Cerebral palsy lifetime care - four musculoskeletal conditions
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY REVIEW
Cerebral palsy lifetime care – four musculoskeletal conditions
KEVIN P MURPHY MD 1 , 2 , 3
1 Gillette Specialty Healthcare Northern Clinics. 2 Department of Physical Medicine and Rehabilitation University of Minnesota Duluth. 3 Minnesota Army National
Guard Medical Corps., MN, USA
Correspondence to Kevin P Murphy, Gillette Specialty Healthcare Northern Clinics 1420 East Londen Road, Suite 210, Duluth 55805, MN, USA. E-mail
kmurphy@gillettechildrens.com
CONFLICTS OF INTEREST Cerebral palsy (CP) has always been considered a static condition in the
The author declares no conflicts of interest. neurological sense. Secondary and associated conditions that occur in the
patient with CPcan progress over time and cause unwanted sequelae. This paper
discusses four musculoskeletal conditions that present across the lifetime and
can lead to progressive loss of function in the patient with CP. Patella alta can be
particularly painful in the early adult years, limiting mobility particularly when
associated with crouch gait. Adults with lower-extremity weight-bearing status
having hip dysplasia, progressive over time, often develop pain and severe
degenerative arthritis, with or without arthrodesis. Spondylolysis, particularly at
the L5 S1 level, is fairly common in the ambulatory adult with diplegia and may,
if not diagnosed early, progress to spondylolisthesis. Cervical stenosis appears
to be more prevalent in adults with spastic quadriparesis and dystonia and is
often associated with myelomalacia and ⁄ or radiculopathy. All four of these
conditions may be lessened, or even prevented, with intervention and diagnosis
in the younger years. Possible interventions and outcomes over time are
discussed in the context of multidisciplinary team management of the individual
with CP.
By definition, the primary condition of cerebral palsy (CP), too often seen as expected sequelae of living with CP, and
in the neurological sense, has always been considered non- no effort is made to pursue a more specific diagnosis.
progressive over time.1,2 Secondary conditions develop A person presenting with a headache may be told that
over time as a result of the CP; they include soft-tissue ‘everybody with cerebral palsy develops headaches at some
contractures, degenerative arthritis, and equinovalgus foot point in time,’ and no further effort at diagnosis is made.
deformities. These conditions can be prevented with Strauss et al.5 in reviewing the public health record for the
appropriate intervention and early diagnosis.3,4 Associated State of California, reported a surprisingly higher risk of
conditions are those that occur with increased prevalence brain cancer in people with CP. With the patient with CP,
in individuals with CP; they include visual or auditory as with any individual presenting with symptoms of medi-
impairment, learning disability, and gastroesophageal cal or surgical need, the main initial goal should be to
reflux. These conditions cannot always be prevented, but establish a correct diagnosis. This will never be achieved if
their impact can be lessened by early diagnosis and inter- we too easily attribute loss of function and medical symp-
vention during the developmental years. Comorbidities toms to the primary condition of CP.
(e.g. diabetes, hypertension) are conditions unrelated to Adults with CP, like other individuals with developmen-
the primary disability. They appear with a similar fre- tal conditions, are living longer as a result of improvements
quency, regardless of a diagnosis of CP. In the author’s in medical and surgical care.3,6–14 With aging come certain
experience, medical care providers too often blame the pri- conditions that can cause pain and significant loss of func-
mary condition for virtually all the symptoms and prob- tion. This article identifies four musculoskeletal conditions
lems that develop in the adult with CP. Symptoms such as that may be problematic over the lifetime. The first three
leg pain, discomfort in the lower back, and headaches are are felt to be preventable, and the impact of the fourth can
ª 2009 The Author Journal compilation ª 2009 Mac Keith Press Developmental Medicine & Child Neurology 2009, 51 (Suppl. 4): 30–37
30 DOI: 10.1111/j.1469-8749.2009.03431.xbe lessened if the condition is identified and intervention is Medical and surgical measures to minimize crouch gait
undertaken during the developmental years. during the developmental and preadolescent years are
encouraged. Such measures include maximizing the knee-
PATELLA ALTA ankle-foot extension couple and hamstring, quadriceps and
Patella alta is a relatively common condition in ambulatory hip flexor stretching, and strengthening the weight-bearing
adults with CP and spastic diplegia.15,16 It is often associ- soft tissues.18,24–26 Excessive tightness to the rectus femoris
ated with anterior knee pain that begins in preadolescence muscle can contribute to this and may even facilitate more
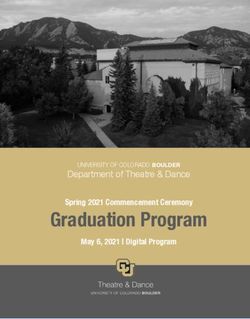
or adolescence and progresses over time. An Insall ratio of a recurvatum deformity.21 In the author’s opinion, more
greater than 117 is generally observed on lateral radio- emphasis could be given to quadricep stretching, which
graphs (Fig. 1). This ratio is determined by dividing the may help minimize patella alta in children with CP.
