3
Figure 4 Figure 5
81. INTRODUCTION
Sustainable Development Goals (SDGs) adopted by the United Nations member states in 2015 is an
international pledge for the current and future well-being of people to end/curb poverty through the
reductions in inequality and improvements in areas such as health and education. Goal 3 of the SDGs focuses
on ensuring healthy lives and promoting well-being for all at all ages3 and calls for increased efforts on health
system strengthening to address new and changing health challenges, increase access to health care, and shift
the perspective and focus toward meeting the needs of the people served by the health care system. To this
end, the notion of integrated and people-centered health care presents a transformation in the management,
funding, and delivery of health care services and emphasizes a structural shift from health systems designed
around diseases to systems designed for people.4
With the increasing pressures of health systems posed on governments, no single actor alone can successfully
improve the population’s health. All involved in the health system, including health care organizations, public
health departments, social service entities, school systems, and employers, need to cooperate. As this
cooperation requires an integrator, policy makers can assume this role through making the right investments
and creating a clear set of high-level measures to monitor progress.5
Improving population health outcomes and the well-being of the populace is an imperative that is shared
globally. Over the last 10 years, the international health care community has recognized that current
fragmented health care delivery and provider systems hinder good patient access, do not provide continuity of
care, are cumbersome for patients to navigate, are inefficient in terms of time and resources, and do not
promote and sustain quality health care. A promising model known as ‘integrated care’ is being widely
implemented and studied to address current health care delivery. Integrated care seeks to improve outcomes
of care by overcoming issues of fragmentation through linking or coordination of services of providers along
the continuum of care. Strong primary care is a key component of integration and continuity between and
across levels of care, which is essential for patients, particularly those with complex needs. Primary care can
contribute to strengthening the overall health system’s performance by providing affordable and accessible
care, coordinating care for patients so that they are given the most appropriate services in the right setting, and
reducing avoidable hospital admissions.6
Health care systems implementing an integrated care approach have achieved reductions in chronic disease
morbidity and mortality as well as improvements in prevention care (for example, immunizations) and early
detection of cancers and chronic diseases resulting in a decreased disease burden impact on systems and the
population.7 Integrated care has also demonstrated reductions in the economic impact of ill health and diseases
on the government, health care systems, and the people.8 A large study conducted in Switzerland demonstrated
3 https://sustainabledevelopment.un.org/sdg3 (accessed December 26, 2018).
4 https://www.who.int/servicedeliverysafety/areas/people-centred-care/en/ (accessed December 26, 2018).
5 Borgermans and Devroey 2017.
6 European Union 2018.
7 European Union 2017.
8 Lyngsø et al. 2014.
9substantial effects of integrated care on reducing medical expenditures (up to 10 percent) and disease-related
hospitalizations reflecting the quality of care in patients suffering from highly prevalent chronic diseases.9
Integrated care also seeks to improve patient experience through systems redesign that improve care
coordination among providers and focuses on service delivery from a consumer’s perspective (also known as
person or people centered). There is substantial evidence that patient experience and satisfaction with the
health care system improve when concepts of integrated care are implemented.10
When these factors are taken into consideration, it is clear that integrated care is a comprehensive and highly
complex approach to redesign the health care system. Policy makers therefore need to pursue a comprehensive
and system-based approach with an emphasis on prevention, effective management of multiple diseases, and
multidisciplinary work. From a broader context, policy makers should consider the need to shift funding from
individual service providers and institutions to networks of organizations with shared goals as integrated care
systems focus mostly on constructs such as patient-centered care, care coordination, continuity of care, chronic
disease management, and integrated health care delivery.11
This report has been drafted within the scope of the Japan Policy and Human Resources Development Fund
(PHRD) Grant focusing on the sustainability of universal health coverage in Turkey. It is expected that the
report supports diagnoses of health policies to provide options that will enable the Turkish government to
identify appropriate policy and regulatory reform measures needed to achieve inclusive and sustainable
expansion in health coverage under the second phase of the Health Transformation Program (HTP).
The main focus of the report is integration at the primary health care (PHC)level. PHC is elaborated for a
number of reasons. First, PHC and public health can be considered as the core of integrated health services,12
where they address the needs of both the population and individuals, as services complementing each other.
