Abdominal, Urologic, and Gynecologic Trauma - Joint Trauma System Emergency War Surgery Course - Joint Trauma ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Emergency War Surgery Course
Joint Trauma System
Abdominal, Urologic, and
Gynecologic Trauma
Joint Trauma System Battlefield Trauma Educational Program
1
EWS Abdominal, Urologic, Gynecologic Scenario 25 year old female was on patrol when struck by blast fragments across her left side from the axilla down to the knee and thrown to the ground. She is taken to the nearest surgical asset with multiple puncture wounds of unknown depth. She is diaphoretic. 1. What are your priorities in managing this patient? 2. What procedures do you expect to perform? 2020, v1.0 2

EWS Abdominal, Urologic, Gynecologic Objectives Indications for laparotomy on the battlefield Use of FAST exam in the evaluation of the combat casualty Management of injuries to major abdominal, genitourinary and gynecological organs 2020, v1.0 14 December 2011 Pre‐decisional FOUO 3

EWS Abdominal, Urologic, Gynecologic
Indications for Laparotomy
Penetrating injuries:
∎ Below the nipples
∎ Above the symphysis pubis
∎ Between the posterior axillary lines
∎ Clinical signs/symptoms of
intraperitoneal injury
Projectiles can take unexpected courses
to the abdomen even if entry outside
abdominal borders Source: Borden Institute: War Surgery
in Afghanistan and Iraq
2020, v1.0 4
EWS Abdominal, Urologic, Gynecologic Indications for Laparotomy Blunt abdominal injuries ∎ As a general rule, a patient with positive FAST or DPA/DPL should undergo exploration. DPA (+) > 10 ml blood. ∎ Patient in shock with negative or equivocal FAST, and no other identifiable source, should undergo laparotomy. 2020, v1.0 5

EWS Abdominal, Urologic, Gynecologic
FAST Examination
FAST: Focused Assessment Sonography for Trauma
Extension of physical examination
∎ Advantages
Noninvasive and repeatable
Identifies significant intraperitoneal & pericardial fluid
Most useful in blunt trauma
May be useful in identifying hemopneumothoraces
May help to decide which cavity to open first
∎ Disadvantages
Operator dependent with possible missed injuries
Unable to stage, characterize or identify specific injuries
2020, v1.0 6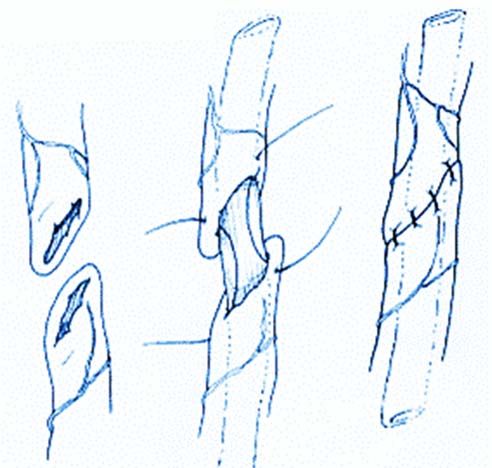
EWS Abdominal, Urologic, Gynecologic
FAST Examination
4 Basic Views
1.RUQ (Morrison’s pouch)
2.Cardiac
3.LUQ (spleen renal reflection)