length of the patellar tendon (measured from the posterior Increased prone lying exercises and abdominal strengthen-
surface of the lower pole of the patella to its insertion on ing to minimize anterior pelvic tilt should provide
top of the tibial tubercle) by the greatest diagonal length of additional benefit. In the young and middle-aged patient,
the patella in at least 30 flexion.17 The ratio should be benefit may be achieved with taping of the patella into
approximately 1, with less than 20% variation. Not a more midline position so that it can track better within
uncommonly, the condition is seen with crouched gait, the trochlear groove. Insall and colleagues16 noted that
which limits the distance a patient can walk and contributes clinical results correlated better with patellar congruence
to further biomechanical and lever-arm dysfunctions.18-20 than with severity of chondromalacia at the time of
Stress fractures may occur at the inferior pole of the patella operation. A Neoprene patellar-tracking knee orthosis
with palpable tenderness; excision is required when conser- may further reduce symptoms. Interarticular injections
vative care fails.21 Subluxation and dislocation of the with a long-acting steroid and anesthetic combination
patella are additional complications.22,23 can provide relief for 6 months or more. The author has
also utilized clostridium botulinum toxin A (BoNT-A)
injections to the distal quadriceps mechanism to help relax
the superior patellar soft tissues. This is followed by a
myofascial technique in ‘milking down’ the patella to a
position closer to the center and midline of the knee joint.
Physical therapy and nonsteroidal anti-inflammatory
agents can be of additional help as part of a conservative
care program.
When conservative care is no longer effective in the
skeletally mature individual having progressive crouch
gait, aggressive surgical options should be considered.
These include multilevel operative, including correction
of femoral and tibial torsion, equinovalgus foot defor-
mities, distal femoral extension wedge osteotomies,
patellar and tibial tubercle advancements, and hamstring
lengthening, in addition to rectus femoris transfers.18,20
Close monitoring of the patellar position over the devel-
opmental years, with heavy focus on preventive strategies
as discussed above, may prevent symptomatic patella alta
and the need for more multilevel orthopedic surgery later
in life.
HIP DYSPLASIA, WEIGHT BEARING, AND
DEGENERATIVE ARTHRITIS
Hip displacement occurs in approximately 1% of patients
with spastic hemiplegia, 5% of those with diplegia, and
up to 55% of those with quadriplegia.22,27 Pain with
Figure 1: Patella alta in an ambulatory adult with cerebral palsy. Lat- degenerative arthritis and joint-spacing incongruity can
eral view. occur over time in at least 50% of individuals with
CP having dislocated hips and ⁄ or pseudoacetabular
Musculoskeletal Conditions in CP Kevin P Murphy 31formation.28–31 This problem is of particular concern in 6 months or more. These injections are often done under
an individual having weight-bearing functions in the fluoroscopy with an arthrogram identifying intra-articular
lower extremities. Weight bearing can be as simple needle placement before assure optimal drug placement
as standing pivot transfers, standing table usage on a and dispersion throughout the articulating surfaces
regular basis, limited household or community ambulatory (Fig. 2).
