Access to End of Life medicines in primary care during COVID-19 Pandemic - Access to EOL medicines in primary care during COVID-19 Pandemic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Access to EOL medicines in primary care during COVID-19 Pandemic
Access to
End of Life medicines
in primary care
during COVID-19 Pandemic
1|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021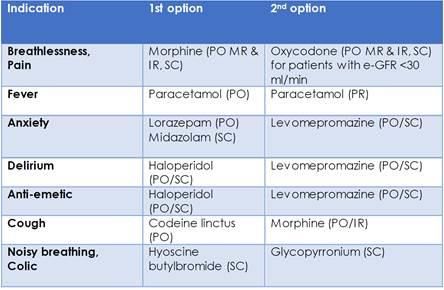
Access to EOL medicines in primary care during COVID-19 Pandemic
Contents
1. Background ...................................................................................................................................................3
2. When community pharmacies are open- ................................................................................................4
3. Urgent Care Provider-IC24 ........................................................................................................................6
4. When community pharmacies are closed ...............................................................................................7
5. Contingency Plan for severe shortage of End of Life Medicines .........................................................8
6. Transport Arrangements ...........................................................................................................................8
Appendix 1-Community Palliative Care Pharmacies ...........................................................................................10
Appendix 2 NHS.Net Email Addresses Palliative Care Pharmacies .....................................................................11
Appendix 3 RPS guidance on ethical, professional decision making in the COVID-19 Pandemic ......................12
Appendix 3 contd: Pertinent extracts from RPS guidance on ethical, professional decision making
in the COVID-19 Pandemic – ............................................................................................................................13
Appendix 3 Priority medicines for palliative and end of life care during a pandemic ........................15
Appendix 4 Red Cross Medication Transport Documentation ............................................................................16
*June 2020-Correction of Well Pharmacy contact details.
2|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021
Access to EOL medicines in primary care during COVID-19 Pandemic
1. Background
Access to palliative care medication has been identified by professionals as one of the biggest concerns
when caring for terminally ill patients and consequently compromises the delivery of good End of Life
(EoL) care. When a patient is to receive EoL care in the community, it is important that the appropriate
medicines to support that patient’s symptom control are readily available, both in and out of normal
hours.
Poor communication, planning, pain management and co-ordination lead to tragic and avoidable
suffering. Current best practice within palliative care promotes proactive anticipatory prescribing to
enable prompt symptom relief at whatever time the patient develops distressing symptoms. However,
due to the unprecedented impact of COVID-19 there are increasing concerns about medicine
availability during the global pandemic. The emerging evidence is that the deterioration is often quick
and difficult to anticipate.
A change in prescribing approach is needed from traditional ‘Just in Case’ prescribing to ‘Just in Time’
prescribing, i.e. medicines must be supplied rapidly on demand rather than in advance to ensure
availability when needed and equitable access to all. Traditional ‘Just in Case’ prescribing for each
patient is likely to exhaust the national supply of End of Life (EoL) medicines resulting in stock
potentially sitting in the wrong places, unable to be moved around quickly and thus leading to
increased waiting times for medicines.
The existing supply of EoL medicines in the community is through community pharmacies and
dispensing GP practices or GP Out of Hours / Urgent Care Centres. The potential demand due to COVID-
19 could constrict the total supply of EoL medicines and result in increased prescription turn-around
time and/or critical shortages.
A rapid approach to prescribing, dispensing and delivery of EoL medicines is being established covering
mid and south Essex STP.
Aims of this document are:
• To ensure we have clarity and consistency in these arrangements for stakeholders in different
organisations.
• To support implementation of ‘pragmatic’ local agreements for aspects of the supply process
which in extremis fall outside the current Human Medicines Regulations (HMR) or Controlled
Drugs regulations.
3|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
2. When community pharmacies are open-
o NOTE: There is at least one community pharmacy open somewhere in mid and south Essex
between the hours of 7am (Sun 8am) until 11pm.-Bank Holiday opening times may vary.
