An african response to covid-19 - From principled first response to just recovery - ReliefWeb
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

An african response to covid-19 From principled first response to just recovery www.oxfam.org
OXFAM BRIEFING PAPER – APRIL 2021 In November 2020 Oxfam and SOAS facilitated an online high-level event to bring together African and international policy and public-health professionals to discuss their experiences during the COVID-19 pandemic, and offer insights into strategies and policies they have enacted in their respective contexts. Speakers tackled a wide range of issues, including government strategies and policies implemented, public health messaging and community engagement, varying threads of intersectionality and an honest discussion about gaps and additional support. This ‘outcomes’ paper draws out the key themes, trends and recommendations emerging from the discussions to inform a people- not-profit-centric Covid response. © Oxfam International April 2021 This paper was written by Deepayan Basu Ray. Oxfam acknowledges the assistance of Dr Michael Jennings and Ellen Goodwin of SOAS in its production. It is part of a series of papers written to inform public debate on development and humanitarian policy issues. For further information on the issues raised in this paper please email advocacy@oxfaminternational.org This publication is copyright but the text may be used free of charge for the purposes of advocacy, campaigning, education, and research, provided that the source is acknowledged in full. The copyright holder requests that all such use be registered with them for impact assessment purposes. For copying in any other circumstances, or for re-use in other publications, or for translation or adaptation, permission must be secured and a fee may be charged. E-mail policyandpractice@oxfam.org.uk. The information in this publication is correct at the time of going to press. Published by Oxfam GB for Oxfam International under ISBN 978-1-78748-744-4 in April 2021. DOI: 10.21201/2021.7444 Oxfam GB, Oxfam House, John Smith Drive, Cowley, Oxford, OX4 2JY, UK. Cover photo: Munashe Nyamuzinga talks to community members about hand hygiene as part of the COVID-19 response in Harare, Zimbabwe. Credit: Tavonga Chikwaya/Oxfam.
INTRODUCTION On November 20, 2020 Oxfam and SOAS facilitated an online high-level event to bring together African and international policy and public-health professionals to discuss their experiences during the COVID-19 pandemic, and offer insights into strategies and policies they have enacted in their respective contexts. Speakers tackled a wide range of issues, including government strategies and policies implemented, public health messaging and community engagement, varying threads of intersectionality and an honest discussion about gaps and additional support. This ‘outcomes’ paper reviews the interventions covered by the speakers at this event, touches on some of the key reference documents produced by their respective institutions and agencies, and draws out some of the key themes, trends and recommendations emerging from the discussions. As such, the paper is organized into six major themes that emerged from the event: 1. Coordination mechanisms and standard operating procedures (SOPs). 2. Community engagement and clarity of public health messaging. 3. Mapping and tackling additional health-related threats. 4. The impact of COVID-19 on women. 5. Food security and nutrition. 6. Gaps and additional support (support to procure vaccines, social protection, and risk management (second wave) and enforcement. In keeping with the original intention of the event, this paper aims to capture good practice, reflect on the successes of African countries, and explore some of the gaps that have emerged in African COVID-19 responses. The paper also sets out some recommendations and policy solution proposals for coping with COVID-19’s primary and secondary impacts in ways that save lives now and in a future just recovery. The six speakers to give presentations at the event were: • Dr Jean-Jacques Muyembe Tamfum, Director General, National Institute for Biomedical Research, Professor of Microbiology at Kinshasa University Medical School, DRC. • Hon. Dr Wilhelmina Jallah, Minister of Health, Liberia. • Dr Ekwaro Obuku, physician, researcher and academic. • Dr David Nabarro, UN WHO COVID-19 Special Envoy. • Siphokazi (Sipho) Mthathi, Executive Director of Oxfam South Africa. • Rev. Nicta Lubaale, General Secretary of the Organization of African Instituted Churches (OAIC). The event was co-moderated by Dr Michael Jennings, Reader at SOAS, and Abby Maxman, President and CEO of Oxfam America.
The two common elements to have featured in all the interventions were mobilizing the lessons learned in combating Ebola to effectively tackle COVID-19, and the impact of the pandemic on women in Africa. Recognition of the impact of the virus on women and taking stock of women’s formal and informal leadership in the pandemic response has proven to be a game- changer in Africa. In addition, lessons learned about multi-agency coordination, clear and consistent public health messaging and rigorous standardized operating procedures (e.g. screen, test, isolate and trace) formed the basis of successful interventions to keep the virus at bay in most African countries. This paper will explore each of the major themes to emerge from the panel discussions. 1 COORDINATION MECHANISMS AND STANDARD OPERATING PROCEDURES (SOPS) The panel speakers reflected on the valuable lessons learned during the 2014–2016 Ebola outbreak, and how these experiences have played a key part in holding COVID-19 at bay in African countries. ‘The Ebola outbreak has taught us many lessons, among them that the response to outbreaks and emergencies must start and end at ground level – which means that certain key capacities have to be in place before launching a response, including leadership and coordination, technical support, logistics, management of human resources and communications.’ 1 It was necessary to ensure a multi- sectoral response, with effective coordination mechanisms at the institutional, grassroots, local, national and regional levels. Women have also led from the front in a number of African government responses, and the speakers on the panel reflected on the importance of this strategy. ‘Women leaders are better placed to draw on informal networks to mobilize rapid responses and community support. They are used to finding alternative resources and building ingenious partnerships to solve problems.’ 2 Dr Wilhelmina Jallah, the Liberian Minister of Health, noted in her remarks that one key lesson her country had learned from the 2016 Ebola response was the importance of effective coordination at central government level, and this was addressed by the establishment of the National Public Health Institute (NPHIL). ‘In collaboration with the Ministry of Health, NPHIL strengthens existing infection prevention and control efforts, laboratories, surveillance, infectious disease control, public health capacity building, response to outbreaks, and monitoring of diseases with epidemic potential.’ 3 Once the threat of COVID-19 had been identified in December 2019, ‘the

