Challenges in the Contemporary Management of Small Kidney Masses - NYU Langone Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Department of Urology
Case of the Month
Challenges in the Contemporary
Management of Small Kidney Masses
CASE 1 PRESENTATION
Healthy 39-year-old man with a 2.2 cm enhancing solid renal mass noted on CT scan
performed for abdominal pain.
Figure 1. CT scan showing an enhancing solid right renal mass.
Management: Robotic partial nephrectomy.
Pathology: Kidney tumor 1, right; partial nephrectomy: oncocytoma (2.1 cm).
Note: The tumor showed diffuse reactivity for CD117 and scattered positivity for CK7,
supporting the histologic diagnosis of oncocytoma.
CASE 2 PRESENTATION
Healthy 54-year-old man with an incidental 2.5 cm complex cyst noted on chest CT scan
prompting a renal MRI, which confirmed a 2.6 cm cystic left upper pole renal lesion containing
a thick peripheral rim and enhancing internal septations, suspicious for cystic renal cell carcinoma
(Bosniak category III).
Figure 2. MRI showing a left upper pole renal cyst.
Management: Robotic partial nephrectomy.
Pathology: Benign multilocular renal cyst.
Note: Multiple deeper levels were examined. No evidence of malignancy was identified.
DC 04/02/2021
CASE OF THE MONTH
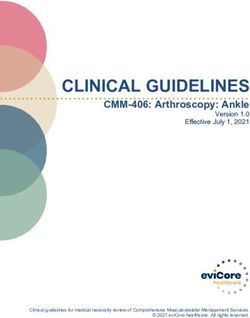
CASE 3 PRESENTATION
59-year-old man with a history coronary artery disease, severe aortic regurgitation, a
cerebrovascular accident, and a thoracic aortic aneurysm repair, referred by his primary
urologist for treatment of a biopsy-proven enlarging solid 2.2 cm papillary renal cell carcinoma.
Figure 3. CT scan demonstrating biopsy-proven right renal cell carcinoma
Management: Active surveillance; 5 months after he was placed on surveillance by GU,
patient died following complications from a valve replacement.
COMMENT
With widespread liberal use of diagnostic imaging, incidental small renal masses (SRMs) account
for nearly 70% of all new diagnosed kidney tumors. The management of SRMs has dramatically
evolved over the past decade and a half. Radical nephrectomy is no longer universally employed
as the treatment of choice for SRMs and patients are now treated with a variety of kidney-sparing
options, including partial nephrectomy and ablation. The management of SRMs has also evolved
to include active surveillance or observation because of an improved understanding of the
heterogeneity of SRMs and the indolent natural history associated with even malignant SRMs.1
Over this period, advances in imaging have led not only to earlier detection of SRMs but also to an
improved ability to identify benign renal masses, such as lipid-poor angiomyolipomas (AMLs) and
benign complex renal cysts. Despite these diagnostic and therapeutic advances, these 3 unique
SRMs cases demonstrate ongoing challenges in the management of SRMs.
