Advances in Narcolepsy from Pathogenesis to Treatment
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Advances in Narcolepsy from
Pathogenesis to Treatment
Chad Ruoff, MD
Sleep and Obesity Medicine
Partner, Southern California Kaiser Permanente Medical
Group (SCPMG), Kaiser Woodland Hills
Adjunct Clinical Assistant Professor, Stanford University
10.26.2019 from 8:45 AM - 9:45 AM
Disclosures • No disclosures to report.
Objectives 1. Pathophysiology 2. Diagnosis 3. Comorbid Conditions 4. Treatments
PATHOPHYSIOLOGY

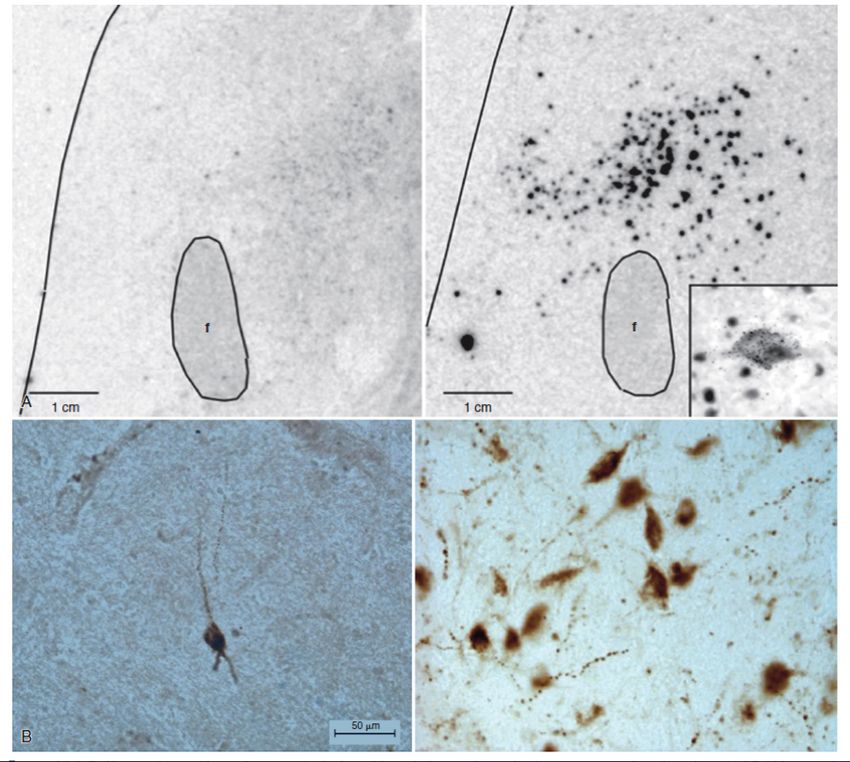
Loss of hypocretin neurons in Narcolepsy type 1
Narcolepsy Control Brain
Loss of hypocretin neurons
in the dorsolateral Significant reduction of hypocretin mRNA
hypothalamus (70,000 expression in the lateral hypothalamus in a
neurons) narcoleptic versus a control brain.
Narcoleptics have an 85%
to 95% reduction in the Significant reduction of hypocretin-stained
peptides in hypocretin cells (in the lateral
number of hypocretin
hypothalamus) in a narcoleptic versus a
neurons control brain.
Peyron C, Faraco J, Rogers W, et al: A mutation in a case of early onset narcolepsy
and a generalized absence of hypocretin peptides in human narcoleptic brains. Nat
Med 2000;6:991-997. B, and modified from Thannickal TC, Moore RY, Nienjuis R, et
al: Reduced number of hypocretin neurons in human narcolepsy. Neuron
2000;27[3]:469-474.)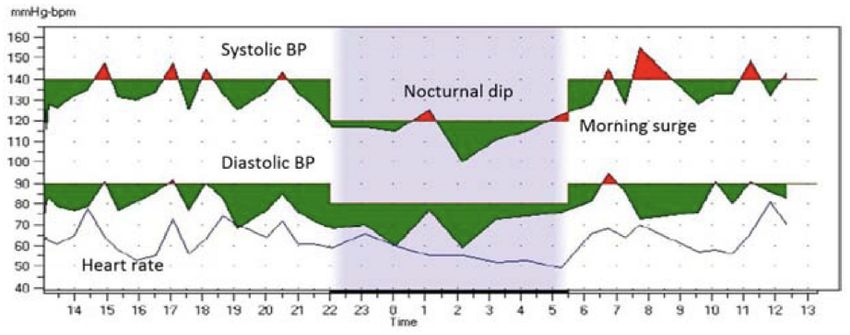
NT1 most likely an autoimmune disease
• Almost all patients with NT1 carry specific HLA marker called HLA DQB1*06:02
– HLA system helps to regulate the immune system
• Often preceded with streptococcus or influenza
• Onset of disease common in late spring/early summer after the winter months
• Pandemrix inoculation: 8–12-fold and 3-5 fold increase in new cases of NT1 in children and
adults, respectively
• H1N1 flu infection: 3 fold increase in new cases of NT1 in the months after the H1N1
pandemic in China
Mahoney et al, 2019 Nat Rev Neurosci;
Miyagawa and Tokunaga, 2019 Human
Genome Variation; Honda et al 1983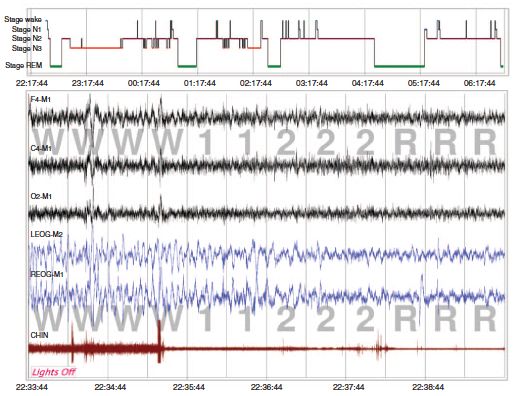
Mounting data coming in that NT1 is likely an
