Breast cancer in São Paulo city, Brazil An assessment of the economic impact and insights from benchmarks - A report by The Economist Intelligence ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Breast cancer in São Paulo city, Brazil
An assessment of the economic impact and
insights from benchmarks
A report by The Economist Intelligence Unit
Sponsored byBREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Contents
1. Executive summary 3
2. Introduction 5
3. Methods 6
4. The economic burden of cancer in São Paulo 10
5. Barriers to effective breast cancer care 13
6. Benchmarks 18
7. Discussion 24
A. References 28
B. Literature search methods 33
C. Summary of treatment options 34
D. Model inputs for direct costs 35
1 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Foreward
Experts providing assistance on this Project
l Dr Luiz Henrique Gebrim—Clinical Oncologist, Hospital Pérola Byington
l Dr Vilmar Marques de Oliveira—Clinical Oncologist, Santa Casa de São Paulo - Hospital Central
l Dr Gustavo Fernandes—President, Sociedade Brasileira de Oncologia Clinica, Brazil
l Professor Rodrigo Gonçalves—Instituto do Câncer do Estado de São Paulo
l Gustavo Albuquerque—Instituto do Câncer do Estado de São Paulo
l Sandra Gioia—The Brazilian National Cancer Institute (INCA)
l Dr João Bosco—Clinical Oncologist, Sociedade Brasileira de Mastologia Reg São Paulo
l Dr Pedro Henrique Arujo de Souza—Clinical Oncologist, Barretos Hospital
l Dr Bruce Mann—Professor of Surgery, The University of Melbourne, Director of Breast Tumour Stream
2 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
1. Executive summary
T he Economist Intelligence Unit (EIU) has been commissioned by the Instituto Avon to prepare this
report estimating the economic impact of breast cancer for Brazil’s largest city, São Paulo. About
12 million people live in this city in the State of São Paulo, located in the southern part of Brazil. About
30% of Brazil’s breast cancer cases occur in the State of São Paulo.1
São Paulo city has some of the best facilities to treat breast cancer in Brazil, yet diagnosis is still
often in the later stages. As well as estimating the direct and indirect costs of breast cancer in the
city based on available data, we also provide insights on the current challenges facing patients,
medical professionals, providers and policymakers. These insights were gained through interviewing
oncology specialists and the available literature. We also present two benchmarks, one local and one
international, which are providing good practice in breast cancer care, for comparison with São Paulo
city.
This report draws these strands together to give an overview of the impact of the disease, and
potential areas of improvement for São Paulo city.
Our key findings are as follows:
l We estimate the overall bill for breast cancer to be in the region of 880 million Real in São
Paulo city. This includes 861 million Real attributable to direct costs and 19.5 million Real in indirect
costs. The latter figure is largely driven by many women being diagnosed when they are of working
age, resulting in productivity losses.
l Access to medical care needs to be improved in three key areas—Increased human resources,
and increased access to medical equipment and drugs.
l Women need to be diagnosed earlier—While limited budgets and resources continue to restrict
early diagnosis, efforts to promote greater awareness among women of the signs and symptoms
of breast cancer to allow self-detection need to be ramped up, as well as making sure women are
aware they are eligible for breast cancer screening. These could be relatively cost effective ways to
improve early diagnosis.
l Partnerships between public/private institutions should be encouraged—This could provide
a way to speed up access to diagnosis and treatment.
l Adequate budget needs to be available for adherence to breast cancer management
guidelines—Healthcare budgets need to allow healthcare professionals to follow national
management guidelines, as many women may not currently be receiving the optimal care these
guidelines describe. Guidelines need to better focus limited resources on treatment and promote
multidisciplinary care.
l Patient advocacy groups can play an important role—The message is clear, that breast cancer
affects many women of working age and therefore the indirect costs are large, but awareness of
this fact is lacking. Indirect costs of this disease could be lower if more women were supported to
3 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
return to work. Advocacy groups are well-placed to meet this need but require support to take root.
In addition, patient advocacy groups could have an important role in ensuring patients get access to
important treatments and can successfully navigate a complicated system.
l Detection and treatment should not be considered the end of patient care—The needs of
patients after they have been diagnosed and treated need more attention and more resources. This
includes both improved support for palliative care and a dignified death, and meeting the needs
breast cancer survivors.
l Improving data monitoring—São Paulo State has two cancer registries, the Population Based
Cancer Registry, and Cancer Hospital Registry. However, despite the existence of these registries,
the data they produce are not always used to consistently inform decision making. If the Brazilian
Government is serious about an effective response to breast cancer, as well as all cancers, they need
to invest in better surveillance. The reasons for which are twofold, to understand the challenge they
face and to monitor the impact of any steps they take to address it.
