AMENORRHOEA FOGSI FOCUS 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

FOGSI
FOCUS
2021
AMENORRHOEA
EDITORS :
DR. ALPESH GANDHI DR. ANITA SINGH
PRESIDENT FOGSI VICE PRESIDENT FOGSI
CO-EDITOR
DR. TRIPTI SINHA
FEDERATION OF OBSTETRIC &
GYNAECOLOGICAL SOCIETIES OF INDIA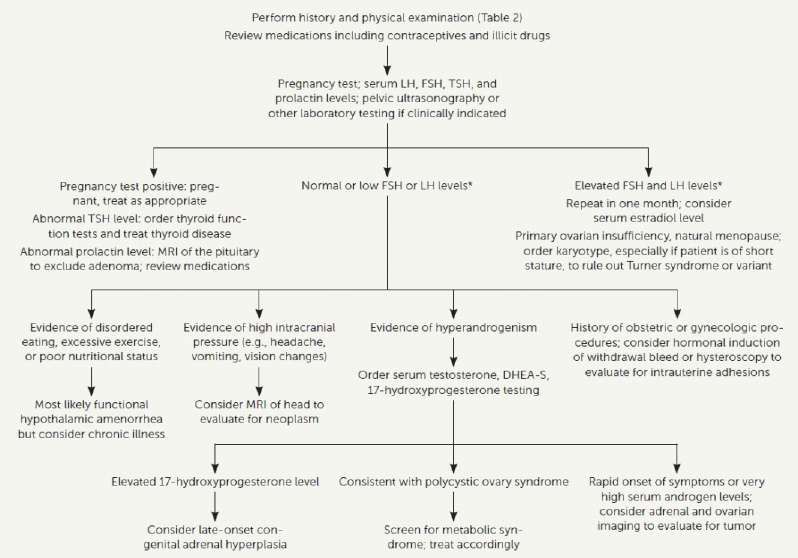
The FOGSI Team
2020
Dr. Alpesh Gandhi Dr. S Shantha Kumari Dr. Nandita Palshetkar Dr. Jaydeep Tank
President President Elect Immediate Past President Secretary General
Dr. Anita Singh Dr. Atul Ganatra Dr. Ramani Devi Dr. Archana Baser Dr. Ragini Agrawal
Vice President Vice President Thirunavukkarasu Vice President Vice President
Vice President
Dr. Madhuri Patel Dr. Suvarna Khadilkar Dr. Parikshit Tank Dr. Sunil Shah
Dy. Secretary General Treasurer Jt. Treasurer Joint Secretary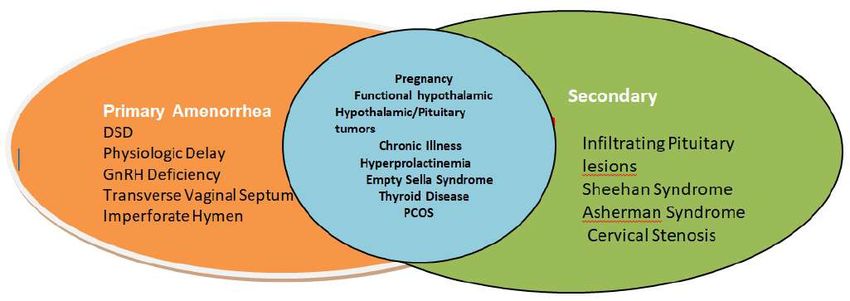
MESSAGE
Dr. S. Shantha Kumari
President Elect
Dear FOGSIANS
It is indeed a formidable and challenging task to don the mantle of the
President of FOGSI and step into the shoes of the stalwarts and doyens who
have brought laurels to FOGSI during their tenure as President. But my
confidence is boosted and gets a fillip since I will be supported by my new team
of office bearers each of whom have righ ully earned their place in our
organisa on.
I would like to congratulate Dr Anita Singh Vice President FOGSI East Zone and
her team of contributors to FOGSI Focus dedicated to the common and o en
perplexing clinical problem of amenorrhea. This issue covers the topic of
amenorrhea from various perspec ves to give a holis c view off this
distressing en ty. Its management o en oversteps the confines of a
gynecologist's domain to ask for solu ons from endocrinologists and imaging
specialists in the quest to ascertain the diagnosis and decide upon a
sa sfactory management protocol for the pa ent ideally individualized for
every pa ent.
Seasoned old me consultants and fresh- in- the -field budding gynaecologists
will fall back on it with relief when hard pressed for me coupled with the
urgency to manage girls and women with amenorrhea in their daily clinical
prac ce.
Happy reading and reflec ng on past experiences of our own encounters with
amenorrhea.
foreword
th
Dear FOGSIANS, 12 June, 2021
It gives me immense pleasure to write this foreword for the FOGSI FOCUS on
'Amenorrhea' which is being edited by our dear and hardworking Dr. Anita Singh,
Vice President FOGSI, 2020 .The en re team of Vice Presidents and chairpersons
working with Dr. Alpesh Gandhi as President FOGSI, 2020 has done very
commendable work, for FOGSI socially, academically and for the fraternity.
The prevalence of amenorrhea is approximately 3,000 to 4,000 per 100,000
individuals worldwide. Amenorrhea can be a very perplexing problem if not
a ended to in an appropriate manner.
The treatment for amenorrhea depends on the underlying cause. So taking a
detailed history, counselling and reassurance of the girl and her parents is a very
essen al part of the management . If primary or secondary amenorrhea is caused by
lifestyle factors, destressing, change of weight and physical ac vity may help . But if
there are cons tu onal factors, congenital factors, endocrinological issues, it needs
a mul disciplinary approach and one must do this at the appropriate me and
systema c manner.
This FOGSI FOCUS covers all aspects of amenorrhea star ng from diagnosis to
treatment . Understanding basic examina on and screening tests would enable
gynecologists to diagnose and treat women.
Hearty Congratula ons to Dr. Anita Singh and her team of authors who have
contributed to this FOGSI FOCUS. We are sure this will be a ready reckoner for
clinicians and facilitate in their diagnosis and management of Amenorrhea.