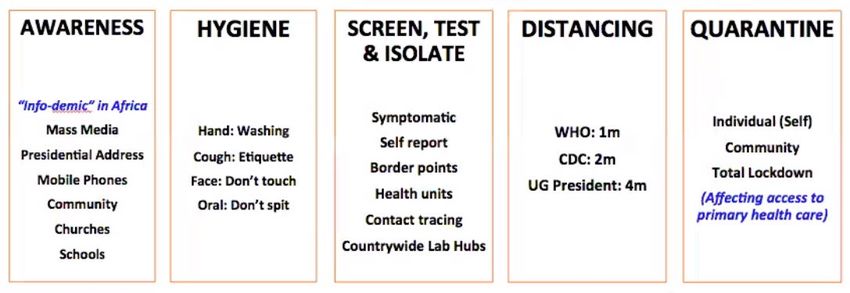
Government, in coordination with the United Nations (UN), Donor Partners, the Ministry of Health and the National Public Health Institute of Liberia put in place the National Multi-sectoral Response Plan (NMRP) to COVID-19’. 4 Dr Jean-Jacques Muyembe Tamfum, 5 the eminent microbiologist who led the Democratic Republic of Congo’s response to Ebola, was subsequently tasked with leading the country’s fight against COVID-19. Dr Muyembe also reflected on the fact that existing systems, structures and procedures that had been developed to combat Ebola were key to ensuring that the COVID- 19 pandemic was contained quickly and effectively. Dr Muyembe’s team enacted an ‘identify, confirm, isolate and trace’ methodology to ensure that COVID-19 cases being brought into the country by travellers from abroad (largely Europe) were prevented from spreading the infection within communities. Aside from the technical elements of this pandemic response, Dr Muyembe was also categorical in noting that the dual tenets of political commitment and raising awareness within communities were crucial to the overall success of the strategy. In Uganda, the response was similarly multidisciplinary, well connected and well coordinated. As noted by Dr Ekwaro Obuku, who is affiliated to the Makerere University College of Health Sciences in Kampala, one of the first steps to be taken in the country was the establishment of the COVID-19 Pandemic Rapid Evidence Synthesis Group (COVPRES). ‘This is a group of multidisciplinary scientists in East Africa who have come together in a synergy to identify and synthesize credible evidence around the SARS-Cov 2 virus and COVID-19 pandemic, relevant to low and middle-income countries.’ 6 The group began monitoring more than just the direct epidemiological impact of COVID-19, and found that as a result of the lockdown measures enacted by the Ugandan government, the negative socio-economic and medical impacts of other diseases and conditions were being overlooked. This recognition has helped ensure that Ugandan public health authorities now factor in the impact of COVID-19-related measures on other health issues, such as malaria, pneumonia, anaemia and tuberculosis. As each of the speakers on the panel noted, the importance of readily implementable standard operating procedures, or SOPs (designed to deal with public-health-related crises such as epidemics), were key to the successes across the African continent. In particular, experiences and systems developed to combat Ebola proved to be similarly successful in holding back the full impact of COVID-19: disease surveillance, case finding, contact tracing and mass communication campaigns to inform affected populations. 7 Related to this, Dr Obuku summarized the main elements of the SOPs in Uganda in the graphic below. Broadly, this was consistent with the experiences recounted in DRC, Liberia, Kenya and South Africa, and those recounted by Dr Nabarro from the WHO in Nigeria, Senegal and Morocco.

Fig 1: Uganda’s SOPs to combat COVID-19 – presentation by Dr Obuku (Friday, 20 November 2020) As a number of the speakers alluded to, the key to success has been a commitment to a system-wide approach, and ensuring that all elements of the SOPs are being implemented meaningfully and simultaneously. As the WHO noted, in countries where one or more elements have not been implemented with equal focus, the results have been devastating. According to the UN in Sierra Leone, ‘the country developed a COVID-19 preparedness plan three weeks before its first case was confirmed. This enabled the Ministry of Health to quickly identify, test and quarantine most of the primary contacts of the index case, thereby limiting spread of the disease.’ 8 Similarly, Liberia, Uganda and DRC also locked down before any death from COVID- 19 was registered in these countries. Evidence suggests that these measures were successful in slowing community transmission rates across the continent, 9 though not all of the results were so positive. This paper will reflect on some of these aspects in a later section. 2 COMMUNITY ENGAGEMENT AND CLARITY OF PUBLIC HEALTH MESSAGING ‘If you want to go fast, go alone. If you want to go far, go together.’ African proverb, recounted by Dr Obuku Bringing communities on board with a national strategy to tackle COVID-19 has consistently shown to be one of the most effective tools across Africa. Governments that have embedded community engagement into the heart of the public-health response and mobilized human and financial resources early within communities have managed to hold community transmission rates of COVID-19 at bay. Ensuring women are helping to shape the engagement strategies and are being put into leadership positions within their communities has proven to be successful time and time again. In DRC,

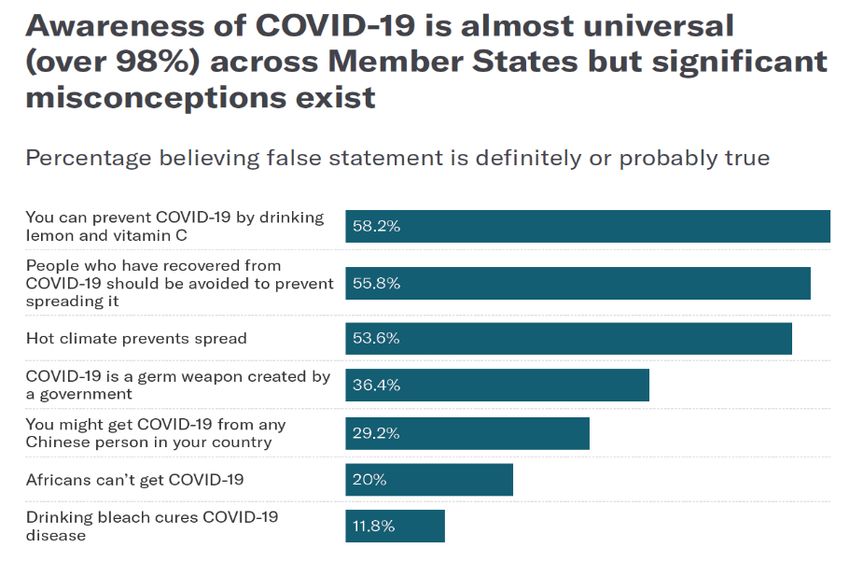
