CONNECTED AND COORDINATED: PERSONALISED SERVICE DELIVERY FOR THE ELDERLY - PWC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

www.pwc.com/global-health
Connected and
coordinated:
Personalised service
delivery for the elderly
October 2015
We are entering a new era of health – New Health
Health matters. It matters to each closer to the citizen and manage
of us as individuals and to society health collectively.
– it connects us all like no other. It
lies at the heart of our economic, New entrants from outside
political, social and environmental industries are already blazing a
prosperity and is one of the largest trail, but preserving the health
industries in the world. of the populace will ultimately
become a shared endeavour.
Two assumptions underpin the
traditional approach to healthcare: This paper focuses on the need
that it’s about the treatment of to shift our mind-set to reform
disease; and that it’s the domain and create more innovative and
of a particular professional group. effective ways to deliver services
We need a different approach to in ageing societies. We believe
cope with the ageing curve and those that quickly respond and
increasing incidence of chronic make sense of the changing
conditions – an approach that landscape will be the winners in
expands the focus from care and the new paradigm.
cure to vitality and wellbeing,
and from episodic intervention The transformation of health is
to personalised integrated upon us. A new era of healthcare is
services. We must also bring care emerging. Will you be ready?
Connected and coordinated: Personalised service delivery for the elderly | 2
Table of contents
The price of progress 4
Why the current way of caring for the elderly is neither 5
cost effective nor sustainable
A new service delivery model for the elderly 7
Addressing needs in a personalised way 8
Bringing everything together 15
The road to a new care model 16
A shared endeavour 24
Connected and coordinated: Personalised service delivery for the elderly | 3
The price of progress
Two related – and remarkable – Western Europeans now live alone. In more options and information about
changes have taken place in the last Australia, if current trends continue, the care they receive, more input into
century. Thanks to sanitation, safe there will be a 90% rise in 65+ single decisions about their care and higher
water, improved nutrition, modern person households from 1996 to 2021.5 standards of treatment.
medicine and better housing, we have Solo living is also on the rise in many
triumphed over many of the maladies emerging countries. Indeed, research Increasingly people want to receive
from which our ancestors died. And firm Euromonitor International services in their own homes. One
the average human lifespan has more predicts that there will be 288 million Australian study found that almost 60%
than doubled. In 1900, infectious single-person households by 2020 – up of Australians aged 70 years or over
diseases were the leading cause of from 240 million in 2010.6 would prefer to receive formal care at
death, even in developed countries like home in the event that they are unable
the United States. Today, the big killers In addition, the quality of the care to care for themselves, compared to
are heart disease and cancer.1 Global individuals of every generation seek is 28% who would prefer to receive
life expectancy at birth has soared increasing. Widespread access to digital residential care. The remainder would
from about 30 years to 70 years over information due to new technology prefer to receive care from family.7
the same period.2 and greater personal expenditure
on healthcare (in the form of higher The question is: how can we deliver
Yet this huge improvement in human insurance premiums, deductibles and this care? If the number of people aged
longevity carries a price. Whereas prescription fees) have both raised 65-plus swells by some 60% in the next
infectious diseases strike down people’s expectations. So have their 15 years, and the care they require
young and old alike, chronic diseases experiences as consumers, where mounts with age, yet there are fewer
become more prevalent with age. So having a voice, choice and convenience workers to support them, how can we
within current health systems, elderly are the norm. As a result, people want look after them all?
people consume more healthcare. In
the United States, for example, older
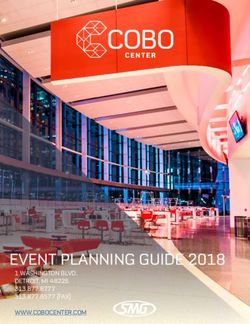
Figure 1: The ratio of retirees to workers is rising
citizens account for 14.7% of the
population but 33.9% of the healthcare The number of people aged 65 or older per 100 people of working age (15–64)
bill.3 A similar pattern prevails in the
35.9
EU15, with per capita expenditure on 33.5
healthcare roughly doubling between 31.2
the ages of 66 and 86.4 25.9
22.7 22.4
Moreover, declining fertility rates 18.1
17.1
have created a demographic double-
whammy: as the number of older 11.0 11.5
people is rising, so the number of 6.3 7.0
workers available to provide, and pay
for, their care is falling (see Figure Australia & Latin America & Northern
Africa Asia Europe
New Zealand the Caribbean America
1). And changing lifestyles mean that
fewer elderly individuals will be able to 2015 2030
rely on their relatives for help. Nearly
a quarter of all North Americans and Source: United Nations, World Population Prospects: The 2012 Revision (2012).