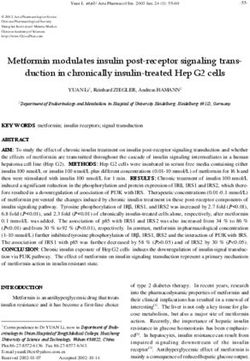
It has been reported historically that up to 20% of small renal masses are benign.2 With adoption
of renal mass biopsy, increased use of observation/surveillance, and improved imaging, it would
be reasonable to assume that the number of benign renal masses undergoing surgical resection
would decline over time. Interestingly, in a recent review of NYU Langone Urology’s prospectively
maintained database of more than 1,800 patients undergoing partial or radical nephrectomy, the
incidence of benign masses remains roughly 20% and includes lipid-poor AMLs, oncocytomas,
and other benign solid renal masses (Figure 4).3
DC 04/02/2021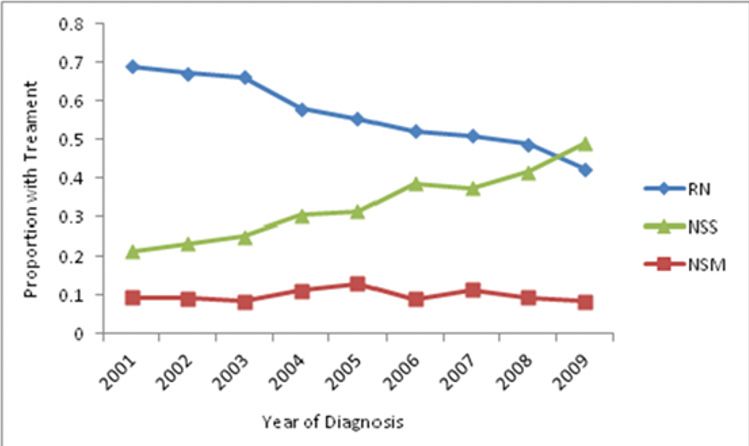
CASE OF THE MONTH
Figure 4. Renal masses: percentage of benign pathology over time.
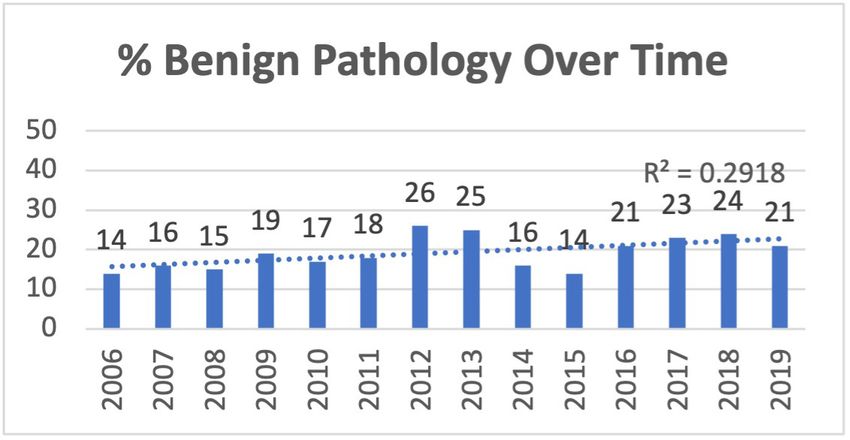
Over this same period, however, the incidence of oncocytoma appeared to increase
(from 51% to 59%) while the incidence of AMLs decreased (from 49% to 30%) (Figure 5).
Figure 5. Percentage of benign masses, by type of mass, over time (3-year rolling average).
Oncocytomas continue to present as a diagnostic challenge in patients with SRMs. On both
imaging and percutaneous biopsy, these tumors have overlapping features with malignant renal
masses, making it difficult to preoperatively differentiate them from malignant tumors. On
contrast-enhanced CT or MRI, oncocytomas share imaging characteristics with clear cell renal
carcinomas.4 In order to overcome the limitations of CT and MRI in identifying oncocytomas, there
has been a growing interest in both percutaneous renal mass biopsy and nuclear medicine imaging
studies such as 99mTc-sestamibi SPECT/CT, which have been shown to differentiate oncocytomas
from malignant renal masses with high sensitivity and specificity.5 Although both sestamibi
SPECT/CT and renal mass biopsy can differentiate oncocytomas from clear cell and papillary renal
cell carcinomas, there are challenges in differentiating oncocytomas from malignant oncocytic
tumors such as chromophobe renal cell carcinomas and hybrid oncocytic tumors, which arguably
have malignant potential.6
DC 04/02/2021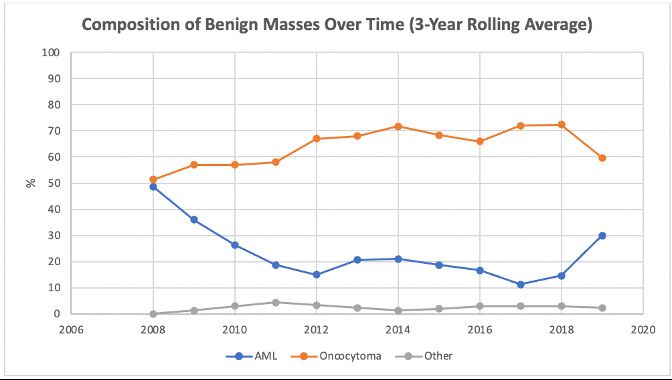