• EoL drugs will be supplied against prescriptions written by independent prescribers- medical
and non-medical and dispensed by either
o the patient’s usual community pharmacy
or
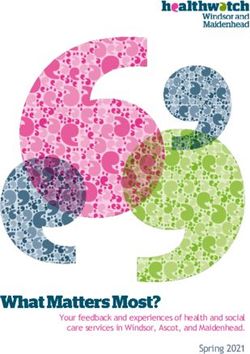
o designated palliative care community pharmacies commissioned by mid and south
Essex CCGs. Contact details of designated pharmacies, opening hours and drugs held
has been directly emailed to organisations and clinicians to hold and should be placed
in files easily accessible e.g. intranets. See Appendix 1
o Patients living on the border of MSE STP may find attending a designated palliative care
community pharmacy in a neighbouring STP more convenient. To find your nearest
open palliative care pharmacy, including neighbouring areas, please go to
https://pcm.prescqipp.info/ and enter your postcode
• All providers should ensure that prescribers have access to FP10s. This includes any NMPs as
well as medical prescribers. Hospices and community providers should ensure that
arrangements are in place for collaborative working to support access to prescribers and
remote prescribing.
• Telephone to check stock availability and agree delivery time--It is recommended in time
critical situations that the prescribing clinician contact the chosen community pharmacy to
check availability of drugs and agree a time frame for supply which meets the patient’s needs.
In very urgent situations pharmacists should make every attempt to get the drugs to the patient
within 2 hours of being notified.
• One drug item per form- it is recommended that each drug item is prescribed on a separate
FP10 prescription form. This is particularly pertinent in time critical situations. Prescribing one
drug item per form allows the patient/pharmacist to transfer any unsupplied items to another
pharmacy without the need to request a further prescription.
• Quantity prescribed- should be the minimum necessary to meet the needs of the patient e.g.
48 hours. Prescribers are reminded that it is not necessary to always prescribe in whole
‘original’ packs. Prescribing smaller quantities more frequently reduces supply chain issues and
wastage whilst continuing to meet patient needs.
• Directions for administration- it is the responsibility of the prescriber to ensure the EoL
medicines are written on a suitable drug administration chart (MAR chart) if community nursing
teams are required to administer. The MAR chart must include prescribed doses, indications,
directions, and be signed and dated by a prescriber. Where in place electronic directions to
administer should be provided (e.g. S1/Ardens). If a MAR chart is/will not available, the
prescriber must include full instructions for administration on the FP10 prescription form, and
the pharmacist must ensure full directions are included on the dispensing label, supported by
4|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
additional written information where necessary. This element could be met by providing, with
the medicines, a copy of the signed/authorised FP10 prescription detailing administration
instructions.
• Prescriptions should be sent electronically via EPS. The prescription can be sent to a
nominated pharmacy or sent to the spine without a nominated pharmacy. In both cases it is
recommended that an image of the bar number be emailed to the patient/family/clinician to
support the pharmacist quickly find the prescription on the spine. (see ‘how to guide’
https://midessexccg.nhs.uk/medicines-optimisation/covid-19-resources/dispensing-and-prescription-
processes/3749-sending-an-eps-prescription-without-a-nomination-for-acute-scripts/file
• Where prescriptions cannot be sent electronically, an image of the fully completed and signed
paper prescription will be emailed securely to the community pharmacy. Ask the pharmacy for
details of their nhs.net email account. Note that handwritten prescriptions must meet legal
requirements, and in particular for any controlled drugs prescribed. See ‘how to
guide’https://midessexccg.nhs.uk/medicines-optimisation/covid-19-resources/dispensing-
and-prescription-processes/3752-remote-prescribing-without-eps-guidance/file). Medicines
can then be supplied under Emergency Supply Regulations-although recognising that CDs Sch 2
and Sch 3 are not covered by these- with the original prescription supplied to the pharmacist
within 72 hours. https://bnf.nice.org.uk/guidance/emergency-supply-of-medicines.html
• The prescriber will post/transport securely the original ‘wet’ signed prescription to the
supplying pharmacy to arrive within 72 hours, unless arrangements can be made to hand over
the original script at the time of supply. Annotate FP10 ‘confirmation original prescription’
across body of script before posting so cannot be dispensed if lost in transit.
