Cardiac Rehabilitation: Is it important with Modern Interventional Reperfusion Techniques?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
18 Cardiac Rehabilitation
Cardiac Rehabilitation: Is it important with Modern
Interventional Reperfusion Techniques?
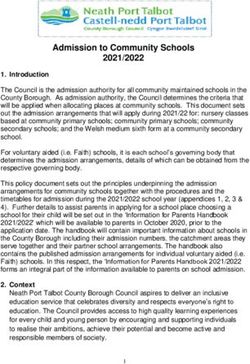
Interventions (PCI) have a Level One must also consider that
Written by Padraig Denn, 1A recommendation from a both CABG and PCI reperfusion
Clinical Nurse Manager 3, multitude of international bodies. techniques are limited to the
Mater Private Network Figure 1 below identifies the type three main coronary arteries
of patient that is best suited to the and a limited number of branch
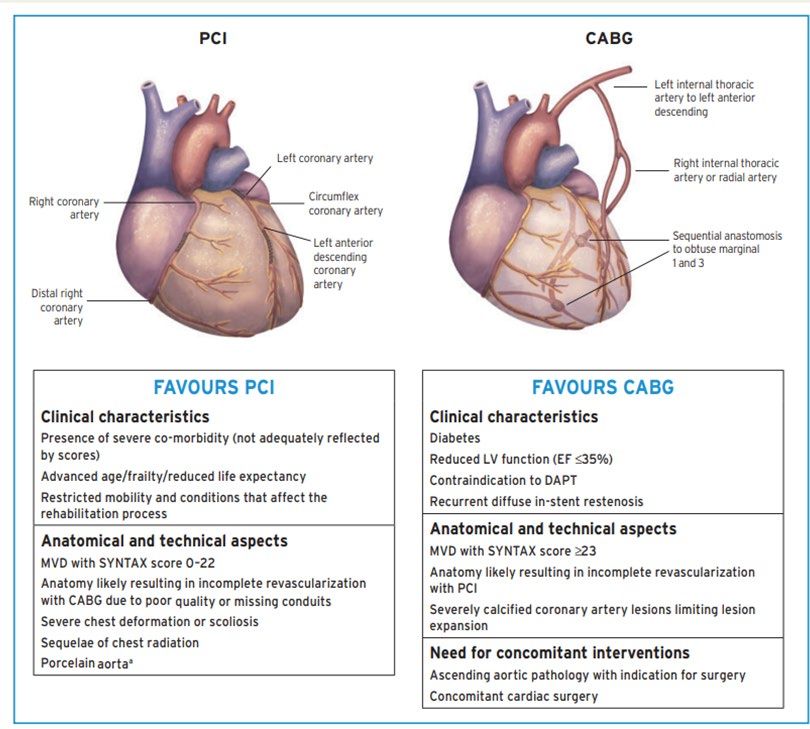
PCI versus CABG intervention. vessels. Therefore, when we
look at Figure 2 we can see that
However, this level of
the coronary perfusion system
recommendation is only valid
is far more elaborate than the
for proven ischaemic or flow
three main arteries and main
limiting coronary disease. New
branches. Therefore, we can see
research released initially in 2019
why pharmacological treatment
has proven that PCI and CABG
after initial intervention for the
have no additional benefit for the
management of certain risk
management of non-ischaemic
factors of coronary artery disease
coronary disease above medical
(CAD)is necessary. However,
therapy. Research has shown
an individual’s tolerance of
that utilisation of non-internal
pharmacological treatments
mammary vascular conduits
varies significantly and in the
for CABG have limited duration
era of an ageing population
of patency especially if there
Reperfusion techniques have to most recent drug eluting with multiple co-morbidities
is competitive flow from the
their origins in the work of the risk of polypharmacy needs
stents and techniques allow native system. PCI techniques
to be considered and can
Alexis Carrell in the early 20th those appropriately trained and are limited to specific areas of
century with his initial concepts experienced to treat the most coronary disease and care needs
regarding coronary perfusion complex of coronary disease to be taken to prevent inadvertent
and subsequent intrathoracic including chronic total occlusions. occlusion of branch vessels
anastomosis of aorta and which can cause on-going
myocardial tissue in dogs. This Both Coronary Artery symptoms of angina after
eventually lead to a technique Bypassing Grafting (CABG) successful treatment of a
Figure 1: PCI Vs CABG
of attaching an adjunct artery and Percutaneous Coronary significant coronary occlusion.
into the myocardium of the left
ventricle with the theorised result
that collateral perfusion would
be provided to the left anterior
descending (LAD) coronary artery
called the Veinberg procedure.
