Alcohol and older people - ALCOHOL AND SOCIETY 2019 - IOGT-NTO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Alcohol and
older people
O L A ND
ALCOH
T Y 2 0 19
SOCIE
A SURVEY OF INTERNATIONAL AND SWEDISH RESEARCH
The Swedish Society of Medicine, Swedish Society of Nursing
and IOGT-NTO are voluntary organisations independent of
commercial interests. The Swedish Society of Medicine is
the scientific organisation of the Swedish medical profession
and has a broad range of interests across the entire field
of medicine. The importance of lifestyle to people’s health
at both individual and societal level, is a priority issue. The
Swedish Society of Nursing is a nonprofit organization and
a forum for discussing and developing nursing care by
promoting nursing research, ethics, education and quality
in nursing. IOGT-NTO focuses on the effects of alcohol and
narcotics on individuals and society, but is also engaged in
broad social and club activities. CERA is an interdisciplinary
and collaborative centre for education and research
into hazardous use, abuse and addiction at Gothenburg
University – which works to strengthen and develop research
and education in the field of addiction, and to disseminate
scientific expertise to people working professionally in the
field of abuse and addiction, and other interested parties.
Suggested citation: ”Andreasson S, Chikritzhs T, Dangardt F, Holder H, Naimi
T, Stockwell T (2019) Alcohol and Society 2019: Alcohol and the Elderly,
Stockholm: Swedish Society of Medicine, Swedish Society of Nursing, CERA
& IOGT-NTO.”
Published by IOGT-NTO, the Swedish Society of Medicine, Swedish Society
of Nursing and CERA in cooperation with Stiftelsen Ansvar, 2019
A Swedish language version of this report is also available from
www.iogt.se, www.sls.se, www.swenurse.se or cera.gu.se.
© IOGT-NTO & Swedish Society of Medicine & Swedish Society of Nursing
& CERA, 2019
Graphic design: Petra Handin, Poppi Design
Printers: Fridholm och Partners, Hindås
ISBN: 978-91-982220-3-6
URN: urn:nbn:se:iogt-2019-aos-en
CENTRUM FÖR UTBILDNING OCH
FORSKNING KRING RISKBRUK,
MISSBRUK OCH BEROENDE (CERA)
FOREWORD
Foreword
Alcohol consumption and alcohol-relat- alcohol policy measures, and offer recommen-
ed harm, whether in the form of chronic dations for guideline alcohol consumption
disease or acute harm, has increased levels for the elderly.
amongst Sweden’s elderly in recent years. The Swedish Society of Medicine, the
The percentage of the population classified University of Gothenburg’s Center for
as elderly has increased and will continue Education and Research on Addiction
to do so. Prevention of disease and harm, (CERA), the Swedish Society of Nursing, the
including alcohol-related disease and harm, “Ansvar för Framtiden” [Responsibility for the
is, therefore, very important – both for all Future] Foundation, and IOGT-NTO issue an
those at risk and for the health and medical annual research report entitled “Alcohol and
care sector. Society”, with the aim of highlighting what
science has to teach us about the effects
The report addresses the elderly’s increased of alcohol consumption on individuals and
sensitivity to the effects of alcohol which, in society. This is the sixth such report. Previous
combination with the ageing process, may in- years’ reports have focused on such issues as
crease the risk of disease and accidents, even alcohol and young adults, the effects of low
at relatively low consumption levels. It de- dose consumption, alcohol’s second-hand
scribes the relationship between alcohol and harm, alcohol and violence, and alcohol-
various diseases and problems from which related cancers. These reports, together with
the elderly may suffer, such as cardiovascu- this year’s edition, are all available on our
lar disease, diabetes, dementia, and cancer. respective websites.
The report also highlights the significance of Alcohol consumption by the elderly is
lifetime lifestyles for health in old age. often unremarked by the health and medi-
The report’s authors comprise some of cal sector. It is our hope that this report can
the world’s leading, international alcohol help increase awareness of this issue, both
researchers, headed by Harold Holder. The amongst medical and healthcare personnel,
researchers have collated and aggregated and amongst other interested parties, and
facts and figures from international studies in that it both provokes interest and stimulates
the field and evaluated the scientific strength discussion.
of the results, and both describe the role of
Claudia Fahlke Britt Skogseid Ami Hommel Johnny Mostacero
director, chair, chair, chair,
CERA, University Swedish Society Swedish Society IOGT-NTO
of Gothenburg of Medicine of Nursing
KAPITELHUVUD
EXECUTIVE SUMMARY
Executive summary
In Sweden, as in most of the developed Risks from alcohol-related harms arise
world, older people comprise an increasing from both chronic exposure as the result
proportion of the population. For this sub- of cumulative consumption over time (e.g.,
group, the aging process in general increas- liver cirrhosis), and acute impairment from
es risks to health, safety, and quality of life heavy drinking episodes (e.g., falls and motor
and, as a result, older persons account for a vehicle crashes). Although many think of
substantial burden of health care problems alcohol-related conditions as being caused
and health-related costs in Sweden, as in only by very heavy drinking or drinking to
most countries. the point of severe intoxication, there has
been a growing recognition that lower levels
While consuming alcohol can add to the of consumption, either in aggregate or on a
health and safety risks of any age group, per-occasion basis, can cause health, safety,
these risks are increased for the older popu- and social problems, especially for older
lation. Typically, older people drink less than persons.
younger age people which may lead to the
improper conclusion that they have less risk • Heavy drinking either on average or
associated with alcohol. However, in reality per-occasion (i.e. binge drinking) increas-
the interaction of greater susceptibility to es the risk of almost all alcohol-related
alcohol’s effects and the greater health risks diagnoses, e.g., cardiovascular disease,
associated with aging combine to actually liver cirrhosis or alcohol use disorder, and
increase the risks of alcohol-related harm certain cancers.
among older people. For example, decreas-
es in body mass associated with aging can • Even drinking lower amounts of alcohol
result in higher blood alcohol concentration by older persons has some risk. For
(BAC) for older persons from consuming a example, the risk of some cancers begins
fixed quantity of alcohol. In addition, chang- to increase with any consumption. Older
es in liver metabolism, slower reaction time persons have increased risk of car crashes
and taking multiple chronic medications may at very low BAC levels, and are more
further increase both BACs and the risk of likely to incur severe injury and death than
experiencing negative alcohol-related effects younger persons.
from a given BAC.
