CLINICAL QUALITY FORUM - MARCH 24, 2022 - TO TEST OR NOT TO TEST: THE BENEFITS AND POTENTIAL HARMS OF FOOD ALLERGEN IGE TESTING
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Quality Forum
March 24, 2022
To Test or Not to Test:
The Benefits and Potential Harms of Food Allergen IgE Testing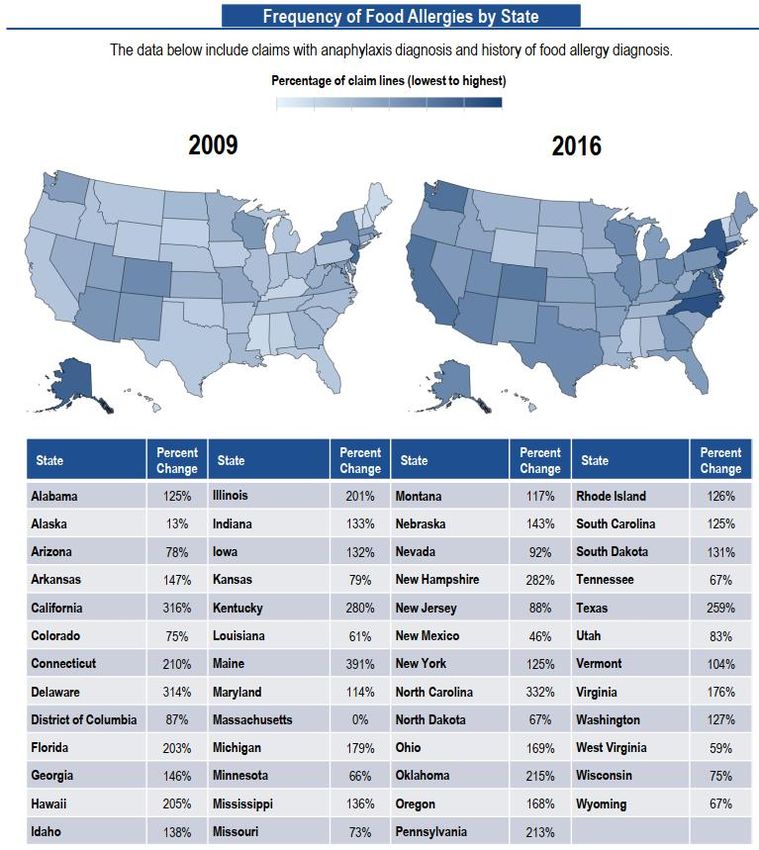
Agenda
Topic Time Presenter
Welcome, Agenda
5 min Brad Weselman, MD
• Update: State of the Union
Primary Care Advisory Council 5 min Karen Dewling, MD
Gerald Lee, MD
Food Allergy Testing 60 min
Brian Vickery, MD
Gerald Lee, MD
Model Conversations 10 min
Brad Weselman, MD
Gerald Lee, MD
Questions & Answers 10 min
Brian Vickery, MD
The Children’s Care Network
2
Primary Care Advisory Council (PCAC)
Council Members:
Nicola Chin, MD – Morehouse School of Medicine
Gerald Clark, MD – North Fulton Pediatrics
Jeff Cooper, MD – Cooper Pediatrics
Rachelle Dennis-Smith, MD – Pedia-Doc Children’s Medical
Center PC
Lori Desoutter, MD – Pediatric Associates of North Atlanta PC
Karen Dewling, MD – Johns Creek Pediatrics PC
Hughes Evans, MD – Emory School of Medicine, Hughes
Spalding Clinic
Karen Dewling, MD
Sally Goza, MD – First Georgia Physician Group Pediatrics
Pediatrician, Johns Creek Pediatrics PC
Primary Care Advisory Council Chair Sally Marcus, MD – Northside Pediatrics and Adolescent
Medicine PC
Kunal Mitra, MD – Cobb Pediatric Associates PC
Elaine Youngblood, MD – Kids First Pediatric Group
The Children’s Care Network 3
Primary Care Advisory Council (PCAC)
• Contact information for suggestions and questions
– Nicola Chin, MD (nickydst@yahoo.com)
– Jeff Cooper, MD (jeff@cooperpediatrics.com)
– Lori Desoutter, MD (drdesoutter@panapc.com)
– Karen Dewling, MD (kdewling@johnscreekpediatrics.net)
– Hughes Evans, MD (hughes.evans@emory.edu)
– Sally Marcus, MD (sm@nspeds.org)
The Children’s Care Network 4
To Test or Not to Test: The Benefits and Potential Harms of Food Allergen IgE Testing Brian P. Vickery, MD Associate Professor of Pediatrics and Division Chief of Allergy/Immunology Gerald Lee, MD Associate Professor of Pediatrics Log in to PollEverywhere: www.pollev.com/drgerrylee

