2019 The State of Obesity: BETTER POLICIES FOR A HEALTHIER AMERICA - Trust for America's Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The State
ISSUE REPORT
of Obesity:
BETTER POLICIES FOR
A HEALTHIER AMERICA 2019
With Special Feature on Racial and Ethnic
Disparities in Obesity and Advancing Health Equity
SEPTEMBER 2019
Acknowledgments
Trust for America’s Health (TFAH) is a nonprofit, nonpartisan The Robert Wood Johnson Foundation (RWJF) provided support
public health policy, research, and advocacy organization that for this report. Opinions in it are TFAH’s and do not necessarily
promotes optimal health for every person and community, and reflect the views of RWJF.
makes the prevention of illness and injury a national priority.
TFAH BOARD OF DIRECTORS
Gail Christopher, DN Cynthia M. Harris, PhD, DABT Eduardo Sanchez, MD, MPH
Chair of the TFAH Board Director and Professor, Institute of Public Health, Chief Medical Officer for Prevention and Chief of
President and Founder, Florida A&M University the Center for Health Metrics and Evaluation,
Ntianu Center for Healing and Nature American Heart Association
David Lakey, MD
Former Senior Advisor and Vice President,
Chief Medical Officer and Vice Chancellor for Umair A. Shah, MD, MPH
W.K. Kellogg Foundation
Health Affairs, Executive Director,
David Fleming, MD The University of Texas System Harris County (Texas) Public Health
Vice Chair of the TFAH Board
Octavio Martinez Jr., MD, DrPH, MBA, FAPA Vincente Ventimiglia, JD
Vice President of Global Health Programs, PATH
Executive Director, Chairman of Board of Managers,
Robert T. Harris, MD Hogg Foundation for Mental Health, Leavitt Partners
Treasurer of the TFAH Board University of Texas at Austin
Senior Medical Director, TFAH LEADERSHIP STAFF
Karen Remley, MD, MBA, MPH, FAAP
General Dynamics Information Technology
Senior Fellow, De Beaumont Foundation John Auerbach, MBA
Theodore Spencer Former CEO and Executive Vice President, President and CEO
Secretary of the TFAH Board American Academy of Pediatrics J. Nadine Gracia, MD, MSCE
Founding Board Member
John A. Rich, MD, MPH Executive Vice President and COO
Stephanie Mayfield Gibson, MD Co-Director,
Senior Physician Advisor and Population Health Center for Nonviolence and Social Justice,
Consultant; Former Senior Vice President and Drexel University School of Public Health
Chief Medical Officer for Population Health,
KentuckyOne Health
REPORT AUTHORS REVIEWERS
Molly Warren, SM Sana Chehimi, MPH Elsie Taveras, MD, MPH
Senior Health Policy Researcher and Analyst, Director of Policy and Advocacy, Executive Director,
Trust for America’s Health Prevention Institute Kraft Center for Community Health
Division Chief, General Academic Pediatrics,
Stacy Beck, JD Bill Dietz, MD, PhD
Massachusetts General Hospital
Consultant Chair,
Conrad Taff Professor of Nutrition in the
Sumner M. Redstone Global Center for
Daphne Delgado, MPH Department of Pediatrics,
Prevention and Wellness
Senior Government Relations Manager, Harvard Medical School
Milken Institute School of Public Health,
Trust for America’s Health Professor in the Department of Nutrition,
The George Washington University
Harvard T.H Chan School of Public Health
CONTRIBUTORS Shiriki Kumanyika, PhD, MS, MPH
Research Professor in Community Health and
Zarah Ghiasuddin
Prevention,
Research and Communications Intern,
Drexel University Dornsife School of Public Health
Trust for America’s Health
Professor Emerita of Epidemiology,
Vinu Ilakkuvan, DrPH University of Pennsylvania
Consultant
Sarah Ketchen Lipson, PhD, EdM
Assistant Professor,
Boston University School of Public Health
Associate Director,
The Healthy Minds Network
2 TFAH • tfah.org
The State of
TABLE OF CONTENTS
Table of Contents
INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . 4 Role of Child Care and Education Obesity
Settings . . . . . . . . . . . . . . . . . . . . . . . . . . 47
SECTION I. S
pecial Feature: Racial And Ethnic E
arly Child Care and Education: Head Start,
Disparities In Obesity . . . . . . . . 10 State Requirements, and CDC Initiatives . 47
E
lementary and Secondary Education: Local
Obesity Data by Race/Ethnicity . . . . . . . . . 13
Wellness Policies, Smart Snacks, and CDC
Policy Considerations and Approaches . . . . 16 Initiatives . . . . . . . . . . . . . . . . . . . . . . . . 48
S
chool-Based Physical Activity and Physical
Meet Two Health Equity Leaders . . . . . . . . 18 Education . . . . . . . . . . . . . . . . . . . . . . . . 49
After-School Settings . . . . . . . . . . . . . . . . 49
SECTION II. O
besity-Related Data and
Trends . . . . . . . . . . . . . . . . . . 22 Community Policies and Programs . . . . . . . 50
B
uilt Environment: Community Design and
Trends in Adult Obesity . . . . . . . . . . . . . . . 22
Land Use, and Safe Routes to Schools . . 50
Trends in Childhood Obesity . . . . . . . . . . . . 28 CDC Community Initiatives . . . . . . . . . . . . 52
Healthcare Coverage and Programs . . . . . . 55
SECTION III. O
besity-Related Policies and
Programs . . . . . . . . . . . . . . . . 33 Medicare and Medicaid . . . . . . . . . . . . . . 55
Healthcare and Hospital Programs . . . . . . 57
Nutrition Assistance and Education . . . . . . 33
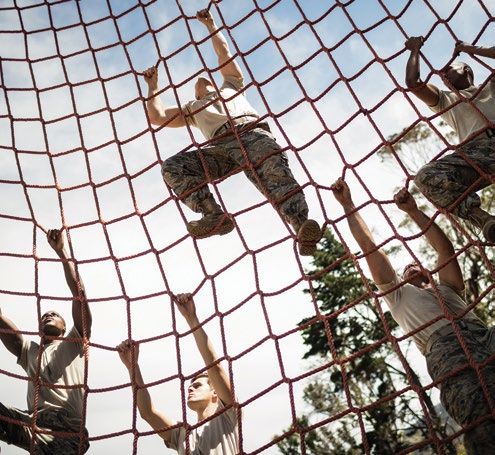
Federal Nutrition Assistance: WIC, School Obesity and the Military . . . . . . . . . . . . . . . 59
Nutrition Programs, SNAP and Nutrition Recruitment . . . . . . . . . . . . . . . . . . . . . . 59
Incentive Programs . . . . . . . . . . . . . . . . . 34 Service Members and Families . . . . . . . . 59
Nutrition Education and Information: Veterans . . . . . . . . . . . . . . . . . . . . . . . . 60
Dietary Guidelines, and Nutrition and
Menu Labels . . . . . . . . . . . . . . . . . . . 41
SECTION IV. Recommendations . . . . . . . . . 61
Economics of What We Eat . . . . . . . . . . . . 43
Food and Beverage Marketing . . . . . . . . 43 APPENDIX: O
besity-Related Indicators and
Policies By State . . . . . . . . . . . 69
Fiscal and Tax Policies that Promote
Healthy Eating: Beverage Taxes, Healthy
Food Financing Initiative, and the New REFERENCES . . . . . . . . . . . . . . . . . . . . . . 74
Markets Tax Credit . . . . . . . . . . . . . . . . 44
View this report online at tfah.org/stateofobesity2019. For more data on obesity
prevalence, policies, and programs, visit stateofobesity.org.
