Business plan April 2015 to March 2016 - AN UPDATE TO OUR THREE-YEAR STRATEGY: RAISING STANDARDS, PUTTING PEOPLE FIRST
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Business plan April 2015 to March 2016 AN UPDATE TO OUR THREE-YEAR STRATEGY: RAISING STANDARDS, PUTTING PEOPLE FIRST, 2013-16

Contents Introduction................................................................................................................................ 1 Shaping the future..................................................................................................................... 3 Part 1: Overview.........................................................................................................................6 Our purpose, role and values................................................................................................................. 6 Who we regulate..................................................................................................................................... 7 How we define whether we are achieving our purpose ..................................................................... 8 How we measure this (strategic measures and key performance indicators) .................................. 9 Priorities for 2015/16.......................................................................................................................... 10 Part 2: Priorities in detail.........................................................................................................11 Objectives..............................................................................................................................................12 Success measures and improvements................................................................................................. 13 Annex 1: CQC new inspection approach timetable.............................................................. 27 Annex 2: The CQC Board, Executive Team and Directorates............................................. 28 Annex 3: Budget...................................................................................................................... 29 Annex 4: Risk management arrangements........................................................................... 30 Annex 5: Strategic measures and key performance indicators by priority and objective......................................................................................................... 31

Introduction
CQC’s strategy Raising Standards, Putting People 3. Build an effective CQC – we will ensure
First 2013-16 set out a radical agenda to change that we have the right people, capacity,
the way that health and care services in England capability, systems and processes in place so
are regulated. Significant changes to the way we that we can successfully deliver our purpose,
regulate NHS trusts, adult social care services and and that we continuously improve – not
primary medical services are now in place. least by listening to those who use and
those who provide services.
Inspections and Intelligent Monitoring of reliable
data now deliver a deeper insight into the quality 4. Demonstrate the difference we make –
and safety of services and provide challenge we will ensure that we are well-run, efficient
and clarity about provider performance. We and effective, and demonstrate that we
are now able to take earlier and more effective make a positive impact and deliver value for
enforcement action against poor care providers, money.
and to recognise and encourage those who deliver
In this final year of delivering Raising Standards,
good and outstanding care.
Putting People First, we will develop a strategy
In this business plan we set out our four priorities: for the next phase of our work. We describe in
Shaping the future (published alongside this
1. Deliver the new approach to regulation
business plan as a standalone document, but also
– we will continue to implement and
set out in full in the next section) our high level
improve the new approach to regulation.
ambitions for the development of health and care
2015/16 will be the first year that we
quality regulation in England. We will work on
will inspect using the new regulations
three key areas in 2015/16:
approved by Parliament as a result of the
Government’s response to Sir Robert Francis zz To develop how we will regulate new models
QC’s report into Mid Staffordshire NHS of care.
Foundation Trust. zz To develop a programme of work to look at
pathways of care to understand better the
2. Shaping the future – we will develop our
outcomes they achieve for people.
approach to inspection so we can respond
to the new models of care that will emerge zz To analyse how health and care services can
over the next few years, such as those set work in a community or a segment of the
out in the Five Year Forward View, in the population, and how well people are served
proposals for Greater Manchester, in the by that health and care system. The focus
Vanguard projects and the new models will be the system and outcomes, not just the
developing in primary medical services performance of the single organisation.
and adult social care. We are clear that
regulation must not act as a barrier to
innovation.
Introduction 1We recognise the inevitable tension between our as the only basis of sustainable improvement.
role to hold providers to account and our role We will always be independent, on the side of
to encourage improvement. CQC has a specific, the public and those who use services, but we
statutory role to “encourage improvement.” We will work hard to have a constructive not an
will give more emphasis to this role over the next adversarial relationship with those who provide
12 months and ensure that we are an important care, the vast majority of whom do so for the best
part of the changing NHS quality improvement and highest of motivation.
architecture. We absolutely recognise, however,
We have an important role to play both to ensure
that the primary responsibility for quality must
that health and care services provide people
lie with the providers and with professions. We
with safe, effective, compassionate, high quality
will do everything we can to strike the right
care and to encourage services to improve. This
balance between accountability for unacceptable
document sets out how we will deliver this in
performance and learning from mistakes. We
2015/16.
subscribe to the concept of a just, learning culture
David Prior . David Behan .
Chair Chief Executive
2 Business Plan – April 2015 to March 2016Shaping the future
The next stage in CQC’s journey CQC’s role in enabling change
in improving health and social CQC is on the side of people using health and
care social care services, their families and carers,
highlighting where services are good and
outstanding, and taking action where there is
The changing health and care landscape need for improvement. We have changed the way
The good news is we are living longer than our we assess services through a stronger regulatory
parents’ generation. The bad news is that those framework.
extra years of life are often lived with more CQC is proving its ability to deliver effective
complex health problems and with more frailty as assessments of organisations we regulate.
we get older. Compared to the past, when there was no shared
Our population is growing, people’s needs view of what good quality looked like, we are
are changing and technology is advancing. now able to provide a comprehensive description
Inevitably, demand for health and social care will of the quality of care delivered by health and
increase at a pace that resources cannot match. adult social care providers. We will bring together
One result is that services may find it difficult to our information, evidence and expertise to
meet public expectations. support change and improvement by highlighting
excellence. We will continue to refine and
In this context, NHS England’s Five Year Forward improve how we assess the quality of providers,
View signals the necessity for radical change and we will set this out in our strategy for 2016
in our models of care delivery – it outlines the and beyond.
new ones that will be developed. All of these
new care models emphasise the need to deliver To support innovation, we will be adaptable
care designed around individual needs to deliver in the way we regulate as new models of care
better outcomes for people using services. develop. New models may bring together
organisations that currently provide fragmented
These new models of care are a radical shift away services to deliver joined-up pathways of care.