4 A L C O H O L A N D O L D E R PEO PLE
EXECUTIVE
KAPITELHUVUD
SUMMARY
• In Sweden, alcohol consumption has to drink would be improved by reducing
increased among older persons over their consumption, either overall or during
the past 14 years in absolute terms and days in which alcohol is consumed. Among
relative to other age groups, and deaths those who drink, the lowest level of risk is
attributed to alcohol have increased one standard Swedish drink per day (12
among older Swedes. grams of pure alcohol) or less on average
and no more than 2 drinks on any one day.
• Heavy drinking is the strongest modifiable
risk factor for dementia onset. Although • Those who don’t drink or who drink While consum-
most non-randomized studies suggest that infrequently should not begin to drink,
low-volume drinking may reduce the risk of reinitiate drinking, or drink more frequently
ing alcohol
dementia, higher quality research using in order to achieve claimed health benefits. can add to
advanced medical MRI brain scans, genetic
randomization studies, and experimental
In addition, no consumption is generally
preferable among those with liver disease,
the health and
animal studies suggest that there is likely peptic ulcer disease, who take psychoactive safety risks of
no protective effect of even low-volume or sedating medications, are driving, have any age group,
consumption on cognition. cognitive difficulties, a history of falls or
poor balance or cardiac arrhythmias. these risks are
• There are a variety of public policy inter- increased for
ventions that can reduce excessive alcohol
use and reduce alcohol-related harms.
• On balance, alcohol is an unhealthy sub-
stance in which harms from heavy use is
the older
These include maintaining government considerable and supported by a robust population.
monopoly systems, increasing the price of base of scientific evidence. Even ‘mod-
alcohol (e.g., taxation, minimum pricing), erate’ use has some risks, particularly in
decreasing the physical availability of alco- older persons, and the evidence for health
hol (e.g., limiting the number of outlets), protection has eroded in recent years such
and restricting alcohol advertising. that we conclude: In many ways moderate
drinking may be a sign but not a cause of
• The level of alcohol consumption with the good health.
lowest health risk is zero. However, the
health of most older persons who continue
ALCOH OL AND OLDER PEOP L E 5
KAPITELHUVUD
Authors
Sven Andreasson Harold Holder
Karolinska Institutet, Department of Senior Scientist Emeritus and former
Public Health Sciences, Stockholm, Director of Prevention Research
Sweden Center, Pacific Institute for Research
and Evaluation, Berkely, CA, USA
Tanya Chikritzhs Timothy Naimi
Curtin University, National Drug Boston Medical Center, Section on
Research Institute, Perth, Australia General Internal Medicine, Boston,
MA, USA
Frida Dangardt Tim Stockwell
Sahlgrenska Academy and University Dept of Psychology, Canadian Institute
Hospital, The Queen Silvia Children´s for Substance Use Research, University
Hospital – Paediatric Clinical of Victoria, BC, Canada
Physiology, Gothenburg, Sweden
6 A L C O H O L A N D O L D E R PEO PLE
1 INTRODUCTION
1 Alcohol and older people
– an introduction
The average age of the world population is ipalities and counties has substantially in-
rising. It is expected that the percentage of creased along with higher medical care costs,
the world’s population over 60 years of age constituting a greater challenge for health
will double by 2050.1 Within Sweden the pop- care and social services.2
ulation older than 65 is expected to rise from Against this backdrop of increasing
1.9 million in 2015 to 2.4 million in 2030, a numbers of older people in Sweden requir-
26% increase.2 Swedish life expectancy has ing more health services, the use of alcohol
increased by 2.5 years, to 82.2 years, between among older people also calls for special at-
2000 and 2015 with women at the age of 65 tention. While alcohol consumption mostly is
expected to live 21.5 years longer and men at a lower level than among younger genera-
18.9 years longer.3 tions, this still is of special concern, given the
As a natural consequence of aging, the growing susceptibility of older people to both
human body becomes more vulnerable to the acute and chronic effects of alcohol.
disease. Furthermore, sight, hearing and The purpose of this report is to review the
cognitive processing all decline. Older people health and social effects of alcohol among
have a higher risk of disability and death older persons generally, and in Sweden in
from all major diseases, such as heart disease, particular. By ‘older’ persons, we are broadly
stroke, chronic respiratory disorders, cancer referring to those aged 55 years and older,
and dementia. With increased longevity, cer- although we have a particular focus on those
tain diseases have increased considerably. For aged 65 or older, which is the more conven-
example, new cases of cancers in the 65 to 85 tional definition of the onset of old age. In
year group more than doubled between 1970 addition, for conditions that predominantly
and 2016. Expressed as new cancer cases affect older persons (e.g., stroke) we draw on
per 100 000, cancer incidence has increased studies of the general population. In this re-
almost 50%.4 port we discuss alcohol use and alcohol-relat-
In addition to chronic illness and health ed mortality outcomes among older persons
issues the incidence of acute harm among in the Swedish population, describe the physi-
older age groups has increased. 5 Acute harms ologic effects of alcohol on older persons,
include falls and other unexpected accidents, describe relationships between alcohol con-
violence and mistreatment.Thus, on average, sumption and a variety of health outcomes in
the personal risk of mortality and morbidity older persons, outline the implications of this
rises as a person ages. In Sweden, even as increased susceptibility to alcohol’s effects
mortality has decreased among the older age among older people, describe prevention and
groups, years lived with disease has increased policy responses, and make recommendations
in absolute numbers.5 As a result, the number for low-risk drinking for older persons who
of older people receiving care from munic- consume alcohol.