SEPTEMBER 2019
I NT RO D UC TION
The State of
INTRODUCTIION
Introduction
Obesity
Obesity is a growing epidemic in the United States—and has been
for decades. Currently, about one in three Americans of all ages—
or more than 100 million people—have obesity.1 Between the most
recent National Health and Nutrition Examination Survey (2015–
2016) and the 1988–1994 survey, there has been an extraordinary
increase in the adult obesity rate of more than 70 percent, and an
increase in a childhood obesity rate of 85 percent.2,3
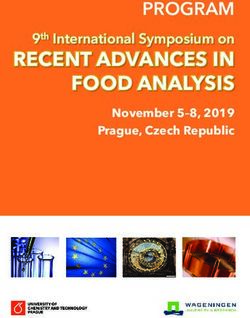
In 2015-2016, 93.3 million adults and
13.7 million children had obesity out
of a total of 309 million Americans
n Adults n Children
Percent of Adults and Youth with Obesity, 1988–2016
50
39.6%
40
30
18.5%
20
10
SEPTEMBER 2019
0
94 00 02 04 06 08 10 12 14 16
–19 –20 –20 –20 –20 –20 –20 –20 –20 –20
88 99 01 03 05 07 09 11 13 15
19 19 20 20 20 20 20 20 20 20
Percent of Adults (Age 20+) with Obesity Percent of Youth Age 2–19 with Obesity
Source: NHANES
New 2018 data from the Behavioral Risk
Factor Surveillance System (BRFSS) Adult Obesity Rates by State, 2018
show that adult obesity rates across the
United States are continuing to climb. In WA
MT ME
2018, nine states had adult obesity rates ND
OR MN VT
above 35 percent—including Kentucky, ID NH
SD WI NY MA
Missouri, and North Dakota for the first WY MI
CT RI
time—and more than half of adults in NE IA PA NJ
NV
OH DE
every state were either overweight or CA UT
IL IN
MD
CO WV DC
had obesity. Between 2017 and 2018, KS MO VA
KY
seven states had statistically significant NC
AZ TN
increases in the adult obesity rate, NM
OK
AR SC
and only one state had a statistically MS AL
GA
significant decrease. When looking over TX LA
the last five years (between 2013 and
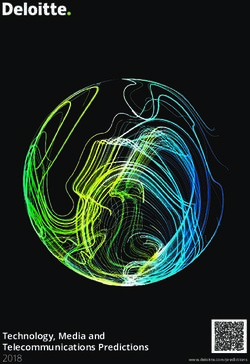
Percent of Adults and Youth with Obesity by Race/Ethnicity, 2015–2016
60%
50%
46.8% 47%
40% 37.9%
30%
25.8%
22%
20%
12.7% 14.1%
11%
10%
0%
Asian Black Latino White Asian Black Latino White
Adults Adults Adults Adults Children Children Children Children
Source: NHANES
While obesity affects all populations, programs are necessary, it’s important
obesity rates are higher in certain to prioritize those populations and
populations where social and economic communities with the highest levels
conditions contribute to persistent of obesity and, historically, the least
health inequities—almost half of Latino government and private investment.
(47 percent) and Black (46.8 percent) Focusing on these communities is both
adults had obesity in 2015–2016, which a matter of equity, as well as offers the
is 24 percent higher than Whites (37.9 greatest opportunity for progress.
percent).9 This pattern holds true for
This is the 16th annual report by Trust
children: obesity rates are substantially
for America’s Health on the obesity
higher among Latino children (25.8
crisis in the United States; we track
percent) and Black children (22
the latest data and policies, and we
percent) than among White children
offer recommendations. This year, we
(14.1 percent). Currently too many
added a feature section to conduct
Americans, particularly those who live
an in-depth exploration—including
in poverty and/or face racism and other
interviews with experts—of a critical
forms of discrimination, face barriers
single aspect of the obesity issue:
to healthy behavior. All Americans—
the intersection of racial and ethnic
no matter where they live, how much
inequity and obesity. Additionally, this
money they make, or what their racial
report, as in previous years, includes
or ethnic background is—must be able
sections on: the latest data available on
to make healthy choices for themselves
adult and childhood obesity (see page
and their families, and communities
22), key current and emerging policies
must support them in doing so through
(page 33), and, finally, recommended
innovative programs and services. When
policy actions (page 61).