from the traditional health and social care that This means that CQC should consider the
people have experienced over the last 60 years. quality of care along these pathways, as well
The organisations that deliver care have had very as within separate organisations. We will also
significant separations between them. Residential see communities giving a much greater focus
adult care is separated from domiciliary care, to health and care ‘economies’ or ‘systems’
which is separated from GP services, which is and population groups, rather than particular
separated from mental health services, which is providers. The planned arrangements for
separated from community health services. And devolution to Greater Manchester are an early
all of these are separated from acute hospital example of this shift. As the legislation in the
services. Care Act 2014 comes into effect, we will see
Care can be fragmented and based on old ways changes in the way that adult social care is
of delivery, so it is no wonder that people can funded, commissioned and delivered.
find it difficult to navigate services.
Shaping the Future 3There is commitment throughout the health and 1. Regulating new care models
care system to transform the way we care for
people and CQC has a critical role here. We will CQC will continue to register new care providers
be a catalyst for change that improves the quality and assess their commitment to deliver safe,
of care people receive, playing our part in finding effective, responsive, caring and well-led
solutions to the challenges the health and care services. Our approach to regulation recognises
system faces, working with innovative providers the development of innovative services,
and focusing our efforts where we can make a and our registration system will reflect new
unique impact. models of service delivery and support their
implementation. We have already started work
to develop a more modern and efficient online
Our journey in 2015/16 registration process.
In 2015 and beyond, we will remain focused CQC will work with the Five Year Forward View
on registration, ratings and enforcement, and vanguard sites to understand how we can assure
improving the way we gather information so high quality and encourage improvement. We
that we can identify risks of poor care. We will share our learning and good practice with
are working to understand and improve our providers and the public. Also, we will be clear
effectiveness and to demonstrate the value for with health and social care providers about how
money we provide. new care models should be registered, so that
We will take action to protect people who use providers know the legal requirements that must
services. We will use our new enforcement be in place to allow the development of their
powers where providers are not meeting the chosen model.
fundamental standards, and place providers in We will also reinforce our expectations about
special measures where we find serious problems, joined-up care centred around the people who
but we will also identify and champion good and use services. Providers that register with CQC
outstanding practice. will be urged to consider their obligation to work
We now need to carry out this role for the closely with other providers to deliver joined-
new as well as the old models of care, and will up care. At the point of registration we will ask
continue to work closely with the Department of for evidence about how providers intend to
Health on our approach and remit as we adapt deliver care that is focused on individuals’ needs.
to reflect new ways of working across health Inspections will examine how well providers are
and social care. We will continue to encourage working with others to deliver a good experience
collaboration, joined-up care and improvement for people in their care.
across local areas, not just within individual
organisations. We are already working with 2. Looking at quality of care pathways
other arms length bodies to support new models
of care and the wider implementation of NHS CQC’s inspections enable a programme of
England’s Five Year Forward View. We will work themed work that focuses on specific health and
with people, providers and other organisations social care issues that matter to people. We will
such as commissioners to develop our approach use these thematic reviews to better understand
and encourage collaboration and improvement. care pathways.
As the quality regulator, we act on the side of For example, in 2014, our Cracks in the pathway
people who use services, their families and carers report highlighted the problems people living
and this is what they expect of us. with dementia face as they move between
In 2015/16 we will do this in three ways: hospitals and care homes. Looking at the
pathway for people with dementia between
different organisations highlighted the problems
of fragmented care.
4 Business Plan – April 2015 to March 2016We will continue our work to look at different we will explore how we can better understand
pathways of care to better understand the and comment on the impact that quality of
outcomes they achieve for people. This year, we leadership, funding and commissioning have on
will follow up inspections we have made of A&E quality across a local area.
departments, out-of-hours provision and the 111
service by carrying out a review of urgent care Encouraging services to improve
pathways.
We work closely with providers, commissioners
In 2015/16 we will do more thematic reviews of and other regulators. CQC will be co-chairing
care pathways, looking at mental health crisis the National Quality Board with NHS England to
care, end-of-life care, care for older people, ensure stronger alignment and collaboration of
and diabetes care in the community. High national organisations in quality improvement.
quality joined-up care often needs to extend
beyond health and social care services, so we CQC will review and share learning from the
will work with Ofsted, HMI Probation and early implementation of the new fundamental
HMI Constabulary to deliver multi-agency standards, especially the duty of candour. We will
inspections of children’s services, with a focus work to understand how this is helping to improve
on safeguarding. We will develop and implement quality and safety, alongside an increased focus on
new ways of inspecting health services in secure learning from complaints and concerns.
settings, including prisons. There are a number of areas where CQC will do
We will test a variety of approaches to better more to support services to improve following
understand how to assess coordinated an inspection, including signposting to external
care provision, including looking at how resources such as guidance and improvement
commissioning arrangements may affect the agencies, and making it easier to access
quality of care. We will share our learning and the examples of excellence and shared learning from
good practice we find to help others improve. organisations that have improved. Finally, we will
review the quality summit process to explore the
potential for a greater focus on whole system
3. Quality of care in your locality
improvement.
CQC has a unique remit to assess the quality
of care across health and adult social care Conclusion
sectors. By the end of 2015 we will have
inspected the majority of all health and adult All of the work set out here will help CQC fulfil
social care services in some local places, and its purpose – to make sure people receive safe,
will be able to bring together our inspection effective, compassionate, high-quality care and
findings across sectors to describe how well to encourage services to improve. There is an
people in those communities are being served increasing recognition that improvement requires
by their local health and care system. We will the whole local health and care system to work
use this opportunity to strengthen our reporting together to make the transformations needed.
on health inequalities and unmet need. We We will play our part in enabling this.
will analyse how health and adult social care
works within a community – not just in single
organisations in that area.