one of the two pillars of the government response was to ensure that communities were sensitized early on to the risks associated with the virus and that community-based organizations, such as women’s groups and faith groups, were supported to get the message out into the communities. 10 Engagement with communities is also a critical element of ensuring that public health messaging and measures are adapted to the local context and take into account specific socio-cultural and ethnic dimensions before rolling out initiatives. In the age of social media where information (both true/verified and false/fabricated) transcends borders, it is critically important to identify inaccurate perceptions that find traction within communities and mobilize clear and comprehensive public health messaging and sensitization activities to combat falsehoods and the stigma they generate. A recent survey, conducted by the Partnership for Evidence-Based Response to COVID-19 (PERC) and looking at 20 African Union countries, showed that although knowledge of the virus was high across the continent, so too was acceptance of false claims and conspiracies. 11 The infographic below lays out the results of the perceptions survey, and the challenge posed by false narratives becomes immediately clear. PERC: Responding to COVID-19 in Africa. What this infographic also clearly outlines is where public-health messaging needs to be focused to achieve positive public-health outcomes in tackling COVID-19. Dr Muyembe noted that community engagement in DRC played a key role in strengthening the uptake of (and proper adherence to) measures like social distancing, PPE, mask usage, handwashing, and public space and gatherings protocols. Reinforcing these messages in communities ultimately became the cornerstone of the DRC’s early success to keep COVID-19

transmission rates down. As has been shown to work across most of Africa, church and faith leaders proved critical in disseminating public health messaging, challenging and rejecting false narratives, and thus enabling public health officials to concentrate on medical interventions, such as mass testing and patient care. Creative public health messaging initiatives included, for example, COVID-19-related health messages spray painted onto the sides of the iconic Kenyan matatus (minibuses), 12 and record numbers of listeners in Uganda tuning into COVID-19 safety messaging on more than 20 community radio channels (this reached some 82% of the population). 13 Women in particular have played a key role in shaping positive community responses – due in large part to the informal networks that women have nurtured and supported. ‘When Ghanaian Member of Parliament Dr Zanetor Agyeman-Rawlings returned to her community in March, she targeted women with messages about the importance of good hygiene to prevent the spread of COVID-19, visiting local businesses, eateries, markets, and transport hubs. She reported that women were not only receptive to the messages and understood their importance, but also began to share them across their own constituencies in their capacity as informal community leaders.’ 14 3 MAPPING ADDITIONAL HEALTH-RELATED THREATS One of the biggest challenges identified by some of the panellists was the impact of COVID-19 on other health-related issues. African countries imposed severe lockdowns to curb the spread of community transmission, which, in turn, had adverse impacts on other health-related indicators. This is in part due to the perceptions of systematic and resource vulnerabilities on the continent. ‘Sub-Saharan Africa is considered particularly vulnerable to COVID-19 because of the relatively weak health service infrastructure and low clinician–population ratios, relatively limited laboratory capacity, and a higher rate of underlying conditions including malnutrition and anaemia, HIV/AIDs, and chronic respiratory conditions due to tuberculosis and air pollution.’ 15 As Dr Obuku pointed out in his presentation, the first 34 days of the COVID- 19-related lockdown saw 418 malaria deaths recorded in Uganda. In addition, data showed a marked drop in detected cases of malaria in the first quarter of 2020 as compared to 2019 – which was again a function of closed health centres and data not being recorded as a result. Dr Obuku also referenced a drop in mothers attending hospitals for caesarean births (while corresponding maternal deaths also went up). Official data from the Ugandan Ministry of Health showed a 29% reduction in healthcare facility deliveries in March 2020 (as compared with January 2020), and an 82% increase in maternal mortality over the same period. 16
Researchers have also explored how the growing ‘prevalence of human immunodeficiency virus (HIV) and tuberculosis (TB) in sub-Saharan Africa [could have] serious implications for those carrying either and often both conditions’. 17 As a result, anyone who is affected by either of these two conditions is immediately vulnerable to COVID-19. Moreover, the lockdown is likely to affect the supply and access to critical preventive medication, which in turn will have long-term implications on health systems in Africa. ‘A recent study that modelled the impact of COVID-19 on the interruption of HIV/AIDS, tuberculosis (TB) and malaria services in low-income and middle-income countries predicted a 10%–36% increase in related deaths over a 5-year period.’ 18 Other studies have found that ‘immunization programmes will likely be disrupted and the longer-term results of this are unpredictable in younger children’. 19 This has the potential to expose many more young people to infection by malaria, TB and HIV, and consequently, their risk of COVID-19 also increases exponentially. Given the predominantly lower average median population age of most African countries, a far greater share of the continent could be exposed to a higher risk factor from COVID-19. Moreover, research also suggests that deaths prevented by continuing routine childhood immunization initiatives in Africa far outweighs the risk of COVID-19 infection (and deaths) as a consequence of relaxing lockdown measures and keeping vaccination centres open. ‘Routine childhood immunisation should be sustained in Africa as much as possible, while considering other factors such as logistical constraints, staff shortages, and reallocation of resources during the COVID-19 pandemic.’ 20 Based on this emerging evidence, Dr Obuku concluded that it is imperative that public health authorities should include consideration of other disease- combating initiatives in an integrated way when developing strategies to address epidemics such as COVID-19. Doing so would safeguard ‘victories’ achieved through investments in combating other long-term diseases. Moreover, longer-term investments in healthcare should also aim to increase public health capacities over time in the way that Uganda has done since 2015 – increasing ambulances, adding ICU beds, reviving community strategies and putting the health sector into the heart of Uganda’s development agenda. 4 THE IMPACT OF COVID-19 ON WOMEN IN SUB-SAHARAN AFRICA Although sex-disaggregated data for COVID-19 shows roughly equal numbers of cases between men and women, each of the speakers on the panel pointed to evidence that illustrates the disproportionate impact the pandemic (and the responses to it by governments) has had on women and girls in sub-Saharan Africa. Some of these include (but are not limited to):