autoimmune disease mediated by T Cells
• Mutation in the TCR α-chain gene doubles risk of NT1
• Rare SNPS within the TCR genes increases reactivity of T cells to
fragments of the orexin neuropeptides
• Variants of OX40L, which is involved in T cell differentiation
• Higher CD4+ memory T cells recognizing hypocretin fragments in
PWN1 (10 fold higher than controls
• CD8 T cells from PWN1 and healthy controls recognize hypocretin
neuron specific antigen
Mahoney et al, 2019 Nat Rev Neurosci; Luo G et al, 2018 Proc Natl Acad
Sci; Latorre D et al, 2018 Nature; Pedersen N et al. 2019 Nature
Communications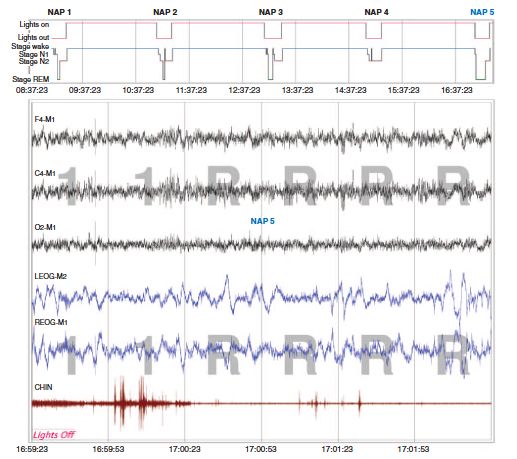
Specific T-cell activation in peripheral blood and cerebrospinal fluid
seen not only in patients with NT1 but also NT2 and IH
Specific T-Cell Activation
• Activated T-cells in
the CNS associated
with higher amounts
of objective
sleepiness in the NT1
group and self-
reported sleepiness
in the IH group
Lippert J et al. 2019 Sleep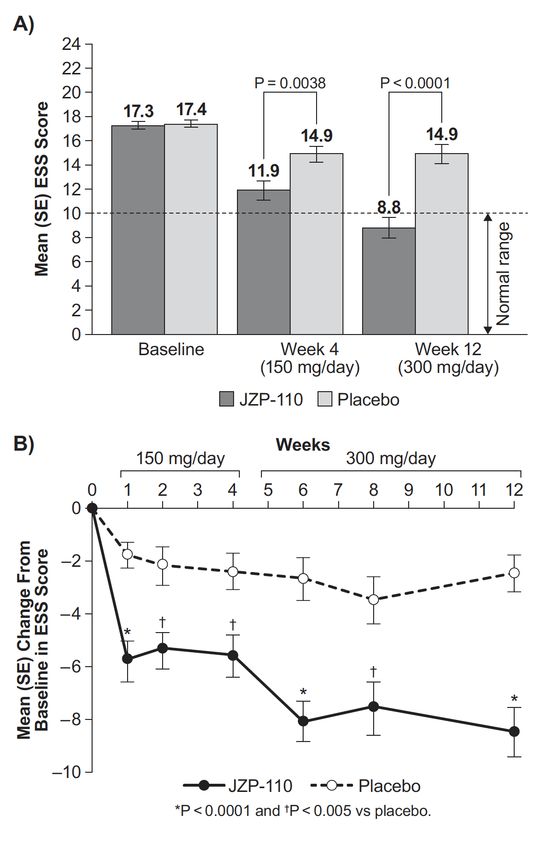
DIAGNOSIS
CNS Hypersomnias
Narcolepsy
Type 1
Type 2
Idiopathic Hypersomnia
Kleine-Levin Syndrome
Hypersomnia Due to a Medical Disorder
Hypersomnia Due to a Medication or Substance
Hypersomnia Associated with a Psychiatric Disorder
Insufficient Sleep Syndrome
Isolated Symptoms and Normal Variants
Long SleeperDiagnostic Tools
History Actigraphy PSG HLA DQB1*06:02
This Photo by Unknown Author is licensed under CC BY-SA-NC
Sleep Diary MSLT
ESS CSF HypocretinThe History: Narcolepsy Pentad 1. Excessive daytime sleepiness (EDS) 2. Cataplexy 3. Sleep-related hallucinations 4. Sleep paralysis 5. Disrupted nighttime sleep
Cataplexy in Dobermans
Courtesy of Emmanuel MignotCataplexy
Overeem S, Mignot E, van Dijk JB, Lammers GJ: Narcolepsy: clinical features, new pathophysiologic insights, and
future perspectives. J Clin Neurophysiol 2001;18[2]:78-105.)Cataplexy
Segment 1. (Patient 1) ‘‘Cataplectic facies’’
with permanent facial weakness on which a
cataplectic attack (jaw sagging, head dropping,
and eye closure) is superimposed, the small
frame shows the trigger stimulus (a cartoon).