4 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
2. Introduction
This report
B reast cancer is the most common cancer in women worldwide. Globally, a quarter of all new
cancer diagnoses in women in 2012 were breast cancer—with colorectal cancer in a distant second
place (accounting for about 9% of diagnoses).2 In Brazil in 2016, there were estimated to be 57,960 new
cases of breast cancer, representing 28.1% of all new cancer cases in Brazilian women, and an incidence
of about 56.2 cases per 100,000 women.3
Breast cancer also accounts for a large proportion of deaths from cancer among women globally
(about 15% in 2012). This equates to about half a million deaths annually.4 Five year survival rates are
relatively high, but vary substantially between countries. In 2010-2014 these rates ranged from about
90% in the US to 66% in India for women diagnosed.5 In Brazil, five year survival is towards the middle
to lower end of this spectrum, at 75%.5
There is, unfortunately, a clear breast cancer mortality gap between countries with differing levels
of development and income. Although the incidence of breast cancer in South American countries is
around half that of Northern European counties (around 52 per 100,000 compared with around 89 per
100,000 in 2012), mortality rates are similar (about 14 per 100,000 in South America and 16 per 100,000
in Northern Europe).2, 6 This underlines problems with access to health services in developing countries
such as Brazil.6 The increasing incidence of breast cancer,7 combined with the incremental costs of
emerging technologies8 places pressure on the Brazilian economy to find cost effective solutions to
manage the disease, yet few studies have assessed its financial implications. Late diagnosis and barriers
to early treatment once diagnosis is confirmed has considerable impact on this mortality gap, among
other healthcare resource restrictions attributable to the political and financial economy.9, 10
Middle income countries like Brazil often have a two tiered health care system, in which access to
diagnostic and therapeutic procedures differ greatly in the public and private healthcare systems.11 The
public system (Sistema Único de Saúde (SUS)), on which around 75% of the Brazilian population rely
for health care, unfortunately does not have the resources to diagnose and treat all the new cases of
breast cancer.12 Unlike hospitals in developed countries, which provide most, if not all care a patient
requires under one roof, in Brazil, these kinds of facilities are rare. Fragmented services, combined with
an under-resourced healthcare system, makes navigating the care pathway an exhausting mission for
patients who are already faced with physical illness and its psychological impact, causing further delays
to timely treatment.13, 14
It is clearly important to look a little closer at the impact of this disease, and current strengths and
weaknesses of those efforts to address it. For this project, we use an economic model to estimate the
direct and indirect costs of breast cancer in São Paulo city, the largest city in Brazil. We also use insights
from regional and international experts in breast cancer oncology, to inform suggestions about how
breast cancer care in São Paulo could be improved.
5 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
3. Methods
We utilised four key approaches in preparing this report:
l a review of the literature (see Appendix B for additional detail on literature searches) to identify:
¡ inputs for the economic model
¡ information relating to the diagnosis and treatment pathway for breast cancer in Brazil
¡ barriers to best quality care in São Paulo city or Brazil more widely
¡ possible benchmarks
l description of two benchmarks providing good quality breast cancer care for comparison with São
Paulo city: one Brazilian centre, and one country achieving good breast cancer survival rates
l interviews with experts in breast cancer care from São Paulo, and from the chosen benchmark
Country, Australia
l economic modelling of the current and future direct and indirect costs of breast cancer in São Paulo
city.
The methods used in the economic model are discussed further below.
Economic model
The economic model estimates the direct health care spend on breast cancer diagnosis and treatment
in São Paulo city. It is also estimates the important—but often overlooked—indirect costs of breast
cancer. These typically consist of loss of work time while employees are ill and receiving treatment,
and also loss of employees through early mortality associated with the disease. Lost productivity
attributable to cancer significantly contributes to estimates of the overall impact of cancer in a
population therefore it is important to capture this in our model.15
The model also forecasts trends in these costs over the next 5-years, based on the increase in
healthcare spending per head trajectory, and the estimated increase in breast cancer incidence in this
period.
Details of the treatment pathway for breast cancer in Brazil, and the corresponding model inputs
were obtained from published data and literature where available. This was supplemented by
information from local oncologists where needed.
Direct costs
Direct costs are the costs associated with diagnosis and treatment for each patient. The direct costs we
considered in this study were:
l Diagnosis (including mammograms, computerised tomography (CT) scans, biopsies)
l Initial medical treatments (including chemotherapy, radiotherapy, and targeted drug treatments)
l Surgery
l Maintenance treatment (hormone therapy)
l Palliative care
6 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Table 1: Data sources for the economic model
Statistic Source Year(s) of data utilised
Incident cases Instituto Nacional de Câncer (INCA) 3
2018 (estimates)
Proportion of breast cancer patients per Silva et al. 201116 2012-2013
stage Liedke et al. 201417 2008-2009
Population in São Paulo city Brazilian Institute of Geography and 2017
Statistics (IBGE)18
Treatment guidelines Brazilian Ministry of Health19 2015
US National Comprehensive Cancer 2018
Network (NCCN)20
Health care spending per head Economist Intelligence Unit projections 2018-2022
Treatment costs public sector Departamento de Informática do SUS 2018
(DataSUS)21
Kaliks et al. 201312 2013
Lee et al. 201222 2009-2011
Treatment costs private sector Brasindice table23 2017
Hierarchical Brazilian Classification of 2005
Medical Procedures (CBHPM)24
Kaliks et al. 201312 2009-2011
Incidence
As a basis for calculating the number of new breast cancer cases in São Paulo city, we used INCA’s most
recent estimates,2 of 5,900 new cases of breast cancer in 2018.
Diagnosis per stage and treatment pathway
Understanding the staging of breast cancer is important for calculating its economic impact, because
stage dictates the treatments a patient can receive, and this affects costs. Staging is based on how large
the tumour is and how much it has spread to surrounding tissue, lymph nodes and the rest of the body.
Table 2 gives brief characteristics of each stage and the treatments used at each stage. Appendix C
gives a more detailed description of these treatment options.
For the economic model we used a treatment pathway which was based on guidelines from the
Ministry of Health in Brazil,19 additional evidence from other published literature, and qualitative
insights from oncologists delivering treatment to patients with breast cancer (see Appendix D).
The specific types of drugs and cycles of treatment received are largely dependent on the resources
available in the hospital the patient is treated in. In reality, this is often a reflection of whether the
hospital is a public or private sector hospital. To reproduce this, we calculated costs separately for
patients accessing private and public sector hospitals, based on the estimate that 75% of the Brazilian
population are covered by public health care insurance.