Second, as an ultimate goal of health systems as well as of the integrated care practices, primary care can be a
good means to achieve better equity for health care and overall improvement in health 13 by focusing on all
health conditions through a number of services. Third, PHC seems to be an effective starting point for
integrating health care services in the Turkish context: the Family Medicine (FM) model was introduced about
a decade ago in Turkey within the scope of the Turkish HTP. The model has been recently supported with the
newly introduced Healthy Living Center (HLC) structures which operate on a multidisciplinary basis and
primarily address chronic and long-terms conditions. Effective integration practices among these primary care
providers is highly needed to achieve better health conditions.
The report aims to give a general framework for integrated care, to take a broad picture of the Turkish health
system from the integrated care building blocks perspective with a particular emphasis on NCDs and PHC and
take stock of current strengths, capabilities, and good practices as well as challenges that need to be addressed.
A series of in-depth literature surveys and desk studies as well as key informant interviews in the relevant
departments of the Ministry of Health (MoH) and field visits to different provinces of Turkey reveal the
progress for integrated care and room for improvement, concerning the implementation in the field as well as
9 Huber et al. 2016.
10 WHO 2015.
11 Borgermans and Devroey 2017.
12 https://www.who.int/docs/default-source/primary-health/vision.pdf.
13 http://www.euro.who.int/__data/assets/pdf_file/0006/96468/E91878.pdf.
10the system and policy design efforts at the central level. The findings from the visits and interviews, together
with the country examples, lead the reader to the recommendations and road map sections, where the report
intends to provide insight to Turkish decision/policy makers in their efforts toward integrated care.
Section 2 of the report provides an overview of the Turkish context together with the status of background
factors necessitating integrated care. Section 3 presents the essential elements of the integrated care according
to published literature. It also explores various country examples and Turkey’s corresponding state for each of
these elements and provides recommendations for efforts toward integrated care in Turkey. Section 4 includes
a road map which summarizes the recommendations with their priority levels and timeline for implementation.
2. BACKGROUND AND CONTEXT FOR INTEGRATED CARE IN TURKEY
Similar to global trends—changing disease patterns from communicable to noncommunicable diseases—the
need to revisit care delivery structures together with the diverging requirements of dealing with NCDs and
shifting of the burden of work toward primary care and thus toward prevention, early detection, and control
are the main factors that necessitate considering integrating care in Turkish health system.
2.1. TURKISH PHC SYSTEM (IN A NUTSHELL)
The first phase of the HTPs was implemented between 2003 and 2013 with the aim of improving access,
efficiency, and quality in health care. Primary care has been reformed through the creation of a new primary
care specialty and service delivery approach through the FM model, bringing family physicians’ salaries up to
those of specialists, promoting/encouraging the use of clinical guidelines, implementing well-functioning
health information and decision support systems (DSS), and designing properly aligned financial incentives.
The FM program was initially introduced as a pilot in 2005 and has been scaled up nationwide in 2010.
Primary care services are delivered in Family Medicine Centers (FMCs) by FM practitioners. FMCs are run by
FM practitioners and support staff. As of December 31, 2018, there are 26,252 FM units. The population
covered is 3,098 per active FM unit and 3,378 per active FM practitioner.14
Family Medicine Physicians (FMPs) and other clinical staff operate under performance-based contracts. They
are paid in accordance with a formula based on (a) the population served; (b) socioeconomic development
index of the province; (c) costs of mobile health services, examinations, and consumables; and (d) FMC
operating costs.
Performance-based contracts are linked with a so-called negative incentive under which up to 20 percent of
the providers’ payments are withheld if performance targets for maternal and child health (MCH), including
vaccinations, are not met.
The FM system does not play a gatekeeper role for the secondary- and tertiary-level care. In addition to FM
units, community health centers (CHCs) in the districts deliver community and public health services, including
environmental health, reproductive health, child and adolescent health services, communicable disease
management and control, and cancer screening.