Prof. Dr. Suchitra N. Pandit
Consultant - Dept.of OBGYN ,Surya group of Hospitals ,Mumbai
President Organisa on Gestosis ( 2016 ll date )
President ISOPARB (2018-20)
Chair AICC RCOG ( 2017-20)
President FOGSI & ICOG ( 2014-15)
preface In con nua on with its well-established tradi on, FOGSI Focus con nues its publica on journey devoted to clinical problems encountered by gynecologists and obstetricians in their pa ent encounters. Amenorrhea is one such front-line problem with far-reaching and over-arching implica ons on a woman's health. In this issue we have compiled inputs of eminent, seasoned clinicians who provide clinical insights into the problems of amenorrhea from various perspec ves. The chapters are listed on the basis of their e ology. Each chapter elaborates on the e o-pathogenesis followed by the clinical presenta on and management op ons available, and which need to be discussed during pa ent counseling. This crisp but comprehensive capsule of informa on between the covers of this issue of FOGSI Focus will come in handy and useful to consultants and post-graduate students alike as they confront a girl or woman who is worried about the absence or cessa on of her menstrual periods. We are grateful to our President Dr Alpesh Gandhi who entrusted this academic task to us and extend our sincere thanks to the contributors in this issue who found me from their busy schedule to send in their write-ups. Dr. Alpesh Gandhi Dr. Anita Singh Dr Trip Sinha

List of Contributors
Dr. Anita Singh Dr. Kusum Lata
MS,DGO, DNB MD, DNB
Vice President, FOGSI (EZ), 2020 Assistant Professor, AIIMS
Ex- Professor, Obs/ Gynae New Delhi
Patna Medical College, Patna
Dr Aswath Kumar Dr Mandakini Pradhan
MD, DGO, FICOG Prof and Head
Professor OBG Department of Maternal and
Jubilee Mission Medical College Reproduc ve Health
Thrissur Sanjay Gandhi Post Graduate
Vice President FOGSI 2019 Ins tute of Medical Sciences,
Na onal Coordinator FOGSI Lucknow
Dr Megha Jayaprakash
Dr. Alka Kriplani MS, DGO, MRCOG
MD, FRCOG, FAMS, FICOG, FICMCH, Associate Professor OBG
FIMSA, FCLS Govt Medical College Thrissur
Director, Department of Minimal
Invasive and ART
Paras Hospitals, Gurgaon
Dr Pra k Tambe
Dr. Duru Shah Chairperson, AMOGS Endocrinology
MD, FRCOG, FICOG, FICS, FCPS, Commi ee (2020-22)
FICMCH, DGO, DFP Governing Council member, ICOG
Director, Gynecworld, the Center for (2021-22)
Women's Health and Fer lity, Chairperson, FOGSI Endocrinology
Mumbai Commi ee (2017-19)
Consultant Gynecologist & Managing Council member, MOGS
Obstetrician, Fer lity Expert and ISAR
Dr Firdousara Siddiqui Dr Suvarna Khadilkar
Resident, Department of Obstetrics Prof & HOD, Department of Obs and
and Gynecology, Bombay Hospital, Gyne, and Consultant Gyne-
Mumbai Endocrinologist, Bombay Hospital
Ins tute of Medical Sciences,
Mumbai
Editor Emeritus JOGI
Treasurer FOGSI
List of Contributors
Dr. Sabahat Rasool Dr Trip Sinha
MD, MRCOG, DNB, FMAS Ass Prof. Obs. Gyn
Obstetrician, Gynecologist and Sri Krishna Medical College,
Fer lity Consultant. Muzaffarpur, Bihar
Lecturer, Government L D Hospital,
Srinagar
Dr. Vandana Bha a
Dr. Sonia Malik MBBS, MD
DGO, MD, FICOG, FIAMS Sr. Consultant
Director & HOD, Southend Fer lity & Southend Fer lity & IVF
IVF, 2,Palam Marg, 2,Palam Marg,
Vasant Vihar, New Delhi Vasant Vihar, New Delhi
Dr. Sunil Shah
Fer lity Expert (Germany)
Joint secretary FOGSI,
Hon. Secretary Ahmedabad.
Past VP., AOGS
Contents
1. Amenorrhea: An Overview .............................................................
Dr. Anita Singh, Dr. Trip Sinha
2. Hypothalamic and Pituitary amenorrhea ......................................
Dr. Suvarna Khadilkar, Dr Firdousara Siddiqui
3. Amenorrhea: Endocrine Issues......................................................
Dr. Pra k Tambe
4. Hyperprolac nemia ....................................................................
Dr. Alka Kriplani, Dr. Kusum Lata
5. Amenorrhea in Polycys c Ovarian Syndrome .................................
Dr. Duru Shah, Dr. Sabahat Rasool
6. Developmental anomalies causing amenorrhea ..............................
Dr. Ashwath Kumar, Dr. Megha Jayaprakash
7. Amenorrhea and Gonadal Dysgenesis ............................................
Dr. Mandakini Pradhan
8. Premature Ovarian Insufficiency ....................................................
Dr. Sonia Malik, Dr. Vandana Bha a
9. Asherman's Syndrome ..................................................................
Dr. Sunil Shah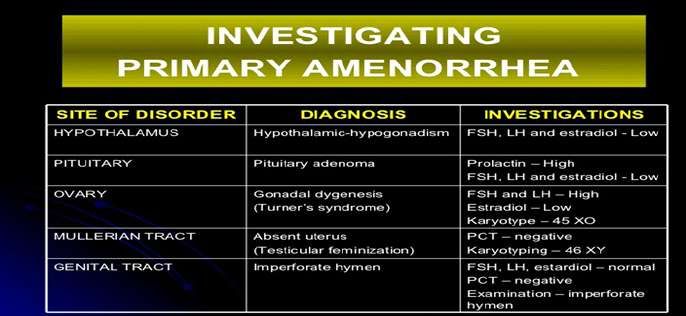
1 Dr Anita Singh
Amenorrhea: An Overview Dr Trip Sinha
Menstrua on is of great significance and concern to orifice, it is only the end-stage of a complex chain of
any woman and her healthcare-provider. The events star ng at the higher centers in the
cessa on of menstrua on is of even greater concern hypothalamus linked to the events at successively
to both and naturally sparks the ques on: why did lower levels in the pituitary and ovary with some
menstrua on stop? What are the implica ons of its confounding controls by other endocrine glands
cessa on in the short and long term? The answers notably the thyroid and adrenals. It is, therefore, not
would be contextual and need to be individualized. difficult to understand why inves ga ng a case of
amenorrhea involves methods and assays which look
Physiological Basis of Menstrua on into the normalcy or otherwise of the en re HPO
In order to understand the e o-pathogenesis of –axis as well as the reproduc ve ou low tract.
amenorrhea it is impera ve to look into the Figures 1 and 2 are simplified schema c and pictorial
physiological basis of menstrua on. Although the re p re s e nta o n s o f t h e e ve nt s l e a d i n g to
outward manifesta on of menstrua on is the menstrua on and the controls at various levels.
ou low of menstrual blood through the vaginal
Ovaries
Figure 1: Simplified schema c representa on of the events leading to menstrua on and controls at various levels
Figure 2: The hypothalamic-pituitary ovarian axis integrated to the reproduc ve ou low tract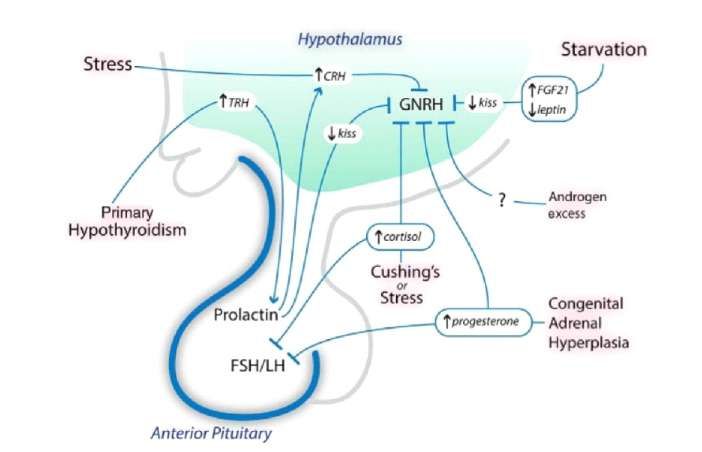
The menstrual cycle is divided into the following Health implica ons depend to a large extent on the
cyclical and sequen al phases: menstrua on, early e ology of amenorrhea. Hence, the need to establish
and late follicular/prolifera ve phase, ovula on, the cause of amenorrhea over-rides all other
early and late luteal/secretory phase followed by its concerns while planning its management. The HPO
repe on at regular or irregular cycle lengths which axis must be normal anatomically and func on
may vary in women and o en in the same woman at synchronously at various levels in order that neuro-
different periods in her reproduc ve age span. The transmi ers and hormones exert a normal end-
different phases of each menstrual cycle have their organ effect on the endometrium ensuring its cyclical
own hormonal milieu and endometrial histology. shedding off at the me of menstrua on.
