Chronic pancreatitis Ali Khalil, MD Lebanese Univ, Lebanese American Univ Head of Endoscopy Department, RHUH Chief of Gastroenterolgy Division, Zahraa
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Chronic pancreatitis
Ali Khalil, MD
Lebanese Univ, Lebanese American Univ
Head of Endoscopy Department, RHUH
Chief of Gastroenterolgy Division, Zahraa
University Hospital
Chronic pancreatitis • Irreversible parenchymal destruction leading to pancreatic dysfunction • Persistent, recurrent episodes of severe pain • Anorexia, nausea • Constipation, flatulence,Steatorrhea • Diabetes

Chronic pancreatitis
• Toxic-metabolic; chronic EtOH abuse (90%), Smoking
• Idiopathic
• Genetic
• Autoimmune
• Recurrent and severe A P
• Congenital malformation
MRCP of pancreas divisum
Evaluation
• or normal amylase and lipase
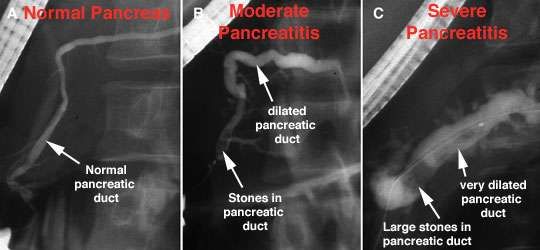
• Plain AXR / CT may show
calcified pancreas
• Pain management critiria
EtOH cessation may improve
pain
Narcotic dependency is common
Complications
• Exocrine insufficiency typically manifests as
weight loss and steatorrhea
If steatorrhea present, a trypsinogen level < 10 is
diagnostic for chronic pancreatitis
Manage with low-fat diet and pancreatic enzyme
supplements (Pancrease, Creon)
• Endocrine insufficiency may result from islet cell
destruction which leads to diabetes
Management • Manifests it self as a recurring, chronic illness requiring medication to control abdominal pain and efforts to preserve quality of life • Options to treat abdominal pain include surgical and other invasive techniques • Some patients require pancreatic enzymes to help in digestion food and insulin to correct diabetes mellitus
Food and diet
• Alcohol restriction as part of the long-term
management strategy to control pancreatitis pain
• A low-fat diet to limit pancreatic enzyme secretion
• Avoid smoking; studies shown that smoking is an
independent risk factor for the development of
both acute and chronic pancreatitis
Arch Intern Med. 2009;169:1035-1045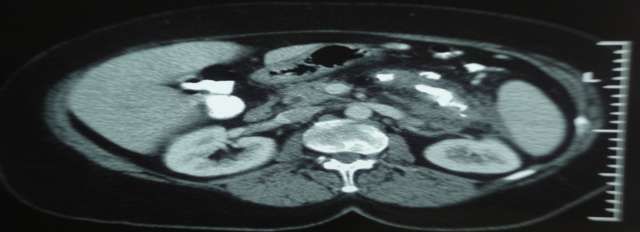
Enzyme Therapy and Vitamin
Supplementation
• Patients with steatorrhea to achieve optimal
enzyme activity in the duodenum
• Enteric-coated preparations
• The use of pancreatic enzyme therapy to treat
pancreatitis associated pain is less certain
• Supplementation with fat-soluble vitamins
Aliment Pharmacol Ther. 2009;29:235-246
Pain management In the absence of prospective studies, In the absence of randomized studies, Analysis of the literature is difficult :

Pain management • Role of abstinence from alcohol, smocking Role of medical therapy: enzymes ? • Variable presentation of pain (chronic, attacks) • Role of the complications (pseudocyst, bile duct) ? • Fragile psychology of the patient • Different endoscopic treatments
Gall stone pancreatitis by ERCP
Endoscopic management PRINCIPLE 1: TO ELIMINATE A PANCREATIC CARCINOMA, Even in patient with an history of chronic pancreatitis, as no surgical exploration • US, CT, EUS, MRI…IDUS • Endoluminal cytology and biopsy : EUS-FNA, ERCP • Strict and frequent follow-up
Endoscopic management PRINCIPLE 2: TO TREAT ONLY IN CASE OF SYMPTOMS AND COMPLICATIONS • Pain: yes • Pseudocyst: yes if symptoms or complications • Fistula: yes
Endoscopic management PRINCIPLE 2: TO TREAT ONLY IN CASE OF SYMPTOMS AND COMPLICATIONS • Biliary stenosis: +/- discussed • Duodenal stenosis: no • Vascular stenosis (portal vein, splenic vein): no • Pancreatic exocrine function: +/- discussed • Diabetes: no
Endoscopic management PRINCIPLE 3: TO USE ADAPTED MATERIAL • Fluoroscopy: high quality, multiple incidences • Accessories: multiple, specific; Guide-wires, dilation balloon, Soehendra dilat • Extracorporeal lithotripsy: 31-75% of cases • EUS (pseudocyst) PRNICIPLE 4: TO TREAT ONLY COMPLIANT PTS
Endoscopic management
PAIN
Endoluminal tt
• Aim: drainage of the main pancreatic duct
(wirsung,santorini)
• Bases: results of surgical bypass
Immediate effect on pain: 70-90%
(Sarles 82, Bradley 87, Longnecker 96, Prinz 90)Endoscopic management
PAIN