CASE OF THE MONTH In addition to ongoing diagnostic challenges, treatment selection remains a challenge for many patients with SRMs, particularly older patients or patients with significant comorbid conditions, who are unlikely to benefit from any treatment. Given the low likelihood of disease progression in malignant SRMs, multiple guidelines offer treatment recommendations based on life expectancy and the risk of treatment-related complications and adverse effects such as chronic kidney disease. Although this tailored treatment approach is used in other indolent genitourinary malignancies such as low-risk prostate cancer, there is a paucity of high-level data supporting an optimal treatment approach with SRMs, resulting in a large degree of uncertainty about the most effective, risk-based criteria for treatment. Currently, the majority of patients with a SRM undergo active treatment. Despite exceedingly low rates of disease progression (
CASE OF THE MONTH
REFERENCES
1. Huang WC, Atoria CL, Bjurlin M, et al. Management of small kidney cancers in the new millennium: contemporary trends and outcomes
in a population-based cohort. JAMA Surg. 2015;150(7):664-672.
2. Frank I, Blute ML, Cheville JC, Lohse CM, Weaver AL, Zincke H. Solid renal tumors: an analysis of pathological features related
to tumor size. J Urol. 2003;170(6 Pt 1):2217-2220.
3. Vijay V, Jericevic D, Huang WC. Incidence of benign renal masses in a contemporary cohort of patients receiving partial
nephrectomy for presumed renal cell carcinoma. Poster #93 presented at: 21st Annual Meeting of the Society of Urologic Oncology;
December 1-5, 2020.
4. Kang SK, Huang WC, Pandharipande PV, Chandarana H. Solid renal masses: what the numbers tell us. AJR Am J Roentgenol.
2014;202(6):1196-1206.
5. Wilson MP, Katlariwala P, Murad MH, Abele J, McInnes MDF, Low G. Diagnostic accuracy of 99mTc-sestamibi SPECT/CT for detecting
renal oncocytomas and other benign renal lesions: a systematic review and meta-analysis. Abdom Radiol (NY). 2020;45(8):2532-2541.
6. Patel HD, Druskin SC, Rowe SP, Pierorazio PM, Gorin MA, Allaf ME. Surgical histopathology for suspected oncocytoma on renal
mass biopsy: a systematic review and meta-analysis. BJU Int. 2017;119(5):661-666.
7. Kang SK, Huang WC, Elkin EB, Pandharipande PV, Braithwaite RS. Personalized treatment for small renal tumors: Decision analysis
of competing causes of mortality. Radiology. 2019 Mar;290(3):732-743
8. Kang SK, Bjurlin MA, Huang WC. Management of small kidney tumors in 2019. JAMA. 2019 Apr 23;321(16):1622-1623.
WILLIAM HUANG, MD
William Huang, MD, is a fellowship-trained urologic oncologist at
NYU Langone Health and the Perlmutter Cancer Institute. He is
associate professor of urology and vice chair for Clinical Affairs in
the Department of Urology at NYU Grossman School of Medicine.
Dr. Huang is also chief of the Urology Service at Tisch Hospital and
co-director of the Robotic Surgery Center at NYU Langone Health.