skills, and crawling. Pain and osteoarthritic changes can Figure 3 shows severe degenerative arthritis with
result in a progressive loss of functional weight bearing pseudoacetabular formation (greater at the right than at
and mobility. Early identification and intervention in the the left) in a 42-year-old male with spastic diplegia. In the
younger child should prevent significant hip dislocation five years before surgery, his ambulatory function had
and pseudoacetabular formation in most individuals. decreased markedly; from more than a mile to less than 10
Screening radiographs at least every 6 to 12 months steps. Severe loss of hip motion was present, limiting hip
after the age of 18 months should identify subluxation abduction to less than 15 with near arthrodesis bilaterally.
or dysplasia early, with hip and acetabular reconstruction Figure 4 shows the same individual one year after he had
as appropriate thereafter. Managing the hip at risk to undergone bilateral total hip arthroplasties. The right hip
flexion contractures less than 20 and functional abduction
of at least 45 in extension at 60 in flexion should be
helpful.22 BoNTA injections to the adductor longis and
hip flexor soft tissues, in addition to phenol obturator
neurectomies, can decrease excessive adduction and
flexion of the hips.32 Spasticity reduction from intrathecal
baclofen can help improve hip positioning and decrease
scissoring. This can be combined with a night-time
abduction hip orthosis to maintain a more centered
position of the proximal femoral head. In the skeletally
mature individual with joint space incongruity and
severe osteoarthritis, intra-articular injections of a long-
acting steroid and anesthetic can provide relief for up to
Figure 3: Severe degenerative arthritis with pseudoacetabular for-
mation in a 42-year-old adult with cerebral palsy and spastic diplegia.
Preoperative status.
Figure 2: Arthrogram identifying needle placement before hip intra-
articular injection with depomedrol and 0.5% bupivicaine in an ambu- Figure 4: Same individual as in Figure 3, one year following bilateral
latory adult with cerebral palsy. total hip arthroplasty.
32 Developmental Medicine & Child Neurology 2009, 51 (Suppl. 4): 30–37was operated on first; the left hip approximately four Reports in the literature have identified the prevalence
months later. The surgery was performed by an adult and of spondylolysis in weight-bearing adults with CP with or
a pediatric surgeon simultaneously as neither felt comfort- without dystonia as between 21% and 30%.21,45,46 This
able doing the operation alone. The patient can now again prevalence may be higher in individuals who have under-
walk pain-free almost a mile, using a single-tip cane in the gone selective posterior rhizotomy and with associated
left hand. Total hip arthroplasties have been reported safe increased anterior pelvic tilt.47–49 In a series of 143 patients
and effective for selected individuals with severe degenera- who had never walked and in whom the condition of CP
tive arthritis and pseudoacetabular formation.21,33–35 dominated, no cases of spondylolysis or spondylolisthesis
Constrained acetabular components may be more effective were detected radiographically.50 Dystonic involuntary
in reducing recurrent dislocation risk, particularly in movements through the lumbosacral spine, particularly
individuals with dystonia.36 Long-term follow-up studies into extension and axial rotation, appear to contribute to
have shown 94% pain relief and improved function over the higher incidences of spondylolysis in this popula-
time, even in patients operated on at the relatively young tion.45,51 Figure 5 displays spondylolysis bilateral at the
age of 30 years.37 Wear and tear appears to be minimal, L5 S1 level in a 35-year-old ambulatory male with
which may relate to the fact that the adult with CP takes cerebral palsy, spastic diplegic type. He had been experi-
fewer steps per day and over time. Proximal femoral head encing back pain for over 3 years (explained by his primary
resections, either Castle or Girdlestone type,38,39 may be care physician as ‘usual and expected’ for people with CP).
helpful in individuals who have no weight-bearing status His symptoms improved greatly with conservative care,
for the lower extremities. including temporary lumbosacral corset, core strength-
The question of crawling needs to be addressed ening, and pelvic-stabilization routines to decrease
before any surgical intervention, as most individuals will anterior pelvic tilt and minimize toe walking. A grade I
not offer this information on their own. The author has spondylolisthesis, non-progressive over time, was also
observed one non-ambulatory individual with a dislocated noted. Within 6 months of treatment his symptoms had
osteoarthritic hip who crawled within his home. The abated and he was again able to enjoy bowling, his favorite
individual, having never been asked about crawling, had recreational sport.