The facial weakness is also present during
normal activity without stimulus.
Segment 2. (Patient 17) ‘‘Cataplectic facies’’
followed by two partial and a full blown
cataplectic attack with fall. During the third
episode and prior to the fall the patient
presents repetitive lapses of postural tone
mainly affecting the legs.Cataplexy: Triggers and Muscle Group(s)
A. Cataplexy-like symptoms reported by 46% of the non-narcolepsy subjects. Best differentiated from other
types of muscle weakness when triggered by three typical situations: when hearing or telling a joke, while
laughing, or when angry. B. Most commonly affected muscle groups involve the legs/knees.
Ruoff C, Mignot E, Central Nervous System Hypersomnias; A, Modified from Anic-Labat S, Guilleminault C, Kraemer HC, et al:
Validation of a cataplexy questionnaire in 983 sleep-disordered patients. Sleep 1999;22[1]:77-87. B, C, and D, Modified from Okun
ML, Lin L, Pelin Z, Hong S, Mignot E: Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002;25[1]:27-35.)Cataplexy: Duration and Frequency
C. Cataplexy typically lasts from a few seconds to nearly 30 seconds. D. Episodes typically occur
from once per day to several times per week.
Ruoff C, Mignot E, Central Nervous System Hypersomnias; A, Modified from Anic-Labat S, Guilleminault C, Kraemer HC, et al:
Validation of a cataplexy questionnaire in 983 sleep-disordered patients. Sleep 1999;22[1]:77-87. B, C, and D, Modified from Okun
ML, Lin L, Pelin Z, Hong S, Mignot E: Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002;25[1]:27-35.)Sleep Hallucinations • Vivid, “waking dreams” that occur during transitions between sleep and wakefulness – Hypnogogic (occurring at sleep onset) – Hypnopompic (occurring upon awakening) • May accompany sleep paralysis or occur independently • Often occurs in normal individuals but is far more common in narcoleptics • Tend to be visual but may also be tactile or auditory (e.g., shadows) • Some awareness of surroundings is preserved
Sleep paralysis • The inability to move for a few seconds or minutes as falling asleep or upon awakening • Often occurs in normal individuals but is far more common in narcoleptics • Paralysis ends spontaneously (fear reaction is most common at least the first few times it occurs)
Disrupted nighttime sleep
• Common aspect of narcolepsy
• Such as:
– Frequent arousals
– Higher wakefulness after sleep onset (WASO)
– Frequent shifts to wake or increased N1 sleep
with reduction in N3 (SWS)
– Decrease in overall sleep efficiency (SE)Diagnostic Criteria: Narcolepsy Type 1
Criteria A and B required:
A. The patient has daily periods of irrepressible need to sleep or daytime
lapses into sleep occurring for at least three months.
B. The presence of one or both of the following:
1. Cataplexy (as defined under Essential Features) and a mean sleep
latency of ≤ 8 = minutes and two or more sleep onset REM periods
(SOREMPs) on an MSLT performed according to standard techniques. A
SOREMP (within 15 minutes of sleep onset) on the preceding nocturnal
polysomnogram may replace one of the SOREMPs on the MSLT.
2. CSF hypocretin-1 concentration, measured by immunoreactivity, is
either ≤ 110 pg/mL orDiagnostic Criteria: Narcolepsy Type 2
Criteria A-E required:
A. The patient has daily periods of irrepressible need to sleep or daytime
lapses into sleep occurring for at least three months.
B. A mean sleep latency of ≤ 8 minutes and two or more sleep onset REM
periods (SOREMPs) are found on a MSLT performed according to standard
techniques. A SOREMP (within 15 minutes of sleep onset) on the preceding
nocturnal polysomnogram may replace one of the SOREMPs on the MSLT.
C. Cataplexy is absent.
D. Either CSF hypocretin-1 concentration has not been measured or CSF
hypocretin-1 concentration measured by immunoreactivity is either > 110
pg/mL or > 1/3 of mean values obtained in normal subjects with the same
standardized assay.
E. The hypersomnolence and/or MSLT findings are not better explained by
other causes such as insufficient sleep, obstructive sleep apnea, delayed
sleep phase disorder, or the effect of medication or substances or their
withdrawal.