• For Controlled Drugs Sch 2 and 3, the original ‘wet signed’ prescription should be handed over
at the time of the supply of controlled drugs Sch 2 and Sch 3. Where the original prescription
cannot be made available at the time of supply, the pharmacist should have due regard and
consider taking action under their own professional judgement on to advice provided by the
regulatory and professional bodies and act in the best interests of the patient. Pharmacists and
pharmacy technicians should be reassured that should decisions be called into question at a
later date, they will be judged according to the circumstances at the time of the decision, not
with the benefit of hindsight. (see Appendix 3). The original ‘wet-signed’ prescription must be
with the supplying pharmacist within 72 hours. This emulates requirements under Emergency
Supply Regulations-although recognising that CDs Sch 2 and Sch 3 are not covered by these.
• Community pharmacists who are unable to ‘fill’ a prescription due to stock issues are
responsible for supporting carers/HCPs find a pharmacy who can supply the requested
medicines, releasing EPS prescriptions back to the spine where necessary and/or signposting to
an appropriate palliative care/community pharmacy. Use of EPS and delivery of dispensed
medicines directly to the patient, co-ordinated by pharmacy staff, should be used when
appropriate to avoid need for carer/HCP to travel between pharmacies. This approach is
facilitated by individual FP10 scripts being written for each item/drug.
• Delivery-medicines should be delivered to the patient as quickly as possible and within the
agreed timeframe. In very urgent situations pharmacists should make every attempt to get the
drugs to the patient within 2 hours of being notified.
5|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Where possible family/friends should collect the dispensed medicines. Where this is not
possible the community pharmacist is responsible for arranging delivery. Where costs incurred
by the pharmacist are not reclaimable within the national community pharmacy framework,
costs will be reimbursed by the patient’s CCG. Consideration will be given to establishing formal
transport contract to support urgent supplies of EoL drugs.
• Security-deliveries the pharmacist shall make arrangements for the medicines to be
transported safely with appropriate record keeping. RPS and GPhC have issued guidance which
clarifies that pharmacists cannot be held responsible for the actions/omissions of others if they
have complied with professional standards and acted in good faith.
3. Urgent Care Provider-IC24
IC24 GPs attending a patient carry a range of end of life medication, including controlled drugs,
for immediate use but will not leave a supply for later use.
IC24 Prescribers issuing an FP10 prescription for end of life medication should follow the
processes as detailed according to whether or not there is a community pharmacy open.
Prescribers are reminded to:
• Telephone to check stock availability and agree delivery time--It is recommended in time
critical situations that the prescribing clinician contact the pharmacist to check availability of
drugs and agree a time frame for supply which meets the patient’s needs. In very urgent
situations pharmacists should make every attempt to get the drugs to the patient within 2
hours of being notified.
• One drug item per form- it is recommended that each drug item is prescribed on a separate
FP10 prescription form. This is particularly pertinent in time critical situations. Prescribing
one drug item per form allows the patient/pharmacist to transfer any unsupplied items to
another pharmacy without the need to request a further prescription.
• Quantity prescribed- should be the minimum necessary to meet the needs of the patient e.g.
48 hours. Prescribers are reminded that it is not necessary to always prescribe in whole
‘original’ packs. Prescribing smaller quantities more frequently reduces supply chain issues
and wastage whilst continuing to meet patient needs.
• Directions for administration- it is the responsibility of the prescriber to ensure the EoL
medicines are written on a suitable drug administration chart (MAR chart) if community
nursing teams are required to administer. The MAR chart must include prescribed doses,
indications, directions, and be signed and dated by a prescriber. Where in place electronic
directions to administer should be provided (e.g. S1/Ardens). If a MAR chart is/will not
available, the prescriber must include full instructions for administration on the FP10
prescription form, and the pharmacist must ensure full directions are included on the
dispensing label, supported by additional written information where necessary. This element
could be met by providing, with the medicines, a copy of the signed/authorised FP10
prescription detailing administration instructions.
