BE THE BOSS OF YOUR BENEFITS - 2021 BENEFITS GUIDE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

B E T H E B O S S O F Y O U R B E NEFITS 2021 BENEFITS GUIDE
Be the BOSS of your benefits!
Investing in your health starts with a great benefits package. At Mission What you need to enroll
Health, providing you with a robust benefits package that gives you
choices and flexibility is one way we invest in our team members. Knowing 1. Are you eligible for benefits?
you have options with your health, financial security, work-life balance and
retirement is one of many ways you can be the boss of your benefits! ■ Employees: You are eligible if you are budgeted to work
20+ hours per pay week or 40+ hours per pay period. PRN
Review your options and take advantage of the resources available to help employees and contract or leased employees are not eligible
you and your family make informed choices. Getting the most out of your for benefits. You are full-time if you are budgeted as 0.875-
healthcare investments start with maintaining your good health and being
1.0 full time equivalent (FTE). You are part-time if you are
thoughtful about how you use your healthcare resources. Read through
this guide and learn about what benefits are available to you.
budgeted as 0.5-0.874 FTE.
■ Dependents*:
o Legal spouse
It’s All Inside... o Children through the end of the month in which they turn 26
o Children included under a Qualified Medical Child Support
What you need to enroll. . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Order
Own your benefist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 o Adopted children, stepchildren, foster children or children
for whom you are considered their legal guardian
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 o Children age 26 or older who are supported by you and
Health Plan Options. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 incapable of self-sustaining employment due to a mental or
physical handicap
2021 Health Plan Premiums. . . . . . . . . . . . . . . . . . . . . . . . 9
* If you elect dependent coverage, you may be asked to
Voluntary Health Benefits & FSAs. . . . . . . . . . . . . . . . . . . 10
provide proof of your dependents’ relationships.
Dental + Vision Coverage. . . . . . . . . . . . . . . . . . . . . . . . . 11 ■ Covering your spouse on your health plan?
Life. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 o You will be required to complete the spouse questionnaire.
If your spouse is eligible for health insurance coverage
Disability. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 through his or her employer and you choose to cover them
on your Mission Health Plan, you will pay $100 per-pay-
More Valuable Benefits. . . . . . . . . . . . . . . . . . . . . . . . . . . 14 period surcharge.Top Facts to Know for 2021
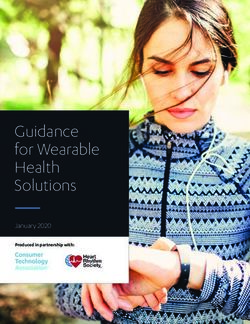
2021 Benefits Enrollment Worksheet
2. Guidelines for New Hires and Newly Eligible As you review the eMag, use this worksheet to jot down some notes to help you keep track of your decisions before you enroll.
Employees Plan
Healthcare
What I Want for 2021
MissionCare Plan (MCP)
Notes
Who do I want to cover? (myself; + 1 child; + children; + spouse; family)
Health Savings Plan (HSP) What do I want to contribute to the HSA (if enrolled in HSP)?
■ If you are a new hire, you must enroll before your benefits No Coverage
(pre-tax premium)
Do I want to contribute to the FSA (if enrolled in MCP)?
If my spouse’s employer offers coverage, it will cost $100 more each pay
effective date (benefits are effective the 31st day you are in an Accident Coverage
period to be on my plan.
Provides money to help pay for medical and out-of-pocket expenses that result
eligible status). No Coverage from an accidental injury.
(after-tax premium) Who do I want to cover? (myself; + children; + spouse; family)
Critical Illness $15,000 benefit Provides a lump sum payment after diagnosis of a covered condition .
■ If you are a rehire or an HCA Healthcare transfer, refer to your Insurance
$30,000 benefit
No Coverage
Non-Tobacco & Tobacco User rates (applies to employee's status)
Who do I want to cover? (myself; +children; +family)
(after-tax premium)
on-boarding letter for information about your enrollment Hospital Indemnity Coverage Provides coverage to help pay for hospitalization.
Who do I want to cover? (myself; +child(ren); +spouse; +family)
deadline. Your benefits may be effective immediately and you No Coverage
(after-tax premium)
Healthcare Spending May not be used if you sign up for the HSP or are enrolled in another high
may only have 14 days to enroll. Account
Election: _________
No Coverage deductible health plan.