International Classification of
Sleep Disorders, Third Edition
(ICSD-3)Diagnostic Criteria: Idiopathic Hypersomnia
Criteria A-F required:
A. The patient has daily periods of irrepressible need to sleep or daytime lapses into
sleep occurring for at least three months.1
B. Cataplexy is absent.
C. An MSLT performed according to standard techniques shows fewer than two sleep
onset REM periods or no sleep onset REM periods if the REM latency on the preceding
polysomnogram was less than or equal to 15 minutes.
D. The presence of at least one of the following:
1. The MSLT shows a mean sleep latency of ≤ 8 minutes.
2. Total 24-hour sleep time is ≥ 660 minutes (typically 12–14 hours) on 24-hour
polysomnographic monitoring (performed after correction of chronic sleep
deprivation), or by wrist actigraphy with a sleep log (averaged over at least
seven days with unrestricted sleep).
E. Insufficient sleep syndrome is ruled out (if deemed necessary, by lack of
improvement of sleepiness after an adequate trial of increased nocturnal time in bed,
preferably confirmed by at least a week of wrist actigraphy).
F. The hypersomnolence and/or MSLT findings are not better explained by another
sleep disorder, other medical or psychiatric disorder, or use of drugs or medications.
Notes
1. Severe and prolonged sleep inertia, known as sleep drunkenness (defined as prolonged difficulty waking up with repeated returns to sleep, irritability, automatic behavior,
and confusion) and/or long (> 1 hour), unrefreshing naps are additional supportive clinical features.
2. A high sleep efficiency (≥ 90%) on the preceding polysomnogram is a supportive finding (as long as sleep insufficiency is ruled out).
3. The total 24-hour sleep time required for diagnosis may need to be adapted to account for normal changes in sleep time associated with stages of development in
children and adolescents as well as for variability across cultures in all age groups.
4. Occasionally, patients fulfilling other criteria may have an MSLT mean sleep latency longer than 8 minutes and total 24-hour sleep time shorter than 660 minutes. Clinical International Classification of
judgment should be used in deciding if these patients should be considered to have idiopathic hypersomnia (IH). Great caution should be exercised to exclude other Sleep Disorders, Third Edition
conditions that might mimic the disorder. A repeat MSLT at a later date is advisable if the clinical suspicion for IH remains high. (ICSD-3)Narcolepsy versus Idiopathic Hypersomnia
Ruoff C, Mignot E, Central Nervous System HypersomniasDIAGNOSTIC CHALLENGES
What Best Predicts Excessive Daytime Sleepiness (EDS) in the
General Population?
Depression (stronger in the younger, independent of use of antidepressant medication)
BMI
Age
Subjective estimate of typical sleep duration
Diabetes
Smoking
Sleep Apnea
Bixler E et al. 2005; Young T et al. 1993A Positive MSLT for Narcolepy/Idiopathic Hypersomnia:
Once Positive, Always Positive on Repeat?
100%
91.2%
90%
81.3%
80%
70%
Study 1
60% 57.1%
Study 2
50% 47.1%
Study 3
40% 36.8%
33.3%
30% 25.0%
20%
10% 7.7% *
0%
NT1 NT2 IH Controls Study 1: Ruoff et al 2018; Study 2: Lopez et
al 2017; Study 3: Trotti et al 2013;How often is a MSLT positive for Narcolepsy in
the General Population?
• 6% of men and 1 % of women
– Repeatability of these findings several years later was poor
• Shift-workers 30 times more likely to have a positive MSLT
• Patients on antidepressant medications up to 11 times more
likely to have a positive MSLT
Mignot et al. Brain 2006; Goldbart et al Sleep 2014No blood test yet
DIAGNOSTIC ADVANCES
Use of the MSLT for the Diagnosis of Narcolepsy
type 1 in Children
• The PSG + MSLT is a good test (sensitivity 94.87% and specificity 100%)
for children with NT1
• At least 2 SOREMPs OR a mean sleep latency ≤8.2 minutes (area under
the ROC curve of 0.985), at the MSLT are valid and reliable markers for
pediatric NT1 diagnosis.
