2018-19 Pre-Budget Submission - Orthotist/Prosthetists: Supporting the Australian Community - Australian Orthotic Prosthetic ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2018-19 Pre-Budget Submission Orthotist/Prosthetists: Supporting the Australian Community

2018-19 Pre-Budget Submission 1 Introduction The Australian Orthotic Prosthetic Association (AOPA) is the peak professional body representing Orthotist/Prosthetists in Australia, with members comprising 80% of the practicing profession. AOPA is primarily responsible for regulating the profession and is a founding member of the National Alliance of Self Regulating Health Professions (NASRHP) in partnership with other professional organisations, including Speech Pathology Australia, the Australian Association of Social Workers and Exercise and Sports Science Australia. Orthotist/Prosthetists assess the physical and functional limitations of people resulting from disease, illness, trauma and disability, including limb amputation, diabetes and neuromuscular conditions, such as Cerebral Palsy and Stroke. Orthotic and Prosthetic services may involve the provision of orthoses and prostheses to restore function, prevent deterioration, and improve quality of life. Orthotist/Prosthetists are commonly found in Australian hospitals, private clinics, research institutions and rural and remote regions, working independently and as part of multidisciplinary healthcare teams to support the Australian community. The 2018-19 Budget provides an opportunity to secure considerable savings whilst reducing the significant number of avoidable hospital admissions. The Australian Orthotic Prosthetic Association Pre-Budget submission details an easily implementable amendment to the Medicare Benefits Schedule that will make a meaningful difference in the lives of many Australians. Contact The Australian Orthotic Prosthetic Association PO Box 1219, Greythorn, Victoria 3014 (03) 9816 4620 www.aopa.org.au Leigh Clarke – Executive Officer leigh.clarke@aopa.org.au
2018-19 Pre-Budget Submission 2
Executive Summary
Australians experiencing chronic disease, including diabetes and stroke, are currently unable to
access vital Orthotic services in the primary care setting in a timely manner. This is because
these services are not included in the Medicare Benefits Schedule Allied Health items.
Research clearly indicates that this inability to access Orthotic services results in:
• Significantly increased healthcare costs
• An increase in the number of lower limb amputations
• Avoidable hospital admissions
• Reduced workforce and economic participation
Research indicates that the inclusion of an Orthotic Allied Health item in the Medicare Benefits
Schedule would provide the Commonwealth Government an opportunity to:
• Realise savings of at least $2.7 billion over 5 years by implementing evidence-based
care for Australians with diabetes-related foot ulcers
• Significantly reduce the 10,000 hospital admissions arising due to diabetes-related foot
ulcers
• Reduce the incidence of falls and associated hospital admissions following stroke
• Improve the quality of life for 1.7 million Australians experiencing diabetes and 475,000
Australians living with the effects of stroke
• Allow Australians experiencing chronic diseases access to Orthotic services, addressing
part of the 39% of preventable hospital admissions that occur due to chronic disease
Recommendation
The Australian Orthotic Prosthetic Association requests:
1. That an Orthotic service item is added to the Medicare Benefits Schedule Allied Health
items