This is a new dimension to CQC’s reporting
capability. We will carry out this approach
in two places in 2015/16. We will develop a
comprehensive picture of the quality of care in
a local place and identify issues that need to
be addressed at the cross-organisational level
as well as at the provider level. As part of this,
Shaping the Future 5How we define How we Priorities for
Our purpose whether we are measure this 2015/16
achieving our purpose
Part 1: Overview
The Care Quality Commission is the
This describes:
independent regulator of health and
zz Our purpose, role and values, and the adult social care in England
health and social care landscape that
we regulate. Our purpose
To make sure health and social care
zz How we define whether we are services provide people with safe, effective,
achieving our purpose – what success compassionate, high-quality care and to
looks like at the levels of impact; encourage care services to improve.
outcomes; quality and effectiveness; and
internal capability – underpinned by our Our role
costing model. zz We register care providers.
zz We monitor, inspect and rate services.
zz How we measure this (through
zz We take action to protect people who use
strategic measures and key performance
indicators) and track and improve services.
our performance. We report on this zz We speak with our independent voice,
to the CQC Board, public, partners and publishing regional and national views of the
stakeholders, as well as to the Department major quality issues in health and social care.
of Health and the Parliamentary Our values
committees who scrutinise our work and
zz Excellence – being a high-performing
to whom we are accountable. We use an
even broader set of evidence (including organisation
evaluation) to assess our value for money zz Caring – treating everyone with dignity and
annually. respect
zz Integrity – doing the right thing
zz Our priorities for improving what
zz Teamwork – learning from each other to be
we do – what we will do in 2015/16 to
the best we can
improve, in order to ensure we deliver our
purpose.
6 Business Plan – April 2015 to March 2016How we define How we Priorities for
Our purpose whether we are measure this 2015/16
achieving our purpose
Who we regulate
Hospitals, mental health and Primary medical services and
community services integrated care
zz 145 acute hospital providers zz 10,292 dental care locations
(NHS non-specialist) zz 8,403 GP practices
zz 19 acute hospital providers zz 89 out-of-hours services
(NHS specialist)
zz 167 prison healthcare services
zz 53 mental health – community and/or
zz 24 remote clinical advice services
hospital providers (NHS)
zz 121 urgent care services and mobile doctors
zz 135 community health providers –
(NHS and independent) zz 952 independent consulting doctors
zz 260 ambulance service providers zz Children’s safeguarding and looked after
(NHS and independent) children’s services – inspection with partner
organisations
zz 78 mental health – community and/or
hospital providers (independent) zz Pharmacy
zz 231 acute hospital and non-hospital providers zz Integrated care
(independent)
zz 332 acute single specialty service providers
(independent)
zz 29 community and 87 residential substance
misuse providers
Adult social care
zz 17,236 residential social care homes with and
without nursing
zz 8,128 domiciliary care services
zz 324 hospices/hospice services at home
zz 71 Specialist college services
zz 66 community-based services for people with
a learning disability
zz 517 Extra Care housing services
zz 128 Shared Lives services
zz 1,745 supported living services
Part 1: Overview 7How we define
How we Priorities for
Our purpose whether we are measure this 2015/16
achieving our purpose
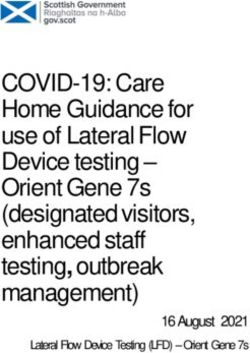
How we define whether we are achieving our purpose
This diagram sets out how we define whether we are achieving our purpose at four levels: impact;
outcomes; quality and effectiveness and internal capability, underpinned by our costing model
Health and social care services provide safe, effective, compassionate and
Impact
high-quality care, and improve
Because…
Providers People using services, their Partners and others
Use our guidance and reports to carers and the public Use our information to inform
make improvements Use our information to make their work
Take action when required to choices Share information with us
Outcomes
improve Use our information to hold Take action in response to our
Speak openly about concerns providers to account findings
Believe we are professional, Share their views and Are confident in us
transparent, consistent and fair experiences with us
Trust us and see us as on their
side
Because guidance is clear about what is expected and…
Our registration We seek people’s views We take targeted We use our
processes are robust and experiences and
Quality and effectiveness – our
and proportionate independent voice to
and establish monitor information to enforcement action share what we find
expectations and target where, when and to protect the public locally and nationally,
operating model
commitments what to inspect, and we from harm and to in ways that are
use inspection to make a make sure that accessible and useful to
thorough assessment of providers take the public and people
the quality of care and action to improve using services, to
to form valid and reliable providers, to our
judgements and ratings partners and other
stakeholders
Because we are an organisation that manages itself effectively….
Internal capabilities
Our values of Excellence,Caring, Integrity and Teamwork are expressed in everything we do
We assure ourselves that we have effective arrangements in place to:
Manage our people, our performance and quality; manage our finance systems and controls; plan
effectively and deliver; and learn from our successes and our mistakes to continuously improve
Because we understand and manage the costs of regulation ….