6|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
• Prescriptions should be sent electronically via EPS to community pharmacy. The prescription
can be sent to a nominated pharmacy or sent to the spine without a nominated pharmacy. In
both cases it is recommended that an image of the bar number be emailed to the
patient/family/pharmacist to support finding the prescription on the spine. (see ‘how to guide’
https://midessexccg.nhs.uk/medicines-optimisation/covid-19-resources/dispensing-and-prescription-
processes/3749-sending-an-eps-prescription-without-a-nomination-for-acute-scripts/file
• For urgent supplies, when prescriptions cannot be sent electronically e.g. following home visit
or to on-call hospital pharmacist, an image of the fully completed and signed paper
prescription should be emailed securely to the pharmacist. Note that handwritten
prescriptions must meet legal requirements, and in particular for any controlled drugs
prescribed. See ‘how to guide’https://midessexccg.nhs.uk/medicines-optimisation/covid-19-
resources/dispensing-and-prescription-processes/3752-remote-prescribing-without-eps-
guidance/file)
• The prescriber will post/transport securely the original ‘wet’ signed prescription to the
supplying pharmacy to arrive within 72 hours. Annotate FP10 ‘confirmation original
prescription’ across body of script before posting so cannot be dispensed if lost in transit.
4. When community pharmacies are closed
o NOTE: There is at least one community pharmacy open somewhere in mid and south Essex
between the hours of 7am (Sun 8am) until 11pm.-Bank Holiday opening times may vary.
When EoL drugs are required and need to be administered before they can be obtained from
a community pharmacy when next open, as a last resort the prescriber shall contact the
hospital on-call pharmacist at their local Trust via the hospital switchboard.
Basildon Hospital Telephone: 01268 524900
Broomfield Hospital Telephone: 01245 362000
Southend Hospital Telephone: 01702 435555
• Advice regarding checking stocks with pharmacist before prescribing, agreeing delivery time
and minimising quantities prescribed as detailed previously should be followed.
• The on-call pharmacist will agree with the prescriber the time frame for supply and where the
EoL drugs have to be sent.
• The prescriber will follow process for emailing securely an image of the completed ‘paper’
prescription to the on-call pharmacist. Note that handwritten prescriptions must meet legal
requirements, and in particular for any controlled drugs prescribed. See ‘how to
guide’https://midessexccg.nhs.uk/medicines-optimisation/covid-19-resources/dispensing-
and-prescription-processes/3752-remote-prescribing-without-eps-guidance/file) Medicines
can then be supplied under Emergency Supply Regulations-although recognising that CDs Sch 2
7|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
and Sch 3 are not covered by these- with the original prescription supplied to the pharmacist
within 72 hours. https://bnf.nice.org.uk/guidance/emergency-supply-of-medicines.html
• The pharmacist will dispense the prescription and send the dispensed items by transport to the
agreed destination.
• The prescriber will post/transport securely the original ‘wet’ signed prescription to the
supplying hospital pharmacy to arrive within 72 hours. Annotate FP10 ‘confirmation original
prescription’ across body of script before posting so cannot be dispensed if lost in transit.
5. Contingency Plan for severe shortage of End of Life Medicines
• If stocks of end of life medicines become extremely limited it may be necessary to restrict
stock holding to the CCG commissioned palliative care community pharmacies and hospital
pharmacies.
• In such circumstances, local community pharmacists will support access to end of life
medicines by transfer of prescriptions using EPS spine/image sent via nhs email, with remote
dispensing and return to patient’s usual pharmacy or deliver to patient’s home to minimise
travel requirement.
• Where costs incurred by the pharmacist are not reclaimable within the national community
pharmacy framework, costs will be reimbursed by the patient’s CCG.
6. Transport Arrangements
Medicines should be delivered to the patient as quickly as possible and within the timeframe
agreed with the requesting clinician. In very urgent situations pharmacists should make every
attempt to get the drugs to the patient within 2 hours of being notified.
Delivering controlled drugs (CDs)
• For delivering CDs, especially Schedule 2 CDs, the delivery driver should note the name of the
individual who collects the medicine from the doorstep and record it in their delivery record.