(pre-tax premium) Must enroll each year.
■ If you don’t enroll in benefits by the stated deadlines, you will Dental
Dental
No Coverage
Who do I want to cover? (myself; + 1 child; + children; + spouse; family)
(pre-tax premium)
not be eligible to enroll again until the next annual enrollment Vision Vision Who do I want to cover? (myself; + 1 child or spouse; family)
period unless you experience a Qualifying Life Event (QLE).
No Coverage
(pre-tax premium)
QLEs include changes such as marriage, divorce, birth or
Dependent Care Election: _________ Pay for eligible dependent care expenses by contributing to the Dependent
Spending Account No Coverage Care FSA. (Not eligible if annual salary is more than $120,000)
(pre-tax premium) Must enroll each year.
adoption or loss of coverage. You will have 31 days from the Life Insurance and Additional 1 x pay Mission provides coverage for one times your base pay up to a maximum of
date of the QLE to request a change. See the “Experiencing Accidental Death &
Dismemberment*
Additional 2 x pay
Additional 3 x pay
$600,000. You can purchase additional coverage in amounts of 1, 2, 3, 4 times
your annual base pay up to a maximum of $600,000.
Some Life Changes” tab on Mission&Me for more information. Additional 4 x pay
(pre-tax premium)
Dependent Life* $30K Spouse $10K Child(ren) Life insurance coverage for your spouse and dependent children up to age 26.
$40K Spouse $5K Child(ren)
$50K Spouse (after-tax premium)
(after-tax premium)
3. Prepare for Enrollment
Short-term 40% Core (Mission provides) Consider purchasing 50% so that you are adequately covered in the event of an
Disability* 40% core + 10% emergency.
(after-tax premium)
■ Before you enroll, make sure you get the facts. Review Long-term
Disability*
40% Core (Mission provides)
40% core + 10%
Consider purchasing 50% so that you are adequately covered in the event of an
emergency.
information in this guide and other information posted on (after-tax premium)
Secure your identity with identity theft protection.
Mission&Me. Decide which benefits are best for you. Identity Theft
Employee only coverage
Employee/Dependent(s) coverage
No Coverage
■ Use this worksheet (pictured at right) to jot down some notes to Pet Insurance
(after-tax premium)
Pet Insurance If you elect to enroll, you will receive an email with enrollment instructions.
help you keep track of your decisions before you enroll.
No Coverage
(after-tax premium)
*Note: Evidence of insurability (EOI) will be required for increases in coverage after initial enrollment. Supplemental Life greater than 1 X increase
requires EOI. $30K, $40K & $50K for spouse life coverage always requires EOI.
1Own Your Enrollment
Get ready to own your benefits in 2021! Get what you want! Enroll in Mission Healthspace
before your benefits effective date.
■ If you don’t enroll before your benefits effective date, you will be
automatically enrolled in benefits as follows:
Decide which benefits are best for you Short-term Disability
40% Base Pay Replacement
Long-term Disability
Online Enrollment Steps Basic Life and AD&D 1x annual base pay
Learn more at missionandme.com > Experiencing Some Life Changes.
Enrollment must be completed through Mission Healthspace.
• From a Mission computer,
go to Mission Healthspace icon on your desktop
• From any computer, enter the Who to Contact
URL: mhs.healthspace.net/Logon/
Provider/Contact Information About Phone Website/Email
HR Direct Connect HR questions 828-213-5600 NCDV.HRDirectConnect@HCAHealthcare.com
1 Hospital Drive, 6th floor 8a-2:30p M-F
You must SUBMIT your enrollment elections before your benefits Lobby 9a-4P M-F
Accident Insurance
effective date or you will be enrolled in: Aflac
Critical Illness Insurance
800-433-3036 Aflacgroupinsurance.com
Hospital Indemnity Insurance
Long Term Disability
• No health coverage Aflac
Short Term Disability
888-862-5732 general
info
Aflaccustomersvc@disabilityrms.com
To File STD Claims: aflacclaims@disabilityrms.com
888-862-4437 STD
• 40% of base pay replacement for short- and long-term disability Claims
• Basic life and Accidental Death & Dismemberment (AD&D) insurance Child Development Child development facility for infants through 828-213-9900
Center school-age children. Rates are comparable
of 1X base pay to other local facilities and can be paid using
payroll deduction. Drop-in care is available.