Dr. Huang has extensive experience in open, robotic, and
laparoscopic surgical techniques and has performed more than
1,200 robotic surgeries. His surgical expertise includes the
treatment of complex kidney, retroperitoneal, and testicular tumors,
along with minimally invasive radical cystectomy, partial and radical
nephrectomy (including inferior vena cana thrombi), retroperitoneal
lymphadenectomy, and prostatectomy. Dr. Huang has published
more than 125 articles in high-impact journals, including the Journal
of Clinical Oncology, Lancet Oncology, the Journal of the American
Medical Association, and the New England Journal of Medicine. He
has lectured at both national and international meetings, particularly
on improving outcomes following kidney cancer surgery. Dr. Huang
continues to advance the field of urologic oncology through his
research into novel approaches to the diagnosis and management
of kidney, testicular, and non-muscle invasive bladder cancers.
DC 04/02/2021Department of Urology
Our renowned urologic specialists have pioneered numerous advances in the surgical and pharmacological
treatment of urologic disease.
For questions and/or patient referrals, please contact us by phone or by e-mail.
Faculty Specialty Phone Number/Email
Kidney stones, Kidney Cancer, Ureteral Stricture, UPJ obstruction, Endourology, Robotic Renal Surgery, 646-825-6387
James Borin, MD
Partial Nephrectomy, Ablation of Renal Tumors, PCNL james.borin@nyulangone.org
Female Pelvic Medicine and Reconstructive Surgery, Pelvic Organ Prolapse-Vaginal and Robotic 646-754-2404
Benjamin Brucker, MD
Surgery, Voiding Dysfunction, Male and Female Incontinence, Benign Prostate Surgery, Neurourology benjamin.brucker@nyulangone.org
Female Sexual Dysfunction, Male Sexual Dysfunction, General Urology, Benign Disease Prostate, 646-825-6318
Seth Cohen, MD
Post-Prostatectomy Incontinence, Erectile Dysfunction, Hypogonadism seth.cohen@nyulangone.org
Robotic and Minimally Invasive Urology, BPH and Prostatic Diseases, Male and Female Voiding 718-630-8600
Frederick Gulmi, MD*
Dysfunction, Kidney Stone Disease, Lasers in Urologic Surgery, and Male Sexual Dysfunction frederick.gulmi@nyulangone.org
Urologic Oncology, Open, Laparoscopic, or Robot-Assisted Approaches to Surgery, Surgical
646-825-6325
Mohit Gupta, MD† Management of Genitourinary Malignancies including Kidney, Bladder, Prostate, Adrenal, Penile,
Mohit.Gupta2@nyulangone.org
and Testis Cancers
Urologic Oncology (Open and Robotic) – for Kidney Cancer (Partial and Complex Radical), Urothelial 646-744-1503
William Huang, MD
Cancers (Bladder and Upper Tract), Prostate and Testicular Cancer william.huang@nyulangone.org
Pediatric Urology including Hydronephrosis, Hypospadias, Varicoceles, Undescended Testicles,
212-263-6420
Grace Hyun, MD Hernias, Vesicoureteral Reflux, Urinary Obstruction, Kidney Stones, Minimally Invasive Procedures,
grace.hyun@nyulangone.org
Congenital Anomalies
646-825-6322
Christopher Kelly, MD Male and Female Voiding Dysfunction, Neurourology, Incontinence, Pelvic Pain, Benign Prostate Disease
chris.kelly@nyulangone.org
Prostate Cancer: Elevated PSA, 3D MRI/Ultrasound Co-registration Prostate Biopsy, Focal (Ablation) 646-825-6327