Disclosures
Dr. Vickery:
• Consultant/Advisor: Aimmune Therapeutics; AllerGenis, LLC;
Food Allergy Research and Education (FARE); Reacta
Biosciences
• Grant support: NIH-NIAID; FARE
• Clinical investigator: Aimmune; DBV Technologies; Genentech;
Regeneron
Dr. Lee:
• No relevant disclosures
The Children’s Care Network 6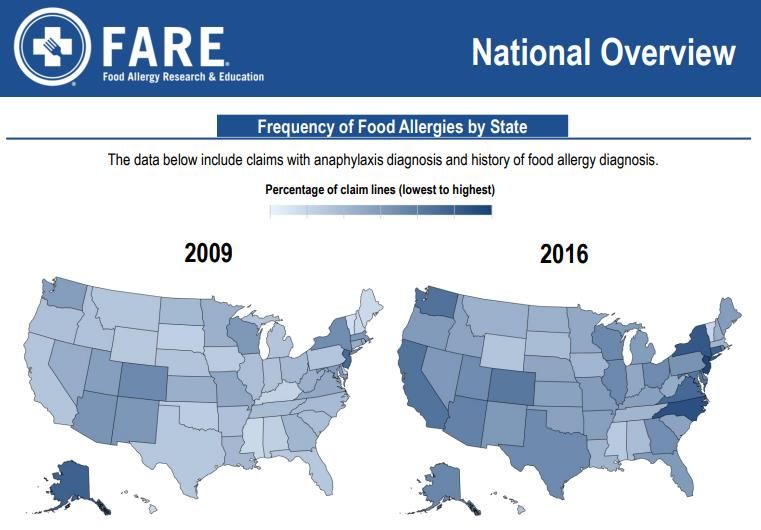
Objectives
By the end of the session, the attendee will be able to
• Determine whether a food allergy history is consistent with a
food allergen IgE mediated reaction
• Educate parents on the pathophysiology and management of
atopic dermatitis/eczema
• Educate parents on the importance of early food allergen
introduction in children with atopic dermatitis/eczema instead
of food allergen avoidance
The Children’s Care Network 7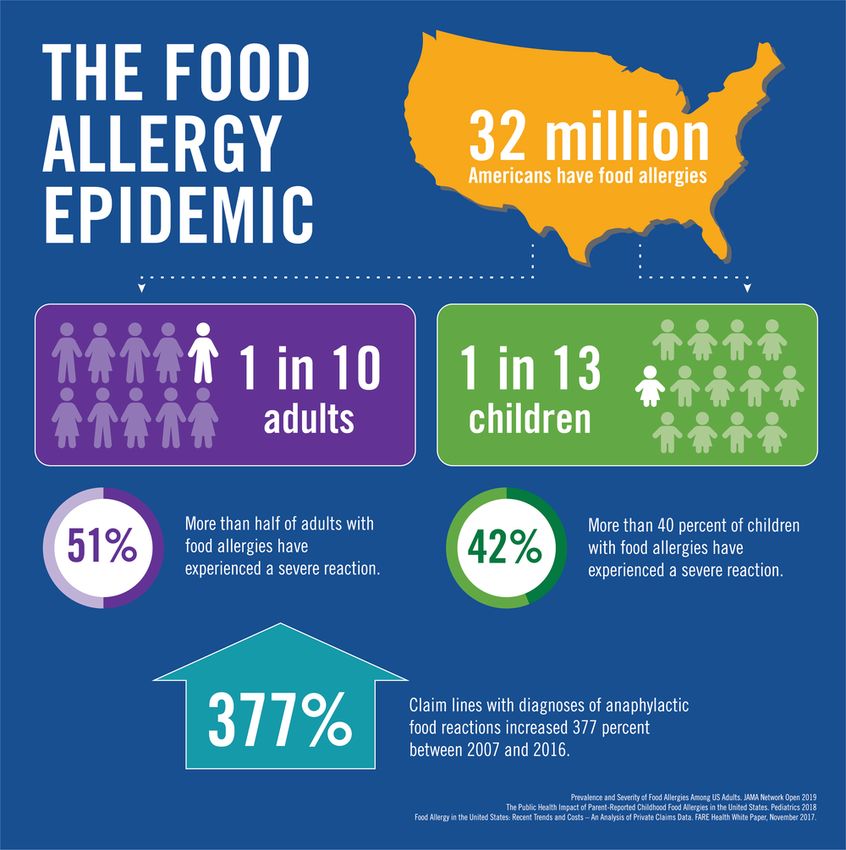
Selecting Patients for Food Allergen IgE Testing Dr. Gerry Lee

Definitions
• Food Allergy
– Adverse health effect arising from a specific immune
response that occurs reproducibly on exposure to a given
food
– IgE mediated food response: rapid onset urticaria/hives,
anaphylaxis
• Food intolerance
– A non-immunologic adverse food reaction (e.g. lactose
intolerance)
• Tolerance
– A state where an individual does not have clinical symptoms
from ingestion of a food
The Children’s Care Network 9
https://www.foodallergy.org/resources/epidemic-infographic
10146% 11
https://www.foodallergy.org/resources?_limit=12&_page=5&type=5
12Symptoms of a IgE Mediated Reaction FARE Food Allergy & Anaphylaxis Emergency Care Plan, Lieberman et al. JACI Sept 2010
Symptoms of a IgE Mediated Reaction
• Typically has onset
within minutes – 1 hour
after exposure
• Occurs reproducibly
• >85% of reactions have
urticaria/angioedema
• Usually resolves after a
day
FARE Food Allergy & Anaphylaxis Emergency Care Plan, Lieberman et al. JACI Sept 2010Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
B. Hives or swelling of unclear cause not related to meal
C. Failure to thrive/gain weight, difficulty eating
D. Colic or abdominal pain/gas
E. Hay fever, asthma