Costing model
CQC Providers Other stakeholders
We understand our costs and We understand the costs to We understand the wider
how we can make the best use providers and how we can system costs and how we can
of our resources minimise the cost and burden to work most efficiently with our
them partners
8 Business Plan – April 2015 to March 2016How we define How we
Priorities for
Our purpose whether we are measure 2015/16
achieving our purpose this
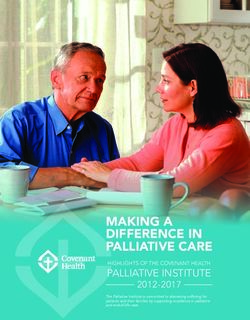
How we measure this (strategic measures and key performance indicators)
This diagram sets out measures we use to monitor progress, to and improve and report to our Board
and the public
Quality of the services we have rated
Impact
% rated outstanding, good, requires improvement or inadequate, and direction of travel
Providers People using services, their carers Partners and others
% providers that tell us our and the public % partners and others that say we
guidance, inspection, and reports % members of the public that say they effectively share information and act
help them to improve trust CQC is on the side of people using together to address failure
% providers rated inadequate or services
Outcomes
requiring improvement that improve % people saying our reports help them
when we re-inspect make choices and are useful to other
stakeholders and providers
Our future plans for regulation help us deliver our purpose and are supportive of the future direction of health
and social care (respondents to engagement and consultation tell us this)
Register Monitor Enforce Independent voice
% newly registered % Intelligent Monitoring bandings that are % providers still not % partners and
providers where we in line with ratings when we inspect meeting a others that say we
Quality and effectiveness – our
need to take Inspect fundamental effectively share
regulatory action on standard after the information
% people who use services, public and care
operating model
first inspection expected time that % people who say
staff who say they were actively involved in improve when further
% providers that tell our inspections and judgements our national reports
us registration is a action is taken. are useful
robust assessment Rate % providers not
% ratings that are challenged and % upheld; meeting a
% providers that say judgements were fair; fundamental
standard and for how
% people saying our reports help them make
long.
choices and are useful to stakeholders and
others
Register Inspect Inspection reports Enforce
% completed in 50 % first ratings inspections undertaken % published within 50 Number of enforcement
days % safeguarding alerts and concerns we days of inspection actions, prosecutions
follow up within target times and special measures
Internal capability
% Mental Health Act visits planned Complaints about CQC received,% Customer service
each quarter completed; SOAD upheld at Stages1 and 2 and key % calls answered in 30 seconds
requests undertaken within target time themes % emails answered in 10 days
% frontline posts filled % variance from budgets
TurnoverHow we define How we Priorities
Our purpose whether we are
achieving our purpose measure this for 2015/16
Priorities for 2015/16
The previous sections described our purpose; We also know that we need to continue to
how we define whether we are achieving it improve our impact, effectiveness and value
and how we measure this. We are working to for money, and we need to be a regulator that
understand and improve our effectiveness and supports changes in health and social care. To
demonstrate the value for money we provide. do this, and ensure we continue to achieve our
We are confident that as we are embedding our purpose, in 2015/16 we will undertake work to
new approach we are achieving our purpose to improve in the following priority areas:
make sure health and social care services provide
people with safe, effective, compassionate, high-
quality care and to encourage care services to
improve.
1 Deliver the new approach to regulation
Continue to implement and improve our changed approach to how we
regulate, and introduce new powers of protection
2 Shaping the future
Including how we can respond to developing models of care
3 Build an effective CQC
Ensure we have the required capacity, capability, systems and processes
4 Demonstrate the difference we make
Ensure we are efficient, effective and can demonstrate our impact and value
for money
10 Business Plan – April 2015 to March 2016Success measures
Priorities for 2015/16 Objectives and improvements
Part 2: Priorities in detail
This describes:
zz Our objectives under each of the four
priorities in the plan – what we will do
over the period of this business plan to
improve, in order to ensure we deliver our
purpose.
zz How we will know we are being
successful – our strategic measures and
KPIs under each objective.
zz What we are doing to improve – the
actions we will be taking to improve what
we do, and the dates for their completion.
zz The annexes – which set out our
structure, staffing, budget, and how we
manage risks.
Part 2: Priorities in detail 11Success measures
Priorities for 2015/16 Objectives and improvements
Objectives
Priority 1 Deliver the new approach to regulation
1.1 Put people who use care services at the heart of everything we do; engage with carers
and the public; provide high quality information to help people choose care, and
deliver our equality, diversity and human rights commitments
1.2 Register care providers: implementing improvements to how we to ensure their
commitment to deliver safe, effective, responsive, caring and well-led services
1.3 Monitor, inspect, and publish a quality rating*: acting quickly and appropriately in
response to information of concern – and implement our new market oversight role in
adult social care
1.4 Enforcement: take action to protect people who use services and hold providers to
account where fundamental standards are not met, through use of our enforcement
powers and special measures
1.5 Speak independently: publishing regional and national views of the major quality issues
in health and social care that highlight improvement and celebrate success
Priority 2 Shaping the future
2.1 Develop our response to future models of care and other changes; develop our
approach to assessing and encouraging improvement in the quality of care services
across providers and sectors; and involve the public, our staff and our stakeholders in
developing our future strategy
Priority 3 Build an effective CQC
3.1 Recruit the full number of permanent staff, professional advisors and Experts by
Experience we need
3.2 Develop the skills and knowledge of CQC staff through our Academy, foster a culture