ALCOH OL AND OLDER PEOP L E 7
KAPITELHUVUD
2 Increased susceptibility
Physiological changes due to ageing result in illness or injury when even relatively small
older people becoming increasingly suscepti- amounts are consumed.
ble to both the acute and longer term effects Ageing is usually associated with a reduced
of alcohol consumption. These physiological capacity of the liver to metabolise alcohol,
changes include reduced muscle mass and re- due to reduced activity of the enzyme alcohol
duced water in the body to dilute the damag- dehydrogenase, which breaks down alcohol.
ing effects of alcohol on human tissue. These This does not affect blood alcohol levels to the
changes that occur in the older body result in same extent as the changes in muscle mass
higher and longer lasting blood alcohol con- however.
centrations (BACs) than would occur for the
same quantity of ethanol intake by younger 2.2 Impacts on stress hormones
drinkers. Exposure to alcohol activates the hypotha-
lamic-pituitary-adrenal (HPA) system, result-
2.1 Reduced body water ing in increased levels of cortisol in a dose-re-
With increased age muscle mass is reduced. sponse manner.6 Cortisol is recognized as the
Since muscle is largely constituted of water main stress hormone and, when chronically
and alcohol is mainly water soluble, there elevated, creates negative metabolic effects
is less water for alcohol to be distributed in, such as hypertension, diabetes, osteoporo-
leading to higher BACs when drinking, and sis and increased susceptibility to infection.
also increased exposure to acetaldehyde, Increased levels of cortisol are also associated
a highly toxic and carcinogenic substance with some neuropsychological disorders,
produced in the body when alcohol is me- including depression and Alzheimer’s disease,
tabolised. The tendency for older people to although it remains unclear whether these
experience higher BACs from a fixed dose are causal associations. Thus, alcohol induced
of alcohol increases with advancing age and exposure to cortisol results in decreased effi-
can be responsible for increasing the risks of ciency and resiliency of physiological function
8 A L C O H O L A N D O L D E R PEO PLE
2 INCREASED SUSCEPTIBILITY
80%
in many organs and an acceleration of the effects are drowsiness, memory impairment,
aging process. Given the increased blood alco- confusion and impaired muscle control with
hol levels from drinking in old age compared increased risk of falls. All these side effects
to younger ages, these effects are especially are compounded by alcohol. Another com-
pronounced among the elderly. mon class of drugs used by elderly include
anticoagulants (blood thinning agents) such
2.3 Interactions with medication as warfarin or newer medications such as Eighty per cent of all
Improper use of medications is estimated to direct thrombin inhibitors. The metabolism of people above 65 years
cause 10 – 15 per cent of all hospitalizations warfarin can be affected by alcohol and may of age in Sweden have
in Sweden. Taking medications along with cause bleeding. Alcohol induced liver disease at least one medication
alcohol does not usually have a significant im- can also affect the effectiveness of medica- prescribed. Alcohol
pact on alcohol metabolism or blood alcohol tions used to thin the blood, thereby increas- can interact with many
levels. Alcohol consumption can, however, ing bleeding risk. Finally, alcohol use may types of medication and
exert strong effects on the effectiveness and increase the risk of peptic ulcer disease or increase the risk of side
action of medications. Eighty per cent of all gastritis and may increase the risk of bleeding effects through a variety
people above 65 years of age in Sweden have for those on aspirin therapy. of mechanisms.
at least one medication prescribed. Alcohol As older people are prescribed more and
can interact with many types of medication more medications, these problems have in-
and increase the risk of side effects through a creased over time. There is a comprehensive
variety of mechanisms. Examples of medica- scientific literature dealing with medication
tions that may interact with alcohol include effects among the elderly, but the role of alco-
those used for the treatment of hypertension, hol is rarely noted in clinical guidelines. This
mood disorders (e.g. anxiety and depression), despite the fact that alcohol is the single most
insomnia and pain.7 Alcohol may also reduce commonly used drug among older people,
the effectiveness of a wide variety of pre- and that negative effects may occur even at
scribed medicines. quite low levels of alcohol consumption.
Interactions of alcohol with other sedative
drugs such as strong painkillers (opioids) 2.4 Social relations
and antianxiety drugs like benzodiazepines A number of social and lifestyle factors may
can be particularly dangerous as they can contribute to potentially hazardous drinking
both increase sedative effects and can change among the elderly. Most important among
blood pressure either upwards or downwards. these appear to be improved purchasing pow-
In extreme cases, alcohol increases the risk er compared to previous generations, smaller
of fatal and non-fatal overdoses from opioid social networks and stressful life events
drugs, an increasingly common concern. such as loss of a spouse. Increasing social
There is evidence that even small quantities acceptance of drinking among older women
of alcohol reduce tolerance to the effects of also plays an important role. Depression and
strong painkillers and so increases risk of increased risk of suicide are quite common
overdose. among elderly people. While depression can
When alcohol is combined with drugs lead to increased use of alcohol, this in turn
used to treat hypertension this can result in can worsen depressed mood over the longer
sudden and potentially serious drops in blood term and increase risk of acting on suicidal
pressure. Alcohol use can also directly impact thoughts.8
the ability to maintain blood pressure when Retirement can be associated with in-
standing upright after sitting, a problem that creased alcohol consumption and/or prob-
is anyway exacerbated with age and leads to lems. This may result from having high
increased risk of falls and other injuries. pre-retirement job satisfaction and enforced
Antidepressant drugs are commonly retirement.9
prescribed to older people. Common side
ALCOH OL AND OLDER PEOP L E 93 HEALTH RISKS
3 Health risks, acute
and chronic
Risk from alcohol-related harms can be cate- population are enhanced with the consump-
gorized as those arising from chronic expo- tion of alcohol. In short, even drinking low
sure over time (e.g., liver cirrhosis) or those amounts of alcohol can add to the health and
stemming from acute impairment (with or safety risks already present during later life.
without symptoms of acute intoxication, e.g., While a relatively small percentage of
motor vehicle crashes). Although many think health and safety outcomes can be attribut-
of alcohol-related conditions as being caused ed to genetic factors, the greater majority of
by heavy drinking or drinking to the point of health and safety determinants in older age
severe intoxication, there has been a growing are problems which could be prevented or de-
recognition that lower levels of consumption, layed by healthy lifestyle in younger years but
either in aggregate or a per-occasion basis, also with advancing age.10 This means that
can cause health and social problems. the overall quality of life for older persons can
be shaped by the physical and social environ-
ments in which they live.
Even drinking low amounts Since many of the health and safety
of alcohol can add to the conditions that occur during older ages are
health and safety risks already preventable, environmental strategies for the
prevention of disease and declines in capacity
present during later life. are important. As with the general popula-
tion, the most effective environmental strat-
This is particularly the case among older egies to reduce alcohol consumption include
people. Alcohol consumption at relatively low public policies such as increasing the price of
doses among the elderly is associated with alcohol (e.g., increased alcohol taxation and
health problems including atrial fibrillation, minimum pricing) and reducing the physical
a number of gastrointestinal disorders and availability of alcohol (e.g., limiting the num-
some cancers. In addition, alcohol consump- ber of outlets, restricting permissible hours
tion can cause declines in cognitive processes, of sale). Health promotion recommendations
reflexes in response to dangerous situations for preventing non-communicable diseases
such as driving, walking and swimming, as among older persons include increased phys-
well as decrements in other skill-based behav- ical activity, good nutrition, increased social
iors. Therefore, the inherent increased risks engagement, and reduced use of tobacco and
of chronic and acute harms among the older alcohol.