F. Parental request but no medical indication
G. Atopic dermatitis/eczema
H. Screening for food allergy in infants prior to introduction
The Children’s Care Network 15Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
• Was there hives/urticaria?
– A “hive” meets 5 criteria:
• Red
• Itchy
• Raised
• Transient (resolves in hours/less than
a day)
• Resolves without a residual mark
The Children’s Care Network 16Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
• Was there hives/urticaria?
• What the rash limited to skin contact or
generalized?
– Is the rash contact irritation vs. food
allergy?
– Common contact triggers:
• Strawberry
• Tomato/pasta sauce
• Citrus
• Ketchup/Ranch dressing
The Children’s Care Network 17Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
• Was there hives/urticaria?
• What the rash limited to skin contact or
generalized?
– Is the rash contact irritation vs. food
allergy?
• Did the meal contain a top 9 allergen?
(milk, egg, wheat, soy, peanut, tree nut,
fish, shellfish, sesame)
• Has the child tolerated that allergen in the
past year?
https://solidstarts.com/why-you-should-introduce-food-allergens-before-your-babys-first-birthday/
The Children’s Care Network 18Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
B. Hives or swelling of unclear cause not related to
meal
• Has the child woken up in the morning with hives or
swelling?
– Could this be an intrinsic process rather than
allergy?
• Is the symptom recurring every day?
– Is it more likely the child is eating same trigger
food every day vs. an intrinsic trigger?
• Has the child been recently ill?
– Could the intrinsic trigger be a viral infection?
https://www.flickr.com/photos/30478819@N08/51011333930 (CC 2.0)
The Children’s Care Network 19Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
B. Hives or swelling of unclear cause not related to meal
C. Failure to thrive/gain weight, difficulty eating
D. Colic or abdominal pain/gas
• Are the symptoms associated with urticaria?
• Are the symptoms occurring shortly after feeding?
• Does the same food reproducibly cause the symptoms?