Pizza F et al 2019 NeurologyHow We Look at Sleep on a Sleep Study Now: A
Sleep HypnogramHow We May Soon Look at Sleep on a Sleep
Study: A Hypodensity Graph
Displays probabilities for a given stage of sleep (rather than discrete stages of sleep) across time (down to 5
seconds compared to 30 seconds)
Color codes: white, wake; red, N1; light blue, N2; dark blue, N3; black, REM Stephansen JB et al. 2018 Nat
CommunFinding a Unique Marker for Narcolepsy on the
Overnight Sleep Test
• Unique, Overlapping Sleep Stages on Overnight Sleep Test is specific (96%) for
narcolepsy
• Adding HLA-DQB1*06:02 typing to this makes it even more specific (99%) for
narcolepsy (sensitivity 91%)
• Compared to MSLT data with a specificity of 98.6% and a sensitivity of 92.9%
Stephansen JB et al. 2018 Nat
Commun; Andlauer, O. et al. 2013
Jama NeurolHypocretin/Orexin Test is
Commercially Available
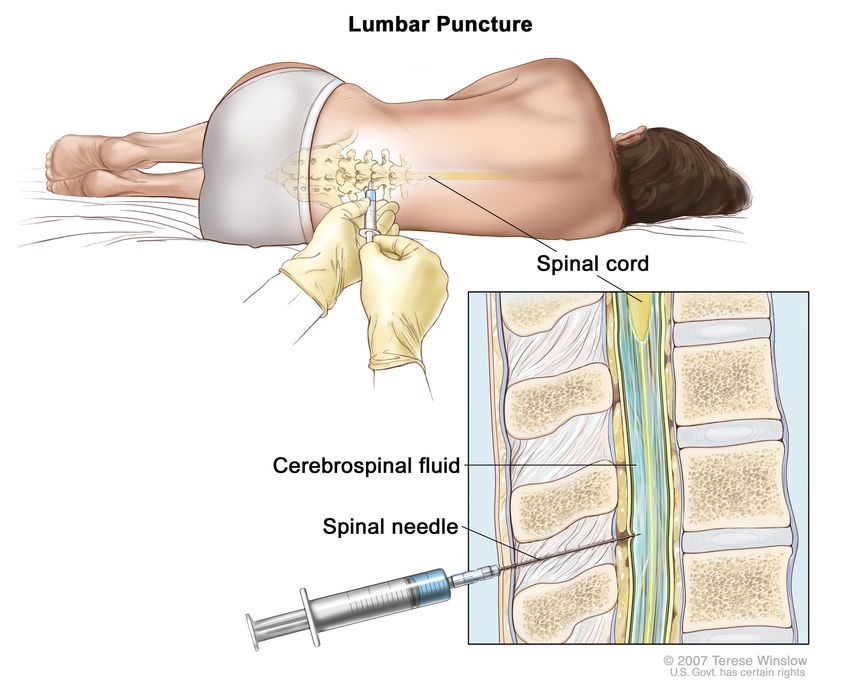
CSF Hypocretin
CSF hypocretin-1 concentration, measured by
immunoreactivity, is ≤ 110 pg/mL is diagnostic for NT1Lower Levels of Hypocretin-1 in Cerebrospinal
Fluid Revealed by a New Method (Mass
Spectrometry) Compared to Old Method
(Radioimmunoassay)
• 19 times lower level in healthy controls
• 22 times lower level in NT1 patients
• Intact hcrt-1 peptide was less than 10% of the total amount using a
different method as well (i.e. high performance liquid chromatography)
• These results question what is being detected by available method
• And, suggests that physiological concentrations of the peptide might be
much lower than previously believed
Bardsen K et al 2019 Anal Chem; Sakai N et al. 2019
Scientific Reports; Hirtz C et al. 2016 Scientific
ReportsMEDICAL COMORBID CONDITIONS
Obesity and Narcolepsy
• Daniels, in 1934, reported up to 50% of patients gain weight (5
– 45 kg) around the time of disease onset
• Obesity has been reported in up to 42 % of adults and 60 % of
children with narcolepsy
Daniels L et al., Medicine 1934; Schuld A et al., Lancet 2000;
Dahman N et al., Eur Arch Psychiatry Clin Neurosci 2001; Schuld A
et al., Lancet 2000; Honda Y et al., Sleep 1986; Kok SW et al., Obes
Res 2003; Inocente C et al., CNS Neuroscience & Therapeutics
2013; Kotagal S et al., Sleep Med 2004; Aran A et al., Sleep 2010;
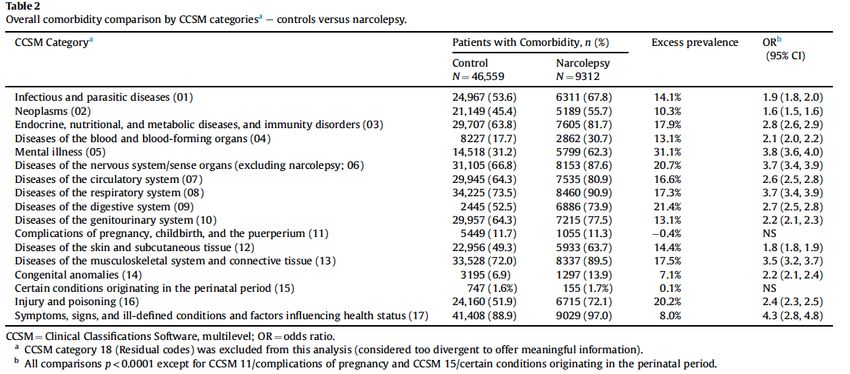
Peraita-Adrados R et al., Sleep Med 2011Medical Comorbidities Increased in Narcolepsy vs
Controls
Black et al. Sleep Medicine 2017; Jennum et al.