The levels of progesterone, estradiol and inhibin-A This opening chapter of FOGSI Focus dedicated to the
from a waning corpus luteum dip pre-menstrually problem of amenorrhea gives a brief capsular
triggering a posi ve feedback on the anterior overview of the subject and sequen ally clarifies
pituitary to release more follicle-s mula ng basic concepts related to amenorrhea so that the
hormone (FSH) to recruit ovarian graffian follicles subsequent chapters are seen in their proper
with its oocytes for the next cycle. Gonadotropin perspec ve. Amenorrhea is discussed under the
–releasing hormone(GnRH) of hypothalamus is following headings:
released into the intra-cranial portal circula on in Ÿ Defini on
the vicinity of the pituitary gland in a pulsa le Ÿ Classifica on/types of amenorrhea
manner to ini ate the follicular phase. The estradiol Ÿ Epidemiology
and inhibin-B from the developing graffian follicles Ÿ Causes of amenorrhea and their classifica on
provide nega ve feedback to pituitary FSH secre on Ÿ Implica ons of amenorrhea: short term and long
so that it wanes by mid-follicular phase. Pituitary term
luteinizing hormone(LH) follows a reverse profile in Ÿ Management issues including pa ent counseling
follicular phase, decreasing ini ally with rising
estradiol of early follicular phase but later rising Defini on :
dras cally late in follicular phase(biphasic response). As a simple defini on, amenorrhea is the absence or
Just before ovula on, FSH-induced LH receptors are cessa on of menstrua on. An adolescent girl or
produced on granulose cells which subsequently woman in the reproduc ve age group who has never
with LH s mula on modulate progesterone had spontaneous menstrua on has primary
secre on. A er adequate estrogen the pituitary LH amenorrhea while a woman who was previously
surge is triggered leading to ovula on 24-36 hours menstrua ng cyclically/acyclically but has currently
later. In the subsequent early luteal phase ll mid- ceased to do so has secondary amenorrhea. The
luteal days the estrogen decreases and again rises as terms primary and secondary are further elaborated
a secre on from the corpus lureum. Inhibin –A is also upon in the next sec on on classifica on /types of
secreted concomitantly by the corpus luteum amenorrhea.
s mula on. Drama c progesterone rise in this
period of the menstrual cycle is a surrogate marker From a care-givers point of view, pa ents fulfilling
for previous ovula on occurrence. Progesterone, the following criteria merit evalua on for evalua on.
estrogen and inhibin –A act in tandem on the central 1. No menses by the age of 14 in the absence of
hypothalamic-pituitary axis in the luteal phase and grow th/development of secondar y sexual
effec vely suppress gonadotropin secre on and new characteris cs
follicular growth. As the corpus luteum withers and 2. No menses by the age of 16 regardless of the
dies these hormones decline thus preparing for the presence of normal growth/development of
subsequent cycles in an orderly sequence. A more secondary sexual characteris cs
elaborate descrip on of the menstrual physiology is 3. In previously menstrua ng women , no
beyond the scope of this introductory chapter on menstrua on for an interval of me equivalent to a
amenorrhea. (1) total of at least three previous cycles or no menses
over a 6 month period(2)Classifica on/types of amenorrhea: be classified as primary and secondary amenorrhea.
It helps in classifying the e ology of amenorrhea
from different perspec ves: its me of onset, the A} Primary: a girl who has achieved the age of 14
level at which the e ological factor operates and the years but has not menstruated nor shown visible
presence and absence of secondary sexual signs of development of secondary sexual
characteris cs. This clarity through classifica on characters, or a girl who has reached 15-16 years of
helps the clinician to guide his workup for that age with developed secondary sexual characters but
par cular pa ent. Management gets simplified if the not menstruated spontaneously are classified as
above e ological causes are ini ally categorized as having primary amenorrhea and merit inves ga on
physiological or pathological on the basis of the and appropriate management.
pa ent's history. The pathological group is further
c a t e g o r i ze d i n t o p r i m a r y a n d s e c o n d a r y B} Secondary: a woman previously having
amenorrhea. This then helps to target more menstrua on has failed to menstruate for the last
defini vely the level at which any defect operates. few months equivalent to her previous three
menstrual cycles at least or for the past six months is
Depending on the me of its onset, amenorrhea may considered to have secondary amenorrhea.
Primary Amenorrhea Secondary Amenorrhea
Constituitional delay(14) % Chronic anovulation(39%)
Gonadal failure/ dysgenesis (43%) Hypothyroidism
Imperforate hymen Hyperprolactinemia
Congenital absence of uterus and vagina Extreme weight change (anorexia/bulimia)
Hypothalamic failure( Kallman’s syndrome) Cushing’s syndrome
Androgen insensitivity Adrenal tumors
(Testicular Feminisation syndrome)
Androgen producing ovarian tumors
Premature ovarian insufficiency/ failure
Pituitary infarction(Sheehan’s syndrome)
Surgical extirpation of uterus &/or ovaries
Radiotherapy
Chemotherapy
Table 1 Summarises the causes of primary and secondary amenorrhea.
Based on its e ology, amenorrhea is classified as Causes of amenorrhea and their classifica on
follows: There is an exhaus ve list of pathological causes of
amenorrhea. The causes have been logically
A} Physiological: amenorrhea in pre-pubertal age classified in the WHO classifica on and by others
group, following physiological natural menopause, working in the field of reproduc ve endocrinology .
during pregnancy and lacta on. Physiological
amenorrhea does not need any interven on apart In the WHO classifica on of amenorrhea originally
from observa on and documenta on of future there were only three groups; the fourth group was
menstrual cycles and/or vaginal bleeding episodes. added subsequently.(3)
B} Pathological: amenorrhea arising from any other Group 1 Hypo-gonadotropic hypo-gonadism
cause apart from the above should induce the care (27.8%),
giver to logically inves gate its cause on the basis of Group 2 Normo-gonadotropic anovula on (23.7%)
and anatomical and physiological basis of Group 3 Hyper-gonadotropic hypo-gonadism
menstrua on and its likely aberra ons in the index (48.5%)
case. These causes may be congenital or acquired. Group 4 Hyper-prolac nemic anovula onLevel of lesion Type of lesions
Hypothalamic Craniopharyngioma, Germinoma, Tubercular granuloma, sarcoid granuloma, dermoid cyst ,
Kallman syndrome
Pituitary Craniopharyngioma, Germinoma , Tubercular granuloma, sarcoid granuloma, dermoid cyst,
Non-functioning adenomas
Hormone - secreting adenomas( prolactinoma, Cushing disease, acromegaly
Infarction
Lymphocytic hypophysitis
Surgical/radiotherapy -induced ablations
Sheehan syndrome
Diabetic vasculitis
Ovary Gonadal dysgenesis, FSH/LH hormone receptordefect, environmental & therapeutic
ovarian toxins, galactosemia, Sex chromosome mosaicism, partial deletion of X
chromosome, 17 -α hydroxylase deficiency in XX/XY individual ,ovo-testicular di sorder,
Uterus Mayer -Rokitstansky - Kuster -Hauser syndrome, absent endometrium, Asherman
syndrome(2*curettage, electro -excision, severe acute PID, tuberculosis, schistosomiasis
Vagina Imperforate hymen, transverse vaginal septum
Miscellaneous Androgen insensitivity
Table 2: E ological causes of amenorrhea opera ng at different levels of the HPO axis and reproduc ve ou low tract
A er clinical examina on, each pa ent can be absence or presence of secondary sexual
categorized into one of two groups on the basis of characteris cs (Table 3).
