Commissioning Intentions 2019 - 2020 NHS Greenwich CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Commissioning Intentions 2019 - 2020
NHS Greenwich CCG
1|Page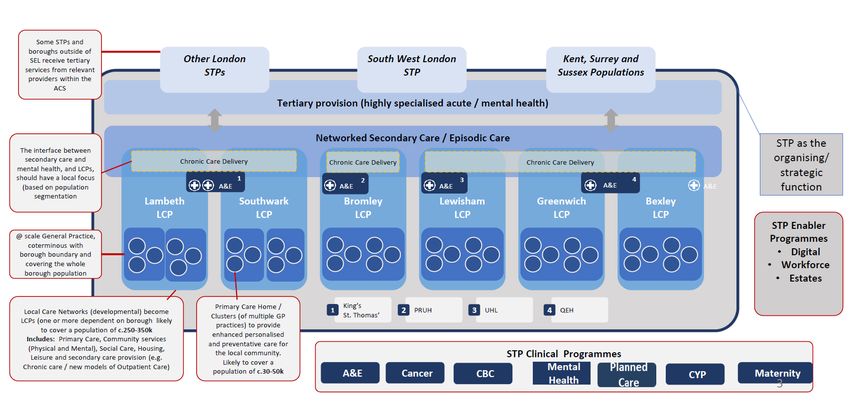
Contents
1.0 Forward ....................................................................................................................................... 3
2.0 South East London ...................................................................................................................... 4
3.0 Borough Based Integration ......................................................................................................... 5
4.0 Prevention ................................................................................................................................... 6
5.0 Acute Services ............................................................................................................................. 7
6.0 Community Services.................................................................................................................. 10
7.0 Integrated Urgent Care ............................................................................................................. 12
8.0 Mental Health Services ............................................................................................................. 14
9.0 Learning Disabilities .................................................................................................................. 16
10.0 Children and Young People (CYP) ............................................................................................. 17
11.0 Primary Care and Primary Care at Scale ................................................................................... 19
12.0 Cancer ....................................................................................................................................... 21
13.0 Rightcare ................................................................................................................................... 22
14.0 Enablers..................................................................................................................................... 23
15.0 Commissioning and Contracting Approaches for 2019/20 ....................................................... 24
16.0 Acknowledgements................................................................................................................... 27
Appendix One – Clinical Commissioning Strategy plan on a page ........................................................ 28
Appendix Two – SEL System of Systems ............................................................................................... 29
2|Page1.0 Forward
Throughout this year we have developed our clinically led Commissioning Strategy for
Greenwich and continued to build our relationships both with the Royal Borough of
Greenwich and neighbouring CCGs. Our emerging strategic direction of travel is that of
prevention, supporting people to live well and to change some of our underlying health and
social care determinates of health through four priorities;
To prevent illness and help our population to live well
To strengthen local support for people with mental illness, including children and
young people
To better meet the needs of frail older people with care closer to home, an integrated
urgent care system, and stronger community-based care
To improve the prevention, detection and treatment of cancers for our local
population
The South East London (SEL) health system continues to develop with increased combined
working across the six CCGs. We have consolidated some of our intentions together with
Bexley and Lewisham CCGs for services we commission from Lewisham and Greenwich
Trust. These are focused on planned and unplanned care. We have also combined some of
our commissioning intentions with the Royal Borough of Greenwich, in areas such as
Children and Young People and Mental Health services. Together these indicates a rich and
complex picture of integrated systems around Greenwich and wider partners, which informs
our considered approach to Integrated Care System as a system within systems.
Our Primary Care services remain challenging in terms of work force and so we are
developing opportunities to develop primary care at scale to provide a more sustainable
workforce across primary care.
Our QIPP challenge remains in 2019/2020 with significant opportunities around Children and
Young People, Mental Health as well as reductions in acute spend and improvements in
quality outcomes for our patients. Our financial QIPP challenge in 2019/2020 will be in the
order of £15m.
Through the Integrated Contracts Delivery Team (ICDT) team and Directors of
Commissioning we are now co-ordinating a common set of commissioning intentions to
providers across SEL together with more detailed specific borough intentions.
This paper sets out our commissioning intentions for the year commencing 1st April 2019 and
gives providers of health services a clear indication of where we are planning to make
changes next year in line with our commissioning strategy.
Krishna Subbarayan
Chairman NHS Greenwich CCG
3|Page2.0 South East London
The SEL Sustainability and Transformation Partnership (STP) has been developing a future
road map to implement our agreed Integrated Care System (ICS) of Systems for SEL. We
have over the last few months given particular focus to the step change in focus and delivery
that we will need to make across specific parts of our system - to support demonstrable
progress towards our end state vision and to ensure we are taking concrete action to
address key identified challenges and unlock opportunities in areas where there is significant
scope to improve our service delivery model and outcomes.