4.Pelvic
Source: Emergency War Surgery, 5th U.S. Edition
2020, v1.0 7
EWS Abdominal, Urologic, Gynecologic
Right Upper Quadrant
A B
C
A. Right upper quadrant. B. Normal. C. Abnormal negative sonographic examinations.
Source: Emergency War Surgery, 5th U.S. Edition
2020, v1.0 8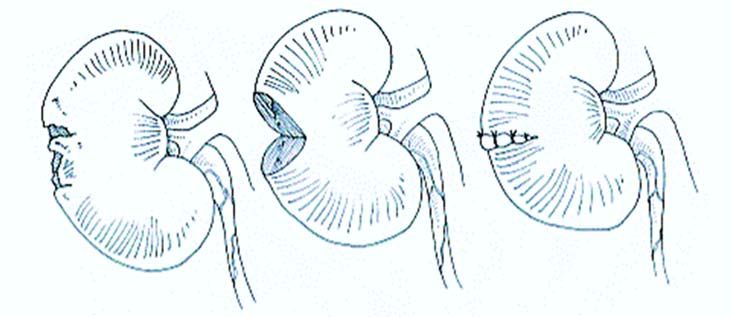
EWS Abdominal, Urologic, Gynecologic
Left Upper Quadrant
A B
C
A. Left upper quadrant. B. Normal. C. Abnormal negative sonographic examinations.
Source: Emergency War Surgery, 5th U.S. Edition
2020, v1.0 9
EWS Abdominal, Urologic, Gynecologic
Epigastrum
A B
C
A. Subxiphoid B. Normal C. Abnormal
Source: Emergency War Surgery, 5th U.S. Edition
2020, v1.0 10EWS Abdominal, Urologic, Gynecologic
Epigastrum
B
A
C
A. Suprapubic. B. Normal. C. Abnormal negative sonographic examinations for pelvic window.
Abd: abdomen; BL: bladder; FF: free fluid.
2020, v1.0 11EWS Abdominal, Urologic, Gynecologic
Diagnostic Peritoneal Aspiration
Diagnostic Peritoneal Aspiration (DPA) defines presence
and character of intraperitoneal fluid.
∎ Positive aspiration
10cc gross blood
Enteric contents
∎ Option if FAST unavailable or equivocal
Invasive, often not reproducible, slower then FAST
∎ Not recommended for penetrating abdominal injuries
2020, v1.0 12EWS Abdominal, Urologic, Gynecologic
Computed Tomography
∎ Computed Tomography (CT) will likely only be available
at Role 3 or higher.
∎ If patient is stable, CT may help exclude fragment penetration
of peritoneal cavity in stable, asymptomatic patients.
Triple contrast (oral, IV, and rectal) recommended.
No role for its use in unstable patients.
∎ May serve as adjunct to wound exploration to determine
trajectory of fragments.
2020, v1.0 13EWS Abdominal, Urologic, Gynecologic
Wound Exploration
∎ Blast injuries can create many
fragments that penetrate the skin and
not the abdominal cavity.
∎ Operative local wound exploration in a
stable patient with normal or equivocal
examination may help determine need
for formal exploratory laparotomy.
Should be performed in the OR.
If any doubt on fragment penetration,
perform exploratory laparotomy. Multiple penetrating injuries
to anterior chest and abdomen
2020, v1.0 14EWS Abdominal, Urologic, Gynecologic OR Planning (1) Operative Planning and Exposure Techniques ∎ Administer broad spectrum IV antibiotic prior to surgery and continue for 24 hours. ∎ Midline incision is ideal. ∎ Quickly pack all 4 quadrants with lap sponges while looking for obvious injuries. ∎ Control hemorrhage with packing/clamping of bleeding vessels and assess physiologic status. 2020, v1.0 15
EWS Abdominal, Urologic, Gynecologic
OR Planning (2)
Operative Planning and Exposure Techniques
∎ Consider casualty physiology, resources, locations, and form
operative plan to control hemorrhage and contamination.
Attempt to limit to < 60 min.
Always consider damage control principles.
In general definitive surgical procedures should be limited to when the
patient is stable and a level of care with the greatest diagnostic and
therapeutic resources.
∎ Massive swelling associated with large amounts of blood loss and
resuscitation can occur.
2020, v1.0 16EWS Abdominal, Urologic, Gynecologic
OR Planning (3)
Operative Planning & Exposure Techniques
∎ Avoid closing the fascia in the following
circumstances:
Further abdominal procedures anticipated
Enteric viscera in discontinuity
Damage control laparotomy
∎ The skin should not be closed.
Temporary abdominal closure
2020, v1.0 17EWS Abdominal, Urologic, Gynecologic
Gastric Injury
∎ Divide gastrocolic ligament to explore both anterior AND
posterior stomach.