Sleep Medicine 2017; Jennum et al. Sleep
2013; Ohayon. Sleep Medicine 2013Medical Comorbidities in Narcolepsy with and without cataplexy compared to
controls
1. Infectious diseases
2. Neoplasms
3. Endocrine, nutritional, metabolic,
immune
4. Diseases of blood and blood-
forming organs
5. Mental Illness
6. Nervous system
7. Circulatory system
8. Respiratory system
9. Digestive system
10. Genitourinary system
11. Complications of pregnancy, peri,
and postpartum
12. Skin and subcutaneous tissue
13. Musculoskeletal system
14. Congenital anomalies
15. Perinatal period
16. Injury and poisoning
17. Ill-defined conditions and factors
Black et al. Sleep Medicine 2017Blood pressure and heart rate in patients with
narcolepsy
• Blood pressure in patients and animal models with NC
associated with non-dipping pattern
• Heart rate in patients and animal models with NC is variable
during wakefulness and normal to high during sleep
Turner J et al. Am J Med 2015Patients with narcolepsy 44 times more likely to have REM
Behavior Disorder (RBD) than controls
• Patients with RBD at increased risk of developing diseases such as
Parkinson’s Disease
– α-synuclein deposits found in Parkinson's Disease
• Skin biopsy was positive for α-synuclein deposits in 86.7% of non-
narcoleptic patients but in none of narcoleptic patients with ’REM
Behavior Disorder’ (RBD)
• GREAT NEWS: Since no patients with narcolepsy with “RBD” had α-
synuclein deposits on skin biopsy then not likely to be at same
heightened risk of developing Parkinson’s Disease as non-narcoleptic
patients with RBD
Antelmi E et al. 2019 Ann Clin Transl Neuro; Black et al. Sleep
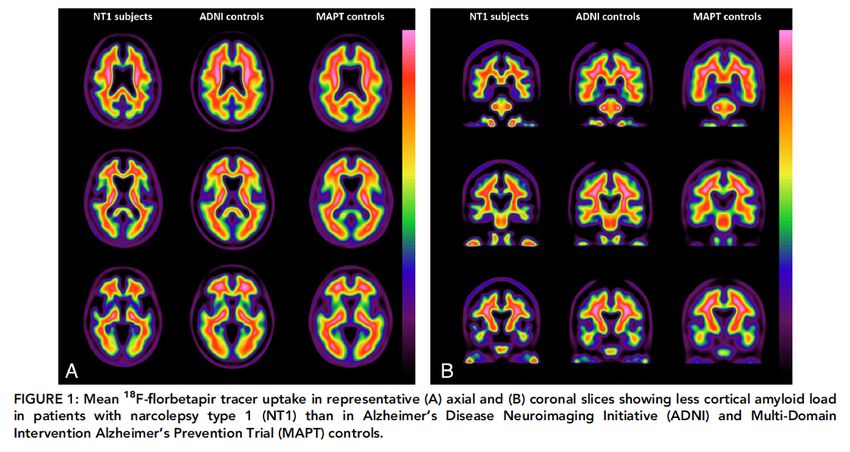
Medicine 2017Reduced brain amyloid burden in elderly patients with narcolepsy
type 1
• Amyloid plaques found in brains of patients with Alzheimer’s
Disease
• GREAT NEWS: Lower levels of amyloid in elderly patients with
NT1 suggests a reduced risk for progression to Alzheimer’s
Disease
Gabelle A et al 2019 Ann NeurolGREAT NEWS: Increased creative thinking in PWNs
• Higher creative potential in patients with narcolepsy and further
support a role of rapid eye movement sleep in creativity
• Most symptoms of narcolepsy (including sleepiness, hypnagogic
hallucinations, sleep paralysis, lucid dreaming, and rapid eye
movement sleep behaviour disorder, but not cataplexy) were
associated with higher scores on the Test of Creative Profile
Lacaux et al. 2019 BrainPSYCHIATRIC COMORBID CONDITIONS
Psychiatric Comorbidities Increased in Narcolepsy
vs Controls
Ruoff et al. J Clin Psychiatry 2017; Ohayon.