On-site emergency day care on snow days is
If you need to make a change after you SUBMIT, you will need to provided.
contact HR Direct Connect at 828-213-5600 before your benefits Community Eye Care Vision Plan 888-254-4290 cecvision.com / info@cecvision.com
effective date. Please remember that your enrollment must be Employee Assistance
Network, Inc. (EAN)
Employee assistance questions, requests for
counseling (you do not have to be enrolled in
828-252-5725 http://www.eannc.com
800-454-1477
resubmitted before your benefits effective date. Mission Health Plan coverage to use the
EAN), and precertification for behavioral
healthcare benefits under the health plan.
Flores & Associates COBRA 800-532-3327
HealthSCOPE Benefits Dental, Health Savings Account (HSA) 877-226-2058 (Dental) www.healthscopebenefits.com
2Glossary
Glossary
Coinsurance – The percentage of health care cost you will pay after Mission Health Partners (MHP) – The Preferred Provider Network for
you meet the plan’s deductible. our health plan. You’ll get the most benefit from the plan when you use
Example: For 2021, MCP participants will pay 25% coinsurance after MHP providers and facilities, rather than other “In-Network” providers.
they meet the deductible; this means the health plan then will pay the
other 75% of costs. Out of Network – If you use providers and facilities that are not part
of MHP or are not otherwise designated In-Network, those services are
Copay – A fixed dollar amount that you pay for a specific medical not covered by the health plan. There are exceptions for emergencies
service.Example: For 2021, MCP participants will pay a $35 copay when and approved gap exceptions when services are not available with a
they visit their primary care provider. network provider.
Deductible – A fixed dollar amount that you must pay each calendar Out-of-Pocket (OOP) Maximum – Once your total spending for
year before the health plan shares in the cost for certain services. covered health plan benefits during the calendar year reaches this
Example: If you have single coverage in the MCP, your 2021 deductible specified amount, Mission begins to pay 100% for covered services.
will be $1,000. After you reach that deductible, you will pay 25%
coinsurance for your healthcare costs (meaning the plan will pay the Premiums you pay DO NOT count toward your OOP maximum.
other 75%).
However, these items DO count toward the OOP maximum: Payments
Formulary – A list of prescription drugs covered by your toward deductible, copayments, coinsurance (both medical and
health plan. There are three tiers of coverage (generic, preferred prescriptions covered by your plan).
brand, non-preferred brand); costs for medications may differ
Premium – The amount deducted from your bi-weekly paycheck to
depending on the tier.
purchase each of your benefits (health plan, dental, disability, etc.).
Health Savings Plan (HSP) – One of two health plans you can choose
Preventive Care – The Affordable Care Act (ACA) designates specific
for 2021. This publication includes information to help you compare
preventive services that are covered at 100% if you use a network
the two plans.
provider (MHP or in-network). These services include annual physical,
MissionCare Plan (MCP) – One of two health plans you can choose for pap tests, pelvic exams, mammogram, prostate test, colonoscopy,
2021. This publication includes information to help you compare the flu shots, well baby care, prenatal care, immunizations, etc. For
two plans. more information, view the health plan SPD or www.healthcare.gov/
preventive-care-benefits.
3Know the health plan network:
Health Plan Options Mission Health Partners: Includes Mission facilities In-Network: Includes
and Mission Health Partners providers other network providers
Health Plan Options, Prescription Drugs and Health Accounts
Our plans are designed to help you make informed decisions about healthcare based on your and your family’s needs. A critical decision around your choice is how
and when you want to spend your money. It’s up to you to learn about the plans, choose the right one for you and understand how to use it when you need care.
Be a smart healthcare consumer! Make a decision just like the one you make when buying car insurance — deciding how much you want to pay each month vs. the
amount of deductible you have to pay when you need repairs after an accident. The best choice for you depends on your previous spending patterns, finances and
comfort level.
You have two plan options. Here’s how the features compare:
MissionCare Plan Health Savings Plan MedCost is our
Third Party Administrator (TPA) for
Lower payroll contributions the health plan.
Optum RX is our
Preventive care services covered at 100% Pharmacy Benefits Manager (PBM).