Must visualize GE junction and Angle of His.
∎ Debride edges of traumatic gastrotomy and close
primarily in one or two layers with permanent sutures.
∎ Leave NG/OG tube in place.
Can consider using a large gastrostomy tube
(large foley/malecot) if needed.
2020, v1.0 18EWS Abdominal, Urologic, Gynecologic
Duodenal Injury (1)
∎ Bile staining or hematoma in A B
periduodenal tissues mandates full
exploration (Kocher maneuver).
∎ Obtain hemostasis.
∎ Control major contamination.
Duodenal exclusion, repairs around
drainage tubes or primary repairs
Wide drainage with multiple closed C
suction drains (anterior and posterior)
A: Pyloric exclusion. B: Duodenal injury
∎ Transfer to next level of care repair. C: Gastrojejeunostomy.
Source: Emergency War Surgery, 5th U.S. Edition
if/when available.
2020, v1.0 19EWS Abdominal, Urologic, Gynecologic
Duodenal Injury (2)
∎ Perform FULL Kocher to completely evaluate duodenum.
∎ Ascertain injury relationship to Ampulla and Bile/Pancreatic ducts.
Should be considered with any injury involving second portion of
duodenum or pancreatic head.
∎ Widely drain the site of all injuries with closed suction drains.
∎ Primary Repair:
< 50% circumference minimal tissue loss
Repair in two layers
Place multiple drains
2020, v1.0 20EWS Abdominal, Urologic, Gynecologic
Duodenal Injury (3)
∎ Extensive Injuries (≥ 50% Circumference):
Close duodenal wall around a tube duodenostomy.
Use 2‐0 absorbable suture (vicryl).
Use largest malecot catheter or drainage tube available.
∎ Must protect your duodenal repair.
Pyloric Exclusion (lasts only 14‐21 days):
Ligate pylorus with 0‐Prolene/PDS via transgastric approach
Fire noncutting (TA) stapler across pylorus (staple but not divide)
Create a gastrojejunostomy.
Place a feeding jejunostomy for nutrition.
∎ Pancreaticoduodenectomy is a procedure of LAST RESORT.
Do not reconstruct in the initial procedure.
2020, v1.0 21EWS Abdominal, Urologic, Gynecologic
Pancreatic Injury
∎ Wide drainage of all pancreatic injuries
∎ Pancreatic ductal assessment
Even if not identified, it should be presumed
Area should be drained with multiple closed‐suction drains
∎ Resect/staple clearly nonviable pancreatic body/tail tissue.
∎ As with duodenal injuries – pancreaticoduodenectomy
is a procedure of LAST RESORT.
Do not reconstruct at initial operation.
2020, v1.0 22EWS Abdominal, Urologic, Gynecologic Liver Injury (1) ∎ Most injuries can be successfully treated with direct pressure and/or packing followed by aggressive resuscitation. ∎ If packing not successful, surgical exposure should be done early and aggressively. ∎ Short duration clamping of hepatic artery and portal vein (Pringle Maneuver) can slow bleeding to allow for surgical control. 2020, v1.0 23
EWS Abdominal, Urologic, Gynecologic Liver Injury (2) If bleeding continues despite initial management/Pringle maneuver, especially from behind the liver, retrohepatic venous injury is indicated. ∎ High mortality rate, high resource utilization ∎ Best managed with aggressive packing to maintain tamponade and resuscitation. ∎ Consider total hepatic vascular isolation or atriocaval shunt. 2020, v1.0 24
EWS Abdominal, Urologic, Gynecologic
Liver Injury (3)
If needed for hemostasis, consider:
∎ Finger fracture of liver to identify and ligate individual bleeding
vessels and bile ducts.
∎ Overlapping mattress sutures of #0 chromic on a blunt liver needle
for raw surface bleeding.
∎ Consider hemostatic adjuncts.
∎ Last resort, cross clamping of aorta in left chest.