The commissioning intentions developed by the SEL CCGs build from our STP ICS Road
Map for 2018/19 and 2019/20 and are presented through the lens of our System of Systems
ICS. They are deliverable focussed and targeted at these areas – this document provides a
high level SEL wide summary and overview together with Greenwich specific intentions. The
detail of agreed implementation plans will be taken forward through a combination of:
Our work as an ICS aspirant programme – noting we are securing dedicated external
support to enable rapid progress be made in agreed priority areas – U&EC, planned
care and finance alongside overall governance and wider ICS development
Our discussions that will take place with providers and within systems over the next
six months to secure agreed plans, underpinned by signed contracts, for 2019/20
Challenges and opportunities
SEL is facing significant in year and forecast challenges – we have a major financial
challenge with a number of organisations in deficit, demand and capacity shortfalls in key
areas, performance challenges which are stark in relation to the delivery of NHS
Constitutional Standards for acute services, quality improvement opportunities including
addressing CQC report recommendations and challenges in relation to sustainable and
resilient services, from primary through to secondary care.
We therefore need to work collaboratively across the commissioning and provider system to
secure agreed changes for 2019/20 that will help us address these challenges and in a way
that supports a shift to integrated care and systems. Specifically we will need to give focus
to:
Agreeing and implementing a number of high impact care pathway changes that will
start to address our challenges across finance, demand and capacity, performance,
quality and service sustainability.
Agreed approaches to setting budgets and managing financial risk that recognise
resource availability, the financial constraints we are operating within, the need to
invest in our out of hospital care system and the need to ensure we are focussed as
a system on overall cost out not deficit shift or growing our way out of deficit.
Challenging ourselves and each other to adopt innovative and transformative
approaches, recognising that this will require a degree of risk taking but also the
need to do things differently and at pace and scale if we are to start to address our
current and future challenges in a recurrent and sustainable way.
A commitment to system working and coproduction to ensure collaborative
approaches that secure system win wins.
4|Page3.0 Borough Based Integration
Each SEL borough is proactively working to secure an integrated delivery model at borough
level, built on:
• Joint commissioning arrangements across CCGs and Local Authorities. Joint
commissioning is at different stages across SEL currently but there is a clear
commitment in each borough to progress integrated commissioning approaches.
• Integrated models of provision and delivery, focussed on and through our Community
Base Care strategies.
To support this each borough has and continues to develop innovative approaches to joint
commissioning and integrated provision as the borough (place) based building block of our
System of Systems ICS. This work includes establishing governance, planning and delivery
processes through which stakeholders will work together at borough level to secure jointly
agreed integrated care objectives. Over time this will result in changes to governance and
the operation of organisational boundaries in the delivery of services, new contracting
arrangements and changes to funding flows and risk management.
Within Greenwich we are developing our ICS programme through building collaboration of
providers and commissioners to develop and implement of an integrated community based
programme.
5|Page4.0 Prevention
The SEL STP has committed to developing concrete plans to enhance our prevention offer.
The aim is to ensure our prevention offer is systematically rolled out and embedded within
each and every level of our ICS development and delivery work. This will include the early
identification of risk and targeted intervention to improve population health, reduce disease
burden and health inequalities across the SEL population.
There is significant work being undertaken to tackle the wider determinants of health – the
SEL CCG commissioning intentions take a narrower focus, concentrating on NHS
interventions to identify and manage risk. In addition there is work on going to develop a SEL
wide prevention framework and strategy as part of the STP Prevention Programme - our
commissioning intuitions are consistent with that and will support progress in delivering this
wider strategy. Within our recently approved Greenwich clinically lead commissioning
strategy prevention is at the core and is the first of our four ambitions. See appendix one for
summary details. The full strategy is available upon request or via our website.
Systematic identification of risk at SEL level.
• We wish to agree a delivery framework, underpinned contractually, to support the
systematic collection of adult risk factors and baseline information - blood pressure,
alcohol, smoking, BMI and mental health – the adult Vital 5.
• In 2018/19 two SEL acute providers have started collecting this information – for
2019/20 we propose to spread the roll out to cover all acute providers, mental health
and community providers and primary care.
• Work also commenced in 2018/19 to develop a Vital 5 for children and older people.
For 2019/20 we propose to commence the collection of the children's vital 5
information – starting in the acute sector – and to enhance our adult Vital 5 with the
additional older people’s risk factors (frailty and falls) for targeted populations.
Commissioning of evidence based interventions at SEL level
There is good available evidence in relation to effective interventions and without waiting for
the rollout of vital 5 information, we wish to make a step change in our effort and investment
in these areas. Work is taking place to determine the most effective value based care
approaches and interventions but we are likely to focus on the following key areas and are
keen to work with providers to develop concrete proposals for 2019/20:
• Implementing the Ottawa model for smoking cessation, ensuring brief interventions
are available for alcohol and ensuring patients are sign posted to these services,
further expansion of our tier 3 services for weight management alongside the
development of tier 2 interventions, Implementation of blood pressure and
hypertension management guidelines and enhanced falls prevention services
Contribution to financial recovery at SEL level
Our assessment is that in the short term we need to increase our investment in the following
areas: infrastructure to support data collection and data sharing across the system plus in
agreed evidence based interventions and services. At the same time we will be seeking to
maximize the prevention element of our current core service provision through ensuring the
demonstrable delivery of Making Every Contact Count (MECC) across all area of our
commissioned services.
In the medium to long term the prevention investment will support reduced cost alongside
improved health outcomes – short term investment will therefore represent a medium/long
term - invest to save to secure an agreed benefits realisation.