Lower annual deductible
If you, your spouse or dependent
child live outside of the 17-county
Lower out-of-pocket maximum (OOPM) regional area* you will be assigned
to an expanded provider network for
Prescription drug coverage** in-network benefits. Please note that
networks will be assigned based on
individuals’ mailing zip codes, so be
HSA with Mission contributions sure to enter the related address and
zip code to your spouse or dependent
Healthcare Flexible Spending Account (FSA) available child’s information in Healthspace if
different from your address.
*17-county area includes: Buncombe, Burke, Cherokee, Clay, Graham, Haywood, Henderson, Jackson, Macon, Madison, McDowell, Mitchell, Polk, Rutherford, Swain, Transylvania, Yancey.
4 ** Out-of-Network prescription drugs are not covered.MCP
MissionCare Plan (MCP)
Plan Information
Mission Health Partners + In-Network
Employee Employee+1 Family
Deductible
You pay this amount before Mission $1,000 $1,250 $2,000
shares the cost through coinsurance.
Out-of-Pocket Maximum
Once you pay up to this amount,
$7,000 $14,000 $13,100
Mission pays 100% of the cost for
eligible expenses.
Medical Provisions
Mission Health Partners In-Network Out-of-Network
Coinsurance (applies after deductible) You 25% Mission 75% You 25% Mission 75% Not Covered
Preventive Care You 0%, no deductible Mission100%
Hospital Inpatient Facility $600 copay
X-ray / imaging - Basic $20 copay
X-ray / imaging - Complex $100 copay You 25% Mission 75%
Not Covered
Lab (Facility) $0 copay
Specialists $50 copay
Primary Care Physician (PCP) $35 copay
Hospital Outpatient Facility $225 copay – Mission Facility Only You 25% Mission 75% – MHP and In-Network
Urgent Care $50 copay $100 copay
Emergency Room Facility Non-emergency: $300 copay
Non-emergency: $300 copay • True emergency: $200 copay
(copay waived if admitted) True emergency: $200 copay
Coinsurance applies after the deductable has been met.
5Prescription Drugs for MCP Embedded Plan Features:
Mission Health Pharmacies OptumRx Network
What Do They Mean?
Deductible None Employee: $200 Family: $400 For each plan, there is an overall
Generic $0 $0
deductible and out-of-pocket
maximum (OOPM) for all of the costs
Brand Preferred $40 copay* $60 copay
(including prescriptions in the HSP)
Deductible: Employee $500 / Family $1,000, Then You pay Additional Deductible: Employee $500 / Family $1,000, Then incurred by covered individuals. An
Brand Non- 50% with a min $100 and max $200 copay You pay 60% with a min $100 and max $300 copay
Preferred embedded deductible or OOPM
Retail
Deductible will be waived for approved medical exceptions. Deductible will be waived for approved medical exceptions. means benefits could be paid by
Insulin, coinsurance or at 100% for one family
Hypoglycemics, $25 co-pay member and not all.
Non-Insulin $25 co-pay after Deductible
Injectables and $60 co-pay (Mission Mail)
These work differently for each plan:
supplies
MCP HSP
Generic** $0
Embedded
Mail Order
Yes No
Brand Preferred** $80 copay Not covered Deductible
Brand Non- Deductible: Employee $500 / Family $1,000, Then You pay Embedded
Yes Yes
Preferred** 50% with a min $200 and max $400 copay OOPM
You 10% Mission 90% Not covered unless
Specialty Drugs
Min $75 copay, max $150 copay referred by Mission pharmacy
*If a brand drug is chosen when a generic drug is available, the covered person must pay the brand drug copay and the difference in cost between the brand
See page 8 for examples of how
drug and the generic drug. these work for both plans.
**All maintenance medications must be filled as a 90-day supply under the Mission health plans and filled at a Mission employee mail-order pharmacy.
6HSP
Health Savings Plan (HSP)
Plan Information
Mission Health Partners In-Network
Deductible
You pay this amount before Mission Employee: $1,500 Family: $3,000
shares the cost through coinsurance.
Out-of-Pocket Maximum
Once you pay up to this amount,
Employee: $7,000 Family: $14,000
Mission pays 100% of the cost for
eligible expenses.