∎ For diffuse bleeding, can leave liver packed.
Some hemostatic adjuncts like Combat Gauze® can be used
to pack the abdomen.
Ensure any retained material can be identified radiographically.
Document that packing material was retained.
2020, v1.0 25EWS Abdominal, Urologic, Gynecologic
Liver Injury (4)
∎ Surgical resection strongly
discouraged.
Only indicated when
packing/pressure fails.
Follow functional or injury pattern.
∎ Provide generous suction around
major liver injuries.
∎ Omentum can be used to reduce Omental packing
dead space.
2020, v1.0 26EWS Abdominal, Urologic, Gynecologic
Biliary Tract Injury
∎ Gallbladder
Cholecystectomy
∎ Bile duct
Repair over T‐tube
Segmental loss requires either:
Choledochoenterostomy: Not a damage control procedure
Tube choledochostomy: Preferred in damage control setting
∎ Wide drainage
2020, v1.0 27EWS Abdominal, Urologic, Gynecologic
Splenic Injury
∎ The default option for the hemostatic control of splenic
hemorrhage is splenectomy.
Explore for associated diaphragm, stomach, pancreatic and renal
injuries.
Empiric left subphrenic drains should not be routinely placed if
pancreas uninvolved.
∎ If a victim of isolated blunt trauma presents at a Role 3 facility that
can ensure adequate clinical follow‐up and evaluation, non‐
operative management can be considered.
Transfer should not be done until all ongoing intraabdominal
hemorrhage is completely assessed and controlled.
2020, v1.0 28EWS Abdominal, Urologic, Gynecologic
Post Splenectomy Immunizations
∎ Immunizations: Done in theater
at the first facility that can do so
23‐Polyvalent Pneumococcal
Haemophilus Influenza
Meningococcal
∎ Important to document
No assumption of completion
at follow‐on facilities
Distal pancreatectomy and splenectomy.
Fragment is visible (arrow) within the
parenchyma of the pancreas.
Source: Borden Institute: War Surgery in Afghanistan and Iraq
2020, v1.0 29EWS Abdominal, Urologic, Gynecologic Small Bowel Injury ∎ Debride to freshly bleeding tissue. ∎ Close enterotomies in one or two layers. ∎ Consolidate and minimize anastomoses to avoid multiple resections. 2020, v1.0 30
EWS Abdominal, Urologic, Gynecologic
Colon Injury
∎ Primarily repair simple, isolated injuries.
Debride wound margins to normal, noncontused tissue.
Perform 2‐layer primary repair.
∎ For complex injuries, strongly consider damage control followed
by diversion, especially with:
Massive blood transfusion
Ongoing hypotension
Hypoxia
Reperfusion Injury
Multiple other injuries and/or pancreatic injury
High‐velocity injuries
Extensive local tissue damage
Distal colon
2020, v1.0 31EWS Abdominal, Urologic, Gynecologic
Colon Injury
∎ Damage control techniques include:
Ligation/stapling of bowel.
Resuscitation in the ICU.
∎ Continuity should be restored or
ostomy performed within 72 hours of
original damage control procedure.
Diverting colostomy.
Note skin is not closed.
2020, v1.0 32EWS Abdominal, Urologic, Gynecologic
Rectal Injury
∎ Question of injury suggested by proximity of other injury,
rectal exam or radiography mandates proctoscopy.
If the injury has not violated the peritoneum, do not explore
the extraperitoneal rectum at laparotomy to avoid
contamination of the abdominal cavity.
∎ Continuity should be restored or ostomy performed
within 72 hours of original damage control procedure.
2020, v1.0 33EWS Abdominal, Urologic, Gynecologic
Rectal Injury
∎ Treatment principles
Diversion (loop or end ostomy) is most important aspect.
Debridement and primary closure of small wounds
not needed if diverted.
Should granulate and heal on their own with time.
Gentle distal rectal washout to assess injury may be needed.
Too much pressure can create contamination of perirectal space.
∎ Prophylactic presacral drains are not advised.