7 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Table 2: Treatments per stage of breast cancer25
Stage Description Treatment
Stage I & II Considered “early stage”, the tumour is still relatively Treatment options for stages I-III are more or less
small, and has not spread to the lymph nodes, or the same and usually consist of surgery, radiation
only to one or a few nearby lymph nodes. Stage therapy, often along with chemotherapy or other
II tumours are slightly larger than stage I, or have drug therapies, either before or after surgery
spread to slightly more lymph nodes
Stage III Considered “locally advanced”, the tumour is slightly
bigger, and/or has spread to nearby tissues, or to
more lymph nodes, or lymph nodes slightly further
away
Stage IV Considered “advanced” or “late stage”, these cancers Stage IV cancers are not able to be cured through
have spread beyond the breast and nearby lymph surgery, and therefore are usually treated with drug
nodes to other parts of the body (metastasised) therapies (chemotherapy, hormone therapy, or
targeted therapies alone or in combination)
Table 3 gives the proportion of people estimated to be diagnosed at each stage in Brazil from the
literature,17 and applies this to the estimated number of new breast cancer cases within São Paulo city
in 2018. We also further divide these women into those receiving public and private healthcare.
Table 3: Split of breast cancer cases by stage at diagnosis17
Estimates for São Paulo City
Breast % diagnosed in each % diagnosed in each stage Number of cases treated Number of cases treated
cancer stage stage (public sector) in the (private sector) in public sector in private sector
Stage I 15% 33% 662 487
Stage II 48% 47% 2,102 693
Stage III 33% 16% 1,438 236
Stage IV 6% 4% 243 62
Totals 100%* 100%* 4,425 1,478
*Rounding means figures appear to sum to more than 100%
We calculated the direct costs for women with breast cancer in São Paulo city in 2018 by estimating
the annual per patient cost in the public and private sectors for diagnosis and treatment according
to our understanding of the treatment pathway. We then multiplied these costs by the number of
patients in each stage of breast cancer being treated in each sector, as outlined in Table 3.
Indirect costs
The costs associated with lost productivity due to employee disability and absence from work due
to ill health among women with breast cancer are likely to be substantial.26 Estimating the indirect
costs—from the impact of work absence and early mortality on economic output—involved looking at
GDP per worker per day; breast cancer’s incidence overall and in specific age bands; and age-specific
workforce participation rates.
In order to calculate the indirect costs of breast cancer we considered the impact in terms of
nominal GDP loss due to work absence and early mortality for people who were part of the work
force. Firstly, we used the number of women with breast cancer per age band and applied the Brazilian
labour force participation rate for each age band27 to these numbers in order to calculate how many
8 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
individuals with breast cancer would have been part of the working population. We then considered
the days of productivity lost and chance of early mortality among these working women.
Work absence
Women in the US who have a double mastectomy and breast reconstruction are more likely to
miss a month or more of work than women who have a partial mastectomy.28 According to official
reimbursement data from DataSUS, around 65% of women with breast cancer who have surgery
receive double mastectomies in Brazil.22 Another US study found women treated for breast cancer
missed a median of 22 days from work, and when treated with chemotherapy and surgery the median
increased to 40 days missed.29 A study of Canadian breast cancer survivors found around 85% reported
at least one work absence of four weeks in the first year after diagnosis.30 The average absence from
work in the year after diagnosis in this study was 6 months.
In advanced (stage IV) breast cancer, 5 year survival in the US is about 22%.31
We used the proportion of people diagnosed in each stage of breast cancer, outlined in Table 3, to
calculate how many working individuals with breast cancer would be in the different cancer stages.
Using these proportions, we made the following assumptions about those able to continue work after
their diagnosis:
l All women with stages I-III breast cancer would be absent from work for four weeks in the first year
after diagnosis
l Because only 22% of people with stage IV breast cancer are likely to survive for 5 years, we
estimated that 22% of women diagnosed in this stage would be able to work, but 78% would not.
To work out the costs for work absences we considered the working population living with
breast cancer per age band and per stage, and the associated number of days missed from work.
By multiplying the days lost by the number of individuals in each age band and stage we got a total
number of days lost from work. We then multiplied the days of absence from work by the daily
gross domestic product (GDP) per member of the workforce for those employed in Brazil, which we
calculate by taking the GDP per member of the workforce and dividing that by working days per year.
From this combination of calculations we estimate productivity lost due to employee absence.
Early mortality
To work out the costs associated with early mortality we assumed that 78% of individuals diagnosed
in stage IV would lose their lives to breast cancer in the same year of diagnosis, meaning we assume a
loss of 100% of productivity for 78% of women in stage IV who die. While these figures are likely to be
an over-estimate (as they are based on 5 year survival), to balance this, the remaining 22% of women in
stage IV were considered not to have any absences, which will be an under-estimate.
Based on this assumption we calculated the number of days lost due to early mortality for women
with stage IV breast cancer by taking 78% of the total working days per year in Brazil (197 days), and
multiplying this number of days by GDP per member of workforce.
9 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
4. The economic burden of cancer in São
Paulo city
Direct costs
Table 4 outlines the direct costs for the public and private healthcare sector in São Paulo city, stratified
by stage of breast cancer. We estimated the overall direct cost of breast cancer in São Paulo city to be
861 million Brazilian Real in 2018. Before discussing the implications of this cost we first consider where
these costs accrue.
The costs per patient for the public sector, as might be expected, are much lower than the per
person costs in the private sector. This means that even though fewer women (25%) are treated in the
private sector, overall costs are higher. The direct costs of breast cancer increase between stages I-III,
and then drop when moving into stage IV. This is largely due to women with stage IV breast cancer not
having as many surgeries and intensive treatment, particularly in the public sector where palliative care
resources are sparse.
Table 4: Cost of breast cancer in São Paulo city (costs in Brazilian Real)
Stage of breast cancer % Women diagnosed New cases in São Paulo Cost per patient Costs per stage for all
in each stage city 2018 women in São Paulo city
Public sector
Stages I 15% 642 29,776 19,105,122
Stage II 48% 2,102 29,776 62,585,743
Stage III 33% 1,439 128,673 185,047,518
Stage IV 6% 244 10,687 2,600,910
Public sector subtotals 100% 269,339,293
Private sector
Stage I 33% 487 415,167 202,082,651
Stage II 47% 693 415,167 287,814,685
Stage III 16% 236 369,393 87,176,737
Stage IV 4% 62 233,923 14,491,554
Private sector subtotals 100% 591,565,626
Overall total 860,904,919
Indirect costs
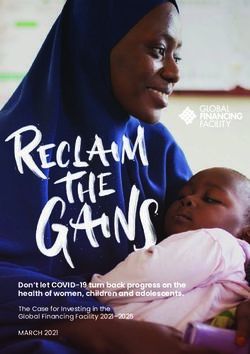
Figure 1 shows the total indirect costs for all stages of breast cancer, estimated to be around 19 million
Real in 2018, 10 million (53%) of which is associated with work absence and 9 million (47%) associated
with early mortality.