The FM system is at the center of the PHC provision in Turkey. HLCs have been recently introduced to
complement and strengthen the FM model. The conceptual framework for HLCs has been developed by the
MoH, including the types of HLCs, general roles and functions, multidisciplinary services to be provided, staffing
14 Ministry of Health Public Health General Directorate, Department of Family Medicine.
11composition, and infrastructure requirements. HLCs have a complementary role within the PHC structure and
they support the FM model. HLCs mainly have two objectives. First, they aim to conduct patient follow-up
activities when referred by FMCs. Second, they aim to carry out population screening programs to identify and
stratify the population for specific diseases (especially for NCDs) and thus be proactive and plan for NCD
management. The need for more effective approaches concerning NCD management, expanded target
population screening for priority NCDs, and a proper process design for NCD screening, diagnosis, and
management has been highlighted in the recent MoH Strategic Plan of 2019–2023 and HLCs aim to complement
the FM model in that sense.
There are no standard or widely used clinical pathways in Turkey to deal with NCDs. While MCH is a part of
the performance-based contracts at the primary care level, NCDs are still not linked with such contracts in the
preventive care programs.
2.2. NCD BURDEN
NCDs and their burden are on the rise globally and Turkey is no exception. In 2016, 71.3 percent of all deaths
worldwide were due to NCDs.15 Among those NCD deaths, 72.9 percent occurred in lower and upper-middle
income countries.16
The Burden of Disease study conducted by the MoH in 2004 highlights the changing disease patterns in the
country toward chronic diseases. The study suggests that 79 percent of the deaths are due to NCDs.17 According
to the Turkish Statistical Institute (TURKSTAT) 2018 statistics, cardiovascular diseases (CVDs) and cancers are
the top two causes of mortality for the entire population (CVD 38.4 percent and cancer 19.7 percent for the
overall population). 18 The 2004 Burden of Disease study also suggests that NCDs have a substantial share
within the top 10 causes of death: ischemic heart disease ranks first - 21.7 percent, cerebrovascular disease
ranks second - 15.0 percent, chronic obstructive pulmonary disease (COPD) ranks third - 5.8 percent,
hypertensive heart disease ranks sixth - 3.0 percent, lung cancer ranks seventh - 2.7 percent, and diabetes
mellitus (DM) ranks eighth - 2.2. Recent World Health Organization (WHO) estimates suggest that NCDs
account for 89 percent of all deaths in Turkey, where CVDs account for 34 percent, cancers 23 percent, and
diabetes 5 percent.19
The Institute for Health Metrics and Evaluation (IHME) estimates also highlight the significant share of NCDs
for mortality where 8 out of the top 10 causes of death are due to NCDs. Additionally, IHME figures reveal the
concerning increase in mortality due to NCDs between 2007 and 2017 (mortality increase: 44.0 percent -
hypertensive heart disease, 32.4 percent - ischemic heart disease, 41.5 percent - COPD, and 11.0 percent -
diabetes). 20
15 http://www.who.int/healthinfo/global_burden_disease/estimates/en/.
16 http://www.who.int/healthinfo/global_burden_disease/estimates/en/.
The classification is the World Bank income groups. As of July 2017, middle-income countries (MICs) are nations with a
per capita gross national income (GNI) between US$1,005 and US$12,235.
17 https://sbu.saglik.gov.tr/Ekutuphane/Yayin/166 (accessed July 28, .2019).
18Ölüm Nedeni İstatistikleri, 2018 TUİK http://www.tuik.gov.tr/PreHaberBultenleri.do?id=30626 (accessed June 14,
2019).
19 http://www.who.int/nmh/countries/tur_en.pdf?ua=1 (accessed October 10, 2018).
20 http://www.healthdata.org/turkey.
12The WHO’s 2014 NCD Turkey country report21 suggests that the share of NCD burden in terms of disability
adjusted life years (DALYs) increased from 71 percent in 2002 to 79 percent in 2012. In terms of the number
of NCD cases, recent data from the MoH General Directorate of Health Information Systems (GDHIS) are
consistent with the discussion above and show a remarkable rise in the total number of cases for the most
common NCDs, namely diabetes, hypertension (HT), and obesity (Figures 6 and 7). 22
Changing disease patterns not only have implications on the health economy as losses due to morbidity and
mortality, but they require different perspectives to be brought in the health service delivery structures since
NCDs are chronic and require long periods of continuous care.
Figure 6 Figure 7
Turkey is experiencing a shift in population demographics toward increasing age. The share of people ages 65
years and above within the total population has increased significantly. The share of people younger than 15
years was 39 percent in 1980 and this number has reduced to 26 percent in 2008.23 The TURKSTAT recent data
also support the decline in the share of the young population and rise in the share of the older population
(Figure 8).24
Figure 8
21 https://sbu.saglik.gov.tr/Ekutuphane/kitaplar/BOH_%C3%9Clke_raporu_TR.pdf.