that promotes health and well-being of our workforce and embed our values of
Excellence – Caring – Integrity – Teamwork
3.3 Embed our operating model (including systems and processes); implement a
knowledge and information strategy
Priority 4 Demonstrate the difference we make
4.1 Manage our quality, evaluate our benefits, costs and value for money, improve our
performance and manage our resources efficiently
*Where we rate the type of service
12 Business Plan – April 2015 to March 2016Objectives
Success measures
Priorities for 2015/16
and improvements
Success measures and improvements
Priority 1 Deliver the new approach to regulation
1.1 Put people who use care services at the heart of everything we do;
engage with carers and the public; provide high quality information to
help people choose care, and deliver our equality, diversity and human
rights commitments
How we will know we are being successful
Strategic measures and KPIs
• % of people that say they trust CQC is on the side of people using services
• % of people reading reports on our website saying they help them make choices & are
useful to other stakeholders & providers
• % of people who use services, public and care staff who say they were actively
involved in the inspection and judgement
• Mental Health Act Commissioner visits – % of those planned each quarter that are
completed. SOAD requests allocated and undertaken within target times
What we are doing to improve Complete by end
Raise awareness and understanding of our role and purpose December 2016
• Including raising awareness of CQC’s inspection teams through
a programme of local and regional public engagement, via
voluntary and community groups, digital engagement and
regional media
Listen to, and act on, people’s views and experiences of care:
• Design a new approach to experts by experience to ensure September 2016
they are fully embedded in inspection activity
• Establish more partnerships with organisations that can enable March 2016
and encourage people to tell CQC their views and experiences
• Develop and expand the use of feedback from people who use March 2016
services and their carers, care staff and others in the wider
system of health and social care, in our monitoring of
providers and inspection briefing
Work with the public to develop and improve our policies,
methods and other aspects of our work
• Deliver a programme of co-production, engagement, September 2015
consultation, analysis and communication to inform the
development of CQC’s new strategy for 2016 onwards
Provide high quality information about care services March 2016
• Build and publish our knowledge of the quality of care
throughout the year, through the analysis of ratings, findings
from inspections, performance data and a wider and richer
evidence base of information and research, as well as through
the publication of the Annual State of Care report
Part 2: Priorities in detail 13Improve the way we deal with concerns – both the experience
of people giving us feedback and how we use the information
(includes safeguarding alerts and concerns):
zz Complete a review into systems and processes for how concerns
March 2016
are received and responded to and implement a new process
zz Contribute to the Department of Health consultation on the
role of a National Guardian within CQC to review and improve In line with
NHS handling of staff concerns consultation
timing
Ensure the rights of people that are subject to the powers of
the Mental Health Act are upheld:
zz Conduct second opinion visits for patients detained under the As they are
Mental Health Act who either refuse treatment prescribed to required
them or are deemed incapable of consenting.
zz Visit and meet patients who are subject to the restrictions
Deliver a
of the MHA, review their statutory documentation and seek programme of
resolution to issues of concern. visits in each
zz Respond to all complaints and adjudication requests received quarter
14 Business Plan – April 2015 to March 20161.2 Register care providers, implementing improvements to how we to ensure
their commitment to deliver safe, effective, responsive, caring and well-
led services
How we will know we are being successful
Strategic measures and KPIs
zz % of registration processes completed in 50 working days
zz % of newly registered providers where we need to take regulatory action on first
inspection
zz % of providers who tell us the registration process provides a robust assessment of
their ability to provide safe, effective, caring, responsive, and well-led care
What we are doing to improve Complete by end
Introduce the new registration approach for new services and March 2015
variation applications, including ’fit and proper person‘ test.
Develop a new minimum data set which we will collect when March 2015
we register providers, beginning with the adult social care sector.
This will ensure we have more evidence to enable us to assess if
a provider meets the minimum standards to enter regulation, and
subsequently support the ongoing monitoring of that provider in a
proportionate way
Deliver an online capability which allows providers and September 2015
managers to register and maintain their registration online
Ensure CQC registration increasingly supports obligations and September 2015
evidence of intention to deliver care focused on individuals’ needs;
joined up care and working with others
Part 2: Priorities in detail 151.3 Monitor, inspect, and publish a quality rating - acting quickly and
appropriately in response to information of concern - and implement our
new market oversight role in adult social care
How we will know we are being successful
Strategic measures and KPIs
zz % providers/ locations rated outstanding; good, requires improvement or inadequate,
and direction of travel
zz % intelligent monitoring bandings that are in line with ratings when we inspect
zz % of people who use services, public and care staff who say they were actively
involved in the inspection and judgement
zz Inspection – % first ratings inspections undertaken
zz Inspection reports - % published within 50 days of inspection
zz % of people saying our reports help them make choices & are useful to other
stakeholders
zz % of providers that tell us our guidance, inspection and report helps them to improve
zz % of providers that say judgements were fair
zz % of times we deviate from our ratings aggregation principles
zz % of challenges to ratings received, and % upheld
zz % of providers rated inadequate or requiring improvement that improve when we re-
inspect
zz % calls answered in 30 seconds (90% for safeguarding and mental health).