• A marked increase in physical violence. • Loss of income. • Increased care responsibilities and household work. • Reversals in women’s health-related progress. • Impacts on access to education and attainment. Perhaps the single greatest threat faced by women during the COVID-19 pandemic has been the horrific surge in gender-based violence and domestic abuse. ‘In the first half of this year, Liberia recorded a 50% increase in GBV and more than 600 reported rape cases. In Kenya, local media reported almost 4,000 schoolgirls becoming pregnant when schools were closed during the lockdown.’ 21 In South Africa, the lockdown had profound implications on women. ‘[T]he [South African] police force’s gender-based violence hotline received 2,300 calls in the first five days of lockdown – nearly three times the rate prior to lockdown.’ 22 According to Siphokazi Mthathi, Executive Director of Oxfam South Africa, the South African lockdown resulted in increased vulnerability of women who were reliant on the informal economy. The economic impacts of the pandemic on women have been particularly acute – due in large part to women losing their livelihoods faster because of being over-represented in sectors that have been the hardest hit by the pandemic. Estimates from UN Women show that in the first month of the pandemic, women workers in sub-Saharan Africa lost as much as 81% of their incomes. 23 Across all low- and middle-income countries (LMICs), some 92% of women earn their income from informal sources, such as small-scale farming, family businesses, market or street vending and domestic service. 24 Moreover, the majority (70%) of front-line community health workers and first responders in sub-Saharan Africa are women, which significantly increased their exposure to the COVID-19 virus. 25 In addition to discussing women being over-represented in the paid care work sector, speakers on the panel also reflected on the increased unpaid care responsibilities on women as the lockdowns took hold across Africa. Here too, women shoulder the majority of the burden of heath and domestic care responsibilities. So extensive is this burden that researchers have estimated that ‘women’s unpaid contributions to health care equate to 2.35 per cent of global GDP or the equivalent of US$1.488 trillion. This includes health promotion and prevention activities, care for persons with disabilities and chronic diseases and assistance to older persons in activities of daily living. When women’s contribution to all types of care (not just health care) is considered, this figure rises to a staggering US$11 trillion or 9 per cent of global GDP.’ 26 In addition, as lockdowns cut off access to additional formal and informal childcare arrangements, the burden is again borne disproportionately by women in providing these arrangements. In situations where women are able to work remotely, the additional care responsibilities are likely to affect physical and mental well-being. 27 Beyond the health-related implications that the COVID-19 virus is directly responsible for, women face knock-on health-related impacts as a result of the socio-economic and societal disruptions. As has already been discussed
in the previous section, data from sub-Saharan Africa is showing worrying trends in diminished access to antenatal and postnatal care, and this in turn is leading to significantly higher maternal mortality rates since the start of the pandemic. Moreover, the UNFPA estimates that as many as 51 million women in 114 LMICs were projected to be unable to use modern contraceptives if lockdowns were to last up to six months, with major disruptions to services. 28 This could result in a considerable spike of unintended pregnancies in LMICs across the same parameters, numbering between 325,000 and 15 million. 29 Initiatives to close the educational gap between girls and boys in Africa has also been immeasurably compromised by the pandemic. Based on data from the Ebola crisis, estimates suggest that in LMICs, up to ‘10 million more secondary school-aged girls could be out of school following the crisis’. 30 The effects are likely to be as profound among educators as well. One report found that following on from the Ebola crisis, only 14% of primary school teachers in Liberia were women – which reflected the double burden on female teachers of managing the personal impact of disease alongside caring for children and sick relatives. 31 Funding gaps are also likely to hit education sectors hard in African countries, as governments attempt to come to grips with the fallout of the pandemic. Here too, cautionary experience suggests that reduced public funding for the education sector has worse implications for girls than boys, serving to exacerbate the effects of interrupted learning and early school dropout. 32 Case study: Gendered disparities of online learning during the Ebola crisis ‘Evidence suggests that the online learning approach, adopted by many countries to reduce the impact of school closures, might increase gender gaps in education. In a study about online learning during the Ebola crisis in Sierra Leone, it was found that only 15% of surveyed girls mentioned participating in home study, compared to 40% of boys (Plan International, 2020a). This could be a result of girls having less access to technology than boys. Boys are one and a half times more likely to own a mobile phone compared to girls (Girl Effect and Vodafone Foundation, 2018), and women are 33% less likely to use the internet than men (Malala Fund, 2020). It could also indicate that girls were unable to participate in online learning due to taking on domestic chores, family care and income generating activities to support the family (Malala Fund, 2020).’ Excerpt from Geraldine Hutchinson and Tal Rafaeli, The Secondary Impacts of COVID-19 on Women and Girls in Sub-Saharan Africa. K4D Knowledge, Evidence, and Learning for Development, Helpdesk Report, p.6.