10 A L CO H O L A N D O L D ER PEO PLEKAPITELHUVUD
4 Trends in alcohol
consumption and related
harms in Sweden
Alcohol consumption across different age also provides further evidence that regular
groups shows some consistent patterns in alcohol consumption in later life may be an
countries from many regions of the world. indicator of good health rather than a cause of
Of particular interest here, is the tendency good health. This limits the interpretation of
evident in both Sweden and many other studies linking level of alcohol consumption
countries for older people to reduce their to health outcomes among older people, as
consumption, especially as they become less discussed throughout his report.
healthy and frail. For example, a major Eng- In Sweden data on self-reported alcohol
lish study of the ageing process following up consumption are found in the ongoing Mon-
a large cohort over time confirmed a pattern itor study12 and the Swedish National Public
of reduced alcohol consumption with age. Health Survey.13 Figure 1 compares trends in
However, among older people, this decline average consumption of different age groups
was less and sometimes consumption even using data from the most recent Monitor
increased among both men and women with report. As shown in Figure 1, younger and
higher income and education.11 This study middle-aged Swedish people are now drink-
ALCOH OL AND OLDER PEOPLE 114 TRENDS
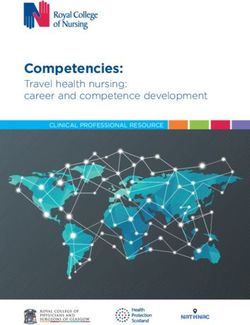
FIGURE 1 Self-reported alcohol consumption liters 100 % alcohol per year in Sweden,
per age group 2004 – 2017
7
6
5
4
3
17 – 29 years
2
30 – 49 years
1
50 – 64 years
0
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
65 – 84 years
Source: Monitor study, from appendix to Befolkningens självrapporterade alkoholvanor 2004 – 2017 (Self-reported alcohol con-
sumption in Sweden 2004 – 2017), CAN report 173, 2018. Upper age limit 80 years before 2014.
ing less on average than they were in 2004. in response to their increased susceptibility to
However, this trend is not evident among its effects.
older people and, while there is some varia- On the surface this reduction in drinking
tion across the years, there has actually been with increasing age suggests a contradiction
an overall increase in consumption among in concerns about alcohol-related health and
people aged between 65 and 84 years since safety risks among the elderly, since people
2004. It is important to note that these data typically drink less in general as they get
are based on self-report surveys and that the older. That is alcohol-related risks would ap-
average levels of consumption reported across pear to be less for the older population based
all age groups are significantly lower than upon alcohol consumption alone. However,
the level of actual consumption of alcohol in even if there is a decline, on the average, for
Sweden when estimated from official alcohol alcohol consumption with increased age,
sales. While the 65 years and older age group the naturally increased risks for health and
in this survey has consistently consumed less safety problems associated with aging are
than the younger age groups, with an estimat- added to any increased risk associated with
ed consumption of 3.3 litres of pure alcohol drinking. In short, the risks of alcohol-related
per person per year compared with 4.5 litres problems, even if lower than for younger age
for those under 30 years of age, both of these groups, can increase overall health and safety
estimates are less than half the actual con- risks associated with aging.
sumption of the population. It is noteworthy A study of changes in drinking habits of
that while older people on average consume Swedish people over the decades found that
a little less than their younger counterparts, there were substantial increases in the per-
this difference has been decreasing over the centage of 75-year-olds drinking at hazardous
years and, as discussed in the present report, levels in 2005/2006 compared with almost
is at least partly counteracted by an increased 40 years ago, in 1976-1977. Among women,
susceptibility to alcohol’s effects among older hazardous drinkers increased from less than
people. Indeed, the reduced consumption of 1% to 10% of the population. Among men this
alcohol by older people is likely at least partly proportion increased from 19 to 27%.14
12 A L CO H O L A N D O L D ER PEO PLE4 TRENDS
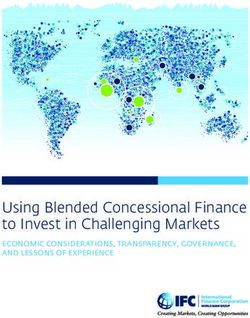
As further evidence of increasing consump- for deaths and years lived with a disability
tion and related harms, there has been a 30% specifically from liver cancer and also vio-
increase in the rate of alcohol caused deaths lence. For example, among those age 65 to
of all kinds between 2000 and 2016. The rate 69, years lived with cancer (YLD) increased
of increase for alcohol-related liver disease by 17% per hundred thousand people and by
has been particularly dramatic having in- 4% for those aged over 70. Years of life lived
creased over this period by more than 100%.15 with a disability due to violence increased
While there have been some variations by between 6 and 7% for those aged 65 years
upwards and downwards over this time pe- and above.5 These are two outcomes highly
riod, there have also been significant overall associated with alcohol use.
increases in Sweden between 2000 and 2016
FIGURE 2 Deaths per 100,000, alcohol index (diagnoses 100 % attributed to alcohol
consumption), ages 65 – 85+, 2000 – 2016, both sexes
60
50
40
30
20
10
0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Source: Swedish National Board of Health and Welfare, Statistical Database, 2018-08-13
FIGURE 3 Deaths per 100,000, alcoholic liver disease, ages 65-85+, 2000-2016, both sexes
12
10
8
6
4
2
0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Source: Swedish National Board of Health and Welfare, Statistical Database, 2018-08-14
ALCOH OL AND OLDER PEOPLE 135 RISKS
5 Methodological
considerations: How do
we determine risks for
older drinkers?
5.1 Assessing Associations and remove a risk factor in which actual drinking
Causation amounts are carefully measured over time
including a control group for non-drinking.