2018-19 Pre-Budget Submission 3 The Impact of Chronic Disease Diabetes Approximately 1.7 million Australians have diabetes and an additional 280 will develop diabetes every day, representing the ‘epidemic of the 21st century and the biggest challenge confronting Australia’s health system’.1 The total annual cost of diabetes in Australia is estimated at $14.6 billion.2 Australia has the second highest lower limb amputation rate in the developed world, with more than 4,400 amputations every year in Australia as a direct result of diabetes.3 This number is increasing; between 2000 and 2010, the number of lower limb amputations in Australia increased by 14% from approximately 7000 to 8000 per annum.4 Amputation is typically preceded by a diabetes-related foot ulcer or lower limb wound.5 In Australia, there are 10,000 hospital admissions every year for avoidable diabetes-related foot ulcers.6 Stroke In 2017, there will have been almost 56,000 new and recurrent strokes and more than 475,000 Australians living with the effects of stroke.7 The number of persons living with the effects of stroke is expected to increase to 1,000,000 by 2050.8 The total annual cost of stroke in Australia is estimated at $5 billion.9 Approximately 65% of stroke survivors experience a disability which impairs their ability to perform activities of daily living unassisted and 30% of stroke survivors are of working age.10 More than two-thirds of stroke survivors experience mobility difficulties and an impaired ability to walk,11 resulting in an increased risk of falls,12 significantly reduced workforce participation and reduced quality of life.13 Falls are the primary medical complication following stroke and stroke survivors experience more severe consequences as a result of falls when compared to other persons.14 The incidence of fractures following falls is four times higher for stroke survivors than the general population.15
2018-19 Pre-Budget Submission 4
Reducing the Impact of Chronic Disease
Orthotic Health Services
Research clearly demonstrates that Orthotic services reduce the incidence of amputation and
diabetes-related foot ulcers that result in excessive healthcare costs and preventable hospital
admissions.16 An Orthotist may employ a number of interventions, including total contact
casting and the provision of orthoses. However, these interventions are only effective when
provided at the appropriate time.17 Orthotic services similarly reduce the risk of falls and
improve quality of life for stroke survivors.18 Orthotic intervention for stroke survivors results in
increased activity, allowing for increased economic and workforce participation.19
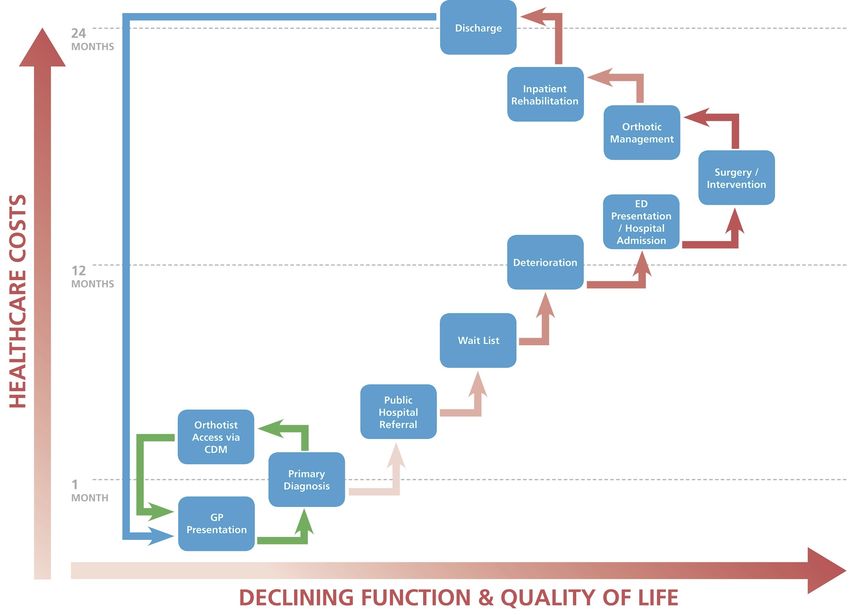
Figure 1 - A comparison of existing and proposed access to Orthotic Services for Australians with chronic disease.
The omission of Orthotic services from the Medicare Benefits Schedule represents the primary
barrier for Australians with chronic disease accessing these vital services. An illustrative
example of the relationship between the patient pathway and health cost is provided above.
The current patient pathway is indicated in red, whereby a patient does not receive early
access to an Orthotist, experiences deterioration of their condition (either amputation,
ulceration or falls) resulting in hospitalisation, increased health costs and a reduction in function
and quality of life. The proposed pathway is indicated in green, illustrating early access to
Orthotic services via a Medicare Chronic Disease Management item and the avoidance of
further complications and associated costs.2018-19 Pre-Budget Submission 5
This pathway emphasises that access to Orthotic services is the most appropriate intervention
to avoid the 10,000 hospital admissions that directly result from diabetes-related foot ulcers.