considering what additional policies and
6 TFAH • tfah.org
CONSEQUENCES OF OBESITY
Obesity hurts Americans individually, at l Children with obesity are also at missed time at school and work, lower
the community level, and as a nation at greater risk for certain diseases, like productivity, premature mortality, and
large—increasing the risk of physical and type 2 diabetes, high blood pressure, increased transportation costs.28
mental disease, and premature death; and depression.21,22,23,24 A 2017 study
l Being overweight or having obesity is
causing additional healthcare costs and of new diabetes diagnoses in children
the most common reason young adults
productivity losses; and reducing the between the years 2001 and 2012
are ineligible for military service. In
nation’s military readiness. found a 7.1 percent annual increase in
addition, the proportion of active-duty
cases diagnosed per 100,000 children
l Obesity increases the risk of a range service members who have obesity
ages 10 to 19 (versus 1.4 percent
of diseases for adults—including type has risen in the past decade—along
increase annually for type 1 diabetes,
2 diabetes, high blood pressure, heart with healthcare costs, injuries, and
which is not associated with obesity).25
disease, stroke, arthritis, depression, lost work time. According to Mission:
sleep apnea, liver disease, kidney l Studies show individuals with obesity Readiness, a nonpartisan group of
disease, gallbladder disease, pregnancy had substantially higher medical costs more than 700 retired admirals and
complications, and many types of than healthy-weight individuals.26 generals, excess weight prevents
cancer—and an overall risk of higher A 2016 study found that obesity nearly one in three young adults from
mortality.10,11,12,13 14,15, 16,17,18,19 A 2019 increased annual medical expenses qualifying for military service, and
study attributes 80,000 cancer cases in the United States by $149 billion. 27
the U.S. Department of Defense is
in 2015, or 5.2 percent of all new Indirect, or non-medical, costs from spending more than $1 billion each
diagnoses, to poor diet and obesity. 20
obesity also run into the billions due to year on obesity-related issues.29,30
TFAH • tfah.org 7
2019 STATE OF OBESITY RECOMMENDATIONS
Since obesity has a multitude of other federal programs that support l Add nutrition as a core program tenet
contributing causes and potential student physical education. to SNAP and identify ways to improve
solutions, Trust for America’s Health diet quality, without reducing access
l Routinely update the Physical Activity
directs its recommendations to government or benefits, though new pilot initiatives
Guidelines for Americans based
officials at the national, state, and local and strengthening current programs.
on the most current scientific and
levels. TFAH’s two guiding principles when
medical knowledge, and support a l T he Dietary Guidelines for Americans
making these recommendations are:
robust public education campaign of must reflect latest scientific evidence
(1) apply a multisector, multidisciplinary
recommendations. and include recommendations
approach (since a single effort in one
tailored to pregnant women, infants,
sector or discipline is unlikely to have l Dedicate a portion of the Surface
and toddlers.
a significant impact); and (2) focus on Transportation Block Grant program
those populations with a disproportionate to transportation alternatives like l E xtend benefits and scope of the
burden of obesity. A summary of pedestrian and bicycle facilities, Special Supplemental Nutrition
TFAH’s recommendations are below; recreational trails, and Safe Routes to Program for Women, Infants, and
the full recommendations begin on Schools (SRTS). Children (WIC) Program to children
page 61. Unless otherwise noted, all through the age of 6 and to
l Make SRTS, Vision Zero, Complete
recommendations are for the federal postpartum mothers through the first
Streets, and other safety projects
government. two years after the birth of a baby, and
eligible for the Highway Safety
fully fund the WIC Breastfeeding Peer
Strengthen Federal Best Practices to Improvement Program.
Counseling Program.
Build State and Local Capacity and
l Incorporate Complete Streets principles
Reduce Disparities l E xpand and improve the Child and Adult
as a condition for state receipt of
l Expand the Centers for Disease Control Care Food Program.
federal funding for major transportation
and Prevention’s (CDC) statewide obesity- projects in all federal infrastructure bills. l Align federal child nutrition policies
prevention program (State Physical and programs with the evidence-based
Activity and Nutrition (SPAN) program).
l State and local education agencies
Dietary Guidelines for Americans.
should prioritize physical activity in their
l Create best-practices guides for states educational plans, including using the l Implement the Nutrition Facts
to maximize effectiveness when they Every Student Succeeds Act Title I and/ regulations in 2020 as currently
implement SPAN. or IV funding. scheduled, and ensure funding for
l Increase funding for CDC’s Racial and Nutrition Innovation Strategy consumer-
l States and cities should enact Complete
Ethnic Approaches to Community Health awareness education campaigns for
Streets and other complementary
(REACH) program. Nutrition Facts and menu labeling.
streetscape design policies to improve
l Create a new CDC grant program active transportation and increase l States should strengthen school
that focuses on addressing social outdoor physical-activity opportunities. nutrition beyond the federal government
determinants of health across sectors. standards, including the length of meal
l States should expand the federal “Every
time, time of the meal, and recess
l Adapt federal grantmaking practices to Kid Outdoors” program to include state-
before lunch.
account for the differential needs and managed lands.
capacity of states and organizations for
l States and local education agencies
Prioritize Healthy Eating by Making
competitive grants. should offer nutritious school-meal
Changes Across the Food System
programs, expand flexible school
Make Physical Activity and the Built l Maintain the current eligibility levels and breakfast programs, participate in the
Environment Safer and More Accessible requirements, and value of benefits of Community Eligibility Provision, and
l Fully fund the Student Support and the Supplemental Nutrition Assistance use the CDC’s Whole School, Whole
Academic Enrichment program and Program (SNAP) and other important Community, Whole Child framework.
food-security programs.
8 TFAH • tfah.org
l States should adopt the Food Service WHAT IS OBESITY?
Guidelines for foods and beverages
procured for government food-service “Obesity” means that an individual’s body fat and body-fat distribution exceed the
facilities and vending machines at all level considered healthy.31,32 There are many methods of measuring body fat. Body-
state agencies. mass index (BMI) is an inexpensive method that is often used as an approximate
measure, although it has its limitations and is not accurate for all individuals (e.g.,
Change How the Nation Markets and muscular individuals often have lower body fat than their BMI would suggest).33 BMI
Prices Unhealthy Foods and Beverages is calculated by dividing a person’s weight (in kilograms) by his or her height (in
l Close federal tax loopholes and square meters). The BMI formula for measurements in pounds and inches is:
eliminate business-cost deductions
related to advertising of unhealthy
food and beverages to children
on television, internet, and places
BMI = ( Weight in pounds
(Height in inches) x (Height in inches) ) x 703
frequented by children.
l States should increase the price For adults, BMI is associated with the following weight classifications:
of sugary drinks, through an excise
BMI LEVELS FOR ADULTS AGES 20+
tax, with tax revenue allocated to BMI Level Weight Classification
local efforts to reduce health and Below 18.5 Underweight
socioeconomic disparities. 18.5 to < 25 Healthy weight
l States should enforce the USDA local 25 to < 30 Overweight
school wellness policies final rule, 30 and above Obesity
which limits marketing at schools 40 and above Severe Obesity
during the day to food that meet Smart
Snacks standards. Medical professionals measure childhood obesity differently. That’s because
body-fat levels change over the course of childhood and are different for boys
l Local education agencies should consider
and girls. Childhood weight classifications are determined by comparing a child’s
including strategies in their local wellness
height and weight with BMI-for-age growth charts developed by the Centers for
policies that reduce unhealthy food and
Disease Control and Prevention (CDC) using data collected from 1963 to 1965
beverage advertising to students, by
and from 1988 to 1994.34
prohibiting coupons, sales, and advertising
around schools and school buses. BMI LEVELS FOR CHILDREN AGES 2-19
BMI Level Weight Classification
Work with the Healthcare System to
Below 5th percentile Underweight
Close Gaps
5th to < 85th percentile Healthy weight
l Clarify for health insurers which U.S.