zz % of safeguarding alerts and concerns we follow up within target times
What we are doing to improve Complete by end
Intelligent Monitoring – continue to deliver updates to March 2016
intelligent monitoring implementing ongoing improvements
Inspect providers/ locations, making a judgement on their
quality rating*:
zz Complete our programme of first rating inspections in Timetable at
accordance with our overall timetable annex 1
zz Publish a rating and a report of our inspection Within 50 days of
*Where we rate the particular service type – the services we rate inspection
are shown in the timetable in annex 1
Undertake timely focused inspections, either:
zz In response to information of concern, or As required
zz To follow up on urgent improvements we have required as part
of a previous inspection
Undertake ‘return and re- rate’ comprehensive inspections, to a Ongoing
frequency determined by the level of rating
16 Business Plan – April 2015 to March 2016Roll out new approach inspection in: From April 2015
substance misuse, independent hospitals, ambulance services
independent doctors, dentists, health and justice
Improve how we respond to information about safeguarding risks
to individuals
zz Publish revised organisational policies on safeguarding, October 2015
including engagement with local statutory Safeguarding Adult
Boards
zz Train all of our staff on basic awareness of safeguarding and December 2015
more advanced training for our inspectors
zz Fully embed the use of enforcement inspectors December 2015
zz Ensure systems and processes identified as part of the
operating model support effective responses by CQC,
continuous improvement and the capability of identifying
trends and themes in safeguarding incidents
Implement the new market oversight regime for “hard to
replace” adult social care providers by undertaking regular
assessments of the financial and quality performance of the
businesses within the scheme
zz Publish who is in the scheme May 2015
zz Specialist providers enter the scheme October 2015
zz Evaluate our approach and impact to support continuous March 2016
improvement in carrying out our regulatory function
Part 2: Priorities in detail 171.4 Take action to protect people who use services and hold providers to account
where fundamental standards are not met, through use of our enforcement
powers and special measures
How we will know we are being successful
Strategic measures and KPIs
zz % of providers still not meeting a fundamental standard after the expected time, that
improve when further action is taken
zz % of providers not meeting a fundamental standard(s) and for how long
zz Number of enforcement actions, prosecutions and special measures
zz % of partners and others that say we effectively share information and act together to
address failure
What we are doing to improve Complete by end
Implement our new approach to how we use our enforcement
powers, including formal enforcement, investigations, special
measures, and how CQC works with other regulators/oversight
bodies in each sector:
Develop capacity and capability to deliver high quality
enforcement action including through:
zz Recruitment of enforcement inspectors June 2015
zz Joint work with HSE to support sector enforcement inspectors Apr-Oct 2015
in establishing their role effectively
zz Training strategy May 2015
zz Training delivery programme March 2016
zz Build on the new arrangements for working with HSE by developing October 2015
arrangements with other enforcement bodies (e.g. police, CPS)
Ensure the systems and processes identified as part of the March 2016
operating model support the delivery and continuous improvement
of the enforcement function
Embed an assurance framework for enforcement – quality Quarterly
standards, controls and a programme of quality sampling aligned programme of
with the quality framework quality sampling
Identify if there are recurrent concerns that we should prioritise,
or if there are potential ‘sentinel’ cases where one instance of Ongoing
enforcement could influence and encourage improvement across a
broader sector.
Give further consideration to possible use of fixed penalty notices June 2015
for failures to submit required notifications to us and, in line with
the Winterbourne View Concordat, the continuing need to assure
the quality of care in inpatient services for people with a learning
disability.
18 Business Plan – April 2015 to March 20161.5 Speak with our independent voice, publishing regional and national
views of the major quality issues in health and social care that highlight
improvement and celebrate success
How we will know we are being successful
Strategic measures and KPIs
zz % of people saying our national reports are useful , including in sharing learning and
informing choice
zz % of partners and others that say we effectively share information
What we are doing to improve Complete by end
Carry out and publish themed inspection activity which examines
specific topics and includes the experience of people using
services and their carers of how integrated and coordinated their
care was June 2015
zz Mental health crisis care June 2015
zz Safety in hospitals December 2015
zz Neonatal care November 2015
zz People's involvement in decisions about their care December 2015
zz End of life care April 2016
zz Integrated care for older people April 2016
zz Diabetes support in the community March 2016
zz Do not attempt to resuscitate March 2016
zz Assessments of the quality of care in your locality (two places
to be examined in 2015/16, also see objective 6 below)
Undertake children’s safeguarding and looked after thematic March 2016
inspection with Ofsted, HMI Constabulary, HMI Probation and
HMI Prisons
Publish the State of Care report for 2014/15 October 2015
Publish Mental Health Act report for 2014/15 December 2015
Publish report on Deprivation of Liberty Safeguards November 2015
Part 2: Priorities in detail 19Priority 2 Shaping the future
2.1 Develop our response to future models of care and other changes;
develop our approach to assessing and encouraging improvement in the
quality of care services across providers and sectors; and involve the
public, our staff and our stakeholders in developing our future strategy
How we will know we are being successful
Strategic measures and KPIs
zz As we develop and test new approaches, we will make sure that they are fully
evaluated to ensure that they help us to deliver our purpose and are supportive of
future direction of health and social care
What we are doing to improve Complete by end
Regulating new care models; ensure our approach encourages
innovation and joined-up care; share good practice with providers
and the public:
zz Be clear with providers about how new care models will be
September 2015
registered
zz Ensure CQC Registration increasingly supports obligations and
evidence of intention to deliver care focused on individuals’ September 2015
needs; joined up care and working with others
Use our thematic reviews and other functions to test a variety March 2016
of approaches to assessing care pathways and coordinated care
provision, including looking at commissioning arrangements
Use our inspection findings to describe how well people in local March 2016
communities are served by their local health and care system and
build a comprehensive picture of quality of care in a local place,
identifying issues that need to be addressed at the system level
zz Carry out this approach in two places in 2015/16
Work with partners to encourage improvement:
zz Co-chair the National Quality Board
zz Review and share learning from new fundamental standards September 2015
zz Ensuring our approach supports services to improve, e.g. September 2015
through signposting to guidance improvement agencies and
examples of excellence March 2016
zz Review quality summit process to provide greater focus on
whole system improvement
Develop CQC’s new strategy for April 2016 to March 2021 and
beyond, involving the public, staff and stakeholders in shaping our
future:
zz Publication April 2016
20 Business Plan – April 2015 to March 2016Priority 3 Build an effective CQC
3.1 Recruit the full number of permanent staff, professional advisors and
Experts by Experience we need
How we will know we are being successful
Strategic measures and KPIs
zz % frontline posts filled
zz Turnover3.2 Develop the skills and knowledge of CQC staff through our Academy,
foster a culture that promotes health and well-being of our workforce