HSA Contribution (by Mission) Employee: $250 Family: $500
Medical Provisions
Mission Health Partners In-Network Out-of-Network
Coinsurance (applies after deductible) You 20% Mission 80% You 30% Mission 70%
Preventive Care You $0, no deductible Mission 100%
Hospital Inpatient Facility
Hospital Outpatient Facility Not Covered
You 30% Mission 70%
Hospital Outpatient Surgery Facility
High-Cost Radiology Facility You 20% Mission 80%
Primary Care Physician (PCP)
Specialists You 20% Mission 80%
Urgent Care You 20% Mission 80%
Non-emergency:
Non-emergency: You 30% Mission 70% You 50% Mission 50%
Emergency Room
True emergency: You 20% Mission 80% True emergency:
You 20% Mission 80%
7Prescription Drugs for HSP The Health Savings Account (HSA)
The HSP is paired with an HSA to help you save for expenses now and in the
Mission Health Pharmacies OptumRx Network future. Learn more at Missionandme.com > Total Rewards > Focusing On My
Deductible After the medical deductible has been met. Health > Health Through Insurance > Health Accounts
Generic** $0 $0 Please note you cannot enroll in the FSA for healthcare if you have an HSA.
Retail
Brand Preferred You 30% Mission 70% You 40% Mission 60%
Mission Health Contributes to your HSA!
Brand Non-Preferred You 50% Mission 50% You 50% Mission 50%
2021 HSA Employee Contribution Limits Mission Health Contribution**
Generic* $0
Employee $3,600 $250
Mail Order
Brand Preferred* You 30% Mission 70% Not covered
Family $7,200 $500
Brand Non-Preferred* You 50% Mission 50%
Catch-up Contributions* $1,000
Not covered unless referred by *If you are age 55 or older, you can make catch-up contributions to save more.
Specialty Drugs You 30% Mission 70%
Mission pharmacy **Prorated based on the month of your effective date of coverage.
*All maintenance medications must be filled as a 90-day supply under the Mission health plans and filled at a Mission employee
mail-order pharmacy.. **$0 after deductible has been met.
Embedded Plan Design Features: How Do They Work?
Embedded Deductible and Out-of-Pocket Maximum in the MCP Embedded Out-of-Pocket Maximum in the HSP
Mary is a Mission employee and is enrolled in the MCP. She gets an x-ray for a Tom, a Mission employee, is enrolled in the HSP. He has surgery and meets
foot injury and meets the individual deductible of $1,000. Additional expenses the individual OOPM of $7,000.
are paid at coinsurance and copays until she meets her OOPM of $6,550.
This means that any additional eligible expenses Mary incurs This means that all of Tom’s additional medical expenses are covered
throughout the year are paid at 100%. 100% for the remainder of the year.
$6,550 $7,000
Her husband and their daughter continue to incur an additional $1,000 in medical His wife and son continue to incur an additional $7,000 in medical expenses
expenses until the family all together meets the family deductible of $2,000. until the family all together meets the family OOPM of $14,000.
After the family deductible of $2,000 is met, any additional eligible After the family OOPM of $14,000 is met, the plan pays any additional
medical expenses are paid by coinsurance and copays until Mary’s medical expenses 100% for the entire family for the rest of the year.
8 husband or daughter meet their individual OOPM or the family OOPM. $6,550 $7,0002021 Health Plan Premiums
Know Healthcare Reform:
■ If you are eligible for Mission Health
benefits, you are not eligible for subsidies
2021 Health Plan Premiums ■
from the government
If you are NOT eligible for Mission Health
benefits, you can access coverage through
the federal government’s healthcare
exchange, or consider other sources of
coverage like your spouse’s plan, your
What You Pay in Payroll Deductions Each Pay Period (pre-tax) parent’s plan, Medicaid or Medicare
(if applicable)
Bi-weekly Premiums
Full-Time Part-Time
MCP HSP MCP HSP
Employee $41.30 $10.92 $82.68 $34.60
Employee + Spouse $162.85 $52.20 $225.21 $75.95
Employee + Child $80.27 $24.28 $116.04 $37.80
Employee + Children $134.93 $42.49 $194.98 $66.24
Family $241.95 $78.91 $323.46 $102.64
*$100 spousal surcharge not included
9Voluntary Health Benefits/FSAs
Hospital Indemnity
(Administered by AFLAC*)
This benefit pays cash when you are admitted to the hospital, and when you
remain hospitalized, including for pregnancy. Review rates and enroll in the
enrollment tool. Healthcare FSA
Learn more at Save for healthcare expenses! You are eligible if you don’t participate in the
HSP or another high-deductable plan.