Various research approaches have been
In practice, it is often practically and ethically
used to study the potential contribution or
challenging to conduct an RCT on a risk
even a causal relationship of alcohol to the
factor for disease like alcohol consumption.
health and safety of older people. A common
For example, a planned RCT to investigate
task when assessing the extent of alcohol’s
whether moderate alcohol use was protective
contribution to different health outcomes is
Some of these to apply the main criteria for causation in the
against heart disease had a budget of US$100
million and would have required many
apparent science of epidemiology i.e. the study of the thousands of people to be randomised to
protective spread of illnesses in populations. The two
major criteria are (i) biological plausibility
either abstain from drinking or drink a small
quantity each day over several years.17 In fact,
effects do not e.g. evidence from experimental laboratory this study was closed down due to ethical and
have biological studies identifying mechanisms of harm (or scientific concerns about its design and undue
benefit) from alcohol’s impact on human
plausibility. functioning, and (ii) evidence of increased
alcohol industry influence.18, 19
A research design frequently used in
risk of an illness or injury associated with the epidemiological research is the study of self-
amount of alcohol an individual consumes reported alcohol consumption by participants
– often referred to as evidence of a ‘dose-re- later linked to health or safety outcomes
sponse’ relationship.16 Neither criteria is suffi- identified in official health archives. These
cient on its own: biological plausibility which “observational” cohort studies have a number
supports the potential of alcohol effects does of threats to validity including: selection bias
not guarantee a significant impact on health arising from study participants essentially
outcomes in practice as factors other than self-selecting themselves into drinker and
alcohol consumption can come into play. non-drinker groups; recall bias about drink-
Our confidence is increased in a causal ing which may become worse over time; and
association if there is evidence from well con- under reporting of major changes in drinking
ducted randomised controlled trials (RCTs) levels and patterns which can impact health
of interventions that experimentally add or outcomes.
14 A L CO H O L A N D O L D ER PEO PLEKAPITELHUVUD
The majority of observational studies of their consumption for health reasons.21, 22
older people’s alcohol use and risk of future Secondly, there is evidence that young adults
illness or death find some evidence of protec- who are lifetime abstainers are more likely
tive effects for people who drink moderately to be disabled, have poor health and low
in comparison with those who abstain. Some income.23, 24 Studies comparing abstainers
of these apparent protective effects do not and moderate drinkers also find they differ on
have biological plausibility. For example, a a range of lifestyle and personal characteris-
review by Fekjaer (2013)20 found reduced risk tics unrelated to their drinking which placed
among moderate drinkers for such implau- them at differential risk of ill-health e.g.
sible conditions as deafness, some cancers, bodyweight, nutrition and exercise (Naimi,
liver disease and the common cold. It is hard 1995).25 There are many “observational” stud-
to explain how such protection is biologically ies linking some exposure to a risk factor for
possible. Instead, it is more plausible to sup- a disease that have been subsequently refuted
pose that important biases exist in many such by RCTs (e.g., hormone replacement therapy
studies that create the appearance of health and reduced risk for heart disease).
protection. Firstly, many older people who Naimi et al (2017)26 have shown how biases
identify as abstainers in these observational in long term follow up studies can accumulate
studies were drinkers who quit or reduced with increasing age resulting in the health
ALCOH OL AND OLDER PEOPLE 155 RISKS
profiles of abstainers being increasingly neg- randomisation studies that relate to alcohol’s
ative and those of drinkers increasingly posi- effect on health. Both of these types of studies
tive. Furthermore, systematic biases towards are less likely to suffer from bias and con-
continuing drinkers appearing healthier than founding than the more frequently conducted
abstainers will be most pronounced among observational design studies (i.e. prospective
older people. Such systematic selection bias cohort, case-control, case-crossover). In addi-
over the life course is also supported by a tion, animal studies often have strong experi-
meta-analysis of all studies on alcohol use mental designs and can assess alcohol-related
and all-cause mortality by Stockwell et al. exposures that might be considered too risky
(2016).27 It was also found in another me- or unethical in human subjects.
ta-analysis by the same authors that evidence
for a J-shaped curve or protection from 5.2 Identifying and Prioritizing
moderate drinking against coronary heart Studies for this Report
disease mortality was only present in studies In preparing this report we set out to summa-
of older cohorts for whom there should be rise key findings and then draw conclusions
most accumulated bias (people aged over 55 from a very large research literature concern-
years at intake). Younger cohorts followed up ing alcohol’s effects on physical and mental
to old age showed no evidence of cardio-pro- health as well as safety. There are many thou-
tection from moderate drinking.28 In many sands of published studies in this area cover-
ways regular “moderate” drinking may be a ing different aspects and health conditions.
sign but not a cause of good health. In order to make sense of this complexity,
One longitudinal study design, referred to and distil what can be learned, we searched
as Mendelian randomisation or genetic ran- for the most representative and authoritative
domization, is however thought to minimise studies by prioritising a) recent comprehen-
confounding and reverse causation and be sive and systematic reviews b) major recent
related to lifetime alcohol exposure. This de- studies from official national and internation-
sign is applied in studies that identify genetic al sources c) high-quality studies with strong
characteristics which are randomly present designs and d) studies of particular relevance
in individuals in a way that is not influenced to Sweden and Scandinavia. As academic
by upbringing and environment. Mendelian researchers who have contributed to the fields
randomisation is the basis for studies that of alcohol epidemiology and policy, we also
compare the risk of disease between individu- took account of well-known systematic biases
als with different genetic profiles (e.g. Holmes and methodological problems in these litera-
et al., 2014).29 Where available we will refer tures in drawing our conclusions.
to evidence from both RCTs and Mendelian
16 A L CO H O L A N D O L D ER PEO PLE6 IMPACT OF ALCOHOL
6 Impact of alcohol on
death, disease, injury
and disability
6.1 Total mortality
More than 60 conditions have been identified
as either partially or entirely caused by expo-
sure to alcohol.30 There is no doubt that alco-
hol is a major preventable cause of premature
mortality for all ages. Increased risk of death
is not limited to high levels of consump-
In recent years, with the emergence of novel
research approaches that substantially reduce
potential for confounding and bias compared
to traditional observational study designs
(i.e. Mendelian randomization studies),
long-standing doubts about the veracity of
J-shaped curves for alcohol have been rein-
forced.34 Mendelian randomization studies
60
More than 60 conditions
have been identified as
tion and in fact low level drinking has been
for instance suggest no protective effect for either partially or entirely
identified as a major cause of excess mor-
low-dose consumption and coronary heart caused by exposure
tality arising from a range of alcohol-related
disease events.29 This is important because to alcohol. There is no
cancers. Past meta-analyses of the observa-
the apparent protective effects for low-volume doubt that alcohol is a
tional studies which dominate this literature
consumption on total mortality are due to major preventable cause
have nevertheless shown J-shaped curves for
observed protective effects on coronary heart of premature mortality
all-cause mortality with beneficial effects at
disease, so the veracity of the J-shaped curve for all ages.