Secondary Sexual Characteristics Secondary Sexual Characteristics
Absent present
Physiological delay Mullerian agenesis (imperforate hymen,
transverse vaginal septum, Mayer-Rokitstansky-
Kuster-Hauser syndrome)
Gonadal dysgenesis Androgen insensitivity
FSH/LH receptor defect Ovo-testicular disorder
Sex chromosome mosaicism Absent endometrium
Partial deletion of X chromosome Asherman’s syndrome
Kallman’s syndrome Severe intra- uterine
infections(tuberculosis,PID, schistosomiasis
CNS Tumors
Hypothalamic/pituitary dysfunction
Enzyme deficiencies in XY individuals(5α–
reductase, 17,20-lyase,17 α- reductase)
Galactosemia
Congenital lipoid adrenal hyperplasia
Environmental & therapeutic ovarian toxins
Table 3: Causes of amenorrhea with and without development of secondary sex characteris cs
Emerging iatrogenic causes of amenorrhea include the importance of a rigorous medical and medica on
radiotherapy and chemotherapy for malignancies history.
as well ex rpa ve surgery on uterus and ovaries. An Table 4 is a comprehensive list of e ological causes
expanding list of medica ons frequently prescribed compiled by the the American Society of
to women needs to be kept in mind thus emphasizing Reproduc ve Medicine.(4)I. Anatomic defects (outflow tract) III. Hypothalamic causes
A. Mullerian agenesis (M -R-K-H syndrome) A. Dysfunctional
B. Complete androgen resistance (testicular 1. Stress
feminization) 2. Exercise
C. Intrauterine synechiae (Asherman 3. Nutrition -related a. Weight loss, diet, malnutrition b. Eating disorders
syndrome) (anorexia nervosa, bulimia)
D. Imperforate hymen 4. Pseudocyesis
E. Transverse vaginal septum B. Other disorders
F. Cervical agenesis —isolated 1. Isolated gonadotropin deficiency
G. Cervical stenosis —iatrogenic a. Kallmann syndrome
H. Vaginal agenesis —isolated b. Idiopathic hypogonadotropic hypogonadism
I. Endometrial hypoplasia or aplasia — 2. Infection
congenital a. Tuberculosis
b. Syphilis
c. Encephalitis/meningitis
d. Sarcoidosis
3. Chronic debilitating disease
4. Tumors
a. Craniopharyngioma
b. Germinoma
c. Hamartoma
d. Langerhans cell histiocytosis
e. Teratoma
f. Endodermal sinus tumor
g. Metastatic carcinoma
II. Primary hypogonadism IV. Pituitary causes
A. Gonadal dysgenesis a. Tumors 1. Prolact inomas
1. Abnormal karyotype 2. Other hormone -secreting pituitary tumor (ACTH,
a. Turner syndrome 45,X thyrotropin -stimulating hormone, growth hormone,
b. Mosaicism gonadotropin)
2. Normal karyotype b. Mutations of FSH receptor
a. Pure gonadal dysgenesis i. 46,XX ii. c. Mutations of LH receptor
46,XY (Swyer syndrome) d. Fragile X syndrome
B. Gonadal agenesis
C. Enzymatic deficiency B. Space-occupying lesions 1. Empty sella 2. Arterial aneurysm
1. 17a-Hydroxylase deficiency C. Necrosis 1. Sheehan syndrome 2. Panhypopituitarism
2. 17,20 -Lyase deficiency D. Inflammatory/infiltrative
3. Aromatase deficiency 1. Sarcoidosis
D. Premature ovarian failure 2. Hemochromatosis
1. Idiopathic 3. Lymphocytic hypophysitis
2. Injury a. Chemotherapy b. E. Gonadotropin mutations (FSH)
Radiation c. Mumps oophoritis
3. Resistant ovary a. Idiopathic
E. Ovarian tumors
1. Granulosa -theca cell tumors
2. Brenner tumors
3. Cystic teratomas
4. Mucinous/serous cystadenomas
5. Krukenberg tumors
6. Metastatic carcinoma
V. Other endocrine gland disorders VI. Multifactorial & other causes
A. Adrenal disease 1. Polycystic ovary syndrome
1. Adult-onset adrenal hyperplasia 2. Autoimmune disease
2. Cushing syndrome 3. Galactosemia
B. Thyroid disease
1. Hypothyroidism
2. Hyperthyroidism
Table 4: Classifica on of amenorrhea (not including disorders of congenital sexual ambiguity)-adapted
from the American Society of Reproduc ve MedicineManagement issues including pa ent counseling group to be pregnant unless proved otherwise.
No consensus has been reached regarding the point
at which oligomenorrhea becomes amenorrhea. Management o en involves inputs from other
Some authors suggest the absence of menses for 6 medical disciplines notably internist,
months cons tutes amenorrhea, but the basis for endocrinologist, neuro-surgeon and psychiatrist.
this recommenda on is unclear. For a post- However, most cases can be managed by
menarchal girl or a reproduc ve-aged woman to gynecologists and even primary healthcare
experience a menstrual cycle interval of more than physicians provided their management plan is
90 days is sta s cally unusual. Prac cally speaking, derived from a clear concept of the HPO axis and the
this should be an indica on for a thorough evalua on reproduc ve ou low tract anatomy.
to seek the cause.
Certain clinical points need to be kept in mind while
Important clinical considera ons in management of inves ga ng a case of amenorrhea. First, though the
amenorrhea involve the following issues:- dis nc on between primary and secondary
1) To manage ac vely or merely to keep under amenorrhea is important from the purpose of
observa on currently classifica on some mes the cause may overlap both
2) Management modali es for ac ve interven on primary and secondary amenorrhea (Figure 3).
3) How long to con nue the interven on Secondly, a girl showing obvious clinical s gmata of
certain disorders like Turner's syndrome or vaginal
Amenorrhea warrants inves ga ons if it occurs in agenesis may be evaluated earlier even before the
periods of life when physiological amenorrhea does normal age of menarche and puberty and the
not occur. It is prudent clinical prac ce to consider all parents counseled regarding her management and
cases of amenorrhea in women of reproduc ve age prognosis holis cally.
Figure 3: Discrete and overlapping causes of primary and secondary amenorrhea
A well taken history may reveal the correct e ology History- taking commences with ques ons related to
of amenorrhea in up to 85% cases. The ini al menstrual-type pains and/or menstrual molimina in
consulta on should be devoted to a systema c a girl who does not report menarche. In such girls the
elaborate history-taking followed by a complete me since when breast development commenced
methodical physical examina on of not only the should be enquired into. Women who cease to have
gynecological organs per se but all systems in general periods a er a previously menstrua ng should be
since amenorrhea may be merely one of the asked to elaborate on their previous menstrual
worrying manifesta ons of a disease which details especially whether lengthening cycles or
secondarily involves the gynecological system of the progressively reduced flow had culminated finally in
woman. the amenorrhea. In a young girl it is important to
clarify whether she only had menstrual-type bleedsfollowing hormone intake prescribed elsewhere. visual defects should guide inves ga ons towards
Such a history categorises her as a case of primary the central nervous system; similarly the renal
amenorrhea rather than secondary amenorrhea system disorders by causing elevated prolac n levels
who responded as a posi ve hormone challenge and inflammatory bowel disease should also not be
withdrawal bleed and gives a pointer to likely overlooked. Progressive hirsu sm and /or virilisa on
e ologies of the amenorrhea. as reported by the pa ent should be looked into and
may be manifesta on of classical late-onset
Obstetric history with regard to severe postpartum congenital adrenal hyperplasia, androgen-
hemorrhage o en requiring blood transfusion producing ovarian or adrenal tumor. Changes in hair
suggests Sheehan's syndrome leading to hypo- distribu on (excessive altered hair growth pa ern or
pituitarism and hypo-gonadotropic amenorrhea; thinning or loss of scalp hair or brows should lead the
manual removal of placenta or severe puerperal clinician to inves gate along the line of thyroid
sepsis may lead to amenorrhea by causing uterine dysfunc on or polycys c ovarian disease.
synechiae (Asherman's syndrome).