Sleep Medicine 2013What about conditions previously associated with
NarcolepsyBEHAVIORAL TREATMENTS
Good Sleep Health and Other Healthy Habits
• Dim the lights at night and get
plenty of light in the morning
• Define optimal sleep duration
• Keep regular sleep schedule
– Keep social events within normal
sleep-wake schedule
• Scheduled naps and optimize
duration of nap
• In addition to healthy eating at
consistent times, staying hydrated,
limiting alcohol intake....CURRENT PHARMACOLOGIC TREATMENTS
Excessive Daytime Sleepiness
Sodium oxybate
Modafinil 100 – 400 mg Armodafinil 150 – 250 mg
4.5 – 9 gm nightly
Combination short and
Methylphenidate/Dextro- Sodium oxybate +
longer acting
amphetamine 5 – 60 mg stimulant/alerting
stimulant/alerting
medication
medication
Solriamfetol 75 – 150 mg Pitolisant 9 – 36 mg
Barateau et al. Curr Treat Options Neurol 2016Effect of Sodium Oxybate on Cataplexy in Children with
Narcolepsy Type 1
Plazzi G, et al., Lancet Child Adolesc Health. 2018Effect of Sodium Oxybate on Epworth Sleepiness Scale in
Children with Narcolepsy Type 1
Plazzi G, et al., Lancet Child Adolesc Health. 2018Excessive Daytime Sleepiness
Inhibits reuptake at
dopamine and
Solriamfetol 75 – 150 mg
norepinephrine
transporters
Barateau et al. Curr Treat Options Neurol 2016Effect of Solriamfetol (JZP-110) on Epworth Sleepiness
Scale in PWN
Ruoff C, et al. Sleep 39(7)2016Effect of Solriamfetol (JZP-110) on Ability to Stay Awake
(MWT Test) in PWN
Ruoff C, et al. Sleep 39(7)2016; Bogan et al 2015Excessive Daytime Sleepiness
Taken in the
Selective histamine
Morning as a single dose;
H3 receptor inverse
Pitolisant 9 – 36 mg May improve cataplexy as
agonist, activates
well but not FDA approved
histamine neurons
for cataplexy
Barateau et al. Curr Treat Options Neurol 2016Effect of Pitolisant, Modafinil, Placebo on Epworth
Sleepiness Scale in PWN
No psychostimulants for >= 14
days before baseline
Could remain on their
anticataplectic drugs (sodium
oxybate or antidepressants) at
stable doses 1 month before and
throughout the trial
8 week trial Dauvilliers Y, et al. Lancet Neurol 2013Effect of Pitolisant on Cataplexy in PWN
Pitolisant decreased weekly
cataplexy rate by 75% from
baseline levels, while the
placebo group decreased rate
by 38% from baseline levels
Szakacs Z et al. Lancet Neurology 2017Effect of Pitolisant on Epworth Sleepiness Scale and Cataplexy in PWN
One-third of patients stopped pitolisant, mostly (19.6%) for
insufficient benefit
Dauvillers Y et al. 2019 SleepEffect of Pitolisant on Cataplexy and Other Features of Narcolepsy
Dauvillers Y et al. 2019 SleepCataplexy
Venlafaxine Sodium oxybate Sodium oxybate + other
37.5 – 300 mgs 4.5 – 9 gm nightly anti-cataplectic
Fluoxetine
20–60 mg/day Clomipramine Duloxetine
Citalopram 10 – 150 mgs 10 – 60 mgs
20–40 mg/day
Atomoxetine * Pitolisant
10 – 60 mg 10 – 60 mg
* Pitolisant is not FDA approved for cataplexy Barateau et al. Curr Treat Options Neurol 2016FUTURE/NOVEL PHARMACOLOGIC
TREATMENTSTAK-925 (IV) and TAK994 (Oral) Selective Orexin Type-2
Receptor (OX2R) Agonist
• TAK-925 tolerated in patients with NT1 and increased
wakefulness compared to placebo
• TAK-925 tolerated in healthy sleep-deprived adults and
increased wakefulness at night compared to placebo
• TAK-994, an oral selective OX2R agonist, reduced
narcolepsy symptoms in narcolepsy mouse models and
is progressing in Phase 1 studies
https://www.takeda.com/newsroom/newsreleases/2019/new-data-presented-at-world-sleep-congress-demonstrate-early-signs-of-efficacy-for-tak-925-
a-selective-orexin-type-2-receptor-ox2r-agonist-in-patients-with-narcolepsy-type-1/AXS-12 (Reboxetine)
• A highly selective and potent norepinephrine reuptake
inhibitor.
• Extensive safety record in Europe and in over 40 countries
where it is approved for the treatment of Depression
• Supported by pre-clinical and preliminary clinical results where
it significantly reduced narcoleptic episodes in hypocretin
(orexin)-deficient mice as well as improving daytime sleepiness
with reduced cataplexy in patients with narcolepsy in an open-
label pilot trial
https://clinicaltrials.gov/ct2/show/NCT03881852?term=reboxetine&cond=narcolepsy&rank=1;
Larrosa O et al. 2001 Sleep; https://axsome.com/axs-pipeline/about-axs-12/GABA Potentiation in Patients with Idiopathic
Hypersomnia
• Cerebrospinal fluid from patients with IH may have enhanced
activity at GABA-A receptors in vitro, in excess of that of
cerebrospinal fluid from controls
• Symptoms of IH may be reversible in some patients with use of
GABA-receptor antagonists or negative allosteric modulators
(e.g., clarithromycin, flumazenil)
Rye D et al. 2012; Trotti LM et al. 2014; Trotti
LM et al. 2016; Dauvillers Y et al. 2016; Trotti
et al. Ann Neurol. 2015 September; Trotti et
al. 2016BTD-001
BTD-001 (Pentetrazol), a GABA-A receptor
antagonist, for IH/Narcolepsy Type 2
Visit https://clinicaltrials.gov to find BTD-001 study and others.