Missionandme.com > Total Rewards > Managing My Financial Security >
Protecting My Finances Use your FSA debit card to pay for eligible healthcare expenses for yourself and
dependents with tax-free funds from your FSA. Contribute up to $2,750 annually.
If you don’t use your Healthcare FSA funds by the end of the year, you will
Critical Illness lose them (unless you qualify to carry over $550 to the following plan year).
(Administered by AFLAC*)
You can receive a lump-sum cash benefit of $15,000 or $30,000 following diagnosis
of a covered condition like a heart attack, cancer or stroke. Review rates and enroll
in the enrollment tool.
Learn more at
Missionandme.com > Total Rewards > Managing My Financial Security >
Dependent Care FSA
Pay for eligible dependent care expenses. Contribute up to $2,500 if single or married
Protecting My Finances and filing a separate return. Contribute up to $5,000 if married and filing a joint tax
return. The minimum pre-tax contribution per bi-weekly pay period is $10. If your annual
Accident Insurance salary is more than $120,000, you are not eligible to participate.
(Administered by AFLAC*)
Provides cash to help pay for the medical and out-of-pocket costs that add up
after an accidental injury. Even with health insurance, you may not be adequately
prepared for expenses that result from an accident. Learn More
Missionandme.com > Total Rewards > Managing My Financial Security >
Learn more at Savings and Financial Incentives > Pay Expenses with Tax-Free Dollars
Missionandme.com > Total Rewards > Managing My Financial Security >
Protecting My Finances
*Underwritten by Continental American Insurance Company (CAIC). Refer to materials for limitations and exclusions.
AGC1803479 IV (9/189)
10Dental + Vision Coverage
Dental (Administered by HealthSCOPE Benefits) Vision (Administered by Community Eye Care)
Getting regular dental care is an important part of overall health.
You’re the boss…only you can take care of your eyes!
Annual Deductible $100 individual $300 family Covered Benefits (per covered member) In-Network
Individual Annual Maximum Routine Vision Exam
$1,500 100% after $15 copay
Non-orthodontia services, preventive, diagnostic, basic, major services (once per calendar year)
Preventive and Diagnostic Services Contact lens fitting, refit or evaluation
100%, no deductible 100% after $15 copay
Exams and cleanings, fluoride treatments, x-rays for diagnosis, sealants (once per calendar year)
Basic Services After deductible Eyewear
Fillings and extractions, periodontics, repairs to crowns or dentures, $350 allowance / $15 copay
You 20% Mission 80% (once per calendar year)
endodontics, oral surgery
1
You are eligible to select either eyeglasses or contact lenses — only one service will be covered.
Major Care Services 2
If you purchase eyeglass lenses and eyeglass frames at the same time from the same network provider, only
Crowns, inlays, dentures, dental implants one copay will apply to the lenses and frames together.
You 50% Mission 50%
Orthodontia Services 3
The allowance for lenses not from the covered contact lens selection will apply at Walmart, Sam’s Club and
No age limit Costco locations.
4
Determined at the provider’s discretion. See plan details.
Orthodontia Individual Lifetime Maximum $1,500
Premiums (pre-tax)
Premiums (pre-tax) What you will pay in payroll deductions each pay period
What you will pay in payroll deductions each pay period:
Full-Time Part-Time Employee $3.81
Employee $ 4.59 $12.27 Employee + 1 $7.92
Employee + Spouse $33.63 $42.74 Family $12.31
Employee + Child $21.46 $27.29
Employee + Children $29.76 $37.82
Family $45.39 $57.68
11Life Know what’s required: Evidence of Insurability (EOI), or proof of good
health, is required if you request $40,000 or $50,000 of Spouse Life.
Life, Accidental Death and Dismemberment (AD&D) You will receive information about completing the EOI application shortly
(Administered by Prudential)
after your enrollment has been processed.
To help protect you and your family financially, Mission Health automatically
pays for Basic Life and Basic AD&D coverage of: Dependent Life
(Administered by Prudential)
Basic Life and Basic AD&D 1x Annual base pay (up to $600,000) You can purchase additional coverage for dependents. Child Life coverage
available for dependent children up to age 26.