6|Page5.0 Acute Services
Across SEL our vision is to implement a planned care model that supports RTT delivery and
wider planned care provision on a sustainable basis though developing:
• A core referral support offer for general practice and other referrers
• A transformed in hospital model – focused on outpatient transformation and best
practice pathways to reduce unwarranted variation and maximise productivity and
efficiency
• Networked provision to support sustainable service and site delivery
The STP has agreed to develop a more comprehensive planned care strategy – which will
address the wider issues such as capacity and configuration options for elective provision,
focused specifically on day case and inpatient provision across SEL. This work will be taken
forward over the rest of 2018/19 but is unlikely to impact on start year plans for 2019/20. The
ICS aspirant programme will support us in developing our plans for outpatient transformation
and networked elective provision – the outcome of this work will inform and may alter the
scope, pace and scale of the commissioning intentions highlighted below.
In hospital commissioning intentions - we wish to significantly increase the pace and scale of
our planned care work, to include:
• A systematic referral support offer – advice and guidance alongside robust referral
assessment services to ensure that patients are only referred if they need to be seen
in an acute setting
• Redesign of new outpatient services - a shift to straight to test, virtual appointments
and one stop appointments, thereby streamlining pathways whenever possible
• Agreed changes to the outpatient follow up model – shift to patient initiated follow ups
wherever possible and shift from face to face to virtual appointments
• Shared care approaches – for patients with chronic multiple long term conditions to
ensure patients are managed in community settings/under self-care, with agreed
triggers for the provision of advice and guidance/referral back in to hospital
• Agreed in hospital pathway improvements to maximise productivity and efficiency –
and reduce unwarranted variation and ensure the implementation of agreed clinical
effectiveness approaches (through the SEL Treatment Access Policy) – further work
is required to agree systematic STP wide approaches to securing optimised elective
pathways, productive and efficiency and clinical effectiveness and the resulting
system savings.
• Agreed development of networked services - with an initial targeting of services
which are currently fragile across SEL – urology and dermatology have already been
identified as key specialties for review and will be progressed in this year for 2019/20.
Out of hospital commissioning intentions - recognising the need to enhance in hospital
actions with robust out of hospital care action to optimise the value of referrals we wish to
ensure the following core OOH offer for 2019/20, recognising that there will be, partly driven
by current provision, differing areas of focus across the SEL CCGs:
• Effective mechanisms to manage referrals at the point of potential referral - a variety
of mechanisms are in place to support this from peer review to Referral Management
Services – aim is a core set of outcomes to be delivered through locally developed
approaches to ensure planned referral rates are consistently met
• The commissioning of community based alternatives – to support the repatriation of
activity from acute to community based settings. Key area of agreed focus are
ophthalmology, kidney disease, ENT, dermatology, cardiology and MSK.
7|PageDemand and capacity - acute services
• Demand and capacity planning and optimised utilisation of available capacity to
support RTT recovery is a key underpinning requirement and priority for 2019/20.
• SEL providers are currently breaching national RTT targets with differential waits
across specialties and site alongside the need to return to RTT compliance in
2019/20. We are keen to ensure that we agree approaches that support equity of
access of patients across SEL though joint approaches to waiting list and capacity
management.
• This is considered to be a sort term solution to current capacity constraints pending
the development of our planned care strategy, the implementation of optimised
productivity and efficiency across our elective pathways and the development of
networked approaches to provision. It will need to include the consideration of
outsourcing and in housing approaches where internal capacity is insufficient to meet
demand.
• We plan to sign off an agreed approach to managing demand and capacity across
SEL as part of 2019/20 agreements.
Diagnostics
Our objective is sustainable delivery of diagnostic targets plus diagnostic turnaround times to
support the delivery of wider planned care and cancer waiting times targets. We need to
agree mechanisms for managing demand and capacity effectively and collaboratively across
SEL providers - to ensure both optimised productivity and SEL wide management of
capacity to secure optimal waiting times and utilisation of available capacity.
Commissioning intentions to support these objectives are:
• Demand management – to triage requests across direct access and internal
pathways, to ensure the most effective utilisation of available capacity and optimise
waiting times.
• Capacity management – to complete the joint SEL STP and Accountable Cancer
Network led diagnostic strategy review – this will highlight demand and capacity
issues that need to be addressed across SEL
• Interim capacity management of 2019/20 – to determine an agreed strategy that
makes best use of available capacity across SEL where there are identified
constraints through the shared use of resource and waiting lists wherever possible,
working through a diagnostic hub model to secure these objectives.
Within Greenwich and as part of our common approach across Bexley, Greenwich and
Lewisham we aim to support the prevention agenda and helping people maintain their health
and wellbeing we are looking to move investment away from Acute into our community
primary care networks;
Long Term Conditions – Transformation of LTC services into primary care through
our GP federations and syndicates / networks. In 2019/2020 we want to start with
diabetes. There will be common service model across the three CCGs and will see
all type 2 patients and most of patients with type 1 diabetes being managed in our
primary care networks. The model will also bring together the current disparate
strands of transformation projects that are currently being delivered by Lewisham and
Greenwich GP Federations. There will be a transfer of resources to support this
development.
8|Page Out Patient Transformation (Surgery) - There has been limited change in the way
that Out Patient services have been delivered. Patients are routinely having multiple
outpatient appointments prior to a decision to list or not list.
Treatment Access Policies – We will continue to work across the six CCGs within
SEL to implement service changes to reduce the use of procedures of limited clinical
value.