You can also visit: http://www.arisestudies.com/
A Study of Safety and Efficacy of BTD-001 in Treatment of Patients With Idiopathic
Hypersomnia (IH) or Narcolepsy Type 2JZP-258
• Sodium oxybate at 9 grams per night contains 1,640 mg of sodium
– Recommended upper limit of normal intake is 2300 mg per day
• JZP-258: 92% less sodium than sodium oxybate (Xyrem®)
• Patients randomized to JZP-258 showed clinically meaningful maintenance
of efficacy for both cataplexy and EDS, while a statistically significant
worsening for both cataplexy and ESS endpoints was observed in the
placebo group compared with JZP-258
• The safety profile of JZP-258 was consistent with sodium oxybate
https://investor.jazzpharma.com/news-releases/news-release-details/jazz-pharmaceuticals-announces-positive-
top-line-results-phase-3FT218
• A once-nightly formulation of sodium oxybate utilizing the Company's
proprietary Micropump® technology
– Micropump® is a microparticulate system that allows the
development of modified and/or controlled release of solid, oral
dosage formulations of drugs
• Demonstrated lower overall peak plasma concentrations (Cmax) and
similar total exposures (AUC), compared to twice-nightly sodium
oxybate in a head-to-head study
• Phase 3, multi-centered, double-blind, placebo-controlled REST-ON trial,
expected to complete enrollment in 2020
http://www.marketwired.com/press-release/flamel-technologies-doses-first-patient-rest-on-phase-iii-trial-ft218-excessive-daytime-nasdaq-
flml-2183873.html; https://www.globenewswire.com/news-release/2019/06/04/1863804/0/en/Avadel-to-Present-New-Data-on-Once-
Nightly-Sodium-Oxybate-at-SLEEP-2019-Conference.html•
Baclofen
Baclofen and Sodium Oxybate increased total sleep time and delta waves during
sleep in PWN
– Only sodium oxybate had an effect on daytime sleepiness and cataplexy at 3 months
– Improvement of total nocturnal sleep time had no beneficial effect on daytime
sleepiness
• R-Baclofen and Sodium Oxybate in Mouse Model of Narcolepsy
– R-Baclofen suppressed cataplexy more than sodium oxybate
• 3 Case Reports/Series
– 40-50 mg qhs improved EDS and cataplexy (ESS 22 to 10; cataplexy from 1-2/daily to 2-3
/week)
– Two patients experienced almost complete resolution of cataplexy
– 5 patients with NT1 treated with Baclofen (25 – 40 mg qhs) showed improvement in EDS
(ESS from 15.8 to 10.4, p < 0.05)
Huang and Guilleminault 2009; S Black et al. 2014 J Neurosci;
Wierzbicka A et al. J Sleep Res Supp 1 2014;
Lee and Douglass, 2015; Morse AM, et al 2019 Pediatr NeurolOpiates in Heroin Addicts and Mouse Model of
Narcolepsy
• Opiates increase the number and decrease size of hypocretin-
producing cells in heroin addicts
• Morphine increase the number of hypocretin-producing cells
in a mouse model of narcolepsy and in wild type mice
• Morphine decreases cataplexy in a mouse model of narcolepsy
and in wild type mice
• Morphine increases hypocretin cell activity in rats
• A patient with cataplexy treated with morphine suggesting a
relative increase in hypocretin-producing cells
Thannickal, T et al. Sci. Transl. Med 2018Opiates in patients with narcolepsy
• In 1981, a report of patient with narcolepsy given codeine for the control of Crohn’s disease noted
“disappearance of his narcolepsy, cataplexy, sleep paralysis, and hypnagogic hallucinations
• In 1996, another patient with narcolepsy, who could not continue taking stimulant drugs because of coronary
artery disease and the necessity for kidney dialysis, urged his doctor to prescribe codeine for his narcolepsy
because of the reversal of narcoleptic symptoms he had previously experienced when given codeine for pain.
His physician published the results indicating a “dramatic improvement in alertness and substantial reduction of
cataplexy,” the defining symptoms of narcolepsy
• In 1996, nine patients with narcolepsy given codeine for one week
– Sleep diaries and patient reports revealed consistent symptom improvement compared to placebo;
however, there were no significant differences in the multiple sleep latency tests
– Cataplexy was not evaluated
– 1-week trial appears to have ended investigation of opiates in narcolepsy
Harper JM, et al. Lancet 1981; Benbadis SR, et al.
Pharmacotherapy 1996; Fry JM ,et al. Sleep 1996https://clinicaltrials.gov • Visit https://clinicaltrials.gov to learn about clinical trials
Today, we have learned more about… 1. Advances in our Understanding of the Cause of Narcolepsy 2. Current Diagnostic tools and their limitations 3. Advances in Diagnostic Tools 4. Medical and Psychiatric Comorbid Conditions in PWN 5. Current and Novel/Future Treatment options
You can also read