a Girdlestone procedure. This eliminated his ability to Efforts to minimize anterior pelvic tilt in weight-
crawl. As a result, he could no longer live independently bearing children with CP may help prevent stress fractures
and was forced to enter institutional care. The need to through the pars interarticularis of the lumbar spine. This
question individuals on crawling behavior cannot be is particularly important in patients undergoing selective
overemphasized.
The possibility of self-injury needs to assessed pre- and
postoperatively. Patients can scratch at their own surgical
incisions and disrupt traction units and immobilization
devices if not carefully managed. Pain management needs
to be assessed, especially in individuals with limited
communication skills and variations of expression.
End-stage hip disease in weight-bearing adults with CP is
virtually certain to result in loss of gait and mobility. In
such situations, total hip arthroplasty is an attractive
option, despite the associated risks and complications.
SPONDYLOLYSIS
Spondylolysis is an acquired condition thought to be
related to a stress fracture through the pars interarticu-
laris resulting from repetitive hyperextension.15 The pre-
valence of spondylolysis has been estimated at 4.4% at
6 years of age, increasing to the adult rate of 6% by
14 years of age.40 With one exception, a defect in the pars
interarticularis has never been identified at birth.41–44
Spondylolisthesis can be associated with spondylolysis, Figure 5: Spondylolysis, bilateral, at the L5 S1 level, in a 35-year-old
the development of which is infrequent after the age of ambulatory male with cerebral palsy.
6 years in able-bodied children.22
Musculoskeletal Conditions in CP Kevin P Murphy 33posterior rhizotomy and ⁄ or aggressive hamstring length- Ex : 4687 05/20/96
ening, especially in the presence of tight hip flexor mus- Se : 3/3 R0.0
cles.18 BoNT-A injections may help in the treatment of Im : 12/22
incapacitating painful dystonia of the lumbar paraspinal
muscles52 facilitating optimal sitting and standing postures
in the hope of preventing future spondylolysis. Other med-
ications and treatments, along with physical therapy, activ-
ity modification, gait aids, and power mobility when
necessary, may offer additional protective factors against
stress fractures through the pars interarticularis. Careful A P
monitoring through serial radiographs of the lumbar spine 5 6
in those individuals at increased risk can allow early 1 9
detection and intervention. Surgical options, including
segmental fusion in the presence of failed conservative
intervention and any neurological compromise, should be
used when necessary. Home exercise, including prone
lying techniques; stretching of hip flexors, hamstrings, and
gastrocnemius muscle groups; abdominal strengthening;
and utilizing appropriate orthotics to minimize toe walk-
ing, is always important. Symptomatic pre-stress fractures
of the pars interarticularis also need to be considered;
nuclear medicine bone scans may assist diagnosis. The
patient history should include a review of any falls or injury
to the lumbar-pelvic region because the patient may not
always recall more-distant traumatic etiologies at the time
of medical evaluation.
Figure 6: MRI of a 38-year-old male with cerebral palsy, spastic
CERVICAL STENOSIS quadriparesis, and cervical dystonia. Segmental encroachment is
One study has shown that the incidence of cervical stenosis noted, particularly at the C4 and C5 levels, with canal compromise.
is higher in adults with CP and athetosis than in other indi-
viduals.53 In this study, 180 patients with cerebral palsy
and athetosis, when compared with 417 controls, showed
an eight-fold increased frequency of early cervical disc preceding 6 months. Surgical decompression with poster-
degeneration and a six- to eight-fold increase in listhetic ior fusion and wiring was provided and the patient
instability in the midcervical spine. The combination of regained his former ability to walk and engage in self-care
disc degeneration with listhetic instability and narrowed functions within 8 months. The individual aspirated upon
spinal canal may predispose these individuals to rapid intubation at the time of surgery and required an additional
progressive loss of function and devastating neurological 2-month stay in the intensive-care unit. Twelve years after
deficit.54 surgery, he maintains independent living skills, can walk,
Additional studies have noted that adults with CP and and requires minimal supervision within his community
athetosis have higher rates of cervical spondylosis and group home residence.