Herbert Lepor, MD
of Prostate Cancer, Open Radical Retropubic Prostatectomy herbert.lepor@nyulangone.org
718-261-9100
Stacy Loeb, MD, MSc** Urologic Oncology, Prostate Cancer, Benign Prostatic Disease, Men’s Health, General Urology
stacy.loeb@nyulangone.org
Benign Prostatic Hyperplasia, Erectile Dysfunction, Urinary Tract Infection, Elevated Prostate-specific 718-376-1004
Danil Makarov, MD, MHS***
Antigen, Testicular Cancer, Bladder Cancer, Prostate Cancer danil.makarov@nyulangone.org
Urethral Strictures, Robotic and Open Reconstructive Surgery for Ureteral Obstruction/Stricture, Fistulas, 646-754-2419
Nnenaya Mmonu, MD, MS
Bladder Neck Obstruction, Penile Prosthesis, Post Prostatectomy and Radiation Urinary Incontinence nnenaya.mmonu@nyulangone.org
Male Infertility, Vasectomy Reversal, Varicocele, Post-Prostatectomy, Erectile Dysfunction, 646-825-6348
Bobby Najari, MD
Male Sexual Health, Hypogonadism, Oncofertility bobby.najari@nyulangone.org
Female Pelvic Medicine and Reconstructive Surgery, Voiding Dysfunction, Neurourology, Incontinence, 646-825-6311
Nirit Rosenblum, MD
Female Sexual Dysfunction, Pelvic Organ Prolapse and Robotic Surgery nirit.rosenblum@nyulangone.org
Pediatric Urology including: Urinary Tract Obstruction (ureteropelvic junction obstruction),
646-825-6326
Ellen Shapiro, MD Vesicoureteral Reflux, Hypospadias, Undescended Testis, Hernia, Varicocele, and Complex
ellen.shapiro@nyulangone.org
Genitourinary Reconstruction.
Kidney stones, PCNL, Kidney Cancer, UPJ obstruction, Endourology, Robotic Renal Surgery, 718-630-8600
Mark Silva, MD*
Ablation of Renal Tumors mark.silva@nyulangone.org
Muscle-Invasive Bladder Cancer, Non-Invasive Bladder Cancer, Radical Cystectomy, 646-825-6327
Gary D. Steinberg, MD
Urinary Tract Reconstruction After Bladder Removal Surgery gary.steinberg@nyulangone.org
Female Pelvic Medicine and Reconstructive Surgery, Pelvic Organ Prolapse, Incontinence in Women, 646-825-6324
Lauren Stewart, MD
Female Voiding Dysfunction lauren.stewart@nyulangone.org
Urologic Oncology – Prostate Cancer (MRI-Guided Biopsy, Robotic Prostatectomy, Focal Therapy, 646-825-6321
Samir Taneja, MD
Surveillance), Kidney Cancer (Robotic Partial Nephrectomy, Complex Open Surgery), Urothelial Cancers samir.taneja@nyulangone.org
Urologic Oncology – Prostate Cancer, MRI-Guided Biopsy, Kidney and Prostate Cancer Surgery,
646-754-2470
James Wysock, MD, MS Robotic Urological Cancer Surgery, Prostate Cancer Image-guided Focal Therapy (Ablation, HIFU),
james.wysock@nyulangone.org
and Testicular Cancer
Robotic and Open Reconstructive Surgery for Ureteral Obstruction, Fistulas, Urinary Diversions, 646-754-2419
Lee Zhao, MD
Urethral Strictures, Peyronie’s Disease, Penile Prosthesis, and Transgender Surgery lee.zhao@nyulangone.org
Kidney Stone Disease, Upper Tract Urothelial Carcinoma, Ureteral Stricture Disease, and BPH/Benign 646-754-2434
Philip Zhao, MD
Prostate Disease philip.zhao@nyulangone.org
*at NYU Langone Hospital – Brooklyn ** NYU Langone Ambulatory Care Rego Park NYU Langone Levit Medical †222 East 41st street; NYU Langone Ambulatory Care Bay Ridge, and NYU Langone Levit Medical
***
nyulangone.org DCYork,
222 East 41st Street New 04/02/2021
NY 10017
U1020You can also read