22(a) Figures are based on data collected through e-pulse since 2015 and (b) data from all health institutions are
included.
23 http://www.hips.hacettepe.edu.tr/TurkiyeninDemografikDonusumu_220410.pdf (accessed December 22, 2018).
24 http://www.tuik.gov.tr/UstMenu.do?metod=temelist.
13Changing lifestyle and rapid urbanization also exacerbate the situation where the population’s exposure to NCD
risk factors is high. A recent survey in Turkey25 suggests high levels of unhealthy behavior, including dietary
habits and physical activity, as well as worrying figures for overweight, obesity, and high blood pressure and
glucose levels. Almost 90 percent of the respondents have inadequate fruit and vegetable intake daily, 64
percent are overweight, 29 percent are obese (with a significantly high share for women), almost 30 percent of
the respondents have high blood pressure, and 11.5 percent have high blood glucose (Figure 9). Almost half of
the respondents have low levels of physical activity; the inactivity levels for women is very high compared to
men (61.1 percent for women versus 37.4 percent for men) (Figure 10).
Figure 9 Figure 10
The MoH Department of Healthy Nutrition and Physical Activity indicates that salt intake is high in Turkey
(twice as much as the WHO’s recommendation 26), although it has reduced from 15.0 grams per day in 2012 27
to 9.9 grams per day in 2017.28 The Department of Healthy Nutrition and Physical Activity also highlights that
obesity and diabetes are two important conditions 29 to focus on in Turkey, where the MoH aims to stop the
increasing trend for these conditions, in line with the WHO 2025 goals.30 The department indicates that halting
the increasing trend for obesity prevalence from 30.0 percent31 and diabetes prevalence from 13.7 percent32
has started. There is also progress in the 2025 target of reducing the physically inactive population by 10.0
percent; this figure reduced from 56.0 percent in 2010 to 43.6 percent in 2017.
25 http://www.who.int/ncds/surveillance/steps/WHO_Turkey_Risk_Factors_A4_ENG_19.06.2018.pdf (STEPS 2017).
26 https://www.who.int/news-room/fact-sheets/detail/salt-reduction.
27https://www.tdd.org.tr/wp-content/uploads/2018/04/t_rkiye_a_r_tuz_t_ketiminin_azalt_lmas_program_2017-2021-
1.pdf (SALTURK-2).
28National Household Health Survey in Turkey 2017,
http://www.euro.who.int/__data/assets/pdf_file/0008/383984/turkey-risk-factors-eng.pdf?ua=1.
https://www.tuseb.gov.tr/enstitu/tacese/yuklemeler/ekitap/UA_kuruluslar/WHO/DSO_Turkiye_Steps_2017.pdf
(Türkiye Hanehalkı Sağlık Araştırması 2017).
29Obesity prevalence is 30 percent according to the Turkey Nutritional Health Survey of 2010 and diabetes prevalence is
13.7 percent according to the TURDEP II .(Türkiye Diyabet, Hipertansiyon, Obezite ve Endokrinolojik Hastalıklar
Prevalans Çalışması, Turkey Diabetes, Hypertension, Obesity and Endocrinological Diseases Study ) study.
30 https://www.who.int/beat-ncds/take-action/targets/en/.
31 https://hsgm.saglik.gov.tr/depo/birimler/saglikli-beslenme-hareketli-hayat-db/Yayinlar/kitaplar/diger-
kitaplar/TBSA-Beslenme-Yayini.pdf (TBSA-2010).
32 http://www.diabetcemiyeti.org/c/turdep-2-sonuclarinin-ozeti (TURDEP-2-2009).