May be required due to gross contamination or infection.
Avoid creating spaces to place drains.
2020, v1.0 34EWS Abdominal, Urologic, Gynecologic
Retroperitoneal Injury
∎ Evaluate all central and all Zone 1
penetrating retroperitoneal
hematomas.
∎ Zone 1: Explore for all injuries.
∎ Zone 2: Explore all penetrating Zone 2 Zone 2
injuries. Avoid exploring blunt Zone 3
injuries if possible.
∎ Zone 3: Explore all penetrating
injuries. Avoid exploring blunt
injuries if possible.
Source: Emergency War Surgery, 5th U.S. Edition
2020, v1.0 35EWS Abdominal, Urologic, Gynecologic Anal Injury ∎ Repaired by approximating cut ends of the anal sphincter with size 0 or 1 absorbable suture. ∎ Tag sphincter if unable to repair. ∎ Consider diversion of fecal stream. Source: Borden Institute: War Surgery in Afghanistan and Iraq 2020, v1.0 36
EWS Abdominal, Urologic, Gynecologic
Renal Injury (1)
∎ Patients with gross hematuria require
evaluation of the kidneys.
∎ Blunt injury: Nonoperative, unless
unstable
∎ Penetrating: Explore
∎ Total nephrectomy immediately
indicated in extensive renal injury if
patient’s life would be threatened by
attempted renal repair.
Renal injury post penetrating injury
2020, v1.0 37EWS Abdominal, Urologic, Gynecologic
Renal Injury (2)
∎ Most renal injuries, except for those at renal pedicle, are not
acutely life threatening.
Medial visceral rotation for life threating kidney injury
Kidney preservation should be considered, but nephrectomy may be
required for severely damaged kidney in an unstable patient.
∎ If repair planned, obtain renal control at the renal vascular pedicle.
Can be done prior to opening the perirenal fascia.
Local debridement of parenchyma
Watertight closure of collecting system with absorbable suture
If salvageable kidney, vascular repair is indicated.
2020, v1.0 38EWS Abdominal, Urologic, Gynecologic
Renal Injury (3)
∎ Reconstructed kidney should be covered by perirenal fat,
omentum or fibrin sealant.
∎ Closed‐suction drain should be left in place.
Steps in Renal Debridement Steps in Partial Nephrectomy
Source: Emergency War Surgery, 5th U.S. Edition
2020, v1.0 39EWS Abdominal, Urologic, Gynecologic
Ureteral Injury (1)
∎ Isolated ureteral injuries are highly unusual; they generally
occur in conjunction with other injuries such as:
Retroperitoneal hematoma
Injuries of the fixed portion of the colon, duodenum, and spleen
∎ Hematuria is frequently absent.
∎ Blast injuries can cause delayed presentation.
Reasonable to place stent when high‐velocity or blast occurs in
proximity to ureter
2020, v1.0 40EWS Abdominal, Urologic, Gynecologic
Ureteral Injury (2)
∎ Identify and localize with indigo
carmine/methylene blue.
∎ Best managed in combat setting by
temporary tube drainage with a small
feeding tube or ureteral stent followed
by delayed reconstruction.
∎ Basic principles of repair
Minimal debridement
1 cm spatulated, tension free anastomosis
Interrupted, absorbable 4/5‐0 suture
Internal stent (Double J)
External drainage Ureteroureterostomy
Source: Emergency War Surgery, 5th U.S. Edition
Isolate repairs with omentum or
posterior peritoneum
2020, v1.0 41EWS Abdominal, Urologic, Gynecologic
Ureteral Injury (3)
∎ Type of repair is dependent on:
Anatomic segment (upper, middle, lower)
Extent of segment loss
Other injuries and patient stability
∎ Upper or middle ureteral injuries
Short segment: Primary repair
Long segment may require temporalizing tube, cutaneous
ureterostomy with stent, or ureteral ligation with nephrostomy
∎ Lower ureteral Injuries
Ureteroneocystostomy
When associated with rectal injury, perform temporary diversion
– not repair.