low doses. Interestingly, these studies also
and protective associations for low-volume
suggest that the level at which maximum
consumption for all-cause mortality remains
potential benefit may be achieved is probably
in doubt. However, based on observational
less than 10 grams of ethanol per day and for
study data, across the general population,
women may be as low as 5 grams a day (e.g.
including for older persons when assessed,
Bagnardi et al 200431). In fact, the latest, and
the lowest risk of death is generally found
largest, report on this subject, from the Glob-
among those drinking less than 10 grams of
al Burden of Disease project, finds that the
ethanol daily.27, 35–39 Furthermore, a Mendeli-
safest consumption level is 0.30 What is more,
an randomization study of older persons finds
social and economic cost studies based on the
reduced all-cause mortality with a genetic
supposition that health benefits from alcohol
variant associated with less alcohol consump-
exist, show that the total social and economic
tion.40
costs of harms from alcohol still outweigh the
sum of the benefits.32, 33
ALCOH OL AND OLDER PEOPLE 176 IMPACT OF ALCOHOL
6.2 Cardiovascular diseases and to be greater for relatively older persons com-
diabetes pared with the general population.28, 41 How-
ever, the concern is that older ages would also
Coronary heart disease, stroke, hyperten-
tend to magnify sources of bias including the
sion and diabetes are all more prevalent
‘sick quitter’ phenomenon and the ‘healthy
among older people, and so studies of these
survivor’ bias, and protective effects attenuate
outcomes among the general population
when attempting to account for these biases.28
are relevant to those in later life, even if the
In addition, Mendelian randomization studies
cohorts used in those studies are sometimes
find no protective effect for low-volume
not restricted to older people. Both congestive
alcohol on coronary heart disease events or
heart failure (associated with heavy consump-
coronary calcification. 29, 42, 43
tion) and atrial fibrillation (associated with
While randomized trials of the Mediter-
any consumption) are for example far more
ranean diet find protective effects for the
common among older individuals but will not
primary and secondary prevention of CHD
be discussed in detail in this report.
outcomes44, 45, those trials were not rand-
There has been no randomized study of
omized with respect to alcohol consumption.
low-volume alcohol consumption and any
Although these latter findings do not pre-
morbidity or mortality outcome related to
clude protective effects of low-dose alcohol
coronary heart disease. Excessive alcohol con-
consumption, they mean that the apparent
sumption, including heavy average consump-
benefits of a Mediterranean diet (i.e. one
tion and binge drinking, are risk factors for
in which the moderate use of alcohol is one
coronary heart disease, stroke, hypertension
small part) may be explained by factors other
and the development of diabetes or to poor
than alcohol consumption.
diabetes control.
Strokes may either be ischemic (in which
In terms of low-dose or “moderate” con-
blood flow is blocked or reduced to a por-
sumption, most observational studies find
tion of the brain) or hemorrhagic (in which
protective effects for coronary heart disease.
a blood vessel bursts, interrupting flow and
Furthermore, protective associations appear
also sometimes creating pressure on sur-
rounding brain tissue); ischemic are the most
prevalent of the two. In observational studies,
high-volume consumption is a risk factor
for both stroke types. Low volume alcohol
consumption appears protective for ischemic
(but not hemorrhagic) strokes among both
men and women, though at lower levels for
men (less than one drink per day) than for
women (about one drink per day).46, 47 A re-
cent well-designed and large study questions
whether even light drinking protects against
ischemic stroke39 while a Mendelian randomi-
zation study finds no protection from having a
gene related to reduced alcohol consumption
on all strokes.29
For hypertension, in itself an important
risk factor for cardiovascular disease and
mortality, most but not all observational
studies find a positive relationship between
alcohol consumption and both higher blood
pressure and incident hypertension across
18 A L CO H O L A N D O L D ER PEO PLE6 IMPACT OF ALCOHOL
all levels of consumption, particularly among dence that heavy alcohol use is responsible
men.48 Furthermore, a meta-analysis finds for worse outcomes and increased risks for
that reductions in alcohol consumption are cardiovascular diseases and diabetes. In par-
associated with reductions in blood pres- ticular, studies of hypertension, a major risk
sure.49 A meta-analysis of Mendelian rand- factor for cardiovascular disease, find only
omization studies also finds positive rela- negative impacts from the consumption of
tionships between alcohol consumption with alcohol even at low doses. In better designed
increased blood pressure and hypertension studies there is little or no evidence of pro-
among men.50 tective effects for low-dose alcohol, especially
In terms of blood glucose and diabetes, ob- for men. Furthermore, genetic studies using
servational studies generally find a protective Mendelian randomisation have found no
effect of alcohol consumption (e.g. 51, 52), with evidence of protective effects from low-dose
the lowest level of risk among those consum- alcohol use on cardiovascular disease or dia-
ing about one drink daily. However, sex strat- betes for either men or women.
ified results find significant protective effects
only among women53 and even these may be
questioned as there are relatively few well de- Alcohol has been classified by the
signed studies of women. Moreover, in anal- World Health Organisation as a
yses restricted to trials with a never-drinking
comparison group (as opposed to all non-cur-
Group 1 carcinogen since 1988
rent drinkers), alcohol was not associated
with any protective effects for either women
or men.53 Mendelian randomization studies 6.3 Cancer
also find no significant protective effect of Advancing age is the leading risk factor for
alcohol consumption on diabetes.29, 54, 55 Fi- incident cancer and for cancer mortality, and
nally, a meta-analysis of randomized clinical those over age 65 account for approximately
trials finds no protective effect of low-volume 70% of all cancer deaths. Increased cancer
alcohol consumption on blood glucose control susceptibility among older persons is likely
among those with diabetes.56 due to a combination of reduced cellular
In experimental studies, alcohol adminis- mechanisms (e.g., DNA repair mechanisms)
tration raises HDL cholesterol levels. Howev- and an accumulation of carcinogenic damage
er, a Mendelian randomization study found from environmental exposures over the life
no cardio-protection for those carrying a gene course (e.g., tobacco, alcohol).61 In addition,
variant that raises HDL. Furthermore, after cancer treatment options may be limited or
controlling for their effects on LDL, rand- less desirable on the basis of age (e.g., stem
omized studies of statin drugs have not found cell transplants, aggressive surgical debulk-
a significant relationship between changes ing), or available treatments may have greater
in HDL and coronary heart disease. Final- relative toxicities than among relatively
ly, several drugs that effectively raise HDL younger persons.