myelopathy, often associated with dystonic contorsional Serial MRIs every 2 years in individuals at higher
head and neck postures.55–63 risk, beginning in young adulthood, may help identify
Figure 6 displays an MRI of a 38-year-old male with cervical spondylosis and stenosis early and allow for
CP, spastic quadriparesis, and cervical dystonia. Segmental proactive intervention and prevention of unwanted
encroachment with canal compromise can be noted, partic- sequelae. BoNT-A injections, along with postural adjust-
ularly at the C4 and C5 levels. This individual was inde- ments and supports, may help minimize cervical dystonia,
pendent with all of his self-care functions and had limited particularly into extension and axial rotation.52 Medica-
community ambulatory ability one year before discovery of tions for control of dystonia are encouraged, including
his cervical stenosis. At time of diagnosis he had stopped intrathecal baclofen therapy in carefully selected indi-
walking and lost bladder control; he had also shown signs viduals. Placing the patient in a calm environment, use
of increased truncal and lower-extremity spasticity in the of sensory biofeedback techniques, and stress reduction
34 Developmental Medicine & Child Neurology 2009, 51 (Suppl. 4): 30–37may also reduce regional dystonia. The author can recall over time is rapidly progressive in this population. For
a patient who, when flying alone in her glider plane, this reason, surgical intervention seems warranted when
was completely relieved of her dystonic features until conservative care has failed to maintain function and a
touchdown, when the ground support staff would come comfortable lifestyle. Early identification and inter-
to her assistance. Cervical discomfort of any sort should vention can, it is hoped, help prevent the unwanted
be taken seriously in this population, as it may be the sequelae of cervical stenosis in this population or at least
only sign of more-devastating neurological compromise. minimize the surgical intervention required to accom-
Serial neurological examinations adapted for individuals plish that objective.
with CP are encouraged. Measurement of certain repro-
ducible voluntary motor functions over time, using a CONCLUSION
clinically reproducible spasticity measure, is suggested. Four musculoskeletal conditions have been discussed
Close monitoring of bowel and bladder functions for within the context of lifetime care for the individual with
changes in frequency, urgency, retention, and continence CP. Further investigation and study seem warranted, in
is advisable. Should conservative measures fail, surgical view of the progressive nature of these four conditions.
decompression of the stenotic cervical canal may be Other, yet to be identified secondary and associated condi-
required. There is a tendency toward a more anterior tions are likely to be present, both within and outside of
approach and interbody fusion with posterior wir- the musculoskeletal system, in the adult with CP. Medical
ing.59,62,64–66 The high risk of surgery, including regio- providers should take care not to blame symptomatology
nal dystonia in the surgical zone, aspiration potential, on the primary condition of CP when other etiologies
bleeding, and limited options for utilization of immobili- exist. Early identification and intervention to prevent
zation devices, should not be overlooked. Nonetheless, unwanted loss of function and lifestyle are the ultimate
cervical stenosis associated with serious functional loss goals.
REFERENCES 9. Murphy KP, Molnar GE, Lankasky K. of incongruence. Clin Orthop Relat Res
1. Ropper AH, Brown RH. Adams and Vic- Employment and social issues in adults 1983; 176: 217–24.
tor’s principle of neurology, 8th edn. with cerebral palsy. Arch Phys Med Rehabil 18. Gage JR. The treatment of gait problems
Columbus, OH: McGraw-Hill, 2005. 2000; 81: 807–11. in cerebral palsy, 2nd edn. London: Mac
2 McCormick A, Brien M, Plourde J, Wood 10. Young NL, Steele C, Fehlings D, Jutai J, Keith Press, 2004.
E, Rosenbaum P, McLean J. Stability of Olmsted N, Williams JI. Use of healthcare 19. Hoffinger SA, Rab GT, Abou-Ghaida H.