10 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Total cost of breast cancer Figure 1: Total indirect costs, 2018
(Brazilian Real m)
The total cost of breast cancer (direct and indirect
20.0 20.0
costs) in 2018 in São Paulo city was estimated at
18.0 18.0
880 million Real. The vast majority of this price 19.0
16.0 16.0
tag, 98%, was accrued from the direct costs, with
14.0 14.0
just 2% accrued from the indirect costs.
12.0 12.0
Future trends 10.0 10.0
8.0 10.0 8.0
We also modelled forecasted figures for the 9.0
direct and indirect costs between 2018 and 2022. 6.0 6.0
These estimations were based on extrapolating 4.0 4.0
historical trends in: 2.0 2.0
l Population growth data from the World Bank32 0.0 0.0
Total indirect Work Early
l Healthcare spending per head33 costs absence mortality
Source: The Economist Intelligence Unit.
The incidence of breast cancer below age 40 is
fairly low (BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
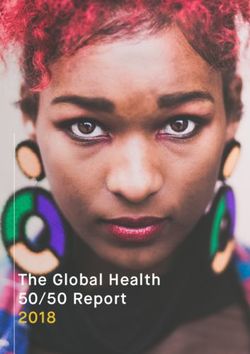
Figure 3: Indirect costs of breast cancer in Figure 4: Total direct and indirect costs in
São Paulo city, 2018 to 2022 São Paulo city, 2018-2022
(Brazilian Real m) (Brazilian Real m)
Work absence Early mortality Total indirect costs Total direct costs
25.0 25.0 1,400 1,400
11 11 1,200 11.0 1,200
20.0 20.0
10 10
1,000 1,000
9
15.0 15.0
800 800
12 12 600 600
10.0 10.0
11 11
10
400 400
5.0 5.0
200 200
0.0 0.0 0 0
2018 2019 2020 2021 2022 2018 2019 2020 2021 2022
Source: The Economist Intelligence Unit. Source: The Economist Intelligence Unit.
Figure 3 shows the breakdown of indirect costs into those due to work absence and early mortality.
Figure 4 demonstrates the considerable share of the overall price tag of breast cancer is attributable to
the indirect costs compared to the direct costs.
12 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
5. Barriers to effective breast cancer care
A s well as estimating the cost of breast cancer, we identified some of the potential barriers to
effective breast cancer care in São Paulo city and Brazil more widely, through both published
literature and interviews with oncologists working in the region. These barriers can give insight into
both the direct costs of breast cancer, and also ways in which breast cancer care could be improved.
Need for earlier detection
As reported above, only about two thirds of women with breast cancer in Brazil are diagnosed at an
early stage (stages 0, I or II). As the disease progresses to later stages, it becomes more difficult to treat,
and the chance of survival worsens (in the US 5 year survival in stage IV is estimated to be 22%).31
In Brazil, as shown in table 3, about a third of breast cancers are diagnosed when they are locally
advanced (stage III), and 9% when they are metastatic (stage IV), in cases where stage is known. This
means that late stage diagnoses represent around 38% of total diagnoses in the public sector. By
comparison, data from 2011 suggests that the corresponding figures in Australia for example are much
“From a medical
lower, at about 13% and 5% respectively. This is likely to contribute to the disparity in 5-year survival—a
point of view,
mammography stark contrast at about 75% for Brazil and 90% for Australia in figures for 2010-2014.
should be done Extending early detection programs is difficult due to inequalities in healthcare access and coverage,
every year because limited funding, and inadequate infrastructure.36 These and other issues are discussed further below.
it reduces mortality
but from the Inconsistent screening policies
manager’s point Decisions about whether (and how) to offer screening for any condition requires an assessment of
of view it is not
the balance of benefit and risk. This balance may differ in different age groups based on their baseline
worth it since it
would demand a risk, as well as other factors such as their life expectancy. Practical considerations also need to be taken
large amount of into account, such as availability and cost of equipment and trained staff, particularly when healthcare
resources and the budgets are limited.
government faces Often the judgments of different stakeholders or organisations about these complex issues
an already restrict differ, leading to controversy. A lack of consensus among professional bodies can be confusing for
constraint.” patients and health professionals. This situation exists in Brazil, where there is a lack of consistency in
Dr Bosco, Specialist Doctor
in breast disease, Sociedade recommendations from different bodies relating to screening for breast cancer.
Brasilera de Mastologia The Brazilian National Cancer Institute (INCA) and the Ministry of Health recommend screening
Regional SP
mammography (digital or conventional) in women aged 50–69 years every two years.37 They do not
recommend mammography screening outside of this age range (i.e. in those younger than 50 or aged
70 years or older) for women at average risk (i.e. not those at high risk based on family history or known
genetic mutations). This is because the evidence suggests that in younger women possible harms
outweigh the possible benefits, and in older women this balance is unclear or likely to favour harms.
However, joint consensus guidelines from a group of Brazilian professional bodies including the
Brazilian College of Radiology and Diagnostic Imaging advise annual mammography screening,
preferably digital mammography, for women aged 40–74 years and also for women aged 75 years or
13 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
older who have a life expectancy of seven years or more.38 This represents both an increased frequency
of screening (annually as opposed to every two years) and an extension of the age range in which it is
recommended compared to the Ministry of Health recommendations.