have not resulted in reduced coronary heart Alcohol has been classified by the World
disease events in clinical trials. For these Health Organisation as a Group 1 carcinogen
reasons, although HDL is associated with car- since 1988 when it was concluded that there
diac outcomes it is not likely causal for heart was sufficient evidence for its causal role in
disease.57–59 Alcohol consumption does not cancers of the oral cavity, pharynx, larynx,
appear to meaningfully affect levels of LDL esophagus and liver. Since that time, several
(bad) cholesterol.60 hundred more epidemiological studies have
In summary, taking account of studies reported on the association between the con-
of biological plausibility and studies with sumption of alcoholic beverages and the risk
stronger designs, there is considerable evi- for cancer at various sites. In 2007, the IARC
ALCOH OL AND OLDER PEOPLE 196 IMPACT OF ALCOHOL
added cancers of the female breast, colon and dementia attributable to alcohol is now recog-
rectum to the list of cancers caused by alcohol nized as much larger than previously thought.
(IARC, 2007).62 World Cancer Research Heavy drinking is strongly associated with the
Fund (2016)63 more recently concluded that development of Alzheimer’s disease. Alcohol
stomach cancer also was causally related to use disorder is the strongest modifiable risk
alcohol consumption. There is also accumu- factor for dementia onset and is associated
lating evidence for causal association between with all other independent risk factors for
alcohol use and both prostate and pancreatic dementia onset.69
cancers.64–66 The areas of cognitive decline and dementia
The increased risk of these cancers is are areas of particular concern for older per-
normally found to be increased even for light sons, and have been increasing in developed
or moderate drinkers with no safe level of nations worldwide. Although it is clear that
consumption (e.g. 64). However, the ap- heavy drinking can cause alcoholic dementia,
pearance of a protective effect does occur in the effects of low-volume consumption on
some studies, likely due to the same kinds dementia, including Alzheimer’s dementia,
571
of confounding factors described earlier in are more controversial. Summarizing the liter-
relation to the apparent J-shaped curve for ature on the effects of low volume drinking on
alcohol and mortality generally. Most studies cognition, four lines of research are consid-
of alcohol and cancer outcomes suffer from ered. One of these supports protective effects
the same kinds of systematic bias discussed for cognitive impairment while the other three
earlier in particular relation to cardiovascu- do not. In the first, the observational studies,
lar disease. In one meta-analysis of prostate a majority of studies find J-shaped curves,
cancer, it was found that when former drinker where low-volume drinking appears protec-
bias was corrected the estimated risk for tive of dementia (e.g. 70). While most of these
For Swedish people 65+
moderate drinkers increased from 8% to studies find a J- or U-shaped curve for alcohol
and older we estimated
22%.66 This means that the increased risk of consumption and the risk of dementia, some
571 deaths attributable
cancers from alcohol consumption are likely have investigated the effects of the apolipo-
to alcohol in 2014 for the
underestimated when based on meta-analysis protein e4 allele, where they find that carriers
seven cancers currently
of the existing literature. of this allele have an increased risk of demen-
deemed by WHO to be
In one of our previous reports67, we applied tia with increasing alcohol consumption.71
caused by alcohol.
the latest methods used internationally to Nearly every review of observational (i.e.,
quantify the burden of cancers attributable to non-randomized) studies however describes
alcohol in Sweden.68 For Swedish people 65+ methodological problems of underlying
and older we estimated 571 deaths attribut- studies, such as under-representation of heavy
able to alcohol in 2014 for the seven cancers drinkers in population-based cohorts; incon-
currently deemed by WHO to be caused by sistent measurement of alcohol use or demen-
alcohol. This is likely to be a substantial un- tia, or both; insufficient control of potential
derestimate as there are likely more cancers confounders; and insufficient consideration of
than these causally related to alcohol use and sample attrition in patients with alcohol use
the risk estimates derived from the existing disorders.
literature are themselves likely to be underes- In the second, the structural studies con-
timated. sistently report increased rates of atrophy of
the brain, and especially the hippocampus (an
6.4 Cognitive function area of the brain associated with memory), at
Alcohol is recognized as a powerful neuro- all levels of drinking including relatively low
toxin, known to cause or contribute to a wide levels.72 In the third, the Mendelian random-
range of neurological disorders including ization studies, the outcomes are mixed, but
dementia and fetal alcohol syndrome, among overall there is no evidence for protective ef-
many others. Furthermore, the burden of fects from moderate drinking.73 In the fourth,
20 A L CO H O L A N D O L D ER PEO PLEKAPITELHUVUD
the animal studies, of which some have the consumption and dementia, found a J-shaped
advantage of having an experimental design risk curve in which low-volume drinking ap-
with controls, all levels of alcohol consump- peared to be protective for dementia.77 On the
tion appear to be harmful to the brain and other hand, the Whitehall II imaging study
cognitive function.74 found increased odds of hippocampal atrophy
Some research has shown a relation- in a dose dependent fashion, with increased
ship between the development of cognitive risk starting at low levels of consumption.78
impairment and lifestyle-related risk factors A recent Swedish study, based on the
that are shared with other non-communicable Swedish twin registry adds to the growing
diseases. These risk factors include physical body of research in which all levels of alcohol
inactivity, obesity, unbalanced diets, tobac- consumption appear detrimental to cognitive
co use and harmful use of alcohol as well as function.79 The study used information from a
diabetes mellitus and mid-life hypertension. sample of people in the Swedish Twin Regis-
Other potentially modifiable risk factors try, who in their midlife (1967) participated in
more specific to dementia include mid-life a survey on alcohol intake and 25 years later
depression, low educational attainment, participated in a longitudinal study on cog-
social isolation and cognitive inactivity.75 A nitive aging. This study showed that alcohol
randomized study of the Mediterranean diet intake was related to lower cognitive perfor-
showed protective effects for the development mance in a dose-response manner, starting at
of dementia; however, the study was not ran- low levels.