5 FOOD SECURITY AND NUTRITION Rev. Lubaale explored considerations of food security and nutrition in relation to additional health implications of the COVID-19 lockdown. He noted that nutrition was a key tool in the fight against HIV/AIDS and that adequate nutrients were part of effective treatment. The lockdowns imposed across African countries had significant impacts on food security. ‘Increases in infant malnutrition and stunting through economic impact of the response […] will have impact for years to come. The World Food Program predicts up to 130 million additional people will face acute food insecurity globally, a large proportion in sub-Saharan Africa.’ 33 Rev. Lubaale also noted that lockdown measures intended to contain COVID-19 have inadvertently weakened informal resilience capacity and safety nets in sub-Saharan Africa. Reduced productivity in the informal sector – on which a majority of people rely for their livelihoods – was not subsequently matched by state-based formal social protection measures. Moreover, rural communities have not had access to resources made available to urban populations to withstand the socio- economic impact of the pandemic. As a result, Rev. Lubaale and Ms Mthathi were both in agreement that the one thing COVID-19 has done is to lay inequalities bare and to significantly exacerbate existing fragilities in Southern Africa. Ms Mthathi reflected on the inadequacies of the South African government-led social protection schemes launched to tackle COVID-19. That some 45 million people in Southern Africa were already experiencing food insecurity between January and March 2020 – before the onset of the pandemic – is one reason why an ‘epidemic of hunger’ has also spread across the region. 34 Combined with the existing risks of climate change – which in 2019 devastated crops in southern Africa – there is potentially a greater crisis brewing that threatens to overwhelm formal and informal resilience capacity. 6 GAPS AND ADDITIONAL SUPPORT 6.1 ACCESS TO SAFE VACCINES Following on from the successive announcements of viable vaccines in November 2020, all 47 countries in the WHO African Region have received WHO’s Vaccine Readiness Assessment Tool, which covers 10 key areas, including: ‘planning and coordination, resources and funding, vaccine regulations, service delivery, training and supervision, monitoring and evaluation, vaccine logistics, vaccine safety and surveillance and
communications and community engagement.’ 35 Though follow-up analysis of actual levels of preparedness are worrying – WHO data suggest only a 33% readiness in the region for vaccine rollout – some countries are well on their way. Dr Jallah spoke about Liberia’s planning processes to both get access to vaccines as well as establish effective mechanisms to deliver the doses to all corners of the country. In particular, she reflected on lessons learned from the Ebola crisis, and spoke to specific logistical challenges around purchasing, partnerships and storage of the vaccine. In order to make the public immunization campaign a success, WHO guidelines suggest some two-thirds of Africa’s 1.2 billion population will require the vaccine – and that will require huge investment and the overcoming of substantial logistical challenges. 36 Dr Jallah, Dr Muyembe and Ms Mthathi all touched on suspicions that some segments of the population in their respective countries have had about the vaccine – and all pointed to the importance of the role of community-based health workers and community and religious leaders in dispelling these myths and allaying fears. Promoting community ownership of the strategy to vaccinate the population, building (and maintaining) trust, effective targeting and prioritization of high-risk members of the population, and ensuring effective two-way communication mechanisms are all elements of strategies that have worked effectively to tackle misconceptions and misinformation. Ms Mthathi emphasized that the response to the pandemic cannot be top-down, and that taking a participatory human rights-based approach (rather than a command and control approach) is the most effective way forward. The next biggest challenge is procuring enough doses for the continent. In a recent article, the People’s Vaccine Alliance revealed that ‘nine out of 10 people in 70 low-income countries are unlikely to be vaccinated against Covid-19 next year because the majority of the most promising vaccines coming on-stream have been bought up by the west’. 37 Moreover, ‘rich countries with 14% of the world’s population have secured 53% of the most promising vaccines’. 38 To combat this, one of the vaccine developers has earmarked 60% of all stocks to be made available for LMICs, but this is not likely to fill the gap. ‘COVAX, the Gavi-led financing mechanism to provide COVID-19 vaccines [to LMICs], plans to have 2 billion doses of vaccine available by the end of 2021.’ 39 Given the inequalities already laid bare by the COVID-19 pandemic, Ms Mthathi stressed the need to follow a path that replaces the traditional profit-making model to that of a public good model – given that the funding for the vaccines has been derived from public funds. Ensuring that vaccines are widely available (and by extension affordable) will also have positive public health implications, as immunity will be built globally, and in turn will prevent pockets of outbreaks from overwhelming the global capacity to respond.
6.2 ADDITIONAL SUPPORT FOR SOCIAL PROTECTION The pandemic has exposed severe inequalities in many parts of the world, not least in sub-Saharan Africa. As noted by Ms Mthathi and Rev. Lubaale, the crisis presents policy makers and political leaders with a unique opportunity to ensure that the rebuilding of societies follows a ‘Just Recovery’ model. The Sustainable Development Goals (SDG) agenda provides a good entry point, and can serve to catalyse a UN-led response that is couched in the SDGs. Important government social protection tools, such as Universal Basic Income, must be reimagined so as to go beyond providing insignificant palliative care amounts. This will require policy makers to go beyond the default consumption-driven economic model that has so grossly exacerbated inequalities in Africa and other parts of the world. Rev. Lubaale identified specific challenges with service delivery and targeting of limited resources and questioned whether current models of social protection are effective in tackling such fundamental upheavals. He referenced the example of women smallholder farmers in rural Uganda who were able to escape being infected by COVID-19, but were locked down and unable to physically travel to their farms. He argued for a move towards food sovereignty so that global shocks, such as the COVID-19 lockdowns, do not diminish local resilience capacities and adversely affect local-level access to food and other resources. 6.3 RISK MANAGEMENT (SECOND WAVE) AND ENFORCEMENT Dr Muyembe, Dr Jallah and Dr Obuku all reflected on the specific challenges of enforcement of social distancing and public health measures during lockdowns. Dr Jallah found that in Liberia, because of the socio-economic burdens that the population experience, it became increasingly difficult for people to abide by the health protocols and respect the rules of the lockdown. Once the lockdown was eased, schools went back into session and churches were able to open. Dr Jallah again reflected on the importance of the community-based public health cadre, especially in reinforcing messaging such as proper use of masks, handwashing, maintaining distance and following all isolation and tracing protocols if infected. Dr Muyembe also identified similar challenges in the DRC, and explored the origin of some of the country’s infection clusters (i.e. predominantly wealthy travellers to European countries who tested positive upon return to the DRC).