85th to < 95th percentile Overweight
Preventive Services Task Force obesity-
95th percentile and above Obesity
related screening and treatments they are
required to cover with no cost-sharing.
l Improve healthcare provider knowledge participation in obesity-prevention or
on obesity-related treatments, like control programming with a particular
intensive behavioral therapy, and relevant emphasis on communities that are
community programs and supports. disproportionally impacted by obesity.
l Public health departments should l Medicaid should reimburse providers
partner with and/or convene for evidence-based comprehensive
healthcare and community partners pediatric weight-management programs
to increase the availability of and and services.
TFAH • tfah.org 9
S EC T I ON 1 :
The State of
SECTION I: SPECIAL FEATURE: RACIAL AND ETHNIC DISPARITIES IN OBESITY
SPECIAL FEATURE: Racial and
Obesity Ethnic Disparities in Obesity
Obesity rates diverge along a number of demographic measures
(for example, sex, race or ethnicity, income, education,
geography, and urban or rural). Some of the starkest variations,
like many other health measures, occur across race and ethnicity.
While obesity rates depend on many factors—from individual-
level behaviors to economic and community effects to cultural
and marketing influences—there are persistent health inequities
in racial and ethnic groups with high obesity rates.
Broader equity issues—like poverty and inequities and underinvestments
institutional racism—and community that result in limited resources in
context shape daily life and available communities to encouraging culturally
choices around healthy food, physical appropriate, healthy choices at the
activity, education, jobs, financial individual level.
security, etc. (together often called
This section outlines obesity data by
“social determinants of health”), which
race and ethnicity, and shares policy
systematically affect people’s weight
considerations and approaches to this
and health.35 Real change in obesity
issue. It also includes interviews with
requires understanding and action
experts and highlights from current
on the various drivers of high obesity
initiatives and programs.
rates—from addressing historical
SEPTEMBER 2019HOW INEQUITY CONTRIBUTES TO OBESITY: From Living Context to Weight Outcomes
Developed from a presentation at the Roundtable on Obesity Solutions, National Academies of Sciences, Engineering, and Medicine36
Historical, social, economic, physical, and policy
contexts
Legal risks and protections Systematic effects on daily life and
Institutional racism and other forms discrimination choices
Political voice and voter registration Food-related: Weight control and related contextual
Economics: • Food access, affordability, appeal outcomes and effects on individuals
• Debt • Exposure to food advertising
• Poverty • Federal nutrition assistance Food intake
• Home ownership • Food and nutrition literacy Dietary quality
• Wealth-building/Inheritance • Food norms Child feeding and parenting
• Health insurance • Dieting
Physical activity
• Minimum wage Physical activity-related:
• Public assistance Sedentary behavior
• Options for safe, affordable recreation
• Housing costs • Personal transportation Excess weight gain
• Employment discrimination • Public transportation Ability to lose weight
• Marketing • Exposure to violence
Ability to maintain weight
• Cost of living • Activity norms
• Exercise Body composition and fitness
Employment and occupation:
• Education attainment Resource limitations:
• Employment discrimination • Discretionary time
• Health insurance/Amenities • Discretionary income
• Physical demand of job/Sitting vs. standing • Income stability
• Job flexibility • Housing stability
Education: • Healthcare access
• School district Chronic stress
• Neighborhood segregation
Sleep health
• Housing discrimination
• Public funding for schools Food security
• School quality
• Higher-education access
Neighborhood/Locality:
• Rurality
• Jurisdiction
• Public transportation
• Distance to healthcare
• Retail outlets
• Food access
• Racial segregation
• Poverty rates
• Wage deserts
• Job access
• Housing stock
• School quality
• After-school programs
• Walking and biking infrastructure
• Community centers
• Neighborhood safety
• Parks
•N eighborhood resources (e.g., higher-education institution)
• Policing and law enforcement
• Stigma and interpersonal racism
• Blight, community ecology
TFAH • tfah.org 11WHAT IS HEALTH EQUITY?
Health equity is a common term that various organizations have defined in different ways over the years. TFAH uses the Robert
Wood Johnson Foundation definition:
“Health equity means that everyone
has a fair and just opportunity to be
as healthy as possible. This requires
removing obstacles to health such
as poverty, discrimination, and their
consequences, including powerlessness
and lack of access to good jobs with
fair pay, quality education and housing,
safe environments, and health care. For
the purposes of measurement, health
equity means reducing and ultimately
eliminating disparities in health and
its determinants that adversely affect
excluded or marginalized groups.”37
THE RACIAL AND ETHNIC APPROACHES TO COMMUNITY HEALTH PROGRAM REACHES
20TH ANNIVERSARY
CDC’s Racial and Ethnic Approaches
to Community Health (REACH)
initiative is a national program
focused on reducing chronic disease
and obesity for racial and ethnic
groups with high disease burden.
REACH has supported locally based
and culturally tailored solutions in
more than 180 communities over the
last 20 years. These communities
have seen decreases in smoking, l Over 2.7 million people have better The current five-year REACH grants
reductions in obesity, increases in access to healthy food and beverages. cover 31 entities across 21 states. The
fruit and vegetable consumption, and Fiscal Year (FY) 2019 funding for the
l Approximately 1.3 million people
improvements in healthy behaviors. core REACH grants was $35 million.
have more opportunities to be
The CDC estimates that, since its Grantees include local public health
physically active.
inception in 1999, REACH has helped departments, local governments,
millions of Americans: l Over 750,000 people have better access universities, and nonprofits in urban,
to new community-clinical linkages.38 rural, and tribal communities.39
12 TFAH • tfah.orgOBESITY DATA BY RACE/ETHNICITY
This subsection summarizes the best Asians, Native Hawaiians, and Pacific
available data on obesity rates by race Islanders
and ethnicity. When available, Trust Asians, Native Hawaiians, and Pacific
for America’s Health uses the Centers Islanders have far lower rates of obesity
for Disease Control and Prevention’s than any other racial or ethnic group
(CDC) National Health and Nutrition (12.7 percent versus 39.6 percent overall
Examination Survey (NHANES), in 2015–2016 according to NHANES).
supplemented by other surveys and However, national studies often group
studies as needed.40 together Native Hawaiian, Pacific
American Indians and Islanders, Chinese, Indian, Vietnamese,
Alaska Natives Korean, Japanese, and other Asian
ethnicities, which conceals important
Due to relatively small population sizes,
differences among these smaller
many national surveys do not report
populations. For example, the 2014
data on health measures for American
Native Hawaiian and Pacific Islander
Indians and Alaska Natives (AI/AN).