Early access to Orthotic Services will reduce the incidence of amputation and associated
costs.20 Similarly, access to Orthotic services will reduce the incidence of falls for stroke
survivors, resulting in a reduction of hospital admissions and improved quality of life.21
Economic Impact of Improved Access to Orthotic Services
The economic impact of timely access to Orthotic services is well supported by research. The
most recent Australian research estimates that if all persons at risk of developing diabetes-
related foot ulcers were to receive optimal care, including Orthotic services, the cost savings
are likely to be $2.7 billion over 5 years.22 In the United Kingdom, it is estimated that access to
Orthotic services alone in the primary care sector will provide savings of £390 million per
annum.23 Economic studies allow a comparison between the cost of providing Orthotic services
to heal diabetes-related foot ulcers and the cost of amputation if Orthotic services are not
provided.
In the United Kingdom, the cost of healing a
diabetes-related foot ulcer is between £3,000
and £7,500, whereas the cost of amputation
is £65,000.24 In Sweden, a similar cost
advantage exists, where the cost of healing a
diabetes-related foot ulcer is SEK 51,000 and
the cost of amputation is SEK 344,000.25 In
the United States, it is estimated that healing
diabetes-related foot ulcers saves US$38,126
when compared to the cost of amputation.26
These costs do not accurately reflect the
ongoing disability cost of providing lifetime
prosthetic care. Access to Orthotic services
via a Medicare Chronic Disease Management
item will lead to a reduced incidence of
‘Economic studies allow a comparison between the
amputation and a significant reduction in health cost of providing Orthotic services…and the cost of
costs. amputation if Orthotic services are not provided.’2018-19 Pre-Budget Submission 6
Recommendations
Research indicates that the cost of chronic disease, including diabetes and stroke, is significant
and likely to increase exponentially. However, access to Orthotic services via a Medicare
Chronic Disease Management item will provide significant cost benefits, as well as a reduction
in the incidence of amputation and hospital admissions. Therefore, the Australian Orthotic
Prosthetic Association recommends:
1. That an Orthotic service item is added to the Medicare Benefits Schedule Allied Health
items, allowing Australians with chronic disease access to vital Orthotic services and
providing significant cost benefits.2018-19 Pre-Budget Submission 7
References
1. Diabetes Australia, ‘Submission into the Standing Committee on Health’s inquiry into Chronic Disease Prevention and Management in
Primary Health Care’, 2015. Available at: https://www.diabetesaustralia.com.au/submissions [Accessed 10 December 2017].
2. Lee CM, Colagiuri R, Magliano DJ, Cameron AJ, Shaw J, Zimmet P, Colagiuri S., ‘The cost of diabetes in adults in Australia’, Diabetes
Research and Clinical Practice, vol. 99, no. 3, 2013.
3. Australian Commission on Safety and Quality in Health Care, ‘The Australian Atlas of Healthcare Variation, 2015’. ACSQHC, New South
Wales, 2015.
4. Dillon MD, Kohler F, Peeva V, ‘Incidence of Lower Limb Amputation in Australian Hospitals from 2000 to 2010’, Prosthetics and
Orthotics International, Available at http://poi.sagepub.com/content/early/2013/06/10/0309364613490441, 2013.
5. Australian Institute of Health and Welfare, ‘Diabetes: Australian facts. AIHW Cat. No. CVD 40; Diabetes Series No. 8’. AIHW, Canberra,
2008.
6. Davis WA, Norman PE, Bruce DG, Davis TM, ‘Predictors, consequences and costs of diabetes-related lower extremity amputation
complicating type 2 diabetes: the Fremantle Diabetes Study’, Diabetologica, vol. 49, no. 11, 2006.