CONCLUSIONS The distinguished panel of speakers provided excellent insights into the successes and challenges of the African response to the COVID-19 pandemic. Key among them were: • Difficult yet meaningful lessons were learned from the Ebola crisis, which enabled African countries to prepare inter-agency coordination mechanisms and standard operating procedures and protocols to tackle serious public health emergencies. Once the COVID-19 pandemic hit, most African countries were able to operationalize existing mechanisms and mobilize pre-positioned capacities – which undoubtedly played a key role in keeping infection at bay during the first half of 2020. • Community engagement, partnership and coordination were key to tackling misinformation, gaining trust and amplifying basic public health messaging around masks, hand-washing and social distancing. • Given the overwhelming nature of the pandemic, many countries neglected the impacts of other diseases (such as malaria, TB and HIV/AIDS), which has led to a surge in deaths and presented complications in the treatment of COVID-19 in patients who have also contracted one of these existing diseases/conditions. • Women have been disproportionately affected by the pandemic in Africa. From facing unprecedented levels of gender-based violence to losing the majority of their income as a result of lockdowns, African women have faced multiple crises simultaneously. This has been exacerbated by additional unpaid care responsibilities during lockdowns, lack of access to contraception and other health care products, and increased barriers to education access. • COVID-19 has had profound implications on food insecurity on the continent, which was further aggravated by climate-related droughts and crop failures from previous years. • Access to vaccines will remain a challenge long into 2021, as the cost and availability continue to be dictated by free-market forces, which severely disadvantage African countries. • ‘Building back better’ will require a fundamental shift in policies, tactics and approaches – a human rights based ‘Just Recovery’ model should serve as the starting point for policy makers.
ANNEX: BIOGRAPHIES OF PANELLISTS Name and affiliation Photo Dr Jean-Jacques Muyembe Tamfum, Director General, National Institute for Biomedical Research, Professor of Microbiology at Kinshasa University Medical School, DRC Mr Muyembe is a Congolese microbiologist. He was part of team at the Yambuku Catholic Mission Hospital that investigated the first Ebola outbreak. In 2016, he led the research that designed, along with other researchers, one of the most promising treatments for Ebola. Dr David Nabarro, UN WHO Covid-19 Special Envoy Mr Nabarro is a medical doctor who has made his career in the international civil service, working for either the Secretary-General of the United Nations or the Director General of the World Health Organization. Most recently, from February 2020 he has helped the DGWHO deal with the COVID-19 pandemic. Hon. Dr Wilhelmina Jallah, Minister of Health, Liberia Dr Jallah is a medical doctor with over 25 years of national and international work experience in clinical services and public health management. She is the Chair of the country’s Incident Management System (IMS) and is responsible for the implementation of the country’s national COVID-19 Preparedness and Response strategy. Siphokazi (Sipho) Mthathi, Executive Director of Oxfam South Africa Ms Mthathi is the founding ED of Oxfam South Africa and has two decades of experience in the human rights, development and social justice movement in Southern Africa. Previously, she served in positions including General Secretary of the Treatment Action Campaign and the South Africa Director of Human Rights Watch.
Dr Ekwaro Obuku, physician, researcher and academic Dr Obuku is a Ugandan health policy expert, who in the past has been the president of the Uganda Medical Association, championing the interests of medical doctors in the country. He is currently a PhD candidate at Makerere University College of Health Sciences, in collaboration with McMaster University. Rev. Nicta Lubaale, General Secretary of OAIC Reverend Lubaale is the General Secretary of the Organization of African Instituted Churches. His career has focused on action programmes and reforms for smallholder farmers, and he has been pushing for the integration of agriculture in the interventions against the COVID-19 virus. Co-moderator: Dr Michael Jennings, Reader at SOAS Dr Jennings is a lecturer and researcher in East African politics and the politics of development. A major focus of his work has been on the role of voluntary agency activity in development in East Africa, including NGOs, missions and faith-based organizations more widely. Co-moderator: Abby Maxman, President and CEO, Oxfam America Ms Maxman has more than 30 years of experience in international humanitarian relief and development. She has particular experience in gender and power in social change, and humanitarian preparedness and response.
REFERENCES Abbas, K., Procter, S. R., van Zandvoort, K., Clark, A., Funk, S., Mengistu, T., Hogan, D., Dansereau, E., Jit, M., and Flasche, S. (2020). Routine childhood immunisation during the COVID-19 pandemic in Africa: a benefit–risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. The Lancet 8 (10): E1264– E1272. https://www.thelancet.com/journals/langlo/article/PIIS2214- 109X(20)30308-9/fulltext Azcona, G. (2020). From Insight to Action: Gender Equality in the Wake of COVID-19. UN Women, 2020. https://www.unwomen.org/- /media/headquarters/attachments/sections/library/publications/2020/g ender-equality-in-the-wake-of-covid-19-en.pdf?la=en&vs=5142 Bell, D., Schultz Hansen, K., Kiragga, A. N., Kambugu, A., Kissa, J., and Mbonye, A. K. (2020). Predicting the Impact of COVID-19 and the Potential Impact of the Public Health Response on Disease Burden in Uganda. The American Society of Tropical Medicine and Hygiene. 103(3): 1191–1197. https://www.ajtmh.org/content/journals/10.4269/ajtmh.20-0546 Boseley, S. (2020). Nine out of 10 in poor nations to miss out on inoculation as west buys up Covid vaccines. The Guardian, 9 December 2020. https://www.theguardian.com/society/2020/dec/09/nine-out-of-10-in- poor-nations-to-miss-out-on-inoculation-as-west-buys-up-covid- vaccines Chan, M. (2015). Learning from Ebola: readiness for outbreaks and emergencies. Bulletin of the World Health Organization. 93(12); 818. December 2015. https://www.who.int/bulletin/volumes/93/12/15- 165720/en/ Cochran, J., Diallo, B., Qayum, S., Seth, A., Staab, S., and Azcona, G. (2020). COVID-19 and the Care Economy: Immediate Action and Structural Transformation for A Gender-Responsive Recovery. UN Women, Policy Brief 16, 2020. https://www.unwomen.org/- /media/headquarters/attachments/sections/library/publications/2020/p olicy-brief-covid-19-and-the-care-economy-en.pdf?la=en&vs=407 Faciolince, M. (2020). #PowerShifts Resources: The Virus of Gender- Based Violence. From Poverty to Power blog. 25 November 2020. Accessed 27 November 2020. https://oxfamblogs.org/fp2p/powershifts-resources-the-virus-of- gender-based-violence/ 18
Fry, L. and Lei, P. (2020). Girls’ Education and COVID-19: What Past
Shocks Can Teach Us About Mitigating the Impact of Pandemics.