• Indications 1: No stenosis
• MRCP +++ ES alone
+/- biliary sphinctero
2: Stenosis, stones 3: Stenosis, no
Extracorp litho (nber ?) stones
then ES + stent (type ?) Sphinctero + stentEndoscopic management
PAIN
Long stenosis
Indicationsto be discussed
Ex: familial CP
Discussion: length of the stenosis
Minor modif
Cremer Type I
Discussion: Tt at the early
asymptomatic stageEndoscopic management
PAIN
Contreindications
Distal stenosis
Cremer type II
Recommendation: left
pancreatectomyPain management PAIN: RESULTS SERIES WITH EXTRACOROPREL LITHOTRIPSY Summary of Published series (12 series) SUCCESS OF FRAGMENTATION: 98% MAIN PANC DUCT CLEARANCE: 54% PAIN DISAPPEARANCE: IMMEDIATE 88% Pain disappearance: LATE (>2y) 64%
Pain management SERIES WITH STENT Summary of published series (7series) Stent insertion: 90% Pain disappearance, immediate: 78% Pain disappearance, late (>2y) :63%
Endoscopic management
MORBIDITY: LOW
Immediate cns: not significative
Stent: Acute panc 6-43%, rapidly reversible
ES: 4,1% (bleeding, mild panc) Jakobs 02 175 pts
Late cns: mild
Stent obstruction:
13% for 10F (HEH 95) to 100% for 7F (Ikenberry 04)
few cases of pseudocysts or abscesses
Stent migration
Cholangitis, bile obstruction / stent: 4% Cremer 91EUS-Guided Celiac Plexus
Blockade
• Anterior approach and real-time imaging of the celiac plexus
• Its role in the control of pancreatic cancer pain is clearly
established
• Its benefit in chronic pancreatitis pain is more controversial
• Achieved through the administration of a combined injection
of a corticosteroid and local anestheticEUS-Guided Celiac Plexus
Blockade
• A review of 6 studies (n=221 patients) found that EUS-
guided CPB was effective in about half (51%) of patients
with chronic pancreatitis
• A meta-analysis and systematic review of 8 studies
(n=283 patients) concluded that EUS-guided CPB was
effective in 59% of patients with chronic pancreatitis
J Clin Gastroenterol. 2010;44:127-134
Dig Dis Sci. 2009;54:2330-2337EUS-Guided Celiac Plexus
Blockade
EUS GUIDANCE
STEROIDSPAIN
Medical tt: enz, alcohol stopped (and smoking)
Endoscopic tt
90%
Technical Success Technical failure
85%
Non efficient Efficient Surgery
Recurrence
EUS neurolysis Result maintained
65%PSEUDOCYST
ENDOLUMINAL TT VS
CYSTOENTEROSTOMY
Cystogastrostomy
Cystoduodenostomy
EUS guided
Main panc duct drainage
CystowirsungostomyPseudocyste: Role of EUS
FINAL METHOD: no scope exchange
large channel EUS scope
appropriate stent « Electrical » guide-wire
delivery system
6.5F catheter
8.5 or 10F stentA B C
Pseudocyste: Role of EUS
Vilmann 98: first case
Giovannini 98: 6 pts, no bulging into the lumen
success: 5/6
Seifert 00: 6 pts, success: 5/6
Giovannini 01: 35 pts, 15 with chronic
pancreatitis and 20 with post-op abcesses
8.5 F stent or 7 F nasocystic drain (8-10 days)
mean FU: 27 months, overall success: 88.5%Our Experience
case AGE Gender Etiology Stent ERCP and ESWL Associated procedures Morbidity Mortality Clinical
Insertion improvement
1 22 M Malformation No No Cystogastrostomy No No Yes
2 65 M Alcohol Yes, minor No Bilary stent No No Yes
papilla
3 48 F Sarcoidosis Yes Yes Bilary stent No No Yes
4 57 M Biliary ? Yes Yes Biliary Sphincterotmy No No Yes
5 28 F heredity Yes Yes Bilary stent No No Yes
6 33 M heredity Yes No No No No Yes
7 68 F IPMT No No Biliary stent No No _
8 18 F Heredity? Yes, minor No Bilary stent No No Yes
Malformation papilla
9 72 M Alcohol _ No Surgery Yes No Yes
10 45 M Autoimmune Yes No Bilary stent No No Yes
11 62 M Alcohol Failure No No _ _ NoCase n 3
Case n 6
Case n 8
Our Result • Uncommon Disease • Gender: Male predominance • Most common Etiology: Hereditary, Malformation • Technical success: 90% • Biliary drainage: 55% • Procedure Mortality and Morbidity: 0% • Clinical improvement: 90% • Combination ES & ESWL: 3/11P
THANK YOU
Pain management
PAIN: RESULTS
SERIES COMBINATION ERCP & ESWL
SUMMARY OF PUBLISHED SERIES (1 PUBLICATION)
STENT INSERTION : 58.6%
PAIN DISAPPEARANCE IMMEDIATE 60%
PANCREATIC SURGERY HAS BEEN AVOIDED 64%
South Med J. 2010 Jun;103(6):494-5You can also read