The Children’s Care Network 20Are These Symptoms IgE Mediated? A. Immediate reaction after meal B. Hives or swelling of unclear cause not related to meal C. Failure to thrive/gain weight, difficulty eating D. Colic or abdominal pain/gas E. Hay fever, asthma • Allergic rhinitis and asthma are triggered by environmental exposures • A chronically runny nose is not caused by food allergy • Asthma is triggered by food in the context of anaphylaxis The Children’s Care Network 21
Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
B. Hives or swelling of unclear cause not related to
meal
C. Failure to thrive/gain weight, difficulty eating
D. Colic or abdominal pain/gas
E. Hay fever, asthma
F. Parental request but no medical indication
Childhood Allergy (Food and Environmental) Profile
The Children’s Care Network 22Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
B. Hives or swelling of unclear cause not related
to meal
C. Failure to thrive/gain weight, difficulty eating
D. Colic or abdominal pain/gas
E. Hay fever, asthma
F. Parental request but no medical indication
• Food allergy IgE testing has a high false positive
rate
The Children’s Care Network 23Oral Food Challenges are Usually Negative in Children
with a Positive Allergy Test but no History of Anaphylaxis
Fleischer DM et al. J Pediatr 2011;158:578-83
The Children’s Care Network 24Only 1/3 of patients had
a history warranting IgE testing
J Pediatr 2015;166:97-100
25Only 1/3 of patients had These foods are difficult to
a history warranting IgE testing reintroduce after elimination
J Pediatr 2015;166:97-100
26Only 1/3 of patients had These foods are difficult to Panel Testing incurs waste in
a history warranting IgE testing reintroduce after elimination our healthcare system
J Pediatr 2015;166:97-100
27Are These Symptoms IgE Mediated?
A. Immediate reaction after meal
B. Hives or swelling of unclear cause not related to meal
C. Failure to thrive/gain weight, difficulty eating
D. Colic or abdominal pain/gas
E. Hay fever, asthma
F. Parental request but no medical indication
G. Atopic dermatitis/eczema
H. Screening for food allergy in infants prior to introduction
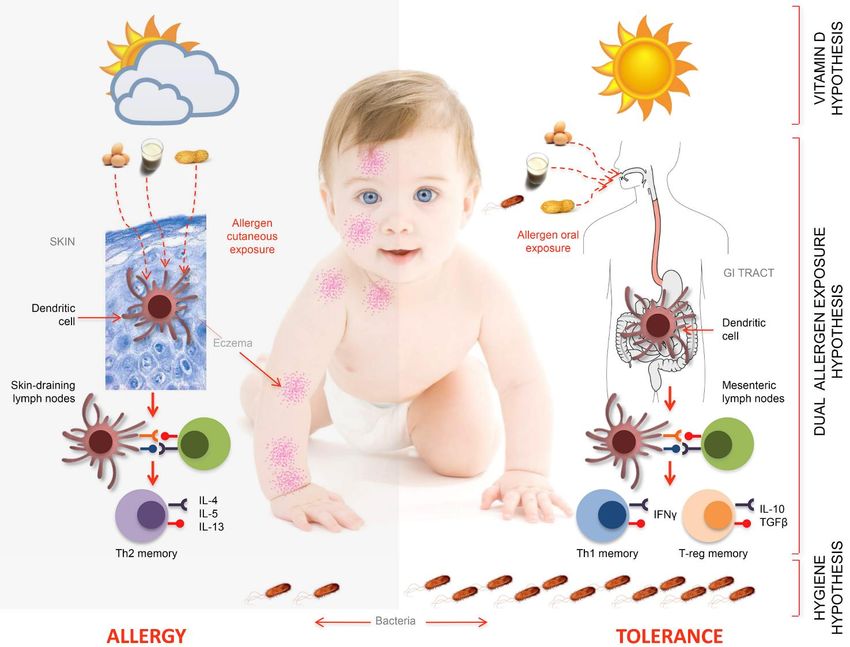
The Children’s Care Network 29Atopic Dermatitis and Food Allergy Dr. Brian Vickery
Early Life Events May Drive Food Allergies
1. Oral exposures induce tolerance in young mice
2. Elimination diets have been ineffective at preventing food allergy
3. Clinical presentation generally occurs in the 1st (maybe 2nd) year of life
4. Substantial observational evidence links lower rates of food allergy to
oral allergen exposure in infants
5. Definitive findings from randomized, controlled trials & meta-analyses
Liu AH NJRMC Update 2006
adapted from Zeiger RS JACI 1989
The Children’s Care Network 31Severity and Timing of Atopic Dermatitis (AD) is
Strongly Associated With Food Allergy
50.8% with early-
onset AD and high-
potency steroids
had challenge-
proven food allergy
• Prevalence of food allergy at 12 months of age is most closely associated
with:
– Time of onset of AD
– Potency of topical steroids (as a proxy for severity)
– Both effects appear to be dose-dependent
Martin PE, et al. Pediatr Allergy Immunol. 2015
Lowe AJ, et al. Annals Allergy Asthma Immunol 2018 The Children’s Care Network 32Common Null Mutations in the Skin Gene FLG Cause a
Leaky Skin Barrier: Risk for Peanut Allergy & Asthma
❌ ✅
Irvine et al NEJM 2011
Leung et al Sci Transl Med 2019 The Children’s Care Network 33Sheehan et al. JACI: In Pract 2019 Fox et al. JACI 2010
The Epithelium is Immunologically Active, Producing Cytokines Like IL-33 That Drive Allergic GI Inflammation Leyva-Castillo et al Immunity 2019 The Children’s Care Network 35
Du Toit G, et al. JACI 2016
36LEAP Study