Agreed that this can be done instead of collecting the patient/carer signature for delivering
Schedule 2 CDs
• A further safeguard could include the pharmacist contacting the patient/family/HCP before
and after the delivery to ensure that the patient/family/HCP is aware of the impending
delivery of their CD medication, as well as to confirm afterwards that the patient has received
the CD items
• If a prescription is to be left with the family/HCP, the driver should be advised to collect this
and return it to the pharmacy. Prescription should be placed on the step and driver
collected once family/HCP return indoors.
Community pharmacies should use the patient’s own network or the pharmacy’s usual delivery
systems in the first place. Where collection by family/friends/HCP is not possible the community
pharmacist is responsible for arranging delivery.
8|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Where costs incurred by the pharmacist are not reclaimable within the national community
pharmacy framework, costs will be reimbursed by the patient’s CCG at the same rate as the
nationally commissioned service for each shielded patient.
Where the pharmacist is not able to arrange delivery as above they can contact the Red Cross to
request delivery for End of Life medication. Medicines will be delivered within 2 hours of the
request. Due to travel times please assess delivery arrangements quickly and put in a request in
good time.
Contact: Tel: 0300 023 0700 (24/7)
Email: ersecovid@redcross.org.uk monitored during the day 7 days a week.
Red Cross volunteers have all been DBS checked, carry ID and follow an agreed process for
delivery of medication agreed by the Pharmacist Adviser Essex County Council. Full details are
provided here (https://midessexccg.nhs.uk/medicines-optimisation/covid-19-
resources/dispensing-and-prescription-processes) but summarised below:
• When making deliveries, medicines in their package may be left on the patient’s doorstep,
and the delivery driver can wait at a distance (>2m) until it has been collected from the
doorstep by the patient/carer, and make a note in the delivery record to confirm that it has
been delivered. The name of the person receiving the medicine (patient / carer / family
member) will be recorded.
• When the door is answered, explain a prescription is being delivered and ask the person to
confirm the name and address of the patient, to ensure correct address and that the patient
lives there
• The person answering the door must be asked to state the name and address of the person
expecting a delivery of medicines – driver must not state this to them.
• If a patient does not answer the door, ring the pharmacy for advice; do not leave the
medicines outside the house or post the medicines through the letter box.
• Some patients may have more than one package of medicines, check with the pharmacy the
number of packages for each patient on collection and ensure that all bags of medicines are
delivered.
• Sometimes the pharmacy may not have all the medicines needed or the full quantity ordered
on the prescription. When this happens, the pharmacy will issue an Owings Slip. It is
important that you pass this Owings Slip onto the patient and advise them that these items
will be delivered when the pharmacy has the items back in stock.
• Some patients’ medication packages may be accompanied by a message for the patient to
contact the pharmacy for specific advice; please ensure this information is passed on to the
patient.
• If the patient has questions regarding the medicines themselves, please advise them to
contact the pharmacy.
• If the patient wishes to return unwanted medicines to the pharmacy for disposal ask them to
contact the pharmacy to discuss how to arrange disposal of the medicines.
• Phone the pharmacy to confirm that all medicines have been delivered.
9|Page
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Appendix 1-Community Palliative Care Pharmacies
To find your nearest open palliative care pharmacy, including neighbouring areas, please go
to https://pcm.prescqipp.info/ and enter your postcode
10 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Appendix 2 NHS.Net Email Addresses Palliative Care Pharmacies
Trading Name Telephone # NHS Mail
Accounts
Audley Mills Pharmacy 01268 776 479 nhspharmacy.rayleigh.audleymilfe149@nhs.net
Blackwater Pharma 01621 855 118 nhspharmacy.maldon.blackwaterpharmafph83@nhs.net
Chemist@Southend 01702 612 003 nhspharmacy.southendonsea.southendpharmacyfea52@nhs.net
Christchurch Pharmacy 01376 328 157 nhspharmacy.braintree.christchurchpharmacyfcm69@nhs.net
Crompton Pharmacy ```01245 357425 nhspharmacy.chelmsford.cromptonpharmacyfjq62@nhs.net
Derix Healthcare Pharmacy 01702 715 558 nhspharmacy.leighonsea.derixhealthcarepharmfh669@nhs.net
Hassengate Pharmacy 01375 641 569 nhspharmacy.slh.hassengatepharmacyft060@nhs.net
Pharmchoice Pharmacy 01277 215 809 nhspharmacy.brentwood.pharmchoicepharmacyfjm44@nhs.net
Well Halstead – Weaver Ct 01787 479 793 nhspharmacy.halstead.wellpharmacyfpl44@nhs.net
To find your nearest open palliative care pharmacy, including neighbouring
areas, please go to https://pcm.prescqipp.info/ and enter your postcode
This includes all community pharmacies across the East of England who have been
commissioned as Palliative Care Pharmacies and hold an agreed list of palliative care
and specialist drugs. Please be aware that lists of drugs held may vary slightly.