Malala Fund.
https://downloads.ctfassets.net/0oan5gk9rgbh/6TMYLYAcUpjhQpXLD
gmdIa/dd1c2ad08886723cbad85283d479de09/GirlsEducationandCO
VID19_MalalaFund_04022020.pdf
Haider, N., Osman, A.Y., Gadzekpo, A., et al. (2020). Lockdown
measures in response to COVID-19 in nine sub-Saharan African
countries. BMJ Global Health 2020. 5:e003319.
https://gh.bmj.com/content/bmjgh/5/10/e003319.full.pdf
Harrisberg, K. (2020). Murders of South African Women Surge as 9-
Week Lockdown Eases. Global Citizen. Thomson Reuters
Foundation, 23 June 2020.
https://www.globalcitizen.org/en/content/gender-violence-covid-19-
lockdown-south-africa/
Hutchinson, G. and Rafaeli, T. (2020). The Secondary Impacts of
COVID-19 on Women and Girls in Sub-Saharan Africa. K4D,
Knowledge, Evidence, and Learning for Development, Helpdesk
Report. 8 June 2020.
https://resourcecentre.savethechildren.net/node/18153/pdf/830_covid
19_girls_and_women_ssa.pdf
Internews. (2020). Mobilizing a Network of Women to Get COVID-19
Information to Rural Villages. 10 September 2020. Accessed 27
November 2020. https://reliefweb.int/report/democratic-republic-
congo/mobilizing-network-women-get-covid-19-information-rural-
villages
ITUC-Africa. (2020). COVID-19 – Response from Liberia. In African
Responses to the COVID-19 Health Crisis and the Role of Trade
Unions (Vol. 2) Newsletter Special Edition, African Regional
Organisation of the International Trade Union Confederation, No.
018/06/2020: 157–162; http://www.ituc-
africa.org/IMG/pdf/newsletter_anglais.pdf
Johnson Sirleaf, E. (2020). Opinion: African women are leading the fight
against COVID-19. Devex. 03 September 2020.
https://www.devex.com/news/opinion-african-women-are-leading-the-
fight-against-covid-19-97980
The Lancet. (2020a). Lancet COVID-19 Commission Statement on the
occasion of the 75th session of the UN General Assembly. The Lancet
COVID-19 Commissioners, Task Force Chairs, and Commission
Secretariat. October 2020; 396: 1102–2410.
https://www.thelancet.com/action/showPdf?pii=S0140-
6736%2820%2931927-9
The Lancet. (2020b). An African plan to control COVID-19 is urgently
needed. The Lancet 5 December 2020; 396: 1777.
https://www.thelancet.com/action/showPdf?pii=S0140-
6736%2820%2932580-0
19Makerere University. (2020). COVID-19 evidence team established at the Africa Centre MakCHS. Makerere University College of Health Sciences. Accessed 25 November 2020. https://chs.mak.ac.ug/news/covid-19-evidence-team-established- africa-centre-makchs Molyneux, D.H., Aboe, A., Isiyaku, S., and Bush, S. (2020). COVID-19 and neglected tropical diseases in Africa: impacts, interactions, consequences. International Health 2020; 12: 367–372. https://academic.oup.com/inthealth/article- pdf/12/5/367/33677254/ihaa040.pdf PERC. (2020a). Partnership for Evidence-Based Response to COVID-19 (PERC). Accessed 1 December 2020. https://preventepidemics.org/covid19/perc/ PERC. (2020b). Responding to COVID-19 in Africa: Using Data to Find a Balance. Partnership for Evidence Based Response to COVID-19 (PERC). https://preventepidemics.org/wp- content/uploads/2020/05/PERC_Regional_5-6-2020.pdf UNFPA. (2020). Impact of the COVID-19 pandemic on family planning and ending gender-based violence, female genital mutilation and child marriage. Interim Technical Note, UNFPA, 27 April 2020. https://www.unfpa.org/sites/default/files/resource-pdf/COVID- 19_impact_brief_for_UNFPA_24_April_2020_1.pdf UNGC. (2020). Learning from the past: UN draws lessons from Ebola, other crises to fight COVID-19. UN Department for Global Communications, 13 May 2020. https://www.un.org/en/coronavirus/learning-past-un-draws-lessons- ebola-other-crises-fight-covid-19 Water Action Hub and UN Global Compact. (2020). National Public Health Institute of Liberia. Accessed 26 November 2020. https://wateractionhub.org/organizations/927/d/national-public-health- institute-of-liberia/ WHO. (2020a). Kenya’s public minibuses help drive the COVID-19 prevention message home. World Health Organization, 28 October 2020. Accessed 3 December 2020. https://www.who.int/news- room/feature-stories/detail/kenya-s-public-minibuses-help-drive-the- covid-19-prevention-message-home WHO. (2020b). EU and WHO working together to defeat COVID-19 in Kenya. World Health Organization, 30 June 2020. Accessed 3 December 2020. https://www.who.int/news-room/feature- stories/detail/eu-and-who-working-together-to-defeat-covid-19-in- kenya 20
WHO. (2020c). WHO urges African countries to ramp up readiness for
COVID-19 vaccination drive. World Health Organization, 26
November 2020. Accessed 9 December 2020.
https://www.afro.who.int/news/who-urges-african-countries-ramp-
readiness-covid-19-vaccination-drive
NOTES
1 Chan, M. (2015). Learning from Ebola: readiness for outbreaks and emergencies.
Bulletin of the World Health Organization. 93(12): 818. December 2015, p.818.
2 Johnson Sirleaf, E. (2020). Opinion: African women are leading the fight against
COVID-19. Devex. 3 September 2020.