A host of frequently prescribed medica ons to
Personal history with respect to appe te, diet and modern day women can cause hyper-prolac nemia
caloric intake and exaggerated weight loss/gain may or other central HPO axis dysfunc on by altering
indicate hypothalamic dysfunc on (anorexia neuro-transmi er secre on and contribute to
nervosa or bulimic disorder) as do excessive mental amenorrhea. Examples include androgens, oral
and physical stress and radical life-style changes contracep ve pills, medroxy- progesterone acetate,
including exercise pa ern. Symptoms related to progestogen intra-uterine systems, GnRH agonists
hypo-estrogenism (hot flushes, mood changes, uro- a n d d r u g s c a u s i n g h y p e r- p r o l a c n e m i a (
genital discomfort) should be enquired into in phenothiazines, reserpine deriva ves,
relevant contextual se ngs. amphetamines, benzodiazepines, an -depressants,
dopamine antagonists, opiates).Table shows
Central nervous system complaints (headache, commonly prescribed medica ons which can cause
seizures, recurrent otherwise unexplained vomi ng, amenorrhea (Table 5)
Group of drug Names of drugs
Steroid hormones Oral contraceptive pills, estrogens, progestogens (medroxy - progesterone acetate,
progestogen intra -uterine systems), anabo lic steroids, GnRH agonists, androgens
Anti -psychotic drugs Resperidone
Anti -depressant drugs Benzodiazepines
Anti -hypertensive Reserpine derivatives
drugs
Anti -allergics ? cetrizine
Cytotoxic agents Alkylating agents (Busulphan, Cis -platinum Chlora mbucil, Cyclophosphamide,
Nitrogen mustardS), Melphalan, , , Procarbazine, , Adriamycin,
Anti -epileptics Phenobarbitones,phenytoin,carbamazepine,valproic acid
Addiction drugs Cocaine, opiods, amphetamines
Miscellaneous Dopamine agonists, cimetidine
Table 5: Medica ons likely to cause cessa on of menstrua onThough amenorrhea ul mately manifests as an levels of circula ng androgens and the presence and
abnormality of the reproduc ve ou low tract, clues recep vity of androgen receptors for sexual hair
as to its cause are o en/generally found in other growth. The dimensions of the clitoris, status of the
systems like the central nervous system, endocrine hymen, presence of any transverse septum vaginal
system and skin. At the commencement of the and vaginal canaliza on/atresia need to be
examina on, the pa ent's habitus, body mass index systema cally documented as indicated by the
and the waist: hip index need to be documented. An pa ent's history. If needed a vaginoscopy with a
obese or asthenic built especially when associated slender vaginoscope may be done to reveal the
with extreme rapid changes. Notable findings in the presence or absence of a cervix. In a sexually ac ve
skin include its dryness or moistness (thyroid woman a complete vaginal speculum examina on
dysfunc on), type and distribu on of hair (hirsu sm, followed by an internal bimanual vaginal
alopecia), acanthosis nigrans, purple stria. Lid lag, examina on is to be recorded in a proper format. For
exophthalmus and loss of lateral third of brow hair those not sexually ac ve per rectal assessment of the
are pointers to thyroid disorders as also fullness in uterus and adnexa is carried out.
the thyroid region of neck, exaggerated reflexes, full
bounding peripheral pulse and fine hand tremors. On the basis of a logical history and a well-conducted
systema c physical examina on the subsequent
Breast development scored on the basis of Tanner's workup of the pa ent can be more directed. In
classifica on should be documented as surrogate pa ents who do not demonstrate any obvious
markers for estrogen exposure whether natural or e ology the workup should be in a stepwise manner
exogenous as also advanced breast growth in addressing all levels of the HPO axis and the
rela on to expected development for biological age, reproduc ve ou low tract.
regression in size of previously well-developed
breasts, breast striae and the presence and The further workup requires blood assays by
characteris cs of any nipple discharge. Purple striae different modali es and laboratory techniques for
on abdominal skin, bu ocks and thighs should be hormones related to the HPO axis. Imaging
taken note of. A supra-pubic lump could be a techniques like high-resolu on state of art
hematometra explaining primary amenorrhea or an ultrasound, computerized tomography and magne c
ovarian tumor causing secondary amenorrhea. resonance imaging look into the normalcy or
otherwise of the reproduc ve ou low tract, ovaries
Pa ern of sexual hair growth in the infra-umbilical and intra-cranial hypothalamic and pituitary lesions.
area, the shape of the pubic hair line whether in male O en karyotyping and laparoscopy are indicated in
escutcheon pa ern or not and vulval hair growth order to reach the diagnosis of the cause of
amenorrhea.
Investigation modality Test performed
Biochemistry Laboratory FSH, LH, estradiol, progesterone, prolactin,auto -immune an tibodies
Microbiology laboratory PCR for mycobacterium uberculosis
Genetic laboratory Chromosomal karyotyping, gene studies, FMR -1, Anti - CYP21
Imaging facility Ultra sound of ovaries and reproductive outflow tract
(Antral follicle count -POI, PCOS dis tribution of multiple peripheral small sized cysts)
CT scan of hypothalamus and pituitary
MRI of hypothalamus and pituitary
Endoscopy Hysteroscopy
Laparoscopy
Table 5: Inves ga ons in evalua ng amenorrheaTables 6 and 7 indicate the levels of hormones and findings useful in clinching the e ology responsible
other relevant clinical findings and inves ga on for causing amenorrhea.
Table 6: Clinical findings and inves ga ons in different
causes of primary amenorrhea
Table 7: Clinical findings and inves ga ons in different
causes of primary amenorrhea
The following two flowcharts depict the sequence to of primary and secondary amenorrhea.
be followed while examining and inves ga ng casesTreatment depends on the underlying cause children or contracep ve inten ons of amenorrhea.
delineated by the abovemen oned workup protocol. Figure 4 is a simplified decision making tree
It also takes into considera on the need for regular summarizing the clinician's approach to a case of
periods, future reproduc ve concerns like desire for amenorrhea.
Ascertain by Hx whether primary or secondary
!! Check for hormone -induced withdrawal bleed
Urine pre gnancy test positive manage
!! all cases appropriately
Negative
Primary Amenorrhea Secondary Amenorrhea
2*sexual characters + ve 2*sexual characters -ve - Progesterone Challenge Test / E.T.*
-Hormone assays
-CNS imaging
Reproductive Outflow External Stigma of
Tract evaluation Chromosomal disorders FSH, LH, TSH, Prolactin
(Clinical exam . & eg Turners, AIS
Ultrasound)
↑FSH ↑TSH ↑Prolactin
HPO axis evaluation ↑
a) Hormonal assays Treat as appropriate
b) Chromosomal studies Premature ovarian
c) Auto -immune a.b.tests failure
Treatment options
usually surgical ↑FSH PCOS
*Counsel parents re. prognosis HRTs
*Special ART for successful Ovum donation Treat as per
pregnancy possible guidelines
*E.T. endometrial thickness
Figure 4: Simplified decision-making tree for evalua ng and trea ng a case of amenorrhea
This opening chapter of FOGSI focus dedicated to the References
very important and o -encountered gynecological 1.Olive D L & Palter S F. Reproduc ve physiology. In Berek
enigma of amenorrhea with all its a endant issues &Novak's Gynecology. Fourteenth Ed.2007. Wolters
and concerns orients the reader to the approach Kluwer/Lippinco Williams & Wilkins. Chapter 7. p 173.
which needs to be taken by the caregivers at primary 2.Speroff's Clinical Gynecologic Endocrinology and
and referral levels when a girl or woman a ends for Infer lity;9th Edi on/South Asian Edi on.2011. Wolters
Kluwer.Vol.1.Chapter 10. Amenorrhea:p.343
consulta on with this presen ng complaint. The
3. Insler V, Melmed H, Mashiah S, Monselise M, Lunenfeld
subsequent chapters individually dilate upon the
B, Rabau E. Func onal classifica on of pa ents selected
most important causes which confront the f o r g o n a d o t r o p i c t h e r a p y. O b s t e t G y n e c o l .
gynecologist. I am confident that readers will find the 1968;32(5):620-6.
contained material most useful for themselves in 4. The Prac ce Commi ee of the American Society for
their clinical prac ce and confidently and ra onally Reproduc ve Medicine. Current evalua on of
manage pa ents in their individual prac ce setups. amenorrhea. Fer lity and Sterility Vol. 90, Suppl 3,
N o v e m b e r 2 0 0 8 . S 2 1 9 -
225.doi:10.1016/j.fertnstert.2008.08.0382 Hypothalamic and Pitutary Dr Suvarna Khadilkar
Amenorrhea Dr Firdousara Siddiqui
Introduc on
Amenorrhea is a common clinical presenta on which
needs a thorough work up to pi point the diagnosis.