7. Deloitte Access Economics, ‘The economic impact of stroke’, Australia, 2013.
8. Deloitte Access Economics, ‘Stroke in Australia – No postcode untouched’, 2017.
9. Deloitte Access Economics, ‘The economic impact of stroke’, Australia, 2013.
10. Deloitte Access Economics, ‘The economic impact of stroke’, Australia, 2013.
11. Jorgensen H, Nakayama H, Raaschou H, Olsen T, ‘Recovery of walking function in stroke patients - The Copenhagen Stroke Study,’
Archives of Physical Medicine and Rehabilitation, vol. 76, no. 1, 1995.
12. Divani AA, Vazquez G, Barrett AM, Asadollahi M, Luft AR, ‘Risk factors associated with injury attributed to falling among elderly
population with a history of stroke,’ Stroke, vol. 40, no. 3, 2009.
13. Paul SL, Sturnm JW, Dewey HM, Donnan GA, Macdonell AL, Thrift, AG, ‘Long - term outcome in the North West Melbourne Stroke
Incidence Study: Predictors of Quality of Life at 5 years After Stroke,’ Stroke, vol. 36, 2005.
14. Holloway RG, Tuttle D, Baird T, Skelton WK, ‘The safety of hospital stroke care,’ Neurology, vol. 68, no. 8, 2007.
15. Mackintosh SLH, Goldie P, Hill K, ‘Falls incidence and factors associated with falling in older, community - dwelling, chronic stroke
survivors (>1 year after stroke) and matched controls,’ Aging Clinical and Experimental Research., vol. 17, 2005.
16. Fernandez MLG, Lozanm RM, Diaz MIG, Jurado M, Hernandez DM, ‘How effective is orthotic treatment in patients with recurrent
diabetic foot ulcers’, Journal American Podiatric Medicine Association, vol. 103, no. 4, 2013.
17. International Working Group on the Diabetic Foot, ‘Consensus - Footwear and off-loading for the diabetic foot: International Consensus
on the Diabetic Foot and Practical Guidelines on the Management and Prevention of the Diabetic Foot.’ IWGDF, 2011.
18. Tyson SF, Kent RM, ‘Orthotic devices after stroke and other non-progressive brain lesions’, Cochrane Database of Systematic Reviews
2009;(1):CD003694.
19. Tyson SF, Kent RM, ‘Orthotic devices after stroke and other non-progressive brain lesions’, Cochrane Database of Systematic Reviews
2009;(1):CD003694.
20. Fernandez MLG, Lozanm RM, Diaz MIG, Jurado M, Hernandez DM, ‘How effective is orthotic treatment in patients with recurrent
diabetic foot ulcers’, Journal American Podiatric Medicine Association, vol. 103, no. 4, 2013.
21. Tyson SF, Kent RM, ‘Orthotic devices after stroke and other non-progressive brain lesions’, Cochrane Database of Systematic Reviews
2009;(1):CD003694.
22. Cheng Q, Lazzarinia PA, Gibb M, Derhy PH, Kinnear EM, Burn E, Graves N, Norman RE, ‘A cost-effectiveness analysis of optimal care
for diabetic foot ulcers in Australia’ International Wound Journal, vol. 14, 2017.
23. Boxer P, Flynn T, ‘Orthotic Pathfinder: A Patient focused strategy and proven implementation plan to improve and expand access to
orthotic care services and transform the quality of care delivered’, Business Solutions, UK, 2004.
24. Hutton J, Hurry M, ‘Orthotic Service in the NHS: Improving Service Provision’, York Health Economics Consortium, 2009.
25. Apelqvist J, Ragnarson-Tennvall G, Persson U, Larsson J. ‘Diabetic foot ulcers in a multidisciplinary setting. An economic analysis of
primary healing and healing with amputation’, Journal of Internal Medicine, 1994.
26. Driver VR, Fabbi M, Lavery L, Gibbon G, ‘The cost of diabetic foot: the economic case for the limb salvage team’ Journal of Vascular
Surgery, vol. 52, 2010.You can also read