3 Water Action Hub and UN Global Compact. (2020). National Public Health Institute of
Liberia.
4 ITUC-Africa. (2020). COVID-19 – Response from Liberia. In African Responses to the
COVID-19 Health Crisis and the Role of Trade Unions (Vol. 2). Newsletter Special
Edition, No. 18/06/2020, pp.157–162.
5 Director General, National Institute for Biomedical Research, Professor of Microbiology
at Kinshasa University Medical School in DRC.
6 Makerere University. (2020). COVID-19 evidence team established at the Africa Centre
MakCHS. Makerere University College of Health Sciences.
7 UNGC. (2020). Learning from the past: UN draws lessons from Ebola, other crises to
fight COVID-19. UN Department for Global Communications, 13 May 2020.
8 Ibid.
9 The Lancet. (2020a). Lancet COVID-19 Commission Statement on the occasion of the
75th session of the UN General Assembly. The Lancet COVID-19 Commissioners,
Task Force Chairs, and Commission Secretariat, 10 October 202; 396: p.1107.
10 Internews. (2020). Mobilizing a Network of Women to Get COVID-19 Information to
Rural Villages. 10 September 2020.
11 PERC (Partnership for Evidence-Based Response to COVID-19) is a ‘public-private
partnership that supports evidence-based measures to reduce the impact of COVID-
19 on AU Member States’. PERC. (2020b). Responding to COVID-19 in Africa: Using
Data to Find a Balance, p.9.
12 WHO. (2020a). Kenya’s public minibuses help drive the COVID-19 prevention
message home. 28 October 2020.
13 WHO. (2020b). EU and WHO working together to defeat COVID-19 in Kenya. 30 June
2020
14 Johnson Sirleaf, E. (2020).
15 Bell, D. et. al. (2020). Predicting the Impact of COVID-19 and the Potential Impact of
the Public Health Response on Disease Burden in Uganda. The American Society of
Tropical Medicine and Hygiene 103(3): 1191.
16 Ibid., p.1193.
17 Molyneux, D.H., et al. (2020). COVID-19 and neglected tropical diseases in Africa:
impacts, interactions, consequences. International Health 12: pp.367–372.
18 Haider, N., Osman, A.Y., Gadzekpo, A., et al. (2020). Lockdown measures in
response to COVID-19 in nine sub-Saharan African countries. BMJ Global Health
2020(5): p.9.
19 Molyneux et al. (2020), p.367.
2120 Abbas et al. (2020). Routine childhood immunisation during the COVID-19 pandemic in Africa: a benefit–risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. The Lancet 8(10): pp.1264–1272. 21 Faciolince, M. (2020). #PowerShifts Resources: The Virus of Gender-Based Violence. From Poverty to Power blog, 25 November 2020. 22 Harrisberg, K. (2020). Murders of South African Women Surge as 9-Week Lockdown Eases. Thomson Reuters Foundation, 23 June 2020. 23 Azcona, G. (2020). From Insight to Action: Gender Equality in the Wake of COVID-19. UN Women, p.4. 24 Cochran, J., et al. (2020) COVID-19 and the Care Economy: Immediate Action and Structural Transformation for A Gender-Responsive Recovery. UN Women, Policy Brief 16, p.3. 25 Ibid. 26 Ibid., pp.2–3. 27 Ibid. 28 UNFPA (2020) Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-based Violence, Female Genital Mutilation and Child Marriage. Interim Technical Note, UNFPA, 27 April 2020, p.3. 29 Ibid. 30 Fry, L. and Lei, P., (2020) Girls’ Education and COVID-19: What Past Shocks Can Teach Us About Mitigating the Impact of Pandemics. Malala Fund, p.5. 31 Ibid., p.5. 32 Ibid., p.6. 33 Bell, D. et. al. (2020), p.1195. 34 Hutchinson, G. and Rafaeli, T. (2020). The Secondary Impacts of COVID-19 on Women and Girls in Sub-Saharan Africa. K4D, Knowledge, Evidence, and Learning for Development, Helpdesk Report, p.13. 35 WHO .(2020c). WHO urges African countries to ramp up readiness for COVID-19 vaccination drive. World Health Organization, 26 November 2020. 36 Ibid. 37 Boseley, S. (2020.) Nine out of 10 in poor nations to miss out on inoculation as west buys up Covid vaccines. The Guardian, 9 December 2020. 38 Ibid. 39 The Lancet. (2020b). An African plan to control COVID-19 is urgently needed. The Lancet. 5 December 2020. 396: p.1777. 22
OXFAM
Oxfam is an international confederation of 21 organizations networked together
in 67 countries, as part of a global movement for change, to build a future free
from the injustice of poverty. Please write to any of the agencies for further
information, or visit www.oxfam.org
Oxfam America (www.oxfamamerica.org) Oxfam India (www.oxfamindia.org)
Oxfam Australia (www.oxfam.org.au) Oxfam Intermón (Spain)
Oxfam-in-Belgium (www.oxfamsol.be) (www.oxfamintermon.org)
Oxfam Brasil (www.oxfam.org.br) Oxfam Ireland (www.oxfamireland.org)
Oxfam Canada (www.oxfam.ca) Oxfam Italy (www.oxfamitalia.org)
Oxfam Colombia (lac.oxfam.org/countries/colombia) Oxfam Mexico (www.oxfammexico.org)
Oxfam France (www.oxfamfrance.org) Oxfam New Zealand (www.oxfam.org.nz)
Oxfam Germany (www.oxfam.de) Oxfam Novib (Netherlands)
Oxfam GB (www.oxfam.org.uk) (www.oxfamnovib.nl)
Oxfam Hong Kong (www.oxfam.org.hk) Oxfam Québec (www.oxfam.qc.ca)
Oxfam IBIS (Denmark) (www.oxfamibis.dk) Oxfam South Africa (www.oxfam.org.za)
KEDV (www.kedv.org.tr)
www.oxfam.orgYou can also read

















