Intact hypothalamo-pituitary ovarian axis (HPO) is
essen al for normal menstrua on. Any dysfunc on in
the HPO axis or other endocrine glands can lead to
amenorrhea. It is also necessary that the reproduc ve
tract is developed fully and normally for normal
menstrua on.
Pa ent fulfilling any of the following criteria should be
evaluated for amenorrhea-
Ÿ No menses by age 14 in the absence of growth or
development- of secondary sexual characteris cs.
Ÿ No menses by age 16 regardless of the presence of
normal growth and development of secondary
Sexual characteris cs.
Ÿ In women who have menstruated previously, no
menses for an interval of me equivalent to a total
of at least three previous cycles or no menses over
a 6-month period [1].
This chapter will focus on amenorrhea caused by
dysfunc on or disorders of hypothalamus and
pituitary. Pathophysiological considera ons:
Condi ons that o en precede anovula on include
Hypothalamic dysfunc on is one of the most common marked weight loss, physical exercise, physical and
causes of Secondary amenorrhea. Secondary mental stress, oral contracep ve use. Amenorrhea is
amenorrhea, occurs in approximately 3–5 % of adult usually a result of hypogonadotrophic
women. According to the American Society of hypogonadism, marked by low or normal LH, FSH,
Reproduc ve Medicine (ASRM), Func onal and estradiol levels. Normal prolac n, and low lep n
Hypothalamic Amenorrhea (FHA) accounts for 20–35 are also seen in this type of amenorrhea. LH and FSH
% of secondary amenorrhea cases and 3 % of primary however do show response to GnRH s mula on.
amenorrhea [ 2]. The incidence is higher in athlete
women. 50 % of women who exercise regularly The cyclic nature of the hormonal changes is at halt,
experience subtle menstrual disorders and so is the pulsa le secre on of GnRH. Persistent slow
approximately 30 % of women have amenorrhea frequency of GnRH secre on is inadequate to
according to study by DeSouza et al [3]. The female maintain the level of LH synthesis and secre on
athlete triad first described in 1997 is complex of required for an ovulatory LH surge, hence leads to
distorted ea ng, amenorrhea and osteoporosis [ 4]. anovula on. Extreme physical, nutri onal or
emo onal stress leads to func onal suppression of
Hypothalamic amenorrhea is diagnosed only a er reproduc on as a psychobiologic response of life
ruling out pituitary and ovarian abnormali es. events.Stress elevates cor cotropin-releasing hormone Clinicians should also obtain a thorough family
(CRH), which inhibits GnRH secre on and history with a en on to ea ng and reproduc ve
reproduc ve func on in animal studies. Some disorders.
women with hypothalamic amenorrhea have
elevated plasma cor sol levels and blunted Inves ga ons
responses to CRH, which suggests stress-induced Complete blood count, es ma on of electrolytes,
abnormali es in CRH secre on. In women where glucose, bicarbonates blood urea nitrogen,
amenorrhea is associated with strenuous exercise, crea nine is recommended. Liver func on tests, ESR,
data suggest a nega ve energy balance is a C-reac ve protein, and basic endocrine work up is
precipita ng factor, and plasma lep n levels are also recommended. Basic endocrine work up
reduced. Hypolep nemia appears to be an includes serum thyroid-s mula ng hormone, free
important factor in athletes and women at low body thyroxine (T4), luteinizing hormone, follicle-
weight. Administra on of recombinant human lep n s mula ng hormone, estradiol, and an -Mullerian
for 3 months may increase GnRH pulsa lity. hormone. Androgen levels are advised only when
clinical hyperandrogenism is present.
Disorders of Hypothalamus and Pituitary Leading to
Amenorrhea: A baseline bone mineral density (BMD)
Ÿ CNS disorders measurement by dual-energy X-ray absorp ometry
-Chronic hypothalamic anovula on (DXA) should be obtained with 6 or more months of
- Stress amenorrhea.
- Increased exercise levels
- Anorexia nervosa Pelvic ultrasound in all pa ents to ensure normalcy,
-Pseudocyesis and MRI pelvis only when indicated is advised.
-Func onal amenorrhea
-Isolated GnRH deficiency Diagnos c tests:
– Head trauma Most commonly performed progesterone challenge
– Space-occupying lesions, infec ons test with 10 mg medroxyprogesterone for 5 days is
Ÿ Pituitary disorders useful to differen ate between ovarian cause and
– Hyperprolac nemia hypothalamic cause. If withdrawal period is
- Prolac noma achieved, then it denotes presence of endogenous
- Medica ons estrogen and ensures ou low tract func on and
- PCOS patency. There will be no withdrawal period if there is
- Renal failure n o e n d o g e n o u s e s t r o g e n p r e s e n t l i ke i n
– Hypoprolac nemia hypothalamo-pituitary causes.
– Pituitary stalk resec on
– Sheehan's syndrome Following tests are used only when the diagnosis
cannot be made with rou ne clinical examina on
Diagnosis and Management : and inves ga ons.
Detailed personal history with a focus on following 1. GnRH s mula on test: this is of use to differen ate
points: between hypothalamic and pituitary causes of
Dietary habits, history of ea ng disorders, exercise hypogonadism.100 μg GnRH is given intravenously.
and athle c training; a tudes such as perfec onism LH and FSH response is measured with samples at 0,
and desire for social approval; highly ambi ous 20 and 60 minutes In pituitary disease, response is
personality, high expecta ons for self and others, too either absent or blunted. In hypothalamic disease,
many weight fluctua ons, irregular sleep pa erns, normal response is seen.
stressors, mood fluctua ons, menstrual pa ern; 2. Clomiphene s mula on test may be useful to
fractures, and substance abuse. dis nguish organic causes of gonadotropin
deficiency (pituitary or hypothalamic pathology)from func onal disorders and idiopathic delayed suscep bility is iden fied on loci for Anorexia
puberty. In healthy adults, clomiphene blocks nervosa on chromosome 1 and for bulimia nervosa
estrogen feedback mechanisms in the hypo- on Chromosome 10.
thalamus, thus leading to a rise in GnRH
(gonadotropin-releasing hormone) and Two types of Anorexia nervosa have been defined
consequently circula ng LH and FSH. A er 7 days of restric ng and binge/purging. The diagnos c Criteria
clomiphene s mula on, if LH levels increase more for bulimia nervosa are dis nct from those for
than 120% and FSH increases more than 40 %, the anorexia nervosa primarily in that they do not
response is considered normal. A normal response include low body weight or amenorrhea.
essen ally rules out organic causes of
hypogonadotropic hypogonadism and in delayed The weight loss due to any reason will result in
puberty, it is an indica on that sexual maturity will reduc on in total percentage of fat in the body. 22%
ensue. of body fat is the cri cal body fat percentage
3. In hypothalamic-pituitary pathology there is no necessary for sustaining menstrua on. If this
response. Not useful in girls with early puberty.To percentage drops below 22% then the amenorrhoa
differen ate between func onal and organic cause or the menstrual dysfunc on results. Anorexa
of amenorrhea, some form of imaging of the brain nervosa pa ents exhibit hypercor solism due to
(CT or MRI) to rule out a tumor may be useful increased cor cotropohin releasing hormone
especially when a history of severe or persistent [CRH}and ACTH. CRH directly inhibits GnRh secre on
headaches; persistent vomi ng, unexplained change through increased endogenous opioids hence leads
in vision, thirst, or urina on, lateralizing neurologic to speroff's compartment IV amenorrhoea. Brain
signs, and any indica on of pituitary hormone senses the blood levels of lep n If weight loss is due
deficiency or excess. to excessive physical exercise, it is found that the
athletes have 3 fold lower levels of lep n .therefore
Treatment : even athletes have amenorrhoea.