These inconsistencies may lead to confusion among practitioners, and could divert resources away
from groups who may benefit most from screening. A survey carried out between 2010 and 2012 in
“If I could change Brazil, discovered that at national level, almost 40% of mammograms were performed in women
one thing about aged 40-49—an age group in which mammography is not recommended by Ministry of Health
breast cancer guidelines.39 In a study of all women who died from breast cancer over the age of 15 in São Paulo state,
detection it would increased mammography screening was associated with increased mortality.40 This suggests there is an
be to change underestimation of the risks associated with mammography screening.
opportunistic
screening to
organised
Poor access to mammography
screening.” Some evidence suggests that the shortage of mammography equipment is not the main problem in
Dr Gioia, Researcher, INCA Brazil.
A survey conducted by the Brazilian Network of Research in Mastology suggested there were 4,228
mammogram machines in Brazil in 2013, with more than half of those being available in the public
system.41 This represents about one machine per 50,000 inhabitants, far in excess of the one piece of
mammogram equipment per 240,000 habitants recommended by the Ministry of Health in 2002.6 As
national recommendations on screening were only first published in 2004, this 2002 requirement may
underestimate need, but other evidence also supports that sufficient equipment is available.
Another study looking at SUS data found that 1,526 mammography machines were available within
SUS in 2012.39 They estimated that the capacity of these machines was about 7.74 million exams per
“The main method
year, only just short of the 7.79 million exams they estimated were needed to meet the demands of
of screening for
breast cancer is the population. However, the total number of mammographies performed that year was just under 4
mammography. million.
Despite the high Clearly the available machines are not being used to capacity. Why?
frequency of The answer is likely to be complicated. Research in São Paulo metropolitan region in 2011 found
breast cancer, that about 6% of the mammography machines were not being used, in some cases because they were
there is still not a
broken.42 Even the machines which were being used were not being used to full capacity, and records of
broad structure in
Brazil that allows the equipment available was not up to date.42
women assisted In addition, there are no centralised systems in place to support an organised screening
by SUS, which programme.39 For example, there are no systems to keep a record of eligible women and issue them
is the majority routine invitations for screening when it is due. This may limit uptake.
of Brazilians, to Other studies have suggested that another factor which limits access is the concentration of
guarantee a decent
mammogram machines in more developed areas of Brazil.6, 22 The North and Northeast regions of
level of care,
Brazil are always at a disadvantage when compared to the South, Southeast and Midwest regions in
focused not only on
treatment but on terms of equipment availability (such as mammography equipment).39 There are also fewer medical
early detection.” specialists available to perform diagnostic and treatment procedures; as a result there are fewer
Dr Gioia, Researcher, INCA procedures performed in this region.
In the North-eastern region of Brazil, mortality rates increased by 5.3% on average every year in the
last decade, but declined slightly in other regions.43 As well as poorer access to diagnosis and treatment,
14 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
“Even within demographic development, changing lifestyles and associated risk factors may be another contributing
Brazil, staging and factor to these disparities. For example, biological reasons may also play a part driven by Southern
survival statistics Brazil having mainly Caucasian Ancestry, while there is a mixed population of African, European and
vary according to Indigenous ancestry in populations in North Eastern Brazil.43 Some research suggests increasing
socio-demographic
numbers of oestrogen breast tumours in African American, Hispanic and white women are linked
characteristics, such
as the type of health with changing incidence of obesity and parity,44 thus increased mortality in the North-eastern regions.
insurance. Women People of African ancestry have also more recently been linked to aggressive high grade oestrogen
treated in the public tumours at a younger age, thus have higher mortality rates compared to Caucasians.45-47
system present with This issue may not be a major concern for São Paulo city, the largest city in Brazil, where resource
the disease in more availability is likely to be higher than other areas. This is supported by the fact that another key piece of
advanced stages
breast cancer care equipment—radiotherapy machines—are much more plentiful in São Paulo state
than women in
the private sector, than the national average (6.01 versus 0.93 per million inhabitants respectively).1 However, awareness of
and public sector better access to care in São Paulo city may result in increased burden for the city if women from nearby
patients have worse regions come to the city for treatment.
disease-free and
overall survival, Inequity between public and private healthcare systems
which may be There are huge disparities between the care available in the public and the private healthcare system,
partially attributed
which is a source of frustration for patients and oncologists alike.
to the greater delay
and advanced In Brazil, analysis of women with breast cancer at one hospital found that having treatment paid
stages at the time of for by SUS is associated with shorter survival.7 This was mostly down to women covered by SUS being
diagnosis.” diagnosed at later stages than women covered by private insurance.
Dr Gioia, Researcher, INCA
“In Brazil, only around 20% of breast cancers are diagnosed at an early stage
of the disease, and women treated in the public health system present
unfavourable outcomes when compared to women treated in the private
sector, with worse disease-free and overall survival outcomes.”
Dr Gioia, Researcher, INCA
This 20% statistic comes from research conducted in Brazil, published by the American Association
of Cancer Research in 2009.48 This research used data from 28 cancer centres distributed throughout
the country, and found: 20% of women were diagnosed with stage I (the “early” stage referred in the
quote to above), 46.8% were diagnosed stage II, 24.6% stage III and 5.5% stage IV. Therefore, the
proportions of women diagnosed per stage in this study quoted by Dr Gioia,48 are very similar to the
staging data used to calculate the economic impact of breast cancer in this study.17
The rate of early diagnosis for women treated for breast cancer in private hospitals is quite different.
A 2018 study looking at treatments received for 1,230 women with breast cancer in a private hospital
in Brazil, found most people were diagnosed in early stages (79% stage I).11 In São Paulo specifically,
another study found diagnosis of breast cancer in stage III and IV was found to be as high as 37% for
women with public health insurance, compared to 16% in the private sector.10 A further study found
that women with breast cancer treated in public hospitals had a significantly longer time between
diagnosis and starting treatment than those who were not.49
15 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
One study has suggested that public-private partnerships between the government and private
hospitals may help to improve speed of access to treatment in Brazil.12 It suggested private hospitals
could step in to assist public hospitals during the more critical phases of treatment where SUS has the
most difficulty, such as rapid access to diagnosis, and surgery within 30 days of biopsy.