11 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Appendix 3 RPS guidance on ethical, professional decision making
in the COVID-19 Pandemic
Full guidance can be found here: https://www.rpharms.com/resources/pharmacy-
guides/coronavirus-covid-19/coronavirus-information-for-pharmacists/ethical-decision-making#7
Summary
There is a wide recognition that all pharmacists and pharmacy technicians, like other health
professionals, are working under extreme pressures during the current pandemic. These are likely to
get worse before they get better and may recur. Staff are already having to make prioritisation
decisions and are planning for previously unseen situations. Pharmacists and pharmacy technicians are
often by their very nature perfectionists and strive to do their best. When we find ourselves in
situations such as these, perfectionism is counterproductive. We recognise that safe and effective care
– rather than ideal care – may be the best and right kind of care to provide, in the context of the COVID-
19 challenge. Pharmacists and pharmacy technicians will need to make quicker, timelier decisions
which may feel uncomfortable, have increased belief in their own experience, and draw upon
experience around them. The guidance in this document is intended for utilisation by all sectors of the
profession and by staff in both strategic roles and those in roles closer to patients.
Decisions we make should be:
• based on the best evidence available at the time
• reasonable and proportionate in the circumstances
• made in accordance with the latest government, NHS, regulatory and professional guidance
and should take account of employers’ guidance
• made as collaboratively as possible, remembering that every decision made will impact on
others, both patients and professionals
• designed to secure safe and effective patient care as far as practicable
• timely, recognising that pressure of time means that rather than striving for perfection,
decisions may have to be “good enough for the circumstances”
• recorded, including the reasons why decisions were made to ensure accountability and
understanding of prevailing circumstances at the time
In line with the principles above, any judgements on decisions and conduct during this pandemic will
be based on all the prevailing circumstances at the time of the decisions and conduct, not with the
benefit of hindsight. This is supported by the joint statement from the health and care professional
regulatory bodies.
www.pharmacyregulation.org/news/regulatory-approachchallenging-circumstances-gphc-and-psni-
joint-statement
The latest guidance on issues relating to the COVID-19 pandemic can be found at
www.rpharms.com/coronavirus/
See also https://www.pharmacyregulation.org/news/how-we-will-continue-regulate-light-novel-
coronavirus-covid-19
12 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Appendix 3 contd: Pertinent extracts from RPS guidance on ethical,
professional decision making in the COVID-19 Pandemic –
Guidance relating to specific issues
Maintaining patient safety
Pharmacists’ key priorities are to protect patients and to make optimal use of medicines.
Allocating scarce supplies of medicines and devices
• Shortages in the medicine supply chain are not uncommon and significantly exacerbated during
surges of demand. Staff at all levels and in all settings may be asked to make difficult and time-
pressurised decisions around which patients receive which medicines, although the form of these
decisions will vary.
• Where decisions are made that would not be taken in normal circumstances, a brief record of the
justifications and prevailing conditions should be made.
• It is common and acceptable practice to operate a “First come, First served” queuing approach,
until medicines availability becomes critical. At this point, pharmacists should use their discretion
and professional judgement as to the apportionment of scarce medication. For example, it may be
appropriate to apportion available stock amongst current patients to allow time for treatment
options to be considered and potentially adjusted.
Following of legislative requirements
• The law is a minimum standard to allow society to function. It is designed in such a way that it is
read as being universally applicable without context. The circumstances being witnessed are
exceptional.
• So long as a pharmacist is able to account for their decisions, some departure from strict legal
requirements may be the right thing to do, for example to reduce the risk of death or reduce
intolerable pain.