This work was developed further
when Ake Senning placed a patch
over the left main stem (LMS)
to improve blood flow. Modern
coronary artery bypass grafting
was eventually an option when
Mason Sones inadvertently
injected contrast dye into the
right coronary artery (RCA) of
a patient with rheumatic heart
disease and mapped the coronary
perfusion system allowing
for direct identification of the
coronary arteries. This discovery
allowed conduit vessels to be
attached directly to blocked
arteries and thus “bypassing”
the occlusions. This has been
refined in the subsequent years
to now being carried out very
effectively utilising microsurgical
techniques with various vascular
conduits to bypass blockages in
main coronary arteries as well
as branch vessels. Such
techniques allow for early
discharge and reduced adverse
events as a result.
Similarly, percutaneous
interventional reperfusion has
had significant improvements
since the early work of the
Italian Dr Gruentzig. From the
initial treatments with balloons
FEBRUARY 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE Figure 1: PCI Vs CABG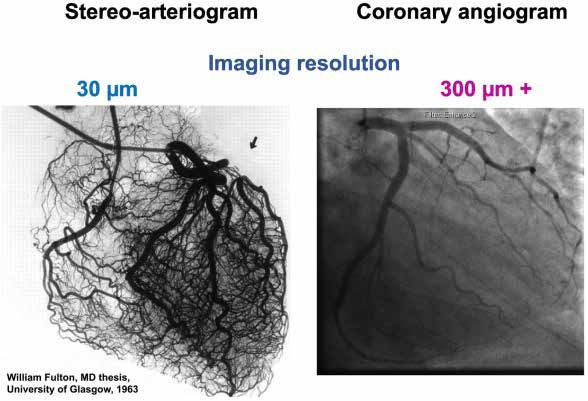
20 Cardiac Rehabilitation
of the COVID 19 pandemic
some facilities have had their
nursing allocation decimated for
prolonged periods due to the
acute care service needs.
It is recommended that the CR
programs be multidisciplinary
to ensure all specialities expert
knowledge is utilised to better
educate the participants on
how best to manage their
condition independently in the
community setting. It is this that
is the cornerstone of the CR
programs. CR phases one and
two are designed to ensure that
participant takes personal
change of the management of
their disease.
In phase I, according to the IACR
guidelines, patients are usually
hospitalised for two to five days
after a significant cardiac event.
It is at this time when the CR
process should commence with
the visit of a member of the CR
team. The duration of stay is
dependent upon the cause of the
patient’s admission to hospital.
The recommendation of the IACR
It is for the above, and many service is overseen by the Irish
Figure 2: Representation of guidelines is that this phase of the
Coronary Perfusion other, research guided reasons Heart Foundation (IHF).
programme should involve
that Cardiac Rehabilitation (CR)
CR in Ireland is recommended to
has a Level 1A recommendation • Give support and information
be delivered on a phased basis.
for all those who have a confirmed to the patient and their families
Figure 3 identifies the four phases
often complicate the decision- diagnosis of CAD without any about heart disease
of CR in Ireland. According to
making processes of effective restrictions from the initial causes
IACR information prior to the • Assist the patient to identify
pharmacological treatment of the or treatment modalities utilised for COVID 19 pandemic CR was personal cardiovascular
risks of CAD. the management of the disease. delivered in thirty-seven centres risk factors
A Cochrane systematic review across Ireland, mostly in the
We must also note that CAD and meta-analysis has shown that • Discuss lifestyle modifications
causes are multifactorial (See acute care setting. The services
participation in a CR programme appeared to have stagnated over of personal risk factors and help
Table 1) and many of them reduces cardiovascular mortality, provide an individual plan to
the previous ten years and were
cannot be managed either reduces hospitalisations support these lifestyle changes
often provided by the nursing
pharmacologically or with invasive
interventions. Risk factors such as Figure 2: Representation of Coronary Perfusion
and improves quality of life.
International governing bodies
profession alone in each setting,
• Gain support from family
despite national and international
increased body mass index (BMI), members to assist the
have recommended the utilisation recommendations that CR be patient in maintaining the
increased alcohol consumption,
poorly managed levels of stress We must also note that CAD causes are multifactorial (See Table 1) and man
of CR for the management of
CAD leading to CR reported to
provided by a multidisciplinary
team (MDT). The guidelines
necessary progress
and smoking all require more
complex interventions to ensure cannot be managed either pharmacologically or with
be utilised in nearly one-hundred
and twenty countries worldwide. invasive interventions.
recommend that the MDT is made
• Plan a personal discharge
up of physiotherapists, social
activity programme and
that they are effectively
managed without worsening the such as increased body mass index (BMI), increasedencourage
CR in Ireland falls under the remit
of the Irish Association of Cardiac alcohol consumption,
workers, occupational therapists,
the patient to
psychologists and administrative
adhere to this and commence po
risk of polypharmacy.
levels of stress and smoking all require more complex interventions to ensur
Rehabilitation (IACR) and this staff. Unfortunately, for periods
daily walks
effectively managed without worsening the risk of polypharmacy.