General principles :
• For acute and morbid pa ents inpa ent therapy is Some mes those suffering with anorexia or bulimia
required do not appear underweight. Some may be of average
• Correc ng the energy imbalance is important weight or slightly overweight. Varia ons can be
• If nutri onal, psychological, and modified exercise anywhere from extremely underweight to extremely
interven on (Cogni ve behavior therapy CBT) are overweight. The appearance of a person suffering
n o t effe c ve , o ra l co nt ra c e p ve p i l l s fo r with an ea ng disorder does not dictate the amount
maintenance of menstrual cycles and Bone mineral of physical danger they are in, nor does it determine
density are required. the severity of emo onal conflict they are enduring.
• Bisphosphonates, denosumab, testosterone, and
lep n are not recommended [5] Preven on and iden fica on of early or par al
• If CBT is not effec ve, treatment with pulsa le disorder to prevent full blown syndrome is
gonadotropin-releasing hormone (GnRH) as a first important.
line, followed by gonadatropin therapy and
induc on of ovula on, is used for treatment of Diagnosis is usually clinical but GnRH levels close to
infer lity. zero in presence of high levels of cor sol differen ate
this disorder from pituitary insufficiency. Weight loss
Ea ng disorders : due to other endocrine or other diseases may be
Cultural influences, other psychological, biologic, misdiagnosed and vice versa.
gene c and social factors likely contribute to
development of ea ng disorders. Peripubertal girls Complica ons:
and young women having first degree rela ves with Pa ent with anorexia nervosa are at risk for many
an ea ng or affec ve disorder or alcoholism are at complica ons related to nutri onal and electrolyte
increased risk of developing ea ng disorder. The imbalances Amenorrhea Anovula on NeuropathiesMyopathies Life-threatening cardiac arrhythmias, Ea ng disorders are rela vely rare in India but may
Gastri s, Esophagi s, Weakness from chronic be picked up more o en if ac vely looked for. Ac ve
anemia. search may help early diagnosis, as well as effec ve
The most common cause of death in anorexia treatment and will reduce high mortality associated
nervosa is suicide. with it. Change of lifestyle, psychological counseling
of not only the peripubertal girls but also of their
Treatment: disturbed family is important.
Management requires a team approach in which
different professionals work together. Individual and Stress or exercise induced amenorrhea:
family psychotherapy are effec ve in pa ents with Women who are involved in strenuous recrea onal
anorexia nervosa and cogni ve-behavioral therapy is exercise or other forms of demanding physical
effec ve in bulimia nervosa. ac vity such as dancing have a high prevalence of
menstrual irregularity and amenorrhea.[3] The
Care of pa ents with anorexia nervosa includes poten al adverse effect of intense exercise and low
stabiliza on for any life-threatening condi ons (eg, body weight on menstrual func on is synergis c.
shock, cardiac arrhythmias). In addi on, protec on
of the pa ent may be necessary if risk of suicide is Exercising amenorrheic women do not exhibit a
present. Treatment may include rehydra on, normal diurnal lep n rhythm; treatment with
correc on of electrolyte abnormali es (eg, exogenous recombinant human lep n can restore
hypokalemia), and ins tu on of appropriate gonadotropin pulsatality, follicular development and
disposi on for con nuing medical and psychiatric ovulatory func on in exercising amenorrheic
treatment. Consulta on with psychiatry and women.[4]
adolescent medicine specialists in order to op mize
inpa ent care and facilitate outpa ent follow-up Congenital GnRH deficiency (normosmic) is seen in
care should be done. rare individuals, congenital specific muta on that
prevents normal GnRH neuronal migra on during
For nutri onal therapy, forced feedings with total embryogenesis or to muta on in the pituitary GnRH
parenteral nutri on or tube feedings provide receptor.
nutrients, stabilize nutrient deficiency syndromes,
and alter mood when the pa ent becomes Kallmann Syndrome is Congenital GnRH deficiency
nutri onally replenished. Preliminary treatments associated with anosmia or hyposmia the disorder is
with opiate antagonists have shown promising known as Kallmann Syndrome, classical X linked
results. Monitoring of nutri onal status (eg, serum disorder, caused by gene c muta on in the KAL gene.
protein and albumin, electrolytes, serum glucose) is Kallmann syndrome can be inherited in autosomal
important. As nutri onal status improves, outpa ent dominant or recessive fashion.
treatment can be offered. Daily caloric intake 2600
cal /day is advised. Ongoing psychiatric care is GnRH Receptor Muta ons- There are more than 20
necessary, as the relapse rate is high. inac va ng muta ons in the GnRH receptor gene
(GNRHR). Some results in interference with normal
Prognosis: Signal transduc on, some effec vely prevent GnRH
• The general prognosis is related to the severity of binding, both results in resistance to GnRH
the underlying personality and family s mula on.
psychopathology.
• The prognosis for pa ents with a bulimic Disorder of Anterior Pituitary
component is worse than for those without bulimia. Variety of disorder involving anterior pituitary may
Death for pa ents with bulimia is 5-40%. cause amenorrhea ,most common by far is benign
A small percentage of pa ents become symptom Adenomas, Other include craniopharyngioma,
free, 30% remain chronically ill, and the rest are meningiomas, gliomas, metasta c tumors and
vulnerable to the return of symptoms during chondromas.
stressful mes .Pituitary adenomas are classified by cell type and size Conclusion:
and may be func onal (hormone secre ng) or Hypothalamic and pituitary Amenorrhea is an
nonfunc onal. Tumors less than 10mm in size are underes mated clinical problem. It is related to
called microadenomas and those 10mm or larger are profound impairment of reproduc ve func ons
called macroadenomas. Pituitary adenomas may be including anovula on and infer lity. Women's health
incidentally diagnosed while evalua ng for in this disorder is disturbed in several aspects
neurological Symptoms or workup of menstrual including their skeletal system, cardiovascular
irregulari es The most common neurological system and mental problems. Pa ents manifest a
symptoms associated with pituitary tumors, decrease of bone mass density, which is related to an
macroadenomas is visual impairment, classically increase of fracture risk. Therefore, osteopenia and
Bitemporal hemianopsia, other symptoms include osteoporosis are the main long-term complica ons
decreased visual acuity, diplopia, headache, CSF of Hypothalamic Amenorrhea. Cardiovascular
rhinorrhea, pituitary apoplexy. complica ons include endothelial dysfunc on and
abnormal changes in the lipid profile. Hypothalamic
Pituitary adenomas (Prolac noma) are treated with Amenorrhea pa ents present significantly higher
Dopamine agonist bromocrip ne, Drug of choice and depression and anxiety and also sexual problems
recommended dose is 1.25mg at bed me daily for compared to healthy subjects.
the first week and then gradually increased. Other
promising drug is cabergoline given in dose of Amenorrhea pa ents should be carefully diagnosed
0.25mg once or twice weekly ll tumors shrink, and properly managed to prevent both short- and
transsphenoidal resec on of tumor is done if medical par cularly long-term medical consequences.
therapy fails.