• 640 infants (4 to 11 m/o) with severe eczema, egg allergy or both
• Randomized to consume or avoid peanut (SPT (+) and SPT (-) cohorts)
• Consumption of at least 6 g of peanut protein/week until 60 months of age
• Primary Outcome: proportion of children with peanut allergy at 60 mos of age
80% Relative Risk Reduction
NNT 7.1
Peanut Avoidance Peanut Consumption Relative reduction
Negative Skin Prick Test 13.7% 1.9% 86.1% (pEffect of Age and Eczema Severity on Peanut Allergy
Diagnosis
Keet C, et al. JACI 2021
The Children’s Care Network3 New Guidelines and Only for Peanut
• Provide anticipatory guidance
• Allergist referrals recommended ASAP after 4-6 month visit
• If successful, encourage regular feeding of > 6 g peanut protein per week
Togias et al. JACI 2016
The Children’s Care Network 40Pediatricians Know About These Guidelines for Peanut Allergy Prevention But Implementation is Difficult for Many Reasons Gupta RS et al. JAMA Netw Open 2020 The Children’s Care Network
Summary – I
• There is strong evidence linking early-life skin barrier dysfunction, pro-
allergic inflammation from epithelial cytokines, environmental allergen
exposure through the skin, and onset of peanut allergy
– “Dual allergen exposure hypothesis:” allergy develops when tolerance
mechanisms in GI tract are not engaged
• Early feeding overrides the pro-inflammatory skin priming, modulated by
complex genetic influences
• We have used this knowledge to successfully prevent peanut allergy in at-
risk babies with moderate to severe AD, but implementation in real world
settings remains frustratingly slow
The Children’s Care Network 42The Prevailing View Until Recently
[Exposure] =
window period
The Children’s Care Network 43The Prevailing View Until Recently
[Exposure] =
window period
The Children’s Care Network 44The Prevailing View Until Recently
[Exposure] = Sensitization
window period
The Children’s Care Network 45The Prevailing View Until Recently
[Exposure] = Sensitization
window period
The Children’s Care Network 46The Prevailing View Until Recently
[ ] = Tolerance
window period closes
The Modern View
Deliberate early = Tolerance
introduction
The Children’s Care Network 47Sheehan et al. JACI: In Pract 2019
Egg, milk, and fish are also detectable in dust, but is dual-exposure true?
“The evidence for clinical implications of
environmental peanut exposure during infancy is
strong and clinically important; however, it is
uncertain whether similar findings would result
from environmental exposures to other foods,
because peanut has been shown to have inherent
adjuvant properties capable of activating innate and
adaptive immune systems. Future similar studies in
other foods are needed.“
Fox et al. JACI 2010Five Egg Prevention Studies
Favors
Intro
Ierodiakonou D, et al. JAMA 2016
The Children’s Care Network 49• Retrospective chart review of 298 AD patients at Lurie Children’s referred for evaluation of FA • 19% with suspected food-triggered AD & no history of immediate reaction developed new IgE-mediated FA after an average of 1 year of an elimination diet • 24 of 31 (77%) of new reactions were to previously tolerated foods now being avoided • 30% of these reactions were anaphylaxis • Retrospective review of 442 at Riley Children’s: 13% “conversion” from trigger food to failed OFC • Similar findings from case series in Dallas, Netherlands, Israel, elsewhere Chang et al JACI: In Pract 2016 Eapen et al Annals 2019
How I Manage AD & FA in My Practice
1. Describe the chronic waxing-waning nature of AD with a parent (gain trust)
2. Establish the possibility that within this context, cause-effect associations could be
spurious
3. Shift the discussion from foods to skin
4. Review the family’s approach to daily skin care, which is quite often missing one or
more steps.