You may also choose Supplemental Life and AD&D coverage of: Spouse $30,000, $40,000 or $50,000 Child(ren) $5,000 or $10,000 per child
Supplemental Life and AD&D Annual base pay (up to $600,000) Evidence of Insurability (EOI) EOI Requirements
1x 2x 3x 4x
Requirements • Not required for any coverage
• All new plan enrollees will require amount
Premiums* (pre-tax) EOI for coverage amounts of
$40,000 or $50,000
Questions about E O I ?
Rate: $0.149 per $1,000
Calculate your bi-weekly cost: (Your annual base pay ÷ 1,000) x $0.149 x 12 ÷ 26 • All plan enrollees will require EOI
if requesting to increase coverage Find out what’s required above.
*The cost of your supplemental life insurance is paid with pre-tax dollars.
amounts during our annual
enrollment time.
Now is your opportunity to elect up to 4X supplemental life and AD&D
coverage for yourself, or $30,000 coverage for your spouse, without Evidence
of Insurability (EOI). If you request to increase your life coverage more than
1x your annnual base pay or your spouse’s life coverage after your initial Premiums* (after-tax) Coverage Bi-weekly Cost
enrollment you will be required to complete an EOI and the increased $30,000 $5.33
coverage will not be effective until approved.
Spouse Life $40,000 $7.11
$50,000 $8.88
$5,000 $0.24
Child(ren) Life**
$10,000 $0.47
*The cost of your Dependent Life insurance is paid with after-tax dollars.
Learn More
**Rate is per family unit, regardless of number of children covered.
Missionandme.com > Total Rewards > Managing My Financial Security > Protecting My Finances
12Know what’s required: Evidence of Insurability (EOI) is required to
Disability Benefits (Administered by Aflac)
Disability Insurance
increase your coverage more than 1x for STD or LTD, life or spouse life
after your initial enrollment.
Life sometimes doesn’t go as planned…so it’s important to be prepared!
You never know when you may need to take time away from work to recover
from an illness or injury — so Mission Health offers both Short-term (STD) and
Long-term Disability (LTD) benefits just in case.
Both of your disability benefits include: Long-term Disability (LTD)
If you are absent from work due to illness or injury beyond the time covered by
■ A core benefit of 40% pay replacement covered by Mission STD (180 days), you may be eligible for LTD coverage.
■ Additional coverage purchase option of up to 50% pay replacement
■ Premiums paid with after-tax contributions (after applicable income taxes Premiums (after-tax)
have been deducted), which means if you are paid an STD or LTD benefit, the What you will pay in payroll contributions:
money you receive will not have taxes withheld at the time the benefit is paid.
Coverage Biweekly Cost Monthly Maximum Benefit*
Short-Term Disability (STD) 40% Mission pays the cost $6,500
If you are absent from work due to illness or injury for more than 14 calendar 50% (Biweekly covered base pay ÷100) x $0.55 $10,000
days, you may be eligible for STD coverage. There is a maximum 14-day waiting
*T
he monthly benefit caps for physicians are $15,000 for 40% coverage and $20,000 for
period before you will start to receive this benefit. The maximum benefit period 50% coverage (subject to 3/12 pre-existing clause).
is 24 weeks, excluding the 14-day waiting period.
Premiums (after-tax)
What you will pay in payroll contributions: Learn More
Missionandme.com > Total Rewards > Managing My Financial
Coverage Biweekly Cost Weekly Maximum Benefit Security > Protecting My Finances
40% Mission pays the cost No limit
50% (Biweekly covered base pay ÷100) x $0.380 No limit
This guide provides a summary of benefits available. It is not a legal plan document or contract, and is not intended to present all final details of the benefit plans described. Mission Health may amend or
terminate its plans at any time by its sole discretion. The descriptions of these programs, the plans themselves or participation in the plans are not an employment contract or any type of employment guarantee
and should not be considered as such. In addition to your SPDs, you can find all Summaries of Benefits and Coverage (SBCs) and Important Notices in the Resources section of MissionandMe.com. If you need
assistance or want to request printed copies of these, contact HR Direct Connect at 828-213-5600. This guide gives highlights of the Mission Health benefit programs. It is not intended to be a Summary Plan
Description (SPD) or Plan Document. If there are differences between the Guide and the SPD or Plan Document, the terms of the SPD or Plan Document will control.