National Health Interview Survey found
The surveys that do exist do not gather
that Native Hawaiian adults ages 18 and
or present findings by tribal nations.
older had obesity rates of 37.4 percent
What is available shows that the AI/
and Pacific Islander adults had obesity
AN population has some of the highest
rates of 44.5 percent; in comparison, all
rates of obesity of any race/ethnic
Asians had an obesity rate of 11 percent
population. The 2017 National Health
in the 2014 National Health Interview
Interview Survey finds 38.1 percent
Survey (and Whites had a 28.2 percent
of AI/AN adults had obesity, which is
obesity rate). Within Pacific Islander
roughly the same as Black adults in
populations there is even substantial
that survey and substantially higher
variation, most notably 60 percent of
than White adults.41 Another 2017 study
Samoan adults had obesity in 2014 versus
found that as of 2015 AI/AN children
38 percent Guamanian, Chamorro, and
ages 2 to 19 had an obesity rate of 29.7
other Pacific Islanders.44
percent, which was almost twice the
obesity rate as the overall population of There is also substantial evidence that
2- to 19-year-olds in the United States. Asians should have a lower BMI cutoffs
Young AI/AN children (ages 2 to 4) for overweight and obesity measures
enrolled in WIC also had the highest than other races and ethnicities,
obesity rates of any race or ethnicity because they have higher health risks at
(18.5 percent for AI/AN 2- to 4-year-olds a lower BMI.45 This includes a higher risk
versus 13.9 percent overall in 2016).42 for type 2 diabetes and other metabolic
diseases at a lower BMI. Medical
The positive news for the AI/AN
professionals typically consider diabetes
population is that the obesity rates
testing for patients who are overweight
among AI/AN children remained
or who have obesity (a BMI of 25 or
stable between 2006 and 2015, and
higher), which means many Asians are
the youngest children (ages 2 to 5)
not getting tested and diagnosed. An
showed a decrease in obesity rates
estimated half of Asians with diabetes
between 2010 and 2015 (from 23.2 to
have not been diagnosed, which is much
20.7 percent).43
higher than the overall population.46,47
TFAH • tfah.org 13Percent of Adults with Obesity by Race/Ethnicity and Sex, 2015–2016
60%
54.8%
50% 50.6%
43.1%
40% 41.1% 37.9% 38% 37.9%
36.9%
30%
20%
14.8%
10% 10.1%
0%
All All Asian Asian Black Black Latina Latino White White
Women Men Women Men Women Men Women Men Women Men
Source: NHANES
Blacks Latinos also have important
In 2015–2016, 46.8 percent of Black adults variations within the group. Like
and 22 percent of Black children ages 2 Blacks, Latina women have much
to 19 had obesity according to NHANES. higher rates of obesity—as of 2015–
In comparison, the obesity rate for 2016, half of Latina women (50.6
White adults was 37.9 percent and White percent) had obesity compared with
children ages 2 to 19 was 14.1 percent. 43.1 percent of Latino men. And,
while the data are a bit older, there’s
The high obesity rate among Black women evidence that there is also variation
drives these differences. According to among Latinos by ethnicity. Puerto
2015–2016 NHANES data, 54.8 percent Ricans and Mexicans (particularly
of Black women have obesity. That’s those born in the United States) have
the highest sex and race or ethnicity higher rates of obesity compared
combination included in NHANES—and with Cubans, Central Americans, and
44 percent higher than White women (38 South Americans.48
percent). In contrast, Black men have an
obesity rate of 36.9 percent, which is about Whites
the same as White men (37.9 percent).
Whites have substantially lower
obesity rates compared with other
Latinos
races and ethnicities, except Asians.
Latinos also have very high obesity Because Whites are the majority of
rates. NHANES found that 47 percent the U.S. population, the White obesity
Latino adults and 25.8 percent of Latino rates and trends drive the overall
children ages 2 to 19 had obesity in 2015– obesity rates and trends. Unlike other
2016. These are the highest combined races and ethnicities, there is no
adult and youth obesity rates among races difference in obesity rates between
and ethnicities included in NHANES. the sexes among Whites.
14 TFAH • tfah.orgSHIFTING TRENDS IN DIABETES AMONG AMERICAN INDIANS AND ALASKA NATIVES
In the 1990s, diabetes prevalence constant.52 Importantly, SDPI grants are team-based approaches to diabetes care
among AI/ANs was higher and community-directed, and grantees adapt led to a decrease of 54 percent in kidney
increasing faster than in the general evidence-based interventions to fit local failure rates among AI/AN diabetes
population—with the largest increases needs and culture. patients between 1996 and 2013.54
among American Indians under 35 The work of SDPI at stabilizing trends in
One specific program, the SDPI
years old, including an astounding 58 diabetes and childhood obesity among
Diabetes Prevention Initiative, studied
percent jump in diabetes rates among AI/AN people shows the importance
the impact of a proven lifestyle program
AI/AN adults ages 20 to 29 between of using tailored, culturally appropriate
for individuals with a high risk of
1990 and 1998.49,50 In response population-health and team-based
developing diabetes. After adapting the
to these alarming trends, Congress approaches for diverse communities.
program to AI/AN communities, SDPI
established the Special Diabetes
found that the intervention successfully Another program focused on the
Program for Indians (SDPI) in 1997.