“The most
important thing is Delays in accessing treatment in the public sector
not the treatments The start of treatment for breast cancer is subject to significant delays in Brazil. To try to counter this,
available for the
in 2012 the government issued the “60 Day Law”, which advises treatment for any type of cancer for
patient to receive;
it’s allowing the patients in the public health system must begin within 60 days from the definitive diagnosis.50 Although
patient to receive this law is an important and well-intentioned effort to begin to reduce delays, surveillance of its
the treatments implementation has been deficient. A survey of 59 public health institutions in Brazil discovered that
that are available. The Cancer Information System (SISCAN), a database set up to monitor adherence to the 60 day law,
Here [in Brazil] we was used in only one quarter of Brazilian municipalities, and only 1% patients with cancer.51
do not have a very Although the statistics vary by region, a 2015 study that collected data from 239 hospitals in Brazil
good plan of breast
found 40% of women with breast cancer did not receive treatment within the 60 day period.49 This may
screening, a woman
usually comes to in part be due to priority for treatment sometimes being given to women in the early stages of disease
us as they feel a with a higher chance of cure, resulting in delays in treatment for women in late stage of disease.52-56
lump in the breast, However, not all studies have supported this explanation. One found the contrary, that the time
after they see us, between diagnosis and treatment is longer for those with early stage disease.49
to see a specialist Another contributing factor may be that diagnostic mammography results are not prioritized over
may take 6 months,
screening mammography results, causing delay in treatment.57
which is a long time
and will change
her prognosis. The Lack of access to newer testing and treatments
most important The optimal treatment for a woman’s breast cancer will depend on the molecular characteristics of her
thing here in Brazil tumour—whether it is hormone (oestrogen and progesterone) receptor positive or negative, or HER2-
is to receive the positive or negative.
treatment in a For example, about 15-20% of breast cancers produce abnormally high levels of a protein called
timely way. We
HER2.58 These cancers are referred to as being “HER2-positive” and have worse prognosis than HER2-
have the treatments
available, but negative cancers. A number of targeted treatments, such as trastuzumab and lapatinib, have been
patients do not have developed specifically for HER2 positive cancers.
the opportunity to For treatments to be selected appropriately, molecular testing needs to be carried out on the
see a doctor.” tumours. One Brazilian study reported that some public laboratories in Brazil do not offer molecular
Dr Marques, Specialist testing, meaning that patients have to pay out of their own pockets if they wish to have it done at a
Doctor in breast disease,
Hospital Santa Casa de São private laboratory.59 Cities like Sao Paulo and Rio de Janeiro are exceptions to this rule and do have
Paulo
access to molecular tests, although there are known delays of around 30 days to receive the results.60
“The molecular tests can identify sub classifications of the tumor more
efficiently than pathologists. For example, if women in initial stages of breast
cancer have this test, chemotherapy wouldn’t be necessary, and therefore, it
would save more resources to the ones who really need chemotherapy.”
Dr Bosco, Specialist Doctor in breast disease, Sociedade Brasilera de Mastologia Regional SP
16 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
There are also a number of newer molecular tests available which look at the activity of a range
of genes in early stage breast cancers, to predict of risk of recurrence of the tumour after surgery.
This information can be used to help women and their doctors to decide whether they should have
adjuvant chemotherapy or not, to avoid potentially unnecessary treatment.
“Only around 30% There is demand to improve access to molecular testing in Brazil, and targeted therapies for HER2
of patients needing positive breast cancers.59
palliative care in
the public sector
receive it compared
Lack of reliable data to inform planning and policy making
to around 70% in Databases responsible for gathering information on breast cancer in Brazil are reported to be
the private sector.” outdated, producing inaccurate and inconsistent statistical information and additional complications
Dr Goncalves, Professor, for health managers.57 There is an urgent need to improve the accuracy of data produced by
Instituto do Cancer do
Estado de São Paulo population-based cancer registries in order to better plan cancer control.36
“Terminal treatment, is a very difficult situation here in Brazil, because you
can’t keep your patient inside the hospital, you need to send them home, as we
need to use the beds for patients in the earlier stages that require surgery etc.”
Dr Marques, Specialist Doctor in breast disease, Hospital Santa Casa de São Paulo
Limited access to palliative care
Palliative care is underdeveloped in São Paulo city, and is usually managed by oncology units and
medical oncologists rather than dedicated palliative care teams. Again, there is a disparity in access
between public and private sectors.
Good palliative care is important to patients and their families, and if specialised palliative care
services are available, and appropriately integrated into mainstream healthcare systems, this may
reduce the inappropriate use of more expensive inpatient medical services.
17 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
6. Benchmarks
B enchmarking is the comparison of different providers, organisations, or geographical areas,
on indicators of quality. Analysing the range of performance in the indicator areas highlights
strengths and weaknesses of each organisation, facilitates goal setting based on what improvement is
known to be possible, and identifies “high achievers” whose performance can be studied and emulated.
The aim is to help identify and implement best practices at best cost.61
Cancer survival is one indicator of care quality. It has historically varied between countries, and if
survival is particularly low in one country compared to others, especially for those with similar wealth,
it can be an indicator that the health system is not functioning as it should.62
Survival rates for breast cancer can be very good, particularly when detected early, and appropriate
treatments are available. For example, in the US the overall 5-year survival rate for breast cancer is
about 90%. Their 5-year survival rate for women with stage I cancer is close to 100%, for stage II it is
about 93%, and for stage III it is 72%.31 It is only when the cancer has spread to other parts of the body
(stage IV) that it becomes much more difficult to treat, and 5-year survival rates drop to about 22%.31
Even then, there are many treatment options available. In countries where breast cancer is less likely to
be detected early, or where access to treatment is more limited, prognosis is poorer.63
Unfortunately, the same treatment and excellent survival rates cannot be guaranteed in Brazil.