5. Seek a commitment to this skin care regimen with follow-up in 8-12 weeks off of
antihistamines for food allergy evaluation
– See: Thompson & Hanifin “Effective Therapy of Childhood Atopic Dermatitis
Allays Food Allergy Concerns” JAAD 2005
6. If not better, *only then* consider testing, elimination/rechallenge at that point…
The Children’s Care Network 51How I Manage AD & FA in My Practice
1. Describe the chronic waxing-waning nature of AD with a parent (gain trust)
2. Establish the possibility that within this context, cause-effect associations could be
spurious
3. Shift the discussion from foods to skin
4. Review the family’s approach to daily skin care, which is quite often missing one or
more steps.
5. Seek a commitment
All patients should have: to this skin care regimen with follow-up in 8-12 weeks off of
•antihistamines
Daily soaking for
bathfood allergy
at least evaluation
15 minutes in length
•– Plain, unscented cleansers
See: Thompson & Hanifin with neutral pH
“Effective Therapy of Childhood Atopic Dermatitis
• Liberal application
Allays Food of aConcerns”
Allergy cream/ointment
JAAD (not
2005lotion) immediately after bath and again
another time if possible
6. •If not
Usebetter, *only then*
of an appropriate consider
potency testing,
topical steroidelimination/rechallenge at thatdirectly)
PRN (address any steroid phobia point…
• Consideration of adjunctive therapies like wet wraps / bleach baths / topical or oral
antimicrobials
• Fingernails cut short
• Written / online instructions to refer to
see Boguniewicz et al: AD Yardstick in Annals January 2018
The Children’s Care Network 52Summary – II: Clinical Takeaways
• Encourage early (~ 6 mo) dietary diversity with complementary foods, starting w/
peanut & egg
– Families need simple, practical advice about what and how to do it (amounts, frequencies, signs/sx):
1. Cereals/grains first between 4 – 6 months
2. Fruit and veg purees next
3. Then start peanut, mixed in, and hardboiled egg -> move on to other foods
– More patient-facing resources are needed that are clear, brief, and easy to understand, ex. ASCIA:
• Early introduction is safe, with most babies tolerant and reactions almost always
mild, cutaneous
• Do not stop consumption unless clear evidence of immediate hypersensitivity;
consider OFC / prompt allergy referral -> expedited scheduling in our practice
• Resist the urge to test first! This is not supported by evidence and may be
counterproductive/harmful
The Children’s Care Network 53Goals for this Quality Improvement Project
Key Drivers:
• Reduction in the number of food allergen panel IgE tests
performed
• Reduction in the number of food allergen IgE tests where
Eczema/Atopic Dermatitis was the indication for the test
Secondary Outcomes:
• Reduction in epinephrine autoinjector prescriptions
• Reduction in healthcare expenditures in children with the
diagnosis of eczema/atopic dermatitis
• Reduction in food allergy incidence
The Children’s Care Network 54Can We Show that GA has the Lowest Rates of Food
Allergy in the US?
146%How we will support you!
• Patient handouts
– Eczema/Atopic Dermatitis
– Early Introduction of Food Allergens
– What to Expect During an Allergy/Immunology Visit
• Website with list of resources (handouts, videos, links to high quality
information): www.tccn-choa.org
• Newsletter
– Report of your practice’s performance on the quality metric
– Ask the expert forum: Send us your questions about eczema and food
allergy, barriers you’ve encountered, and we’ll answer them!
– SpecialtyQuality@tccn-choa.org
• Future initiatives
– Education videos for parents
56Conclusions
Food allergen IgE panels have several potential harms:
• They often test for foods the child is tolerating without a reaction
• A positive food allergy test can lead to misdiagnosis of food allergy
–Parent/patient anxiety
–Increased healthcare costs
–Potential increased risk of developing food allergy from avoidance
Atopic dermatitis/Eczema is a skin condition caused by a skin barrier defect
• Eczema patients have an increased risk of developing other atopic diseases
• Early introduction of food allergens reduce the risk of developing food
allergy
• Therefore, we should encourage early introduction of allergenic foods in
infants with eczema prior to the onset of food allergy, not elimination
The Children’s Care Network 57Ansley Atlanta
Hammill Family Foundation
Marshall Family
McMillen Family
Reynolds Family
Acknowledgements Steve Goodman
Thank you for your attention and your help / support!
bpvicke@emory.edu / www.choa.org/foodallergy
Follow me on Twitter: @ATLergistYou can also read