reduced the number of new diabetes health of American Indians and
SDPI provides grants for diabetes
cases expected, increased healthy- Alaska Natives is the CDC’s Good
prevention and treatment programs in
eating and physical-activity levels, and Health and Wellness in Indian Country
AI/AN communities, including weight-
reduced participants’ BMI. 53
program. The 5-year, $13 million per
management and nutrition services,
year initiative enlists tribes and tribal
community- and school-based physical- SDPI has also tackled high rates of
organizations to be change agents
activity programs, diabetes education, diabetes complications within AI/AN
within their communities
and diabetes clinical teams. The current communities. New population-health and
2016–2020 SDPI grants allocate $150
million per year to 301 grantees across
35 states. Grantees include programs Rate of Kidney Failures (Per 100,000 Population) by Race/Ethnicity, 1996 and 2013
across 252 tribes, 29 urban Indian 60% 57.3%
health programs, and 20 Indian Health 52.2%
50%
Service entities.51
42.7%
40% 40.1%
SDPI significantly increases the 36.9%
34.2%
availability of prevention and treatment 30%
26.5%
programs in AI/AN communities—and 23.1% 22.2%
20%
can help improve the trajectory of 15.5%
diabetes and childhood obesity among 12.1%
10%
AI/AN people. Since 2006, diabetes
rates have stabilized among AI/AN adults 0% 1996 2013 1996 2013 1996 2013 1996 2013 1996 2013
American Indians/ Asians Blacks Latinos Whites
(although they are still higher than the Alaska Natives
overall population’s), and childhood Source: United States Renal Data System
obesity and diabetes rates also remained
TFAH • tfah.org 15POLICY CONSIDERATIONS AND APPROACHES
Despite current efforts, obesity rates a strategy that seeks to increase food
across the United States are too high, access through land-use planning and
particularly within certain populations. policies must work with and involve the
Additional focused research, more community by:
investment, and bolder policies
l artnering with credible
P
centered on groups with the highest
organizations with ties to residents
levels of obesity is a crucial step in
in order to cultivate meaningful
tackling the obesity crisis overall and
engagement;
in ensuring that all Americans have an
opportunity to lead his or her healthiest l ffering training to expand residents’
O
life. This subsection shares insights leadership skills and to deepen
from experts about understanding the understanding of the planning
underlying equity issues as well as ideas process; and
for making progress.
l stablishing processes to ensure
E
resident concerns are gathered and
CDC’s Recommendations on
echoed in the plans.55
Advancing Health Equity
In response to the needs of public Equity Approach to Obesity
health practitioners seeking effective, Framework
evidence-based tools to mitigate
The equity approach to obesity
inequities in chronic diseases, CDC
framework, developed by Dr.
developed A Practitioner’s Guide for
Shiriki Kumanyika for the National
Advancing Health Equity. The guide
Academies of Sciences, Engineering,
focuses on making the places where
and Medicine, suggests the need for
people live, learn, work, and play
interventions intentionally tailored
better support health through
to populations with high obesity rates
environmental, policy, and systems
(as opposed to the population at large
approaches, including:
or those with less of a need), in order
l esigning, implementing, and
D to effectively mitigate health-related
evaluating strategies with an inequities seen in obesity. Kumanyika
intentional focus on health equity; proposes a strategy that focuses on
both short-term and long-term efforts
l uilding a team that reflects a diverse
B
in altering social determinants of
set of partners; and
obesity. 56 The key to advancing equity
l mbedding health equity into local
E when it comes to obesity-causing
efforts by engaging the community, factors and related outcomes is using
building partnerships, establishing an operational approach comprising
organizational capacity, and four major solution categories: (1)
conducting evaluations. increase healthy options; (2) reduce
deterrents to healthy behaviors;
In their recommendations, CDC
(3) improve social and economic
suggests ways to achieve health equity
resources; and (4) build community
as well as detailed opportunities for
capacity. Integrating solutions across
which public health practitioners can
the four categories can lead to better
maximize the impacts. For instance,
and more equitable outcomes.
16 TFAH • tfah.orgThis equity-oriented method can be
used with a specific demographic group Proposed Equity-Oriented Obesity Prevention Action Framework to assist
or within a particular geographic in selecting or evaluating combinations of interventions that incorporate
region and translated into action by: (1) considerations related to social disadvantages and social determinants of health
convening groups of relevant experts
and stakeholders with knowledge Food retail and provision Promotion of unhealthy products
of approaches in each category Schools and worksites Higher costs of healthy foods
Built environment Threats to personal safety
or solution of this framework; (2) Parks and recreation Discrimination
engaging experts and stakeholders Transport Social exclusion
to create a coordinated strategy; and
INCREASE REDUCE
(3) identifying metrics for evaluating DETERRENTS
HEALTHY
success. It is of paramount importance OPTIONS TO HEALTHY
that public health practitioners, BEHAVIORS
experts, and stakeholders leverage
existing community assets when
IMPROVE BUILD
developing solutions, as opposed to SOCIAL AND COMMUNITY
identifying deficits alone. ECONOMIC CAPACITY
RESOURCES
Public Health Approach to Reducing
Inequity in Obesity: Examples from Anti-hunger programs Empowered communities
Economic Development Strategic partnerships
Native American Communities
Legal services Entrepeneurship
The National Academies of Sciences, Education and job training Behavior change knowledge and skills
Engineering, and Medicine created Housing subsidies; tax credits Promotion of healthy behaviors
the Roundtable on Obesity Solutions
Source: National Academies of Sciences, Engineering, and Medicine
in 2014 to engage leadership from
multiple sectors to solve the obesity
crisis. During a Roundtable workshop
experience, as they relate to obesity,
in April 2019, Dr. Valarie Blue Bird
Jernigan offers five key recommendations:
Jernigan, the director of the Center for
Indigenous Health Research and Policy 1. Use participatory approaches that
at Oklahoma State University, shared respect tribal sovereignty.
insights on the historical and current
2. Fund culturally centered, rigorous,
inequities, particular challenges, and
robust, and evaluative research.
policy recommendations for reducing
obesity among AI/AN populations. AI/ 3. Build research and implementation
AN populations experience high levels capacity among tribes and research
of obesity; significant social, economic, partnerships.
and environmental inequities; and a
4. Translate practitioners’ applied
lack of research on effective models,
knowledge and disseminate findings.
programs, and policies for indigenous
communities. Furthermore, current 5. Focus on AI/ANs residing in urban
national and state obesity-related areas as well as rural ones.
policies don’t necessarily affect those
While Jernigan tailored her insights
residing in tribal nations due to the
to Native American communities,
sovereign status of tribal nations.
her recommendations include
In order to address the persistent considerations for other populations
inequities Native communities with high obesity rates, too.57
TFAH • tfah.org 17MEET TWO HEALTH EQUITY LEADERS
This subsection features interviews with two community and policy leaders who share their perspective on the
role of health equity in obesity prevention.