Gross Motor Function Classification among adults with chronic and complex Hamstrings in cerebral palsy crouched
System in adults with cerebral palsy. physical disabilities of childhood. Disabil gait. J Pediatr Orthop 1993; 13: 722–6.
Dev Med Child Neurol 2007; 49: 265– Rehabil 2005; 27: 1455–60. 20. Rodda JM, Graham HK, Nattras GR,
69. 11. Rimmer JH. Physical fitness levels of per- Galea MP, Baker R, Wolfe R. Correction
3. Turk MA, Scandale J, Rosenbaum PF, sons with cerebral palsy. Dev Med Child of severe crouch gait in patients with spas-
Weber RJ. The health of women with Neurol 2001; 43: 208–12. tic diplegia with use of multilevel ortho-
cerebral palsy. Phys Med Rehabil Clin N 12. Hemming K, Hutton JL, Pharoah PO. paedic surgery. J Bone Joint Sur Am. 2006;
Am 2001; 12: 153–68. Long-term survival for a cohort of adults 88: 2653–64.
4. Turk MA, Geremski CA, Rosenbaum PF, with cerebral palsy. Dev Med Child Neurol 21. Morrell DS, Pearson JM, Sauser DD.
Weber RJ. The health status of women 2006; 48: 90–5. Progressive bone and joint abnormalities
with cerebral palsy. Arch Phys Med Rehabil 13. Rapp CE Jr, Torres MM. The adult with of the spine and lower extremities in
1997; 78:(12 Suppl. 5) S10–7. cerebral palsy. Arch Fam Med 2000; 9: cerebral palsy. Radiographics 2002; 22:
5. Strauss D, Cable W, Shavelle R. Causes of 466–72. 257–68.
excess mortality in cerebral palsy. Dev Med 14. Kemp BJ. What the rehabilitation pro- 22. Morrissy RT, Weinstein SL. Lovell and
Child Neurol 1999; 41: 580–5. fessional and the consumer need to know. Winter’s pediatric orthopedics, 6th edn.
6. Murphy KP. Medical problems in adults Phys Med Rehabil Clin N Am 2005; 16: 1–18. Philadelphia: Lippincott Williams & Wil-
with cerebral palsy: case examples. Assist 15. Able MF. Orthopedic knowledge update. kins, 2006.
Technol 1999; 11: 97–104. Rosemont, IL: American Academy of 23. Simmons E Jr, Cameron JC. Patella alta
7. Granet KM, Balaghi M, Jaeger J. Adults Orthopedic Surgeons, 2006. and recurrent dislocation of the patella.
with cerebral palsy. N J Med 1997; 94: 16. Insall JN, Aglietti P, Tria AJ Jr. Patellar Clin Orthop Relat Res 1992; 274: 265–9.
51–4. pain and incongruence. II: clinical applica- 24. Andersson C, Grooten W, Hellsten M,
8. Murphy KP, Molnar GE, Lankasky K. tion. Clin Orthop Relat Res 1983; 176: Kaping K, Mattson E. Adults with cerebral
Medical and functional status of adults 225–32. palsy: walking ability after progressive
with cerebral palsy. Dev Med Child Neurol 17. Aglietti P, Insall JN, Cerulli G. Patellar strength training. Dev Med Child Neurol
1995; 37: 1075–84. pain and incongruence. I: measurements 2003; 45: 220–8.
Musculoskeletal Conditions in CP Kevin P Murphy 3525. Taylor NF, Dodd KJ, Larkin H. Adults cerebral palsy. Long-term follow-up ylolisthesis in non-ambulatory patients.
with cerebral palsy benefit from participat- results. Clin Orthop Relat Res 1993; 296: Spine 1981; 6: 35–8.