Este folleto contiene un resumen en inglés de los beneficios disponibles en el Hospital Mission para los empleados. El resumen de todos los documentos del plan también está disponible en el Internet y puede
también obtener una copia impresa en la oficina de Recursos Humanos. Si usted tiene dificultad para entender cualquiera de estos documentos del plan, por favor póngase en contacto con el departamento de
intérpretes al teléfono (828) 213-0289. 13More Valuable Benefits Paid Time Off (PTO) — Relax and Recover! Adoption Assistance Mission Health’s Retirement Plan
Receive a one-hour telephonic adoption consultation You are immediately eligible to participate in the
■ You must be a full-time or part-time employee budgeted to work 20 hours
to learn more about the process, timeline and costs Mission Health 401k retirement plan – there is no
or more per week or 40 hours or more per pay period to be eligible for PTO
for adoption, locate support groups and more. waiting period. If you do not elect to participate
■ PTO is available to use the pay period of your 90th day of employment You also may be eligible to receive up to $3,500 in earlier, all new or rehired employees will automatically
■ You may use PTO to increase STD coverage to 100% for the first two reimbursement of direct adoption expenses. Call be enrolled in the plan with a 2% deferral shortly
months of disability (including the 14-day waiting period) 800-454-1477 or learn more at Missionandme.com > after 90 days. If you have .5 FTE status or greater, you
Total Rewards > Living My Life > Getting Help with receive a matching contribution from Mission after 12
PTO Accrual Life’s Challenges months of service and 1,000 hours. (PRN employees
Pay Bi-Weekly Maximum Accrual Maximum are not eligible to receive the matching contribution.)
Years of Service Periods (per 80 hours) Annual Accrual Identity Theft You will become 100% vested in the matching
Date of hire to 2 years 52 6.77 hours 22 days (176 hours) Secure your identity with Allstate Identity Protection. contributions after 3 years of vested service.
Receive identity monitoring, credit monitoring and Learn more at Missionandme.com > Total Rewards >
2 – 5 years 53 – 130 8.31 hours 27 days (216 hours) Managing My Financial Security > Preparing for
restoration services for you and your family. Review
5 – 10 years 131 – 260 9.85 hours 32 days (256 hours) rates and enroll in the Infor enrollment tool. Learn Retirement
Year 10+ 261+ 11.39 hours 37 days (296 hours) more at Missionandme.com > Total Rewards > To access your Transamerica account, learn more
Living My Life > Getting Help with Life’s Challenges about maximizing your retirement savings, name your
If hired prior to January 1, 2003: Year 14+ 365+ 12.31 hours 40 days (320 hours)
beneficiary and more, visit mission.trsretire.com or
If you are a Physician or Advanced Practitioner, you receive a Time Away From Practice benefit.
Phased Retirement call 800-755-5801.
Learn more Ease into what’s next for your life, while staying
engaged at Mission. Continue working by changing
Missionandme.com > Total Rewards > Living My Life > Taking Time
to part-time as you transition into retirement. Contact
Away from Work your manager to learn more or go to Missionandme. Employee Assistance Program
com > Total Rewards > Managing My Financial (EAP)
Security > Preparing for Retirement All employees and immediate family members
Additional HCA Benefits Available To You living in the home have access to meet with an
■ Employee Stock Purchase Plan with a 10% discount on HCA Healthcare Pet Insurance EAN counselor at no cost to you. The program is
We want to help protect all those who are most completely confidential and can be accessed by
stock. Learn more on Missionandme.com.
important to you — including your best-pet, furry calling 828-252-5725 or online at www.eannc.com.
■ Expanded education Reimbursement. Learn how you can go back to friends! Choose between a wellness plan (covers
Appointments can be made by telephone, secure
school with the HCA Healthcare Reimbursement program. services, annual vet exams and vaccinations) and
video or in person. no problem is too small or too
major medical plan (illness and injuries) from
■ Get assistance paying of your student loan. Learn more about the HCA large to get help.
Nationwide. Enroll in the Infor enrollment tool. Review
Healthcare Student Loan Assistnace Program. information at Missionandme.com > Total Rewards >
re’osre !
Protecting My Finances
Long-term care
h
T me NC 529 College Savings Plan
missionandme.com
Questions about your 2021 Mission benefits?
14 Missionandme.com > Total Rewards > My Benefits > Benefits Guide and Enrollment ResourcesYou can also read