Record keeping
• Accountability of professionals is an important part of our covenant with the public. To achieve this
and to protect ourselves, we make records.
• Pharmacists and pharmacy technicians are advised to make notes of all key decisions made
including the environmental circumstances at the time the decisions were made and any key facts.
Should a complaint be received at a later date, decisions relating to conduct will be made in the
context of the prevailing conditions at the time.
• Such conditions might include urgency/time available to make decision, needs of other patients,
availability of medicines, access to prescribers and other specialist colleagues, time at work,
availability of rest/meal breaks, availability of resources, indicative competing demands (including
personal circumstances), and staff to patient ratios.
Procurement and distribution
• When there are known shortages of medicines and devices there is a potential conflict between
obtaining stock to meet the needs of regular patients and reducing stock available for patients
elsewhere.
• To ensure fairness to all patients, pharmacists and pharmacy technicians should not stockpile. It is
vital that knowledge regarding shortages is shared in a timely manner with all relevant
13 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
professionals. This allows for better decision making all round, better care for patients, especially
palliative patients, and can reduce stress.
• Stockpiling of medicines in areas not in official supply pathways should be strongly discouraged
such as doctor’s bags, community hubs and care homes as such actions are likely to disrupt supply
to those who need it most.
• Pharmacists and pharmacy technicians in both primary and secondary care procurement and
distribution, and in clinical care functions, may be faced with supply challenges. This may involve
consideration of alternative suppliers or sources of medicines. Care should be taken to ensure use
of approved suppliers and quality of medicines offered.
• Normal procedures regarding deliveries and returns may need to become more flexible to take into
account opening times, staff availability and minimise wastage.
Re-purposing of medicines
• All pharmacists and pharmacy technicians should act to ensure the most prudent use of medicines.
• Under no circumstances is it currently acceptable* to supply patient-returned or date-expired
medicines without further regulatory advice as this would be in contravention of section 64(1) of
the Medicines Act 1968 if a patient is harmed by taking a medicine that is not of the nature or
quality demanded.
• Should the situation arise that key medicines become unavailable, it may be necessary to give
consideration to the use of some patient returned medication (for example from end of life packs)
or that which is recently expired.
• Subject to the availability of space and segregation from in-date stock, pharmacists and pharmacy
technicians should retain patient-returned medicines that are likely to be in short supply (taking
account of the latest COVID-19 infection control guidance) as well as recently expired medicines
that appear of suitable quality for triage and potential reuse in case they are needed for future
supply should in-date stocks be declared exhausted.
*Note: Since the RPS guidance was written the UK Government has published ‘Standard operating
procedure on how to run a safe and effective medicines reuse scheme in a care home or hospice during
the coronavirus outbreak.’ https://www.gov.uk/government/publications/coronavirus-covid-19-reuse-of-
medicines-in-a-care-home-or-hospice.
Mid and south Essex SOP for Re-Use of Medicines in Care Homes can be found here:
https://midessexccg.nhs.uk/medicines-optimisation/covid-19-resources/care-homes-1
14 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Access to EOL medicines in primary care during COVID-19 Pandemic
Appendix 3 Priority medicines for palliative and end of life care
during a pandemic
During the coronavirus pandemic, additional demand on some medicines and other supplies is
inevitable. The demand for drugs used, especially for managing symptoms frequently seen in people
infected with coronavirus, will increase.
This guidance sets out a small set of key medicines for palliative and end of life care that need to be
managed nationally with local collaboration across all sectors.
This has been produced in conjunction with the Chief Pharmaceutical Officer and National Clinical
Director for End of Life Care at NHS England and NHS Improvement. Although direct alternative
drugs are offered, the options identified are not exhaustive and local formularies may continue to
guide decisions where stocks are available.
This formulary covers use of medicines for palliative and end of life care across all sectors.
https://apmonline.org/wp-content/uploads/2020/04/priority-meds-for-end-of-life-care-290420-final-2.pdf
15 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021Appendix 4 Red Cross Medication Transport Documentation
16 | P a g e
20200405MSESTPAccess to EoL Medicines June 2020 Review May 2021You can also read