Interview with Xavier Morales, PhD, MRP
Executive Director, The Praxis Project refers to the material outcomes that can be i.e. improving the robustness of the presence
The Praxis Project is a national non-profit measured by quantifying the determinants of the determinants—think food justice,
that works with national, regional, state and of health in a given geographic area—for housing, transportation—are similar, but
local partners to build healthy communities example, data on food security, access to the operationalization of the verb of health
quality housing, educational attainment, and equity—addressing structural inequities
and achieve health equity.
so forth. The verb of health equity refers to that lead to poor health outcomes such as
TFAH: Please briefly describe the work of contemporary and historical processes or obesity—is greatly impacted by worldviews,
The Praxis Project. structures that have caused or perpetuate priorities, funding, perfect-vs-good policy,
Morales: The Praxis Project’s overarching how robustly present—or absent— each how knowledge for action is produced and
goal is to center community power determinant is in a particular area. We firmly accepted, and political/economic/academic
to advance health justice and racial believe that inequity in processes leads to positioning within the vast ecosystem of
equity. We do this three ways: 1) helping inequity in social conditions and distribution public health.
our national network of basebuilding of the determinants of health.
In a nutshell, we see professional public
community partners—community-based To solve an issue like obesity, both the noun health making general progress towards
organizations that build local power by and the verb need to be addressed. If we health equity. However, these gains are
addressing local priorities - to improve don’t change the process and structures that not equally felt across all communities—
health justice and racial equity better, faster, lead to health inequity, our work towards especially those living in areas with the
more sustainably, and more profoundly; health equity will never be sustainably highest levels of disinvestment. It is these
2) creating space for these organizations effective. So, for me, as I look at the obesity areas where basebuilding organizers
within professional public health by crisis, which in my estimation, dwarfs almost typically work. In these community settings
promoting and coaching opportunities for every other contemporary health crisis on with folks that really understand the
authentic collaboration, and 3) producing every measure — in lives lost, costs to society, structures that lead to inequity, work can
evidence to show that public health’s efforts costs to productivity, costs to dignity— often get messy and complicated—truths
to improve health justice need to equally addressing the verb of health equity is are said, realities are dissected and exposed,
invest in basebuilding community groups central to stemming the crisis. contradictions and hypocrisies of systems
for their inherent value to the broader and the people who perpetuate these
fight for health. This work is nuanced and TFAH: The Praxis Project emphasizes
systems and structures are questioned and
complex due to power dynamics, scarcity of partnerships and community centered
called out. This environment is not always
resources, and most importantly, trust issues power in its work. Can you talk about the
pleasant. But we need to go through the
resulting from real and persistent trauma. importance of these factors?
messiness to build the trust that is needed
We address the obesity crisis by looking Morales: Praxis is fortunate to be in for professional and organic public health to
at the underlying systemic conditions in a place where we can participate in authentically come together to work towards
people’s lives and engage with the fiercest efforts to improve health justice both at a healthier and more just world. The work
basebuilding organizers and innovative the professional level—i.e. researchers, towards addressing the verb of health
traditional public health partners who share professional advocates, program developers/ equity will go much faster and further with
the goal of a world where health justice and implementers/evaluators, funders, and policy authentic partnerships between professional
racial equity are the norm. advocates— and at the organic level—i.e. and organic public health.
community basebuilding partners— to share
TFAH: What role does health equity play in TFAH: What have you learned from your
learning in ways that bridge, synthesize,
the obesity crisis?
connect and interpret between these levels work that policymakers need to better
Morales: First, a bit of framing to better of professional and organic public health. As understand?
understand where Praxis is coming from; we we travel between the professional and the Morales: Policy solutions need to fit the
reference grammar to illustrate our health organic, we find that the distance between problems and be practical. They need to be
equity work. The noun of health equity the larger goals of the noun of health equity, grounded in diverse perspectives, especially
18 TFAH • tfah.orgif the reason for policy action is the and the Berkeley good. In the end Measure outdoors won’t get you hurt or make you sick
inequitable conditions in communities that D, the name of the initiative, held forth a are also adding to the crisis.
are experiencing the most disinvestment. one cent tax per ounce of soda, it was an
We need to find the authentic partnerships
Policymakers and advocates need to excise tax (taxing the producers/distributors
that can address these overwhelming
recognize that there is “public health rather than the consumers), and it was a
structural contributors to the obesity
perfect” based on sound research. And there general tax—which meant that it’s revenue
crisis, and, we need to increase the
is “politically good” which is shaped by both would go into the general fund. But, we
bandwidth of the frontline leadership.
the research and the political complexities also provided for a commission made up of
Obesity, like climate change, epitomizes
required to advance policies in a manner Berkeley residents that would advise our City
the contradictions inherent when massive
that addresses the problem but may not fully Council on investments to help our children
profits, and the political power of those
maximize the research. I share an example consume less soda and drink more water.
who are profiting, are greater than the
that teases out this tension between the Without intending it, we created a strategy
influence of those who seek solutions that
“perfect” and the “good” concerning an that included as an outcome participatory
threaten those profits.
attempt to pass a local soda tax. If we think budgeting. The result: we received nearly
back less than five years ago, our field had 76% of the vote and created the first TFAH: In your opinion, what is the single
attempted and failed to pass a local soda municipal soda tax in the United States. This most important policy action that needs to
tax many times. The folks that were leading model helped advance some other municipal be taken to address obesity?
this work are incredible public health soda taxes that have passed since 2014.