ing in a strength training programme and 148–53. 51. Wang JP, Zhong ZC, Cheng CK et al
a community gymnasium. Disabil Rehabil 38. McCarthy RE, Simon S, Douglas B, Finite element analysis of the spondyloly-
2004; 26: 1128–34. Zawacki R, Reese N. Proximal femoral sis in lumbar spine. Biomed Mater Eng
26. Allen J, Dodd KJ, Taylor NF, McBurney resection to allow adults who have severe 2006; 16: 301–8.
H, Larkin H. Strength training can be cerebral palsy to sit. J Bone Joint Surg Am 52. Gallien P, Nicholas B, Petrilli S et al
enjoyable and beneficial for adults with 1988; 70: 1011–6. Role for botulinum toxin in back pain
cerebral palsy. Disabil Rehabil 2004; 26: 39. Widmann RF, Do TT, Doyle SM, Burke treatment in adults with cerebral palsy:
1121–7. SW, Root L. Resection arthroplasy of the report of a case. Joint Bone Spine 2004; 71:
27. Laplaza FJ, Root L, Tassanawipas A, hip for patients with cerebral palsy: an out- 76–8.
Glasser DB. Femoral torsion and neck come study. J Pediatr Orthop 1999; 19: 53. Harada T, Ebara S, Anwar MM et al The
shaft angles in cerebral palsy. J Pediatr 805–10. cervical spine in athetoid cerebral palsy. A
Orthop 1993; 13: 192–9. 40. Fredrickson BE, Baker D, McHolick WJ, radiological study of 180 patients. J Bone
28. Cooperman DR, Bartucci E, Dietrick E, Yuan HA, Lubicky JP. The natural history Joint Surg Br 1996; 78: 613–9.
Millar EA. Hip dislocations in spastic of spondylolysis and spondylolisthesis. 54. Ando N, Ueda S. Functional deterioration
cerebral palsy: long-term consequences. J J Bone Joint Sur Am 1984; 66: 699– in adults with cerebral palsy. Clin Rehabil.
Pediatr Orthop 1987; 7: 268–76. 707. 2000; 14: 300–6.
29. Moreau M, Drummond DS, Rogala E, 41. Borkow SE, Kleiger B. Spondylolisthesis 55. Reese ME, Msall ME, Owen S, Pictor SP,
Ashworth A, Porter T. Natural history in the newborn. A case report. Clin Orthop Paroski MW. Acquired cervical spine
of the dislocated hip in spastic cerebral Relat Res 1971; 81: 73–6. impairment in young adults with cerebral
palsy. Dev Med Child Neurol 1979; 21: 42. Newman PH, Stone KH. The etiology of palsy. Dev Med Child Neurol 1991; 33:
749–53. spondylolisthesis. J Bone Joint Sur Br 153–8.
30. Pritchett JW. Treated and untreated 1963; 45: 39. 56. Anderson WW, Wise BL, Itabashi HH,
unstable hips in severe cerebral palsy. Dev 43. Taillard WF. Etiology of spondylolis- Jones M. Cervical spondylosis in
Med Child Neurol 1990; 32: 3–6. thesis. Clin Orthop Relat Res 1976; 117: patients with athetosis. Neurology 1962;
31. Hodgkinson I, Jindrich ML, Duchaut P, 30–9. 12: 410–2.
Vadot JP, Metton G, Berard C. Hip pain 44. Beguiristain JL, Diaz-de-Rada P. Spondyl- 57. Levine RA, Rosenbaum AE, Waltz JM,
in 234 non-ambulatory adolescents and olisthesis in pre-school children. J Pediatr Scheinberg LC. Cervical spondylosis
young adults with cerebral palsy: a cross- Orthop B 2004; 13: 225–30. and dyskinesias. Neurology 1970; 20:
sectional multicentre study. Dev Med Child 45. Sakai T, Yamada H, Nakamura T et al 1194–9.