9|Page6.0 Community Services
Community Based Care and our community services are the key building block to our ICS
system of systems at borough and sub borough level and will be vital in supporting our
planned strategic development of community based services.
Community provision and the community offer is currently differential across SEL, driven in
part by the investment that CCGs have been able to make over the last few years. Our SEL
CBC strategy is seeking to ensure that we further develop our community services to ensure
the provision of a core consistent offer, recognising that it will take time to secure this
objective. The CBC/community services priorities identified by the STP focus on the
following areas of development:
Admission avoidance services – to ensure all SEL residents have access to timely
admission avoidance services to enable them to be managed in their own homes and
avoid a hospital admission wherever possible.
Supported discharge services – to ensure all SEL residents have access to
community based supported discharge and reablement services to enable patients to
be discharged as soon as they are medically optimised. This will required the full and
systematic implementation of discharge to assess pathways and processes.
Targeted support for complex patients – community wraparound of primary and other
CBC services to provide care coordination and navigation for complex patients,
focused on supporting patients with multiple long term conditions, frailty assessment
and management, Care Home support and the last year of life (EOLC).
Community based alternatives - across planned and U&EC, including specialised
Long Term Conditions (LTC) Teams.
Bexley, Greenwich and Lewisham – the agreement and development of a community
services development plan that supports a more systematic, consistent and core community
offer that is focussed around a shift to home based support for patients, with a priority focus
on admission avoidance and supported discharge pathways.
As we increase our support to patients to live well and remain in their own homes we will
need to invest savings made in acute care into both community and as we will see later
primary care. Our main areas of priority and investment will be:
Community at Scale providers – continued development of alternative community
providers at scale both within Greenwich and wider across BGL. These will initially be for
Dermatology and Gynaecology.
Hospital at home – during 2018/2019 we transferred the hospital at home contract over
to Oxleas. We see the development of this service as key to the delivery of the urgent
and emergency care strategy by supporting people to live and remain at home. It’s our
intention to increase this.
COPD/Respiratory – patients with respiratory conditions often experience admission
into hospital and they are the largest cohort of patients attending ED and being admitted.
Following a combined respiratory summit across the three CCGs, a revised proposal for
commissioning respiratory services outside of hospital is being developed. It will be our
intention to implement the recommendations of the commissioning case, once it has
been approved.
10 | P a g e End of Life - Increase capacity and access to palliative care specialist support to enable
patient to achieve their preferred place of death and/or have improvement in their
symptom management and control.
Care Homes – We will continue our developments with telemedicine into care homes
and increase the community services support.
Transfer Of Care Collaborative – Continued development of the Transfer of Care
Collaborative process with providers in partnership with RBG to prevent and reduce
delays in transfer of care. This will include developments in:
Discharge 2 Assess model at Duncan House
Hospital at Home (see above)
Geriatric Intermediate Care Service at Eltham Hospital
Self-directed support and personalisation
11 | P a g e7.0 Integrated Urgent Care
Urgent and Emergency Integrated Care System - The STP has identified U&EC as a key
test bed areas for the further development of our borough based ICS model recognising that
effective U&EC provision is dependent upon whole system working across health and social
care to deliver an integrated offer support optimal patient outcomes and pathway efficiency.
Our commissioning intentions aim to support a step change in our delivery of this integrated
service offer underpinned by:
• A core in hospital service offer that provides a consistent and standardised pathway
model across the front door, same day and inpatient services and discharge,
delivered through national best practice approaches.
• A core out of hospital service offer that provides proactive admission avoidance and
supported discharge services, underpinned by best practice approaches.
• An integrated delivery model that supports single points of access and service
delivery across health and social care and community and acute based care.
• Joint approaches to managing services, budgets and risk across the system to
underpin our integrated delivery model.
The ICS model will take time to implement and we will need to jointly consider and agree
practical steps to enable progress to be made in 2019/20.
Across SEL our overall objective is a U&EC pathway that reflects optimised pathway
management – which will result in a significant shift from hospital to out of hospital care. This
will support:
• A sustainable U&EC system care across health and social care, underpinned by the
above consistent SEL in and out of hospital core offer that enables locally responsive
services delivered as part of an integrated delivery model.
• Improved performance across the U&EC system, underpinned by a more cost
effective, productive and efficient pathway model that manages resource across the
system to secure the best possible outcomes within available funding.
• Better provision of people’s needs in the most appropriate setting and if admitted
patients are discharged home for assessment of ongoing care needs as soon as they
no longer require acute based care.
In hospital commissioning intentions - roll out of the core in hospital offer
• Clinically led front door streaming model that ensures optimal use of alternative
pathways – both diversion of patients away from ED to OOH services (primary care &
admission avoidance services) and direct transfer to in hospital same day emergency
care or assessment units, as required.
• Full roll out of same day emergency care models operating 7 days a week – to
ensure that all patients presenting with ambulatory sensitive conditions are treated in
an ambulatory care setting and to secure a comprehensive frailty assessment and
acute frailty model.
• Full roll out of best practice internal flow initiatives - in ED, within assessment units
and on wards. Objective is to support flow, ensure no avoidable admissions take
place and reduce length of stay for those patients that require admission. A key
priority is ward flow processes and specifically the consistent implementation of
SAFER care bundles, Red to Green days and criteria led discharge, underpinned by
system support to ensure discharge at the point of medical optimisation.