Sheehan Syndrome
Necrosis of the pituitary following postpartum REFERENCES:
hemorrhage may lead to Sheehan syndrome. 1. Hugh S Taylor, Lumina pal, Emre Seli, Speroff''s
Syndrome may develop slowly over 8–10 years' me. Clinical Gynecologic Endocrinology and Infer lity,
The hormones like GH, FSH and LH, TSH and ACTH are 9th Edi on; Wolters kluwer; 2019: (342-395)
reduced. Ini ally failed lacta on can be the 2. Prac ce Commi ee of American Society for
presen ng symptom. Secondary amenorrhea and Reproduc ve Medicine (2006) Current evalua on of
loss of secondary sexual characteris cs are seen in Amenorrhea.Fer l Steril 86:S148
most cases. Replacement of deficient hormones is 3. De Souza MJ et al (2009) High prevalance of subtle
necessary in majority of cases to maintain quality of and severe menstrual disturbances in exercising
life. women: confirma on using daily hormone
measures.Hum Reprod 25:491-503
Inappropriate secre on of prolac n (including drugs, 4.O s CL et al (1997) American college of Sports
other diseases, e.g. hypothyroidism, prolac noma) medicine posi on stand. The Female athlele triad.
will affect secre on of LH and FSH. Med Sci Sports Exerc 29:1-9
5. GORDON, Catherine M., et al. Func onal
GnRH s mula on test differen ates between hypothalamic amenorrhea: an endocrine society
hypothalamic and pituitary cause of hypogonadism. clinical prac ce guideline. The Journal of Clinical
Clomiphene s mula on test dis nguishes organic Endocrinology & Metabolism, 2017, 102.5: 1413-
cause of gonadotropin deficiency from func onal 1439. h ps://doi.org/10.1210/jc.2017-00131
d i s o rd e r a n d i d i o p at h i c d e l aye d p u b e r t y. 6. Dr Suvarna Khadilkar's Endocrinology in Obstetrics
Clomiphene blocks estrogen feedback mechanism in and Gynaecology, 1st Edi on; FOGSI , Jaypee
hypothalamus, normal response rules out publica on;2015: (155-167)
hypogonadotropic hypogonadism and delayed
puberty, no response is seen in hypothalamus-
pituitary pathology, diagnosis of func onal disorder
is made by CT or MRI imaging.[6]3
Amenorrhoea: Endocrine Issues Dr Pra k Tambe
Background hyperandrogenism and polycys c ovary syndrome
The recogni on that rhythmic produc on of have all been dealt with in publica ons since over 50
oestrogen and progestogen by the ovary is central to years ago.1
the cycle of follicular ripening, ovula on, corpus
luteum forma on, degenera on and menses has Ae ology
been part of medical science since centuries and is The commonly encountered causes of amenorrhoea
affirmed in medical texts. The pathological issues can be categorised as ou low tract abnormali es,
surrounding amenorrhoea including congenital and primary ovarian insufficiency, hypothalamic and
acquired disease of the ovary, faulty ovarian pituitary disorders, neuroendocrine issues and
development, gene c issues and sex reversal, sequelae of many chronic disease.
Outflow tract abnormalities Hypothalamic or pituitary disorders (continued) Other endocrine gland disorders
Acquired Constituional delay of puberty Adrenal insufficiency
Cervical stenosis Empty sella syndrome Androgen-secreting tumor (e.g., ovarian
Intrauterine adhesions Functional (overall energy deficit or stress) or adrenal)
Congenital Eating disorder Cushing syndrome
5α-reductase deficiency Stress Diabetes mellitus, uncontrolled
Androgen insensitivity syndrome Vigorous exercise Late-onset congenital adrenal hyperplasia
Imperforate hymen Weight loss Polycystic overy syndrome (multifactorial)
Műllerian agenesis Gonadotropin deficiency (e.g., Kallmann syndrome) Thyroid disease
Transverse vaginal septum Hyperprolactinemia Amenorrhea attributed to chronic disease
Primary ovarian insufficiency Adenoma (prolactinoma) Celiac disease
Acquired Chronic kidney disease Inflammatory bowel disease
Autoimmune Medications or illicit drugs (e.g., antipsychotics, Other chronic disease
Chemotherapy or radiation opiates) Physiologic or induced
Congenital Physiologic (pregnancy, stress, exercie) Breastfeeding
Gonadal dysgenesis (other than Infarction (e.g., Sheehan syndrome) Contraception
Turner syndrome) Infiltrative disease (e.g., sarcoidosis) Exogenous androgens
Turner syndrome or variant Infectio (e.g., meningitis, tuberculosis) Menopause
Hypothalamic or pituitary disorders Medications or illicit drugs (e.g., cocaine) Pregnancy
Autoimmune disease Trauma or surgery
Brain radiation Tumor (primary or metastatic)
Table 1 Spectrum of disorders presen ng with amenorrhoea2
Clinical findings T h e p hys i ca l exa m i n a o n s h o u l d i d e n f y
A detailed history and thorough clinical evalua on is anthropometric and pubertal development trends.
a must though with the advent of new diagnos c All pa ents should be offered a pregnancy test and
methodologies in our armamentarium, this is assessment of serum follicle-s mula ng hormone,
some mes ignored. The history should include luteinising hormone, prolac n, and thyroid-
menstrual onset and pa erns, breast and pubic hair s mula ng hormone levels. Addi onal tes ng,
development, ea ng and exercise habits, presence including karyotyping, serum androgen evalua on
of psychosocial stressors, body weight changes, and pelvic or brain imaging should be
medica on use, galactorrhoea and any chronic
individualised.[2,3,4]
illness. Addi onal ques ons may target neurologic,
vasomotor, hyperandrogenic or thyroid-related
symptoms.Findings Asociations
History
Chemotherapy or radiation Impairment of specific organ or structure, (e.g., brain, pituitary, ovary)
Family history of early or delayed menarche Constitutional delay of puberty
Galactorrhea Pituitary tumor
Hirsutism, acne Hyperandrogenism, PCOS, ovarian or adrenal tumor, CAH, Cushing
Illicit or prescription drug use syndrome
Loss of smell (anosmia) Multiple associations, consider effect on prolactin
Menarche and menstrual history Kallman syndrome (GnRH deficiency)
Sexual activity Primary vs. secondary amenorrhea
Significant headaches or vision changes Pregnancy
Temperature intolerance, palpitations, diarrhea, Central nervous system tumor, empty sella syndrome
constipation, tremor, depression, skin changes Thyroid disease
Vasomotor symptoms (e.g., hot flashes or night
sweats) Primary overian insufficiency, natural menopause
Weight loss, excessive exercise, poor nutrition, Functional hypothalamic amenorrhea
psychosocial distress, diets
Physical examination
Abnormal thyroid examination Thyroid disorder
Acanthosis nigricans or skin tags Hyperinsulinemia (PCOS)
Anthropomorphic measurements; growth charts Multiple associations; Turner syndrome, constitutional delay of puberty
Body mass undex High: PCOS
Low: Functional hypothalamic amenorrhea
Bradycardia Functional hypothalamic amenorrhea (e.g., anorexia nervosa)
Breast development (normal progression) Presence of circulating estrogen*
Dysmorphic features (e.g., webbed neck, short Turner syndrome
stature, low hairline)
Male pattern baldness, increased facial hair, acne Hyperandrogenism, PCOS, ovarian or adrenal tumor, CAH, Cushing
Pelvic examination syndrome
Absence or abnormalities of cervix or uterus
Clitoromegaly Rare congenital causes including Müllerian agenesis or androgen
Presence of transverse septum or imperforate insensitivity syndrome
hymen Androgen-secreting tumor; CAH; 5α- reductase deficiency
Reddened or thin vaginal mucosa Outflow tract obstruction
Sexual maturity rating abnormal Decreased endogenous estrogen
Striae, buffalo hump, central obesity, hypertension Turner syndrome, constitutional delay of puberty, rare causes
Cushing syndrome
2
Table 2 Pathognomonic findings on clinical examina on
Inves ga ons missed, the socioeconomic status of the pa ent
These should be tailored to the differen al diagnosis should be taken into considera on so that we do not
a er history and clinical examina on. While a ba ery over-burden the pa ent.
of tests is o en ordered to ensure that no diagnosis is
Findings Associations
Laboratory testing (refer to local reference values)
17-hydroxyprogesterone level High: late-onset CAH
(collected at 8 a.m.)
Anti-Müllerian hormone High: Functional hypothalamic amenor-
rhea, PCOS
Low: Primary ovarian insfciency
Complete blood count and Abnormal: chronic disease (e.g., elevated
metabolic panel liver enzymes in functional hypothalamic
amenorrhea)You can also read