2020, v1.0 42EWS Abdominal, Urologic, Gynecologic
Ureteral Injury (4)
∎ Lengthening procedures that can provide tension free repair:
Ureteral mobilization
Kidney mobilization
Psoas hitch
Baori flap
Psoas hitch Ureteroneocystostomy
Emergency War Surgery, 5th U.S. Edition
2020, v1.0 43EWS Abdominal, Urologic, Gynecologic
Bladder Injury
∎ Consider bladder injury in patients with:
Lower abdominal penetrating wounds.
Pelvic fractures with gross hematuria.
Those unable to void post trauma.
∎ Bladder disruption occurring on the intraperitoneal or
extraperitoneal are treated differently.
∎ After ensuring urethral integrity, evaluation of the
bladder with cystography may be appropriate.
2020, v1.0 44EWS Abdominal, Urologic, Gynecologic
Bladder Injury
∎ Intra‐peritoneal injury
Surgical exploration
Multilayer repair with absorbable closure
Foley (preferred) or suprapubic cystostomy (alternative)
Drainage of perivesical space
∎ Extra‐peritoneal injury
Foley drainage of bladder for 10‐14 days
Repair as intra‐peritoneal injury if encountered and peritoneum
opened next to bladder injury.
2020, v1.0 45EWS Abdominal, Urologic, Gynecologic
Urethral Injury
∎ Urethral injury is suspected in
patients with scrotal hematoma,
blood at the meatus, or high riding
prostate.
Catheterization contra‐indicated
until integrity confirmed by
retrograde urethrography.
∎ If any difficulty passing catheter,
the urethra should not be
instrumented and a suprapubic tube Complicated penile and scrotal injury
cystostomy should be performed.
2020, v1.0 46EWS Abdominal, Urologic, Gynecologic
External Genitalia (1)
∎ Management: be conservative as possible.
Hemorrhage control
Debridement
Repair early to prevent deformity.
∎ Injuries to penis that disrupt buck’s fascia
should be sutured to prevent bleeding
and avoid curvature with erection.
Avoid aggressive over sewing of corpus
spongiosum to avoid distal ischemia.
∎ If extensive skin loss:
Cover with remaining skin.
Moist dressing. Complex perineal wound
involving genitalia
2020, v1.0 47EWS Abdominal, Urologic, Gynecologic
External Genitalia (2)
∎ Extensive debridement is usually
unnecessary.
∎ Scrotum
Any penetrating injury must be explored.
Primarily close scrotal lacerations with
3‐0 absorbable suture, 2‐layers if
wound is less than 8 hours old and
no life threatening injuries.
Leave penrose or drain to reduce
hematoma formation if closing.
Post scrotal exploration
2020, v1.0 48EWS Abdominal, Urologic, Gynecologic
External Genitalia (3)
Testicle
∎ Goal: To conserve as much tissue as possible.
Debride herniated parenchymal tissue.
Close tunica albuginea with absorbable mattress sutures.
Testicle is placed in the scrotum or wrapped in moist gauze.
∎ Never resect the testicle unless hopelessly damaged
or devascularized.
2020, v1.0 49EWS Abdominal, Urologic, Gynecologic
External Genitalia (4)
Vulvar lacerations
∎ For lacerations that are superficial, clean, and less than 6
hours old, perform primary repair with absorbable suture.
∎ Deep lacerations
Debride.
Evaluate for urethral, anal, rectal, or periclitoral injuries.
Closure of ureteral injuries, periclitoral, and rectal injuries should
be closed with 4‐0 or smaller absorbable suture.
Close ureteral injuries over a Foley catheter and leave in place.
2020, v1.0 50EWS Abdominal, Urologic, Gynecologic
External Genitalia (5)
Vulvar hematoma
∎ Most can be treated non‐operatively (compression).
∎ May require foley catheter for ureteral obstruction.
∎ May require incision and ligation of bleeding vessels.
Extraperitoneal expansion with signs of shock.