Morales: In addition to the national public
activists that had the best of intentions. They
TFAH: As a nation, why haven’t we seen health campaigns the field engages in, there
followed the accepted research that said if
better results in efforts to address obesity? also needs to be significant investment into
you wanted to use a soda tax to curb the
building community capacity, knowledge,
consumption of sugary drinks 1) the tax had Morales: There are many reasons we
and resilience through investing in local
to be two cents per ounce to have any effect, haven’t seen better results in efforts to
organizations that are working hard to
2) that it needed to be a retail tax so that the reduce the number of people with obesity.
improve health. We need to be more
consumer could see and feel that they were The main reason is that the corporate profit
intentional to ensure that investments are
paying more, and 3) that the tax needed to opportunity in people contracting or having
changing the underlying structures that
be a specific tax—one that explicitly stated obesity is very high. Examples of the profit
promote health inequities and obesity.
where the revenues were going. This was the opportunity are numerous, starting with the
The way we are currently approaching
public health perfect, attempted many times agricultural subsidies designed when famine
the obesity epidemic — in silos and with
but never adopted. and hunger pervaded more areas of the
national campaigns/priorities that may not
U.S.; to the processed food companies that
In 2014 folks from Berkeley, CA decided to fit all local complexities, resources, and
are very good at engineering how much salt,
pursue a soda tax to help continue to fund priorities — is creating “solutions” that
fat, and sugar are needed so we “can’t have
our gardening and cooking classes in our often don’t address the structural causes of
just one”. Additionally, predatory marketing,
schools to improve nutrition education— obesity. As I work across professional and
placement, and pricing of unhealthy foods
another approach to reducing sugary drink organic public health, I feel we have reached
and beverages and the oversaturation and
consumption. A small group of advocates the limits of what professional public health
ubiquity of liquid sugar are adding to the
spoke with representatives from another alone can do going up against powerful
crisis. A whole industry has evolved to
California municipality who were still moneyed interests. We have to bring in the
make, distribute, and market unhealthy
stinging from their overwhelming defeat rest of the team (organic public health)
food. A dependency has been created
on a soda tax two years earlier. Berkeley’s in a manner that is authentic, dignified,
by different sporting/social/community
advocates asked, what would you do different equitably valued, and funded. The power of
activities and events that are funded by
if you could do this again? The answer was, those profiting from the obesity epidemic
donations from this industry. We have zones
involve diverse community input, especially is immense. Our public health solutions
of food apartheid where it is difficult to get
voices from those who we are claiming to need to be equally powerful. In Berkeley,
affordable fresh fruits and vegetables and
serve, as early in the process as possible. we were effectively outspent over 10:1 in the
clean water. Health promoting cultural
Taking this advice, our core group invited a most expensive campaign our little city ever
practices that are benign have been
few more residents who closely worked within experienced. The way we were able to beat
replaced by manufactured realities selling
the populations that suffer the most when the industry was through sustained people
us images of happiness frosted with sugar.
it comes to the overconsumption of sugar power deployed house to house, block by
The disinvestment in youth activities and
water. This new leadership configuration block, across our city. Led by neighbors who
city infrastructure that help to make sure
worked to overcome deep-seated bias about put our children’s health first.
communities are safe and that exercising
the space between the public health perfect
TFAH • tfah.org 19Interview with Devita Davison
Executive Director, Food LabDetroit out into the community, and hear what retails, like the entrepreneurs I worked
FoodLab Detroit is a non-profit member- is happening on the ground. with, access such funding. We’re not a big
based association of 200 good food regional grocery store—we’re bodegas
One thing that I’m excited about—
businesses. and green markets—but why shouldn’t
on [July 28, 2019], the United States
we get support like the big guys? Drawing
TFAH: Tell me about your work at Surgeon General, Dr. Jerome Adams,
the connection between how policy plays
FoodLabDetroit and what you’re trying was in Detroit speaking at the NAACP
a part in allocating funds and resources
to do in Detroit. Conference and he wanted to get
that eventually get to one’s community is
beyond the banquet halls and out into
Davison: FoodLab Detroit sits at the really important.
the community. So FoodLab Detroit,
intersection of economic development
along with member businesses and TFAH: Let’s talk food system and
and public health. We provide
partners, hosted Dr. Adams in their restaurant industry. What are some
incubation and acceleration for
neighborhoods. Those are the things key changes that the food system and
entrepreneurs to open healthy food
that we should be excited about—when restaurant industry overall can do to
businesses in the community. All our
our policy leaders have an opportunity to help reduce obesity?
efforts, our workshops, our trainings,
engage with people on the ground who Davison: What I want is for Detroit to
our classes, our technical assistance—all
are affected by policy. leverage our food. We have 1,600 urban
the work that we do and the services
that we provide—are for Detroiters who TFAH: What have you seen and learned farms in Detroit that are tapping into
have traditionally been underserved in your community and from your beautiful fruits and vegetables in our
and marginalized. Of FoodLab Detroit work that you wish policymakers better own backyard, that all Detroiters can
businesses, 78 percent are women-led, understood? take pride in. And we are creating a
52 percent by women of color, and 63 community—growers, restaurateurs, and
Davison: As an Executive Director
percent by African Americans. Which chefs—and using creative ways to create
of a non-profit organization, I’m
reflects the city of Detroit, where about a Detroit movement that takes advantage
constantly fundraising and looking for
83 percent of residents are African of what we’re growing. That’s not to say,
opportunities for funding. With that lens,
American and over 90 percent people we’re going to disconnect ourselves from
I think many people don’t realize how
of color. It’s really important for us that the globalized food system, but we need
federal policy [and resource allocation]
we create an equitable landscape as it to bring local food systems in, so we’re
impacts them, how important voting
relates to entrepreneurship and small all connected. It’s a rising tide lifts all
is because elected officials are passing
business development. boats model—because beautiful, healthy
legislation that can affect you, locally,
food should be available for all. How do
TFAH: What do you wish policymakers in your community. [For example], the
we democratize that and get some of the
were doing more of? federal government created the Health
best foods from Detroit into our poorer
Food Financing Initiative (HFFI) looking
Davison: I wish policymakers communities? It’s hard to ensure that all
at communities designated as food
understood how important it is to get folks have equitable access. We’re taking
deserts (defined as communities without
out into the community. I don’t know that on in Detroit.
a full-service grocery store within a one-
all the interworking’s of how legislation
mile distance) and created a fund to TFAH: Why hasn’t there been more
becomes law, what I do know is that
tackle that problem. These funds were success in reducing obesity rates over the
there is an awful lot of influence of
tapped by large grocery stores, which past decade?
money and big companies in our
go into underserved, marginalized Davison: Couple things. First, it’s great
politics. I wish policymakers had a
neighborhoods to build stores. HFFI to open a store in a community that
balanced perspective—that they listen
was an important initiative but if we has not had a full-service grocery store
to constituents in the neighborhoods
understood it more, it would help us in that neighborhood for years. But
and really talk to small business
fight for a policy that would also allow you cannot think that if you build it,
entrepreneurs, hold roundtables and
community-supported healthy food that they will come, and it solves the
discussions, making it a point to come
20 TFAH • tfah.orgYou can also read