142.3. THE NEED FOR CHANGE IN CARE DELIVERY STRUCTURES
The rise of NCDs on a global scale calls for rethinking the health care delivery structures which are mainly
based on the diagnosis and treatment of acute conditions and finding novel ways to let the system evolve
beyond the acute care model which would effectively incorporate the notion of health care delivery for long-
term health problems.33 To this end, the concept of ‘integrated care’ is drawing interest for better and more
cost-effective health systems, and it is seen as a demand-driven response to the challenges of changing
demographics, increased NCD burden, and pressures to reduce costs on avoidable hospitalizations and services
that modern health care systems face.34
A joint study of the MoH and the WHO on cost-effective practices for NCDs and risk factors (using the
‘OneHealth Tool’) has shown that the total cost of NCDs amounted to TL 78 billion, corresponding to 3.3 percent
of gross domestic product (GDP), in 2015.35
The burden of ambulatory care in hospitals is high in Turkey. The 2017 WHO STEPwise Approach to Adult Risk
Factor Surveillance (STEPS) survey suggests that more than 81 percent of respondents’ NCD care in hospitals
was ambulatory (Figure 11) and shifting this to the primary care level is critical. The MoH statistics also support
this fact as there is an increasing trend in hospital utilization since 2013, surpassing the FM utilization, with
the exception of 2016–2017 (Figures 12 and 13).
Figure 11 Figure 12
The MoH 2017 statistics also suggest that the hospital outpatient burden is extremely high and shows an
increasing trend since the share of inpatient visits is less than 2 percent since 2013 (Figure 14). These data
clearly show that the health care is mostly hospital centric and there is a need to shift ambulatory care to the
primary care level to the extent possible.
33 WHO 2002.
34 Lyngsø et al. 2014.
35 MoH 2015.
15Figure 13 Figure 14
2.4. INTEGRATED CARE AT HIGHER POLICY LEVEL IN TUR KEY
The MoH of Turkey, being aware of the pressures posed on the health system through the changing contextual
factors, has shown commitment to address these challenges through its strategic plans. To this end, one of the
goals of the Strategic Plan covering 2013–201736 is to provide accessible, appropriate, effective, and efficient
health services to individuals and the community. The MoH intends to improve the integration and continuity
of care by strengthening the role of PHC, especially through strengthening the integration of other PHC services
into the FM model and through strengthening the integration of the FM model into hospital care and laboratory
services. The plan also suggests strengthening the infrastructure and technological capacity of FM laboratory
services, developing a system that will enable family physicians to consult with relevant specialists, improving
the hospital appointment system by integrating it into the FM system, and improving laboratory services by
integrating them into the FM system.
The Strategic Plan 2013–2017 also emphasizes the MoH’s objective to control and reduce complications of
NCDs through improving the quality of health care services for chronic diseases and establishing a system to
manage the complications of chronic diseases by integrating PHC and hospital services and developing and
using clinical quality standards.
The recently drafted MoH Strategic Plan 2019–2023 emphasizes the increasing burden of NCDs as their share
in overall disease burden increased from 69.0 percent in 2002 to 82.4 percent in 2017. The plan highlights the
need to improve health care delivery models and ensure continuity, proactive approaches, and close patient
follow-up for NCD management.
One of the main goals of the new Strategic Plan focuses on preventing the exposure of the population to
environmental risks and promoting healthy lifestyles through healthy nutrition and a physically active lifestyle
and increasing health literacy. Another goal is to assign a central role to the FM system, to make patients
responsible for their health (as stakeholders of health) and support the FM model through integrated care
models which bring different disciplines 37 together at the primary level. This new strengthened PHC model is
expected to prioritize NCD management. The MoH intends to carry out systematic population-based screenings
since early detection is one of the most important elements of NCD management. Both the screening processes
and NCD management processes will be defined from end to end, standardized, and supported with technology.
Physical infrastructure of PHC institutions will be improved and FMPs will play a more active role in the
36 https://sgb.saglik.gov.tr/Shared%20Documents/OrtaAlan/15.02.2012%20stratejik%20plan.pdf.
37 Such as dietitian, physiotherapist, and psychologist.
16screening, diagnosis, patient education, and management of NCDs. Capabilities of PHC staff will be enhanced
through improvements in the curriculum and in-house trainings.
Tables 1 and 2 provide the details of performance targets related to integrated care and NCDs and the
integrated care related context of the MoH Strategic Plan 2019–2023.