Large hematomas may cause skin necrosis.
Vagina
∎ Thorough inspection required.
∎ Concomitant urological trauma in 30% with vaginal trauma.
∎ Lacerations can be closed with 4‐0 absorbable suture.
Clinically significant vaginal hematomas should be treated with incision,
evacuation, ligation, and packing.
2020, v1.0 51EWS Abdominal, Urologic, Gynecologic Gynecological Trauma Uterine injury ∎ Repair simple cervical/uterine lacerations with #0 absorbable suture. ∎ Hemorrhage not responding to ligation/extensive cervical damage requires hysterectomy Fallopian Tubes ∎ Simple laceration equivalent to a salpingotomy should be allowed to heal by secondary intention. ∎ Significantly damaged tube should be treated with salpingectomy. 2020, v1.0 52
EWS Abdominal, Urologic, Gynecologic
Gynecological Trauma
Basic anatomy and locations for ligation of structures
Refer to pages 292‐3
of Emergency War
Surgery, 5th U.S.
Edition, for the Steps
to Perform an Emergent
Total Abdominal
Hysterectomy.
2020, v1.0 53EWS Abdominal, Urologic, Gynecologic
Gynecological Emergencies (1)
Fallopian Tubes
∎ Ruptured ectopic pregnancy
Wedge resection of the uterine body with salpingectomy
∎ Unruptured ectopic pregnancy
Linear salpingotomy with extraction of ectopic gestation
Leave open to heal by secondary intention.
∎ Spontaneous abortion into abdominal cavity should
simple be evacuated and tube left in situ if no hemorrhage
2020, v1.0 54EWS Abdominal, Urologic, Gynecologic Gynecological Emergencies (2) Ruptured ovarian cyst ∎ Cystectomy Shell out cyst wall Cauterize bleeding vessels at base of cyst Ovarian Torsion ∎ Untorse and evaluate Healthy and no abnormality – leave in situ Large Cyst (>4 cm cyst) – cystectomy Dark and Dusky – Salpingo‐oophorectomy 2020, v1.0 55
EWS Abdominal, Urologic, Gynecologic Gynecological Emergencies (3) Acute vaginal hemorrhage unrelated to trauma ∎ Pregnant patient < 20 weeks (fundus below umbilicus) Spontaneous abortion Dilation and curettage Acute abdomen – may be ectopic ∎ Pregnant patient third trimester (>4 cm above umbilicus) Placental abruption or previa If hemorrhage does not stop within minutes, emergent cesarean section Hemorrhage does not stop, may require hysterectomy ∎ Hemorrhaging mass is likely cervical cancer Pack to tamponade with urethral catheter Suturing is futile 2020, v1.0 56
EWS Abdominal, Urologic, Gynecologic
Gynecological Trauma
a. Uterine incision c. Delivered infant on abdomen
b. Delivery of fetus d. Uterine fundus exteriorized
2020, v1.0 57EWS Abdominal, Urologic, Gynecologic Exercise 25 year old female was on patrol when struck by blast fragments across her left side from the axilla down to the knee and thrown to the ground. She is taken to the nearest surgical asset with multiple puncture wounds of unknown depth. She is diaphoretic. 1. What are your priorities in managing this patient? 2. What procedures do you expect to perform? 2020, v1.0 58
EWS Abdominal, Urologic, Gynecologic
References
∎ JTS CPGs https://jts.amedd.army.mil/index.cfm/PI_CPGs/cpgs
Urologic Trauma Management, 01 Nov 2017.
Emergency General Surgery, 01 Aug 2018.
Blunt Abdominal Trauma, Splenectomy, and Post‐Splenectomy
Vaccination, 12 Aug 2016.
Nutritional Support Using Enteral and Parenteral Methods, 04 Aug
2016.
∎ Emergency War Surgery 5th Edition, 2018. Chap 17, 18, 19. Borden
Institute.
* All photos and images are courtesy of the JTS Collection unless otherwise cited.
2020, v1.0 59You can also read