While Brazil has developed a successful public health system, and achieved important gains for the
population, there are many limitations, causing problems for patient treatment. In cancer care, this
is largely due to the delayed diagnosis and therefore treatment at the earliest possible stage. There
have been international efforts to reduce disparities in healthcare access in low and middle income
countries,64 in the hope that this would in turn, reduce mortality from disease such as breast cancer.
However these do not take into account individual needs, which vary from country to country.22
Choosing local and international benchmarks
Benchmarking overall cancer survival (including breast cancer survival) to identify countries
performing well and those performing less well has been the focus of several, longitudinal,
international studies spanning the years 2003-2018.5, 62, 65-69 These studies formed the basis for our
selection of an international benchmark.
Table 6 summarises estimates for the countries with the highest 5-year survival, along with Brazil for
comparison. The CONCORD working group compares international survival rates, and the EUROCARE
working group compares European survival rates. The countries which perform consistently well are
Australia, the US, Sweden, Finland and Japan. The two countries with the highest survival rates in the
most recent data are the US and Australia. Despite the US having a slight edge, we choose to focus on
Australia as the international benchmark for this study. Many of the cancer care guidelines in Brazil are
already based on treatment guidelines from the US, so we hoped to offer new insight from Australian
practices and guidelines. Secondly Australia has some similarities with Brazil in terms of having a hard
to reach indigenous population.
18 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Table 6: Five year survival from key multi-country studies
Time period
Country
1990-1994 1995-1999 1999-2007 2010-14
Data source CONCORD69 EUROCARE-365 EUROCARE-462 EUROCARE-568 CONCORD5
Australia 80.7 — — — 89.5
US 83.7 — — — 90.2
Sweden 82.0 82.7 84.3 86.0 88.8
Finland 80.2 80.0 83.6 85.7 88.5
France 79.8 80.9 82.7 86.1 86.7
Netherlands 77.6 78.1 82.7 84.5 86.6
Canada 82.5 — — 88.2
Japan 81.6 — — 89.4
Brazil - - 58.4 — 75.2
“If you look at
improvements of
survival over the
Australian benchmark
last 30 years, the Australia’s breast cancer outcomes have shown substantial improvement over time, with the
two issues are early proportion of female total cancer mortality attributable to breast cancer decreasing from 19% in 1982
diagnosis and better to 6.5% in 2016. Nowadays Australians diagnosed with cancer experience some of the highest cancer
multidisciplinary survival rates in the world, as evidenced by the GLOBOCAN data.
team (MDT) Expenditure on cancer by the Australian government, private health insurers, individuals and
treatment, both of
households increased by 56% between 2000-01 and 2008-09, from $2.9 billion to $4.5 billion. The
them work together
and for a system government set up Cancer Australia in 2006 as the national cancer control agency; it aims to reduce the
to offer optimal impact of cancer, address disparities, improve outcomes and inform effective and sustainable cancer
outcomes it needs care.70
to address both of
those things.”
Early diagnosis
Dr Bruce Mann, Professor
Nationally organised population screening programmes for breast, cervical and bowel cancers have
of Surgery, The University been effective and remain an important strategy in reducing incidence and mortality from these
of Melbourne, Director of
Breast Tumour Stream cancers in Australia.70
“We have a national breast screening programme modelled on the UK/NHS
programme that has been going for around 20 years. It has a broad public
acceptance that screening and early diagnoses are valuable, although there
is some controversy about screening, particularly from some Scandinavian
commentators regarding the harms of screening, but generally it’s accepted
that early screening is good. The government has established a national
screening programme where all women 50-75 are invited to screening 2 yearly.
The participation rate in the BreastScreen Australia programme is ~56% of
invited women, however a significant extra portion do undertake private
screening. One impact has been that the rate of late diagnosis is quite small.”
Dr Bruce Mann, Professor of Surgery, The University of Melbourne, Director of Breast Tumour Stream
19 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
The general idea around screening is that the earlier the condition is found, the easier it is to treat
and therefore the better the chances of surviving it. Women are also less likely to need a mastectomy
or chemotherapy if breast cancer is detected at an early stage. The main concerns around screening
are that it can pick up cancers that would not have gone on to cause any symptoms or become life
threatening. Because it is not possible to identify who this applies to, some women will end up having
tests and treatment (and the ensuring side effects) for breast cancer that would never have otherwise
caused them harm.71
Patient advocacy
Directly engaging women with breast cancer through advocacy groups, which provide support through
sharing experiences, as well as clinical information and general education, has been an important
part of effective breast cancer treatment in Australia. Advocacy groups have also played a role in
informing women of the importance of breast cancer research and as a result facilitate enrolment
into clinical trials.72 The Breast Cancer Network Australia (BCNA), is a national advocacy group which
has been running since 1998, and is the main organisation for Australians affected by breast cancer. It
has a network of more than 120,000 individual members and 300 member groups. It is one of the key
organisations responsible for effective education and awareness of breast cancer in Australia.
“There is an organisation called the BCNA, which is a national advocacy
organisation, to advocate for better cancer care. They have been fairly
effective in advocacy for high quality comprehensive care for all. The concept
of the multidisciplinary team (MDT) was adopted in breast cancer very early,
BCNA was part of it but not the only reason. It was implemented taking the
lead from the UK in many ways, to address the problem that in the past breast
cancer was a surgical condition only, and a number of patients were not given
optimal treatment because their treating surgeon was not up to date, and
denying effective treatments beyond surgery, so called adjuvant treatments.”