and embed our values of Excellence – Care – Integrity – Teamwork
How we will know we are being successful
Strategic measures and KPIs
zz Engagement index score and key staff survey results
zz % grievances received and number upheld
zz Turnover3.3 Embed our operating model (including systems and processes);
Implement a knowledge and information strategy
How we will know we are being successful
Strategic measures and KPIs
zz % of members of the public that say they trust CQC is on the side of people using
services
zz % of people who use services, public and care staff who say they were actively
involved in the inspection and judgement
zz % inspection reports published within 50 days of inspection
zz % of providers that tell us our guidance, inspection and report helps them to improve
zz Staff survey results relating to ease of working and improvement in systems
What we are doing to improve Complete by end
Our Operating Model describes how the organisation delivers on
its operational responsibilities. The Operating Model will make it
easy for colleagues to do the right thing, support decision making
about continuous improvement across the organisation; and
provide a prescriptive framework within which we operate:
zz Document and agree descriptions of the operating model April 2015
core functions and how they are intended to work, and the
quality standards, controls and assurances that apply to those
functions
zz Implement improvements to the operating model in the September 2015
following priority areas:
−− Improving the cost, quality and timeliness of inspection and
reporting
−− Improving management of staff
−− Identifying and managing provider risk systematically
−− Improving use of data and evidence across whole inspection
process
−− Reducing reliance on manual processes
−− Well established quality standards, controls and assurance
zz Identify and begin work on further systems and tools issues in September 2015
other Directorates supporting the operating model
Part 2: Priorities in detail 23Implement our Knowledge and Information strategy including:
zz Implement improvements to our Intelligence systems and tools, March 2016
records and data management, to support ease and accuracy of
collection of data by inspectors and to inform IS/ICT systems
review recommendations
zz Develop and extend our Intelligent Monitoring into a
comprehensive surveillance model, combining numerical data March 2016
and feedback from people who use care services. This will
enable CQC to better protect people who use services by
triggering action where concerns are raised.
24 Business Plan – April 2015 to March 2016Priority 4 Demonstrate the difference we make
4.1 Manage our quality, evaluate our benefits, costs and value for money,
improve our performance and manage our resources efficiently
How we will know we are being successful
Strategic measures and KPIs
zz Our value for money assessments demonstrate we are achieving our purpose and
becoming more efficient and effective
zz Management assurance evidence shows our Directorates are regularly considering
their key performance information, and are using it to deliver change and
improvement
zz Our corporate performance reporting shows performance improvements in required
areas
zz Our quality audits show we are managing our quality effectively
What we are doing to improve Complete by end
Manage and improve the quality and effectiveness of our
operating model through embedding a framework of quality
standards; controls and assurances within the our operating model:
zz Embed and improve assurance processes (peer review; regional June 2015
and national quality fora)
zz Deliver a programme of quality sampling* to monitor adherence Carried out and
to key quality checks and assurances and the impact this has on reported quarterly
regulatory decisions, and to continuously review and improve
zz Report to the Board on the findings bi-annually (key themes November 2015;
will be incorporated into performance reporting to the Board May 2016
and Department of Health)
*Quality sampling programme will be built around the key themes
of consistency and corroboration in use of evidence; quality of
draft inspection reports; timeliness of inspection report production
and publication; accountability and responsibility for oversight of
decisions; response to safeguarding concerns; registration; and
enforcement.
Develop our approach to efficiency savings across CQC for September 2015
2015/16 and 2016/17
Continue to implement our system of management assurance October 2015;
carrying out biannual self- assessments of each of our five February 2016
Directorates against the standards in these areas, using findings to
inform additional internal audits
Part 2: Priorities in detail 25To assess our value for money no less than once a year, June 2015
and continue to develop our programme of evaluation, our
understanding and evidence of the benefits we are delivering, and
measurement of our costs and the costs to providers and other of
our regulation, and use the evidence to improve
zz Develop our systems and processes to ensure we are capturing,
recording and reporting our costs accurately
zz Develop case studies of where we have brought about
improved care and sustained improvement
26 Business Plan – April 2015 to March 2016Annex 1: CQC new inspection approach timetable
Inspection categories Start of new . All first rating
approach inspections undertaken
Residential adult social care 1 October 2014 30 September 2016
social care
Adult
Community-based adult social care services 1 October 2014 30 September 2016
Hospice services 1 January 2015 30 September 2016
Out-of-hours 1 October 2014 30 September 2016
Primary medical services
GP practices 1 October 2014 30 September 2016
Dentists 1 April 2015 Will not be rated
Prison healthcare services 1 April 2015 No ratings planned
Remote clinical advice service (inc 111) 1 February 2015 111 by 30 Sept 2016
Urgent care services and mobile doctors To be piloted 3 Subject to regulations 4
Independent consulting doctors To be piloted 3 Subject to regulations 4
Acute hospital providers (NHS) 1 1 April 2014 31 March 2016
Hospitals
Acute hospital providers (NHS specialist) 2
1 January 2015 30 June 2016
Mental health community and/or hospital 1 October 2014 30 June 2016
providers (NHS)
Community health providers (NHS) 1 October 2014 30 June 2016
Ambulance service providers (NHS) 1 January 2015 30 June 2016
Mental health community/hospital providers 1 January 2015 30 June 2016
(independent)
Acute hospital providers (independent) 1 April 2015 31 December 2016
(includes cosmetic surgery providers)
Ambulance service providers (independent) Pilot 1 October 2015 Subject to regulations 4
Acute – single specialist providers To be confirmed Subject to regulations 4
(independent)
(1 October 2015 for (30 September 2016 for
termination of pregnancy) termination of pregnancy)
Acute – non hospital providers (independent) To be confirmed Will not be rated
(includes clinics and single handed
practitioners)
Community health providers (independent) To be confirmed 31 December 2016
Substance misuse (community & residential) To be confirmed Subject to regulations 4
providers (NHS & independent)
1 These all have A&E departments
2 Specialist trusts include those without A&E departments (total 19)
3 Piloting is to test methodology and determine the need for regulations
4 Subject to further discussions with the Department of Health and, where required, change to regulations
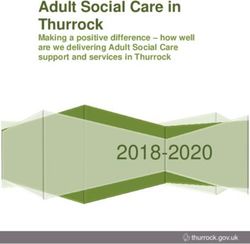
Part 2: Priorities in detail 27Annex 2: The CQC Board, Executive Team and Directorates
Chair and Board
David Prior
Chief Executive
David Behan
Strategy and Adult Social Care Hospitals Primary Medical Customer and
Intelligence Directorate Directorate Services Corporate
Directorate Directorate Services
Directorate
Executive Director Chief Inspector of Chief Inspector of Chief Inspector of Executive
Adult Social Care Hospitals General Practice Director
Paul Andrea Mike Steve Eileen
Bate Sutcliffe Richards Field Milner
FTE 585 FTE 1,037 FTE 603 FTE 341 FTE 949
Budget Budget Budget Budget Budget
Pay £29m Pay £55m Pay £35m Pay £24m Pay £30m
Non - pay £15m Non - pay £5m Non - pay £8m Non - pay £2m Non - pay £37m
Staff FTE numbers are those planned to be in place by 31 March 2016. Excludes £2m change budget. Total
budget includes £16m risk sharing agreement with the Department of Health to fund the costs of staff to
deliver the new approach to regulation. This will only be drawn on as required.