12 | P a g eOut of Hospital commissioning intentions - roll out of the core out of hospital care offer
SEL’s OOH provision is inconsistent with a variety of available services and differing access
routes and criteria – this makes navigating the OOH care system challenging. Levelling up
our OOH provision and further developing the OOH care offer across SEL will take time –
but we are keen to ensure that for 2019/20 key tangible progress is made to secure this
objective. Across all boroughs we wish to ensure that there is clear provision for:
• Easy access to GP extended access from A&E, access to admission avoidance
services for GPs, LAS and A&E, services that target high intensity users and that
manage patients with multiple long term conditions, targeted support to Care Homes,
full access to Discharge to Assess pathways to include bridging capacity, community
based alternatives for UTIs and DVT and a review of therapy services to ensure
therapists are placed at all required stages of the U&EC in and OOH pathway.
In Bexley, Greenwich, Lewisham (BGL) and Bromley we wish to further develop our OOH
offer to include a shift over time from bed based to home based provision and to streamline
our admission avoidance and discharge services and access points. Significant development
work is required to develop an agreed CBC/OOH U&EC plan in BGL.
We will continue to work with partners across the health economy through the A&E Delivery
Board in delivering the Emergency Care Improvement Programme and support the transition
from an Urgent Care Centre (UCC) into an Urgent Treatment Centre (UTC) provider at the
Queen Elizabeth hospital. This will initially involve:
DVT service development
UTI treatment
Alternative streaming through community and social prescribing
Streaming improvements
Develop a dressing’s service in our primary care at scale a dressing’s service to
release capacity at the UCC/UTC.
Finally we will support our provider in the implementation of the new National 111
Contract.
We remain committed to commissioning the developing Ambulatory Care Pathways at both
Queen Elizabeth Hospital as part of their clinical model redevelopment and at UHL. Both of
which will be critical to the emergency pathway and reducing avoidable admissions. Integral
to the pathway is providing access to GPs for referrals and timely and appropriate advice
and guidance from clinicians.
13 | P a g e8.0 Mental Health Services
Mental health has not been identified as a key area of ICS test bed development,
recognising that the majority of MH services are jointly commissioned with Local Authorities,
across a range of organisations, on a borough basis.
SEL wide commissioning intentions are therefore less relevant in this area than in the test
bed areas identified, although MH services will form an essential element of our place based
Integrated Care Systems. Similarly acute networked provision, with the three south London
providers working collaboratively, will be an essential component of our horizontally
integrated system based ICS delivery.
In Greenwich we have developed borough specific commissioning intentions for MH together
with the Royal Borough of Greenwich for 2019/20 for discussion with local providers.
However we co-ordinated across SEL to ensure that we achieve;
• The systematic and consistent delivery of national performance standards in relation
mental health services – to include IAPT, CAMHS national standards
• Improvements in our acute pathway – working with the south London Mental Health
and Community Partnership to develop concrete implement and transformation
proposals and plans, that maximise collaborative and networked approaches across
providers, to do so.
• Ensuring effective system wide interfaces to support the management of MH patients
in crisis or requiring emergency care – to include a specific focus on ensuring robust
psychiatric liaison services and an onsite MH presence in SEL A&E departments plus
the ability to transfer patients in to community or bed based services from A&E in a
timely manner. The objective will be to ensure that patients are transferred from A&E
within national waiting times standards and without the need for admission to acute
assessment beds or wards.
• Ensuring the implementation of best practice pathway and bed management for MH
patients – to mirror acute based approaches and to include Red to Green days and
focused work to support discharge to assess pathways and optimised discharge.
• Development of approaches – through integrated community based care and within
acute and mental health inpatient settings - to support the holistic management of
physical and mental health needs. Specific areas of focus and development will be
combined mental and physical health rapid response teams, in reach support to the
acute sector for patients with dementia and delirium and in reach support from the
acute sector to support the management of physical health issues within MH wards.
• The phased implementation of Vital 5 across community and acute based mental
health services, to include a targeted risk assessment and intervention package for
patients with serious mental illness.
Within Greenwich we are going to target investment to support patients with mental illness to
manage their condition with improved escalation and intervention as well as prevention in
order to reduce mental health admissions. To achieve this we intend to start and build
alliance framework with providers in both statutory and voluntary sector together with both
the CCG and RBG:
Recovery College, Oxleas, early discharge planning together with a strong
integrated housing and placements without prejudice to support people to
return to a safe home.
Increased investment in IAPT and Crisis line wrapped around a new Primary
Care Plus (PCP) service to help people with mental illness to prevent
escalation.
14 | P a g e Dementia service development to support people to live in a safe
environment.
Continued development of the Live Well Greenwich programme with strong
links into PCP.
Increased focus on making every contact count.
15 | P a g e9.0 Learning Disabilities
Support people with learning disabilities to understand their rights, have inclusion,
independence and control of their lives;
Home Life – People with learning disabilities have a home of their own.
Work Life – People with a learning disability have job opportunities, and to be
able to make a valued contribution to the local work force either through paid
employment, voluntary work or work experience.
Family Life – We want to support carers and make sure they have fulfilled
lives.