Dr Bruce Mann, Professor of Surgery, The University of Melbourne, Director of Breast Tumour Stream
A key focus of BCNA advocacy is to work with health policymakers and health service delivery to
ensure all Australian’s receive equitable and affordable access to the latest and best practice. BCNA
reaches out to its members by sending a “My journey kit” to all their members, outlining what cancer
care entails and possible side effects, as well as medical and counselling contacts.73
20 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
Helping patients to navigate their care
Specialist breast cancer nurses are also valued as a key aspect of breast cancer care in Australia:
“So we have the nursing subspecialty of the breast care nurse, who plays a
very complex role. It is partly patient navigation, as for effective and efficient
treatment, surgery, medical oncology and radiation oncology, need to work
together. Expecting a patient to be able to do that unassisted is unreasonable.
Our breast care nurses do a certain amount of the coordination of that care,
and also focus on psychosocial care. How important are patient navigators?
It depends on the structure of the treatment pathway. Where the structure
is cancer centres or breast centres, where the multidisciplinary team work
in parallel then the patient navigator is less important, but when a patient is
expected to get from a surgeon’s office to a medical oncologist’s office to a
radiation oncologist’s office in a coordinated manner, then assistance from a
knowledgeable individual is needed.”
Dr Bruce Mann, Professor of Surgery, The University of Melbourne, Director of Breast Tumour Stream
These kinds of services help minimise the effects of institutional, socioeconomic, and other barriers
“The problem in
São Paulo is not the to optimal patient care.13 Patient navigators aim to guide a patient’s pathway through diagnosis and
number of doctors, treatment, ensure they get the referrals they need and continue to pursue their treatment. Studies
it is [patient] have indicated that they improve time to confirmation of diagnosis and treatment.74, 75-77 Despite the
education. The impact patient navigation systems have had in developed healthcare systems, they have not been
patient does not widely implemented in lower middle income countries such as Brazil.
know how to move
There is a need for similar assistance for women with breast cancer in Brazil.
through the public
system. She does Tackling inequality
not know what kind Cancer Australia also tries to focus on populations which experience poorer health outcomes,
of doctor she is including Aboriginal and Torres Straight Islander peoples and people living in rural and remote
looking for.”
Australia.70 The reach to these populations is not perfect, with Aboriginal and Torres Strait Islander
Dr Marques, Specialist
Doctor in breast disease, peoples being 6% more likely to be diagnosed with cancer and 50% more likely to die from cancer than
Hospital Santa Casa de São
Paulo non-indigenous Australians.
“We have a public private health system where, all legal residents are entitled
to free care in a public hospital, and we have some requirements of the public
hospitals that urgent cases are done within 30 days. This means that for
something like breast cancer even people with low resources can generally
get access to high quality services at no costs. Therefore there are not the
economic barriers of some systems.”
Dr Bruce Mann, Professor of Surgery, The University of Melbourne, Director of Breast Tumour Stream
21 © The Economist Intelligence Unit Limited 2018BREAST CANCER IN SÃO PAULO CITY, BRAZIL
AN ASSESSMENT OF THE ECONOMIC IMPACT AND INSIGHTS FROM BENCHMARKS
While there are both public and private hospitals in Australia, there are fewer disparities between
them in terms of the services patients receive.
“In Australia the two [public and private systems] are very closely associated
and complimentary. Most of us, [doctors] work in both. The treatment
algorithms are the same in public and private. The main differences are
the private patients get more of a choice over their surgeon, whereas the
public patients, it may be one surgeon or another or a trainee supervised the
operation. As far as follow up is concerned, for private patients I will see them
personally to manage their care whereas the public patients come to a clinic
where the surgeons are working but supervising the care of a lot of patients.
The public service are therefore high quality, but less personalised and the
patients have less control over who they see or when they see them.”
“There are essentially no differences between drug access between the
public and private healthcare system for most cancer medications. There
are some medications that are available for sale but not nationally funded.
These are often the new drugs. This means anyone is able to purchase one of
these drugs if they wish but there is no government subsidy for it. It is an area
where there is a lot of advocacy to get the new drugs funded. There is also a
new class of drugs called the CDK [cyclin dependent kinase] inhibitors, which
is a substantial breakthrough in the treatment of advanced breast cancer.
They have been standard in the US for probably 18 months. They have been
available for purchase in Australia for a while, but they have only just got a
public subsidy. That subsidy has been delayed. Has this had an impact on
outcomes? Well a little bit, but in the big picture not very much.”
Dr Bruce Mann, Professor of Surgery, The University of Melbourne, Director of Breast Tumour Stream
“Barretos works
with treatment
protocols other Brazilian Benchmark: Barretos Cancer Hospital
public hospitals
An important development for breast cancer treatment in Brazil was the introduction of
can’t, including
hormone mammography screening programmes. These were implemented in 2003 by the 5th Regional Health
therapy for post- Administration of the State of São Paulo, and headquartered in Barretos. Barretos is a municipality
menopausal in the northern part of the São Paulo State. Its hospital, the Barretos Cancer Hospital, is a non-profit
cases, ovarian health organisation which started a free breast screening programme for women aged 40-69 years
suppression, living in the Barretos region, and 19 adjacent municipalities.78
and provides the
The Barretos hospital treats cancer patients from all over Brazil, around 2,000 cities, and
option of six lines
of treatment with approximately 1,000 medical appointments are carried out daily. As such it is recognised as one of
chemotherapy and the most important organisations for the treatment and medical research of cancer in Brazil.79 It has
hormone therapy also focused a lot of its efforts in the last few years into medical education and research.79 Because of
for metastatic its research focus, Barretos can offer treatments to patients above and beyond that of other public
patients.” hospitals in Brazil.
Dr Pedro Henrique Arujo de
Souza, Clinical Oncologist, The socioeconomic characteristics of patients treated in Barretos are particularly variable, due to
Barretos Hospital wide range of risk factors and cultural norms in different Brazilian populations.79
22 © The Economist Intelligence Unit Limited 2018You can also read