domized with respect to alcohol consumption
and so the results were inconclusive.76 6.5 Injury
The scientific controversy is illustrated Injuries may result from a wide range of ex-
by conflicting evidence from the Whitehall ternal causes such as road crashes, falls, near
II study. On the one hand, an observational drowning, burns, or violence. Here we have
study on the Whitehall II cohort, on alcohol considered the research evidence for three
ALCOH OL AND OLDER PEOPLE 216 IMPACT OF ALCOHOL
major forms of injury, road crashes, falls scientific papers published between 2003 and
and physical/psychological abuse. Several 2013.88 The U.S. Centers for Disease Control
meta-analyses find significant associations in reviewing national crash records for all
between alcohol use and risk of injury within of the U.S. found that involvement in fatal
six hours of drinking compared to abstainers crashes per mile travelled begins increasing
for all ages.80–82 For older drinkers specifi- among drivers ages 70 – 74 years and are
cally, risk of injury is also likely to be higher highest among drivers aged 85 and older in
immediately after alcohol exposure but may the U.S. This later trend has been attributed
also be compounded by the onset of physio- more to an increased susceptibility to injury
logical changes that occur with aging includ- and medical complications among older
ing reduced bone density, decline in balance, drivers rather than an increased risk of crash
coordination and reaction time, vision and involvement.89
hearing problems and medication use.83 While driving and drinking alcohol increas-
es crash risk for all ages, there is evidence
that older drivers have higher risk of crashes
There is evidence that older than younger drivers at the same BAC levels.
drivers have higher risk of This has been confirmed by one controlled
laboratory study of driving simulation in
crashes than younger drivers which participants were given alcohol prior
at the same BAC levels. to the simulation. The study found in general
that older adults performed more poorly with
driving precision and impairment as a result
6.6 Road crashes of alcohol consumption measured by steering
It is well established that in relation to motor rate and the ability to maintain a constant
vehicle injury, alcohol use, even at relatively speed than younger drivers. The study also
low levels, is a risk factor for drivers of all found that one serving of alcohol was enough
ages.84, 85 Road crashes are of concern in most to affect seniors’ driving abilities in contrast
industrialized societies and as increased to younger age groups with the same level
wealth increases the availability of private of alcohol consumption.90 A national study
automobiles for personal transportation, the in the U.S. based upon fatal crash records
risk of traffic crashes and resulting injuries examined BAC levels for drivers and found
and fatalities becomes increasingly serious that among fatal crashes in which drivers had
across the world. Increased wealth also leads BAC levels less than 0.08% there was a much
to increased resources to traffic safety work higher proportion of older drivers compared
which in the longer run decreases the risks for with the youngest aged driver group, despite
road crashes.86 Since safe driving is depend- the latter also being a sub-population at high
ent upon both training and personal driver crash risk.91
skills and ability to operate complex tasks, the In short, not only are older drivers of great-
aging process may affect some older driver er risk of injury and death than all younger
abilities and also increase driving risks due to ages, but this accident risk is increased with
changes in vision and cognitive functioning the consumption of alcohol, even at very low
(ability to reason and remember), as well as dosages. Moreover, there is the addition-
physical changes.87 In 2002, international- al risk of interaction between alcohol and
ly more than 193,000 traffic deaths traffic psychoactive medications taken by the older
were registered among people who were 60 driver. While younger drivers are at greater
years and older. The mortality rate for such risk for crashes at a given BAC, the risk of
accidents for 100,000 persons in this age serious outcomes is greater for older drivers
population was the highest compared to other at similar BAC.
age groups based upon a systematic review of
22 A L CO H O L A N D O L D ER PEO PLE6 IMPACT OF ALCOHOL
6.7 Falls report drinking lower amounts of wine have
a significantly lower risk of falls and hip frac-
For the general population research evidence
ture compared to non-drinkers100, 101 but that
on the association between falls and episodic
risk increases at 2 or more drinks per day.96
alcohol use generally shows a linear dose-re-
However, these observational studies are sub-
sponse relationship such that the more
ject to the same kinds of design limitations
alcohol that is consumed the greater the risk
described in earlier and apparent protective
of falling.81 Older people fall more often than
effects at low doses are likely to be due to
their younger counterparts often as a conse-
uncontrolled confounding and bias.
quence of chronic health conditions, impaired
vision, ear problems, muscle weakness or
6.8 Physical and psychological abuse
possibly medication use. They may also have
of older people
an increased fear of falling as the consequenc-
es can be more serious, long lasting and occur Physical and/or psychological abuse of older
at times and places where they are alone.83 people by others (‘elder abuse’) has gained
One of the few systematic reviews of attention as a significant societal problem in
alcohol’s effect on risk of falling among older more recent years. A large meta-analysis of
drinkers specifically (65+ years) was con- data collected from 28 countries estimated
ducted by Ridolfo and Stevenson (1998).92 that about one in six people aged 60 years or
They noted that one of the problems with older had experienced elder abuse of some
studies in this area is that they often recruit form including psychological, financial, ne-
participants from nursing homes and that glect, physical and sexual.102 Elder abuse may
both self-reported alcohol use and the nature be even higher among vulnerable dementia
of falls among those residing in institutional patients with estimates ranging from about
settings will differ to individuals living in 28% to 52%.103 As average population age
unsupervised situations. People living in res- continues to increase worldwide, the prev-
idential aged care are likely to be more frail, alence of elder abuse is also likely to grow
take more medications and be at higher risk rapidly.
of falling but also less likely to consume sig-
nificant quantities of alcohol. They concluded
that for people aged 65 years and older, acute
intoxication is a cause of 12% of male and 4%
of female falls. These findings matched results
from a recent experimental study showing
that even low level alcohol use adversely
affects postural stability among persons over
65 years, especially among those who already
have poor balance.93
However, some recent studies have pro-
duced mixed findings with some showing no
association at all (e.g. 94) and others showing
a protective effect for falls at low doses (e.g.
95
). Research on hip fracture, osteoporosis
and low bone mass density also suggests that
compared to abstainers, those who regularly
drink small amounts of alcohol (between
0.5 to 1 drink per day) have a lower risk of
developing these conditions.96–99 At least
two studies suggest a J-shaped curve where
older drinkers, particularly women, who
ALCOH OL AND OLDER PEOPLE 23You can also read