Lifestyle – We want people with a learning disability to be well and healthy
through equal access to health care and health promotion services and to
receive reasonable adjustments to achieve this.
Social Life – Support people with a learning disability to make friends and
have relationships.
16 | P a g e10.0 Children and Young People (CYP)
To continue to make progress in implementing our STP children’s services priorities and to
ensure that our broader commissioning intentions - across prevention, U&EC, planned care,
metal health and community based care – include an appropriate and dedicated focus on
children’s services and outcomes.
Implementation of borough specific commissioning intentions – these will reflect joint
commissioning intentions across Local Authorities and CCGs – and will have been subject
to discussion with providers in year, noting they will in the main relate to community services
provided across health and social care commissioning portfolios. This summary does not set
out the borough specific CIs but summarises the SEL wide objectives and deliverables.
Acute services
• The implementation of agreed planned care approaches – referral support, referral
triage, in hospital pathway outpatient redesign and transformation - across children's
services.
• The consideration of networked provision for DGH services across SEL to support
effective demand and capacity management, service sustainability and resilience – as
part of our Acute Based Care Programme.
• The roll out of the Vital 5 for children on a pilot basis for 2019/20 – potentially working
with the Evelina Children’s Hospital across acute and community services.
Out of hospital services
• The continued development of admission avoidance and supported discharge services
for children, building on an at home model – including a specific focus on respiratory and
asthma admissions avoidance
• The development of agreed approaches to support care coordination and management
of complex patients
Integrated service delivery
Work to ensure that referral criteria and thresholds across services are clear - to include
specifically reviewing criteria thresholds for access to CAMHS services and expectations in
relation to the management of patients who require treatment but fall below acceptance
criteria e.g. current ADHD pathways
Work to ensure an enhanced support offer for schools around prevention, with a specific
focus on emotional health and wellbeing and weight management
We will build on our collaborative approach with RBG to develop a partnership with providers
to implement new models of care which support sustainable delivery of services that will:
Improve child health
Make the health and social care system more equitable for CYP
Reduce Acute hospital admissions and attendances
Create a health and social care learning system for CYP, Parents, Clinicians and
other professionals and carers.
We aim to achieve these by an increased focus upon prevention in partnership with the
Royal Borough of Greenwich.
17 | P a g e Targeting the management of long term conditions into primary care setting
with a focus upon:
Asthma
Diabetes
Dermatology
Epilepsy / Neurology and
Behavioural difficulties (ASD, ADHD)
Enable sustainable training – investment in training and education to make
prevention and self-care sustainable targeting;
Parents and YP
For all health and non-health professionals involved with CYP
Training in schools to identify and address physical and emotional health
and wellbeing
Paediatric Assessment Unit – We will standardise the paediatric ambulatory
offer at both Lewisham and Queen Elizabeth hospital sites.
CAMHS – Continue to develop integrated approach with providers across STP to
increase access for CYP with a diagnosis of mental health to 35%.
Bluebell – We have implemented a revised model to support children and their
families with respite care. We will now look to develop this model further in
collaboration with RBG in 2019/2020.
CYP often fall through the gap between childhood and adults so it’s our intention together
with RBG to start and create a change transition into adulthood strategy where we collective
ensure a smooth transition for CYP from 18 through to 25.
CYP CHC placements and personalised budgets – As we see our costs for
placements and CHC continue to rise, it’s even more important that we ensure we
get the best value and outcomes for our patients. To achieve this we are going to:
Development the marketplace to enable increased use of technology and new
models of care.
Increase the appropriate use of personalised budgets to increase the opportunity
to develop different types of package of care to improve patient outcomes.
18 | P a g e11.0 Primary Care and Primary Care at Scale
To support increased resilience and innovation in our primary care offer – to enable a
consistent and high quality offer that provides accessible, proactive and preventive care –
through a more explicit articulation of our core and enhanced service offer, working to
reduce unwarranted variation.
To develop our model of primary care delivery at a greater scale linked to our Local Care
Network delivery model.
To develop our GP Federations, in partnership with others, to provide the infrastructure and
organising function for primary care to secure an effective foundation for and primary care
contribution to our borough based integration.
Core primary care offer - To agree a consistent and targeted approach to primary care
incentive schemes for 2018/19 with incentives based on collective endeavour
Focussed around demonstrating a step change in delivering our core objectives:
•Proactive prevention – the roll out of a proactive Making Every Contact Count
approach across primary care, to include risk identification though the measurement
of Vital 5 risk factors (smoking, blood pressure, BMI, mental health and alcohol) for
our adult population and the proactive provision of advice, support and signposting to
follow up services for at risk patients.
•Care coordination for complex patients – the roll out of care coordination
approaches for patients with long term chronic conditions to ensure proactive
management of these patients in community based settings.
•Primary care extended access - To deliver a more efficient and targeted use of
primary care extended access to include promoting the assessment of patients at risk
of A&E attendance/hospital admission, a step increase in support to Care Home
residents and people in the last year of life and to proactively receive planned
hospital discharges.
•Referral optimisation - ensuring the full utilisation of all available referral support
tools and the utilisation of community based alternatives to acute referral.
GP Federation and Integrated Care development - The development of GP Federations and
support to local Integrated Care Systems in line with the deliverables set out in the SEL
primary care transformation bid:
• Infrastructure development – to support the development of core foundations for
supporting organisational capability and effective governance
• Supporting neighbourhood delivery – to support advancement in the use of
population health and performance data to drive a more systematic approach to
Quality Improvement and delivery at a neighbourhood (Primary Care network
delivery) level.