Table 1
Indicators related to integrated care and 2019 value Planning period 2023 target
NCDs baseline value
Number of FMCs (cumulative) 27,000 26,252 (2018) 32,190
Population per FMP 3,069 3,098 (2018) 2,700
Share of population who do not visit FMCs 22.26% 22.40% (2018) 18.25%
within registered population
Yearly per capita FMC visits (cumulative) 3.3 3.1 (2018) 4.0
Number of HLCs (cumulative) 205 193 (2018) 275
NCDs whose screening and follow-up processes 3 0 (2018) 7
defined at the primary level and integrated
within Disease Management Platform
(cumulative)
Colorectal cancer early diagnosis rate (phase 0– 35.5% 35.4% 37.0%
1)
Breast cancer early diagnosis rate (phase 0–1) 50.3% 50.0% 52.0%
Cervical cancer early diagnosis rate (phase 0) 58.0% 57.8% 59.5%
HT screening coverage 10% 0% (2018) 50%
CVD risk assessment coverage 20% — 60%
Obesity prevalence (15+ population) 31.0% 31.5% (2017) 29.1%
Overweight prevalence (15+ population) 35.8% 35.9% (2017) 35.5%
Physically inactive population prevalence (15+ 38.0% 39.6% (2018) 32.0%
population)
DM prevalence 12.4% 12.5% (2017) 12.1%
HT prevalence — 27.9% (2017) 24.9%
Salt intake per capita per day 9.4 g 10.2 g (2017) 7.7 g
Level of awareness of activities concerning — 30% (2018) 60%
health literacy
Share of population with sufficient or superior — 31.1% (2017) 40.0%
health literacy
17Indicators related to integrated care and 2019 value Planning period 2023 target
NCDs baseline value
Number of nurses and midwives per 100,000 312 302 (2018) 350
population
Share of population who are satisfied with FMC 72% 72% 76%
services
Number of active profiles in e-pulse individual 11 million 9.4 million (2018) 15 million
health system platform
Table 2
Goal 1: Promote and expand healthy lifestyles
Encourage healthy dietary habits through
(i) The introduction of incentive mechanisms that would encourage people for healthy dietary habits and physically active
lifestyle;
(ii) Systematic communication activities to increase public awareness; and
(iii) Efforts to increase health literacy (increase awareness and competency of health workers on population health literacy,
design digital platforms, applications, and processes that would facilitate increasing population health literacy and
introducing health literacy volunteer model).
Goal 2: Strengthen PHC and increase its effectiveness within the health system
Provide multidisciplinary and highly preferred PHC through a strengthened FM structure.
Transform the primary care performance model so that it is quality based, satisfaction based, and results based for all stakeholders.
Establish standardized PHC processes where all steps are planned and incorporate related technological devices as well as ability to
effectively follow patients in the processes.
Improve primary care staff capacity and qualifications through improvements in specialization programs and training curricula and
through in-house training.
Goal 3: Ensure accessible, effective, efficient, and high-quality care delivery
Improve clinical quality of health care.
Ensure effectiveness and productivity for outpatient and emergency care.
Improve accessibility and sustainability of health care services.
Goal 4: Introduce Integrated Health Care Model
Carry out NCD screening at PHC institutions on HT, DM, and CVD risk assessment.
Establish a regular individual-based NCD follow-up system which would incorporate information on different areas such as patient
history, patient’s other medical conditions, patient’s communication preferences, and behavioral patterns.
Change the public perception toward PHC by improving the PHC strategic design to include the following elements:
(i) Design a new PHC service delivery model where PHC will assume a priority role for NCD follow-up. Ensure that the FM
system is at the center and patients are the continuous health stakeholders. To support and strengthen the FM model, introduce
different disciplines such as dietitian, physiotherapist, and psychologist to operate at the PHC and provide integrated services.
(ii) Redesign the FM performance system to be more effective and to include elements such as quality, satisfaction, and results-
based focus and to reflect the MoH priorities.
(iii) Design all PHC processes end to end for long-terms cases such as NCDs. The processes should be standard and should aim to
improve the patient experience. The processes will include case-based clinical treatment protocols, decision trees, service
points, actors to assume the roles, and service delivery flow diagrams. Clinical and administrative processes also have to be
thoroughly reflected to the HIS and there should be perfect information flow between stakeholders.
18(iv) Increase PHC staff competencies through effective FM training schemes that are redesigned and improved to reflect effective
NCD management at the primary level.
Increase effectiveness of the early diagnosis and management of complications of NCDs.
Prevent, maintain, and improve the mental health of people.
Strengthen the multistakeholder governance model to improve health responsibility.