Neurol 2001; 43: 806–8. Lumbar spinal disorders in patients with 58. Angelini L, Broggi G, Nardocci N, Savo-
32. Molnar GE, Alexander MA. Pediatric athetoid cerebral palsy: a clinical and bio- iardo M. Subacute cervical myelopathy in
rehabilitation, 3rd edn. Philadelphia: Han- mechanical study. Spine 2006; 31: E66– a child with cerebral palsy. Secondary to
ley & Belfus, 1998. 70. torsion dystonia?. Childs Brain 1982; 9:
33. Koffman M. Proximal femoral resection or 46. Harada T, Ebara S, Anwar MM et al 354–7.
total hip replacement in severely disabled Lumbar spine in spastic diplegia. A radio- 59. Fuji T, Yonenobu K, Fujiwara K et al Cer-
cerebral-spastic patients. Orthop Clin N graphic study. J Bone Joint Surg Br 1993; vical radiculopathy or myelopathy second-
Am 1981; 12: 91–100. 75: 534–7. ary to athetoid cerebral palsy. J Bone Joint
34. Root L, Spero CR. Hip adductor transfer 47. Peter JC, Hoffman EB, Arens LJ, Peacock Sur Am 1987; 69: 815–21.
compared with adductor tenotomy in cere- WJ. Incidence of spinal deformity in chil- 60. Nokura K, Hashizume Y, Inagaki T, Ojika
bral palsy. J Bone Joint Sur Am 1981; 63: dren after multiple level laminectomy for K, Yamomoto M. Clinical and pathologi-
767–72. selective posterior rhizotomy. Childs Nerv cal study of myelopathy accompanied with
35. Root L, Gross JR, Mendes J. The Syst 1990; 6: 30–2. cervical spinal canal stenosis—with special
treatment of the painful hip in cerebral 48. Li Z, Zhu J, Liu X. Deformity of lumbar reference to complication of mental retar-
palsy by total hip replacement or hip spine after selective dorsal rhizotomy for dation or cerebral palsy. Rinsho Shin-
arthrodesis. J Bone Joint Sur Am 1986; 68: spastic cerebral palsy. Microsurgery 2008; keigaku 1993; 33: 121–9.
590–8. 28: 10–2. 61. Hirose G, Kadoya S. Cervical spondy-
36. Blake SM, Kitson J, Howell JR, Gie GA, 49. Peter JC, Hoffman EB, Arens LJ. Spond- litic radiculo-myelopathy in patients with
Cox PJ. Constrained total hip arthroplasty ylolysis and spondylolisthesis after five athetoid-dystonic cerebral palsy: clinical
in a pediatric patient with cerebral palsy level lumbosacral laminectomy for selec- evaluation and surgical treatment. J Neurol
and painful dislocation of the hip. A case tive posterior rhizotomy in cerebral palsy. Neurosurg Psychiatry 1984; 47: 775–
report. J Bone Joint Surg Br 2006; 88: Childs Nerv Syst 1993; 9: 285–7; discus- 80.
655–7. sion 287-8. 62. Pollak L, Schiffer J, Klein C, Mirovshy Y,
37. Buly RL, Huo M, Root L, Binzer T, 50. Rosenberg NJ, Bargar WL, Friedman B. Copeliovich L, Rabey JM. Neurosurgical
Wilson PD Jr. Total hip arthroplasty in The incidence of spondylolysis and spond- intervention for cervical disk disease in
36 Developmental Medicine & Child Neurology 2009, 51 (Suppl. 4): 30–37dystonic cerebral palsy. Mov Disord 1998; ment of cervical spondylitic myelopathy analysis. J Neurosurg 1996; 85: 206–
13: 713–7. complicating athetoid cerebral palsy. 10.
63. Ebara S, Harada T, Yamazaki Y et al J Bone Joint Sur Br 1984; 66: 504–8. 66. Connolly PJ, Esses SI, Kostuik JP. Ante-
Unstable cervical spine in athetoid cere- 65. Bishop RC, Moore KA, Hadley MN. rior cervical fusion: outcome analysis of
bral palsy. Spine 1989; 14: 1154–9. Anterior cervical interbody fusion using patients fused with and without anterior
64. Nishihara N, Tanabe G, Nakahara S, autogenic and allogeneic bone graft cervical plates. J Spinal Disord 1996; 9:
Imari T, Murakawa H. Surgical treat- substrate: a prospective comparative 202–6.
Musculoskeletal Conditions in CP Kevin P Murphy 37You can also read