• System partnerships – to support development of formal relationships with partner
organisations to realise wider benefits.
19 | P a g eIn order to provide the delivery capacity at scale but still maintaining the balance of local
delivery with practices and syndicates there will need to be investment and changes to our
GP Federation:
Long Term conditions transformation into primary care, with initial focus upon
diabetes. This will be done in partnership across the three federations and will
see all type 2 patients and a majority of type 1 supported through primary and
community networks.
Proactive care management of frailty patients. The implementation of primary
care elements of frailty model.
Pathways - Referrals optimisation and management with increased triage and
support for new pathways.
High Impact Changes – Implementation of SCF and £3 per head monies into
infrastructure and support delivery of high impact changes releasing time back
into practices.
Children and Young People (CYP) implementation of initial schemes to support
the management of long term conditions and everyday health care for CYP:
In reach clinics
Paediatric Hot line / on line support
GP Decision support
20 | P a g e12.0 Cancer
To continue to make progress in implementing our STP cancer plan – focus on improved
early detection and diagnosis of cancer as well as improved cancer survivorship and
recovery care and support. Our key focus for 2019/20 however remains securing pathway
improvements across SEL to support the treatment of patients suspected of having and
diagnosed with cancer in line with national waiting time’s standards.
We wish to build on the positive progress made in 2019/29 in developing a system approach
to recovery – across planning and delivery. We wish to further develop this system approach
as part of our ICS development to push the concept of an integrated Accountable Cancer
Network that takes shared responsibility for delivery of cancer services and outcomes.
In hospital commissioning intentions
• Systematic roll out of best practice across all our hospital sites – to include pathway
and demand and capacity changes to enable us to deliver: 8 day polling on ERS for
all 2 week wait referrals, median waits of less than 7 days for first outpatient
appointment, Straight To Test (STT) models for agreed tumour groups, diagnostic
waiting times of less than 7 days, 14 day radiotherapy and surgery turn around, Red
to Green PTL tracking, overall adherence to tumour group timed pathways,
underpinned by shared PTLs and data management, utilising the Somerset system
• Review for 2019/20 implementation of: a system model for the delivery of EBUS
activity utilising a GSTT led hub and spoke model of provision, plus a review of
urology and dermatology provision (linked to planned care) to secure a SEL
networked model of provision.
• Networked approaches and sharing of resources related to underpinning
infrastructure to support cancer delivery – to include diagnostics, workforce, cancer
data teams, MDM coordinators and information systems.
• Implementation of system wide contractual approaches and governance to provide a
shift in accountability and responsibility across the system rather than on an
individual provider basis for the delivery of cancer timed pathways and waiting time’s
standards.
Out of hospital commissioning intentions
• Diagnosis - Work with primary care referrers to ensure the optimised utilisation of two
week wait pathways, implementation of the Faecal Immuno chemical Test (FiT)
across primary care, increase uptake of cancer screening
• Cancer recovery – agreed approach and standards in relation to stratified follow up of
patients and survivorship models/recovery support
• Implementation of a community based lymphedema service, targeting those CCGs
with a limited current service
21 | P a g e13.0 Rightcare
NHS Rightcare and Choosing Wisely - The STP will be taking forward work in the following
areas in 2019/20 as national NHS Rightcare priorities:
Musculo-skeletal, specifically work on the back pain pathway, ensuring adherence to
NICE and other best practice guidance, including the London Choosing Wisely back
pain management policy
CVD prevention, focusing on identification and effective management of patients with
hypertension, atrial fibrillation and familial hypercholesterolemia
Improved management of people with respiratory disease including asthma (in adults
and children) COPD and pneumonia
In each of these areas we would expect reductions in hospital admissions, through
investment in community primary care and prevention activities. As we develop our
business cases we will need to jointly discuss and agree the likely impact of this work on
acute activity.
22 | P a g e14.0 Enablers
We recognise that there are enablers that will require focus in order to support delivery of the
intentions. We will continue to work with providers and other commissioners to ensure
enablers are delivered to underpin our commissioning intentions:
Information Technology / Interoperability
Increase patient access to self-help information – Pre-GP
Increase access to e-consults
Build on infra-structure for virtual MDTs
Estates
Review estates strategy to improve utilisation
Future proofing through flexible approaches to utilisation – Gallions,
Kidbrooke
Resources
Building resilience into primary care through GPFV funded initiatives
Supported access to education and training via CEPN
Increase diversity of skill mix in primary care – i.e. Clinical
Pharmacists/Wellbeing coaches
23 | P a g e15.0 Commissioning and Contracting Approaches for 2019/20
Context
• Historically we have agreed bilateral contracts between each CCG and providers. We
will need to adapt and develop this bilateral approach to support the effective delivery
of integrated care approaches – moving over time to agree system based contracts,
outcomes and deliverables, budgets and risk management approaches.
• Current sources of funding are insufficient to meet current costs – a combination of
cost exceeding income due to inefficient service delivery models, prices that do not
cover delivery expectations and requirements and national pricing and charging
rules, resulting in an unaffordable acute funding mechanism that inhibits our ability to
invest in the out of hospital care system, an essential prerequisite to supporting a
shift to CBC.