28 Business Plan – April 2015 to March 2016Annex 3: Budget
Budget
. Budget Difference.
2014/15 2015/16 2015/16
£m £m £m
Pay 162 179 17
Non-pay 61 70 9
Expenditure 223 249 26
Fee income (103) (113) (10)
Grant in aid 120 120 -
Risk sharing agreement* - 16 -
Depreciation 12 12 -
Total net expenditure 132 148 16
Capital 15 17 2
Includes budgets for Healthwatch England (£4m), Change (£2m), Chief Executive & Board (£1m) and Central budget
(£3m) not shown in the organisational chart in annex 2
Capital and depreciation budgets subject to Department of Health agreement
*Budget shown includes £16m risk sharing agreement with the Department of Health to fund the costs of staff to deliver
the new approach to regulation. This will only be drawn on as required.
Part 2: Priorities in detail 29Annex 4: Risk management arrangements
As a regulator we deal with risk on a day-to- Our process of escalation is simple and
day basis. We monitor and assess whether straightforward. Individual functions identify
providers are managing the different risks to and manage risks to the areas which they are
patients and people who use services that exist responsible for.
when delivering health and social care services.
Risks that cannot be managed at a functional
Poor risk management by providers can have
level or that are increasing are escalated to
significant impacts on members of the public.
the Executive Team for consideration, before a
We will bring to the attention of providers
decision is made to add a particular risk to the
risks that they may not have identified for
CQC Strategic Risk Register for the Board to
themselves. Finally, we must also ensure that we
be aware of. Board members will also identify
are managing the risks to our organisation in a
significant risks to the organisation from the
highly effective way and set the standard that we
wider health and social care system, as well as
expect of others.
considering those escalated from within CQC.
The CQC Board expects risk management to be
The Strategic Risk Register is presented to the
the responsibility of all staff, with appropriate
Board each quarter as part of the quarterly
action taken in line with this risk tolerance
performance report and is available on the CQC
statement. CQC’s risk management framework
website in advance of each Board meeting where
seeks to ensure that there is an effective process
performance and risks are discussed.
in place to manage risks across the organisation.
We manage risk through clear processes CQC has published its risk tolerance statement.
that emphasise the importance of public
accountability, openness, transparency, integrity,
and judgement.
We look to adopt a top-down as well as a
bottom-up approach to risk management.
30 Business Plan – April 2015 to March 2016Annex 5: Strategic measures and key performance indicators by priority and objective
Priorities and objectives
1 2 3 4
Strategic measures and KPIs
Monitor Inspect Rate
Put people at the
heart of what we do
Register
Enforce
Independent voice
Shaping the future
Recruit the full
number of staff
Training./wellbeing
values
Embed operating
model
Manage quality,
evaluate benefits/cost
& VFM
Impact % of services rated outstanding, good, requires improvement, or inadequate
% of providers agree our guidance, inspection and reports helps them to improve
% of providers rated inadequate or requires improvement that improve on revisit
% of people tell us they trust CQC are on the side of people who use services
% of people who say reports help them make choices/useful to other stakeholders
Outcomes
% of partners say we effectively share information work with them to address failure
% of newly registered providers where regulatory response is required
% of providers who tell us registration process is a robust assessment
% Intelligent Monitoring bandings in line with ratings
% of people who use services who say they were actively involved in inspections and judgements
% of ratings challenged and upheld; number of judgements providers say were fair
% of providers still not meeting fundamental standards after improvement deadline
% of providers not meeting fundamental standards (and for how long)
% of partners who say we share information effectively/ act together with them
Quality and effectiveness
% of people who say reports help them make choices and are useful
% of completed registrations (within 50 days)
% of first ratings inspections undertaken
% of safeguarding alerts and concerns we follow up within target times
Number of enforcement actions, prosecutions and special measures undertaken
% of inspection reports published within 50 days of inspection
% Mental Health Act visits planned each quarter completed
SOAD requests undertaken within target time
% of complaints about CQC and % upheld at stages 1 and 2
% of calls answered in 30 seconds
% e-mails answered in 10 days
% of frontline posts filled; turnoverYou can also read