CHILDHOOD DIABETES WHAT IS THE WAY FORWARD? - July 21, 2013 Keystone, Colorado Robert H. Slover MD
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CHILDHOOD DIABETES
WHAT IS THE WAY FORWARD?
July 21, 2013
Keystone, Colorado
Robert H. Slover MD
Challenges
1. Type 1 diabetes is increasing in the population
2. Type 2 diabetes is increasing also, and notably amongst
teens
3. Diabetes care is education intense, requires an array of
specialists, and is expensive
4. Diabetes care, however, is inadequately funded, with
large blocks of necessary care completely unfunded
5. Emerging technology offers opportunities for improved
outcomes, but adds to the expense and complexity of
care
6. There is a paucity of trained clinical diabetes specialists
7. Diabetes has a large and growing economic impact on
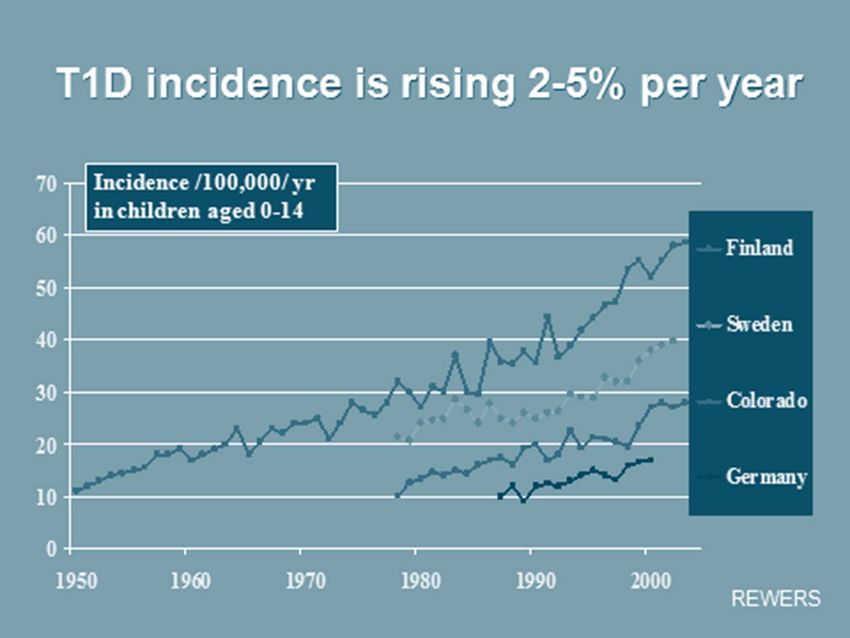
societyType 1 Diabetes is increasing in incidence worldwide, and the age of onset may be moving toward younger aged children
“…Type 1 diabetes is an autoimmune disease the accounts for approximately 5% of US diabetes cases. Ominously, the greatest increase (in onset of Type 1 diabetes) occurred in the youngest children, with new cases projected to double in European children younger than five years and increase by 70% in those younger than 15 between 2005 and 2020.” Judith Fradkin, MD Director of the Division of Diabetes, Endocrinology, and Metabolic Diseases, NIDDK Confronting the Urgent Challenge of Diabetes: An Overview Health Affairs 31 (2012):12‐19
Type 2 Diabetes in increasing in the population,
and notably is increasing in adolescents.
– >8% of the US population is currently affected
with T2D
– It is estimated that >20% will be affected by 2050.
– T2D has a disproportionate impact on the poor
and minorities
– This represents a significant public health crisisEconomic Impact of Diabetes in 2012
in the USA
Total Cost $245 billion
Direct Cost $176 billion
Reduced Productivity $69 billion
Direct Costs:
Inpatient care 43%
Drugs to treat complications 18%
Antidiabetic drugs/supplies 12%
Office Visits 9%
Residential Care 8%The Cost of Diabetes
• 2007‐Total estimated costs $174 billion
– $116 billion in medical expenditure
– $58 billion in lost productivity
– 59% of medical expenditures was inpatient
hospitalization and physician visits
– $1 in $5 spent on Diabetes in the United States is
spent on taking care of someone with diabetes
– About 157,000 (0.2% of US populationThe Cost of Diabetes
• 2012 –Total estimated costs $254 billion (41%
increase)
– $176 billion in medical expenditure
– $69 billion in lost productivity
– 52% of medical expenditure was inpatient
hospitalization and physician visits
– $1 in $5 spent on diabetes in United States is
spent on taking care of someone with diabetes
– 189,000 children ages 0‐20 with diabetes, 168,000
with type 1 diabetes“People with diagnosed diabetes, on average, have medical expenditures approximately 2.3 times higher than what expenditures would be in the absence of diabetes.” American Diabetes Association Statement Diabetes Care 36 (April 2013): 36: 1033‐46
How much does Type 1 Diabetes
cost?
Three phases:
1. First – Onset; Higher costs
2. Second – Early years without complications; Lower costs
3. Third – Later years with complications; Much higher costs
In the pediatric population we bear the costs of onset
and education, as well as the costs of therapy and
prevention or treatment of early complications, but
only rarely the high costs of complications.Direct Costs in T1D Texas study of 784 patients
‐ 7% of costs are from diabetes related
complications (excludes new onset admissions
and education)
‐ Direct cost per person year $4730
Supplies 38%
Medication 33%Texas Study (continued)
‐ Factors associated with higher costs in T1D
Older age
HbA1C >8.5%
Technology (pumps, sensors)
Female
Living in a single‐parent household
‐ Factors associated with hospitalization in T1D
HbA1C >8.5%
Female
Conclusion: Improved metabolic control and stable two‐parent
households lower direct medical costs in T1D.
Ying AK et al.,Predictors of direct costs of diabetes care in pediatric patients with type 1 diabetes.