Goal 5: Ensure patient and provider satisfaction and health system sustainability
Increase patient satisfaction.
Continuously improve health worker satisfaction.
Increase the use of information technologies in the health care provision and decision-making processes to strengthen the health
system.
Increase the effectiveness of human resource planning and skills building.
Improve effectiveness and efficiency of health management.
3. ESSENTIAL COMPONENTS OF INTEGRATED CARE: OVERVIEW, COUNTRY EXAMPLES,
STATUS OF TURKEY, AND RECOMMENDATIONS
The widespread move toward integrated care is being driven by the increasing burden of chronic disease,
multimorbidity, and high-risk populations, which present an overwhelming case to better manage the
processes and outcomes related to the needs of the population that a health care system serves. Evidence
suggests that an integrated care approach can improve care quality, patient/staff experience, process efficiency
and effectiveness; reduce costs; and improve patient outcomes and well-being.38
Integrated care occurs on different dimensional areas of the health system, including organizational, functional,
and service integration. Organizational integration usually includes formal mergers of health care provider
systems (bringing together different sectors of the health care) or establishing collective structures for
coordinated provider networks often through contracts or policy. Functional integration recognizes and
necessitates the need to integrate nonclinical business practices (such as back-office activities) and electronic
patient records. Service integration focuses on bringing different clinical services together at the organizational
level through teams of multidisciplinary professionals.39 (Figure 15)
Figure 15
38 Bertram et al. 2018; Rosland et al. 2017.
39 WHO 2016b.
https://www.nuffieldtrust.org.uk/files/2017-01/where-next-integrated-care-english-nhs-web-final.pdf.
19Integration is often referred to as vertical or horizontal. Horizontal integration is defined as establishing formal
care delivery between two or more health care entities at the same stage/level in the process of care, such as
integrating two hospitals. Vertical integration involves organizations addressing care needs at different levels
of care such as primary care and secondary care or general practice and the community health care. In terms
of the scale, integrated care can be implemented at three levels: micro, meso, and macro. The micro level
focuses on the individual care experience made through a personalized care plan. The meso level represents
integrated care for a specific group or population with the same disease or condition. Implementing care at the
macro level entails needs stratification for an entire population and then tailoring services to attend to those
needs.
Depending on the level of intensity, integrated care models range from partial to complete. While the latter
aims to integrate health and social sectors into a new organizational model, the former is about forming
voluntary links to support integration and to enhance coordination between health and social sectors.40 Some
integration models focus on the needs of high-risk groups, others focus on groups with specific chronic
diseases.41
The WHO outlines three models of integrated care: (a) individual models where the goal is to facilitate
coordination among providers to reduce fragmentation and to improve chronic illness/disease management
(case management, individual care plans, patient-centered medical home, personal health budget); (b) models
that target wider groups of patients (chronic care model, integrated models for frail and the elderly, and
disease-specific models); and (c) population-based models (Kaiser Permanente USA, Veterans Health
Administration, USA [VHA], and Integrated Care Basque Country).42 The WHO notes, however, that the broader
models often contain subsets and portions of disease and case management aspects found in individual models
of integrated care.
As the integrated care approach aims to improve access, quality, and continuity of health care services, the role
of the primary care in integrated care settings becomes crucial. In fact, the basic functions of the primary care—
first point of contact; continuous, comprehensive, and coordinated care—make primary care the starting point
for efforts to improve and integrate care. The integration of the biomedical, psychological, and social
dimensions of health and well-being is the core value of primary care and addresses both the concepts of
person-focused and population-based care, which constitute the guiding principles to achieve better care
coordination across the care continuum. Health systems where the principles of primary care (first point of
contact; continuous, comprehensive, and coordinated care) actively function achieve better health outcomes
and improved health care equity when compared with systems focusing on specialty care. In fact, several high-
income country settings reveal that health care service integration is disrupted by the existence of fragmented
health service provision which in turn brings about suboptimal care and increased costs due to duplication and
poor quality of care.43
There is now substantial evidence that outlines the essential components of integrated care, delivery strategies,
success factors, and challenges faced by many countries and health care systems as they move to transform
their health system toward a more integrated model.
40 WHO 2016b.
41 WHO 2016.
42 WHO 2016.
43 Valentijn et al. 2013.
20You can also read