• It is clear that if we are to live within our means and secure the step change from
fragmented organisationally focused delivery we will need to change our approach to
ensure new ways of contracting that support our ICS ambitions for the future.
Allocation of CCG growth funding - proposal
• The expectation is that CCG growth will increase in 2019/20 and for future years, to
an average of 3.4% per annum, an increase from the 2-2.5% received in recent
years.
• Whilst there are significant underlying cost pressures, associated with 2018/19
forecast outturn and potential 2019/20 growth and other pressures, we are keen to
secure a strategic utilisation of at least an element of the growth funding to
supporting ring fenced investment in agreed priority areas. Specifically we wish to
secure the agreement of STP partners to a growth top slice to support funding in the
following areas – prevention, community services and ICS development.
• Doing so will ensure we can make demonstrable progress in these areas –
investment in which will be key to our short, medium and long term sustainability as
well as improved patient outcomes across physical and mental health – but will
require us to take a different approach to agreeing funding for other commissioned
services, both those for which we determine an annual block value and those which
are funded under cost and volume arrangements.
• Our proposals will need to be reviewed in the light of national guidance and the
National Plan that is expected to be published in the autumn, although it is hoped
that our proposed top slice priorities will fit with identified national priorities too.
Contractual approaches
• Alongside consideration of funding we will also need to consider the most appropriate
contractual framework for 2019/20. We are likely to need to be flexible, recognising
the differential pace and scale of ICS development across SEL and the short period
of time before contracts will need to be signed.
• At a minimum we will be seeking to ensure that bilateral contracts are clear in their
reference to our ICS plans and associated commissioning intentions, including
system wide contractual deliverables and outcomes.
• We will ideally also wish to secure an agreed Memorandum of Understanding across
ICS partners to underpin system wide agreements alongside shadow monitoring
where appropriate.
• In other areas we may go further with more formalised system wide agreements – for
example though an Alliance contract or utilising the new national Integrated Care
Provider contracts.
24 | P a g e• Further discussion and agreement will be required with providers to determine the
most appropriate contractual arrangement for 2019/20.
COMMISSIONING AND CONTRACTING APPROACHES FOR 2019/20
Agreement of funding envelopes - acute and mental health providers
We would like to explore with providers the scope for shifting our current contractual
approaches, focussing specifically on those areas of commissioned service where
payment is made or assessed on a fee per item (PbR) basis. For acute areas of
spend we believe we need to move away from full PbR to adopt an alternative
service model that:
o Considers and sets for U&EC an agreed resource limit driven by an
assessment of available resources and cost reduction opportunities -
underlying activity and associated cost at full PbR and blended rates, plus
cost reduction opportunities if pathways were optimised utilising nationally
modelled expectations supported by out of hospital investment - to
determine an acute financial envelope. This envelope would then form part of
a wider U&EC system budget within which a system U&EC service offer could
operate and be delivered – on either a shadow monitoring or a full shared
budget and risk basis, depending on the progress made in developing a
concrete ICS proposition for 2019/20 across U&EC services.
o Considers and sets for planned care a funding envelope that is sensitive to
underlying referral demand but which differentiates fixed and variable cost
funding requirements and which incentivises both the collective management
of available capacity on a system basis and the optimisation of planned care
pathways.
o Ensures appropriate risk management mechanisms are in place for other
areas of acute commissioned spend to appropriately incentivise the
containment of costs and spend.
o For mental health providers funding arrangements tend to be block focussed
with some risk share around inpatient activity – we would wish to build on
approaches that secure block type funding agreements that take due account
of the opportunities related to pathway optimisation and pan provider
collaboration, building on the approaches to risk and gain share implemented
for tertiary pathways by the South London Partnership.
System management of finance moving to a system control total
ICSs are part defined by their approach to managing system finances – with an
expectation that shared budgets and approaches to risk management and gain
share are agreed, alongside a commitment to work to a system Control Total.
In South East London current underlying deficits and specifically the differential
position across organisations means this will be challenging to achieve but we
are keen to make demonstrable progress through:
• Utilising the approach outlined above to the setting of acute and mental health
budgets to enable a wider application of shadow or live system budgets to
support integrated care delivery and management.
• Linking the budget approach to an agreed approach to financial recovery and
sustainability – that understands deficit drivers across internal, system and
structural issues – and ensures that the implementation of our commissioning
intentions and specifically savings and efficiency opportunities support a
proportionate contribution to deficit recovery. In doing so we will be seeking
25 | P a g eclear commitments from all organisations to proactively deliver all internal
productivity and efficiency and pathway management opportunities and to
secure agreed actions to enable the release of wider system opportunities, to
ensure overall incremental cost out and deficit reduction across SEL.
26 | P a g e16.0 Acknowledgements
Integrated Contracts Delivery Team
• Sarah Cottingham
• David Smith
Unplanned Care
• Diana Braithwaite
• Gemma O’Neil
Mental Health & LD
• Colette Meehan
• Rachel Kharn
Children and Young People
• Kelly Sylvester
• Florence Kroll
• David Pinsent
27 | P a g eAppendix One – Clinical Commissioning Strategy plan on a page
28 | P a g eAppendix Two – SEL System of Systems
29 | P a g eYou can also read