Pediatric Diabetes 2011, 12: 177‐182Cost of Type 1 Diabetes in the USA • Use of a propensity score matching system to estimate annual and lifetime direct and indirect costs for T1D • T1D costs $14.4 billion annually in direct and indirect costs • T1D patients incur a disproportionate share of T1D + T2D costs • If T1D were eliminated, lifetime cost savings would be $422.9 billion for existing patients and another $10.6 billion for new cohort each year. Tao B, Petropaolo M, Atkinson M, Schatz D, Taylor D. Estimating the Cost of type 1 Diabetes in the US: A Propensity Score Matching Method. PloS One (July 2010): Vol 5 Issue 7, e11501
Table 11. Summary of estimated costs attributable to T1D (2005 dollars).a Tao B, Pietropaolo M, Atkinson M, Schatz D, et al. (2010) Estimating the Cost of Type 1 Diabetes in the U.S.: A Propensity Score Matching Method. PLoS ONE 5(7): e11501. doi:10.1371/journal.pone.0011501 http://www.plosone.org/article/info:doi/10.1371/journal.pone.0011501
Glycemic Control: effect on short‐
terms costs
• A 1% increase in HbA1C leads to:
6% increase in cost for Type 1 Diabetes
4.4% increase in cost for Type 2 Diabetes
Aargen M and Wenli L. Association between glycemic control and short‐term
healthcare costs among commercially insured diabetes patients in the United Statds.
Journal of Medical Economics 2011: Vol 14 No 1, 109‐114So where are we? • Diabetes in childhood and adolescence is increasing. • Both Type 1 and Type 2 Diabetes have a have a large and growing impact on our economy and health care system. Even now, up to 1 in every 5 health care dollars in the USA is spent on diabetes care. • Improved metabolic control can reduce short term and long term costs, but – • Who will deliver the care? • Who will pay for time‐consuming education, social and psychological support, and technology that at present holds the promise of allowing tight metabolic control?
Is diabetes education cost effective? 2009 meta‐analysis reviewed 23 studies of this question from a literature review of 609 articles – 18 showed cost effectiveness – 4 were cost neutral – 1 showed cost ineffectiveness None was specifically based on the AADE’s 7 self‐care education requirements: healthy eating, being active, monitoring, taking medication, problem solving, healthy coping, and reducing risks. Only one study specifically addressed adolescents, and none addressed younger children. Boren S, et al. Costs and Benefits Associated with Diabetes Education: A Review of the Literature. 2009: The Diabetes Educator 35: 72‐96.
Should new onset education be done
in the hospital?
‐ One year randomized trial of 84 non‐urgent new onset patients at
Baystate Children’s Hospital
‐ No significant difference in metabolic outcomes at one year
‐ Cost for first year of patients educated in hospital $12,332
‐ Cost for first year of patients educated as outpatients
$5,053
‐ Physician costs were not significantly different
Conclusion: In non critically‐ill children there is no
metabolic advantage to be gained by more expensive
inpatient education.
Jasinski CF et al. Heathcare cost of type 1 diabetes mellitus in new‐onset children in a hospital compared
to an outpatient setting. 2013: BMC Pediatrics 13:55‐65.BUT… Will insurers reimburse outpatient education as well as they reimburse hospitalization with education? Will hospitals be as willing to support outpatient education programs, given the loss of inpatient revenue?
Who Pays? 1. National Health Care programs 2. Government funded programs (Federal and state) 3. Private insurance with member premiums and co‐pays 4. Public institutions – federal and state related hospitals and clinics, medical schools and universities 5. Private foundations 6. Philanthropy 7. Individual families
Patients seen in Pediatrics at the Barbara Davis Center
June 2011 – June 2013
T1D 3285 New Onset Patients
T2D 73
MODY 15 2011 375
Neonatal 3
CFRD 50 2012 391
Secondary 33
Other (incl R/O) 158 2013 (projected) 415At the Pediatric Clinic at the Barbara Davis Center for Diabetes 65% of the cost of providing clinical care comes from clinical income. The remaining 35% is funded by physician research funds (the majority of our faculty support much of their own salary through research grants), philanthropy (Children’s Diabetes Foundation, CU Foundation, Children’s Hospital Foundation, and private donations), and Children’s Hospital support.
Telehealth Short‐term studies from Denmark and the Barbara Davis Center after initiation of telehealth agree in showing: – No deterioration in A1C, and in individual cases, improvement – Extremely high patient satisfaction – Significant reduction in lost work and school time and reduction in travel costs (addressing the indirect costs of diabetes) – Reimbursement is not significantly different from in‐ person clinic visits
RECOMMENDATIONS
1. Improve metabolic control to improve outcome and
reduce stage 3 costs.
2. Provide outpatient new onset education for non‐critically
ill patients.
3. Lobby for improved funding for diabetes education,
psycho‐social support, use of advanced technology,
including reimbursement for the large amount of time
spent in providing support by telephone and email.
4. Reduce stage 1 costs by vigorous professional and
community educational programs to reduce DKA by early
recognition of the signs and symptoms of diabetes.RECOMMENDATIONS 5. Tie the judicious use of technology to patient compliance. 6. Telehealth and other outreach means of increasing the impact of trained diabetes providers in larger geographic areas 7. Create new ways to see patients to increase effectiveness of education and care (Example – shared appointment visits) 8. Focus the skills of diabetologists and other trained diabetes professionals on creating educational programs to teach the physicians, nurses, and dieticians that actually see most of the children with diabetes: workshops, seminars, educational conferences
Thank you Questions?
You can also read

















