Table 1: Risk Factors for CAD
Table 1: Risk Factors for CAD
FEBRUARY 2022 • HPN | HOSPITALPROFESSIONALNEWS.IE
21
Figure 3: Phases of Cardiac
Rehabilitation
Phase I: In hospital Phase lI: Post discharge
patient period pre exercise period
Cardiac
Rehab
participating sites to complete
Excel spreadsheets regarding
numbers and outcomes for
Phase III: Exercise and individual patients through each
Phase lV: Maintenance CR site but this information has
Education Programme not yet been made public.
International research has
shown that CR is inconsistently
implemented not only between
countries but within individual
countries. Further research
has shown that guideline
implementation is often improved
• Inform patients regarding of exercise in this phase which • Stress management and through the utilisation of
Phase II and Phase III is often self-directed and is relaxation techniques Information and Communication
programmes, if available, and dependent upon the initiating Technologies (ICT). The use of
encourage their attendance event that caused the referral to • Counselling and behaviour such technologies may also assist
modification as we migrate from previous
the CR system.
The CR member who meets group setting for CR to the new
with the patient in this phase is • Smoking cessation COVID restriction limitations on
Phase III is a structured
dependent upon the structure of longitudinal exercise programme • Vocational counselling indoor group activities, allowing
the programme in that specific that entails regular attendance for remote interaction of groups.
setting. Ideally education on (most often twice weekly for six This phase is dependent upon The CR team in the Mater Private
the components of the CR weeks) and each session the expertise of the MDT to Cork have managed to utilise
programme (e.g. disease process, involves a warm-up, aerobic ensure that all components of the Skype to allow for group exercise
medication management, exercise and cool down phase. Some programme are met. and education sessions to be
regime) should be provided programmes may also include facilitated without impinging on
by those with that specific Phase IV of CR is designed to the restrictions in effect during
heart rhythm monitoring and consolidate the improvements in
expertise (e.g. CNS, Pharmacist, resistance training. this international pandemic.
Physiotherapist). This phase is exercise levels and to reinforce Further utilisation of ICT should
also an opportunity for the patient According to the IACR 2013 the education provided in be considered not only to assist
to become actively involved in Guidelines Phase III comprises Phase III. The aim is to maintain the members of the MDT to
their own care through completion all the following: lifestyle changes to best ensure effectively document the various
of assessments and identification long-term change. This can be components of CR programs
of their own risk factors for CAD. • Exercise prescription based facilitated in several settings if but to subsequently assess
This will facilitate the patient to on clinical status, risk there are appropriately qualified the effectiveness of individual
take ownership of their condition stratification, previous activity and experienced providers of programs and potentially improve
and its future management. and future needs this phase of the programme. the effectiveness of programs.
The focus of this phase of Unfortunately, this appears to be
• Education for patient and an area that is lacking in Ireland It is clear that the utilisation
the programme is to create
family regarding: with only ten recognised providers of CR for those who have a
an individualised plan of care
for each patient. This involves of Phase IV CR and only one of confirmed diagnosis of CAD is
• Cardiac anatomy and physiology
assessments of the various the thirty-seven registered CR clearly beneficial for the long-
related to the cardiac event term outcomes of patients
components of CAD including sites providing this phase within
psychological status, risk factor • Recognition of cardiac pain and their facility. irrespective of the interventional
profile, activity level, smoking symptom management reperfusion method utilised for
There is no published evidence confirmed occlusive CAD. CR is
and others. Based on these
• Risk factor identification as to what extent each of the designed to equip the participant
assessments appropriate referrals
and management thirty-seven sites for CR in Ireland with the skills and knowledge to
should be made to relevant
adhere to these guidelines. The best manage all aspects of their
healthcare professionals. • Benefits of physical activity author was further unable to gain lifestyle to reduce symptoms of
In Phase II the aim is to reinforce • Energy conservation/graded access to any official numbers and progression of their CAD.
the education that was provided return to activities of daily living of patients that attend each of It is also designed to create a
in Phase I and to maintain the programmes. Similarly, there support network for on-going
lifestyle changes. It happens • Cardio protective healthy eating is no available information to management of symptoms and
after discharge but prior to the the author regarding the short, the psychological impact of a
commencement of Phase III. It • Prescribed cardiac medication medium or long-term benefits diagnosis of CAD. Therefore,
can occur in a wide variety of and importance of compliance of CR programmes in Ireland Cardiac Rehabilitation should
settings (e.g. phone contact, with same as any information regarding be considered a pivotal
clinic reviews, patient’s own • Resumption of sexual activity this is generally maintained in treatment modality for any
home or GP’s office). The patient site specific databases. The individual with a diagnosis of
should commence some degree • Benefits and entitlements IACR have previously requested coronary artery disease.
HOSPITALPROFESSIONALNEWS.IE | HPN • FEBRUARY 2022You can also read