Connected and coordinated: Personalised service delivery for the elderly | 4
Why the current way of caring for the elderly
is neither cost effective nor sustainable
The current way of caring for the what they need, he notes, their top
elderly is economically unsustainable three priorities are pain management,
because it is based on a costly, companionship and financial advice –
hospital-centred health system. If we in that order.9 So healthcare providers
are to devise a better alternative, we are focusing on the wrong thing:
need to start by understanding the what’s the matter with the patient, not
real needs of the elderly and why we what matters to the patient.
currently spend so much on their care.
However, engrained clinical
Culture is one key factor. Health is assumptions are only one reason why
usually defined in terms of ‘disease’, caring for older people costs so much.
and older people have more diseases The other factors are structural. In
than younger people do. Hence, most countries, primary, secondary,
seen from a clinical perspective, the community and social care are
elderly suffer more illness – and the organised separately, with professionals
solution is more healthcare. But older who operate in an environment
people themselves often view things that encourages specialisation and
differently. In one survey of 650 segregation. At best, this means
elderly citizens in the Netherlands, that those who need care have to
for example, two-thirds of the navigate a circuitous path through
respondents – irrespective of age – said the system. At worst, it causes friction
their general state of health was good between different care providers and
or very good.8 In other words, they unnecessary expenditure on duplicate
enjoyed life, didn’t see themselves as tests and services, as the elderly get
sick and didn’t want to be medicalised. shuffled from one department or
organisation to another. Faced with the
Research by British gerontologist difficulty of navigating a fragmented
Ian Philp reinforces these findings. system, the simplest option for many is
When you actually ask older people to go to the Emergency Department.
Connected and coordinated: Personalised service delivery for the elderly | 5Similarly, in most countries, funding helped to live independently end
is allocated to individual institutions up in hospital, sometimes for quite
rather than networks of organisations lengthy periods of time. Yet hospitals
with shared goals. Each institution is were originally designed to isolate
a financial silo, with its own income people with infectious diseases, not to
from central or local government, care for those with protracted, non-
health insurers and patients or a communicable conditions.
mixture of the four. Many of the
reimbursement mechanisms that are In short, cultural biases, systemic
used also provide perverse incentives flaws and historical precedent have
(see sidebar, Volume versus value). all driven up healthcare spending on
And no one agency is responsible for the elderly, creating a model that is
coordinating the care people receive neither suitable nor sustainable.
or accountable for outcomes and
total costs. If we are to cope with the ageing curve,
we must adopt a new approach: one in
The net effect is to direct expenditure which health and wellbeing services
towards the costliest part of the are seamlessly coordinated to meet the
healthcare system: the hospital. needs of individual elderly citizens,
Many older people who could be many of whom may have complex co-
treated within the community and morbidities, effectively and efficiently.
Volume versus value
All the most common reimbursement models have drawbacks. The fee-for-
service approach rewards productivity but actively discourages efficiency,
while payment per day (where hospitals and nursing homes are paid an
agreed fee per bed-day) provides an incentive to treat patients for longer than
is really necessary.
Payment per case (where hospitals receive a single, standard payment for
every case, regardless of the actual cost of care) encourages the opposite
problem: early discharge and frequent readmission. And diagnosis-related
grouping (where hospitals receive a bundled payment covering a number of
treatments and services for a specific condition) is very difficult to administer.
Capitation (where healthcare providers receive a fixed amount of funding per
capita to cover the medical needs of a specific population for a specific period
of time) is probably the best model. But this must also be managed very
carefully to prevent skimping on care at the expense of outcomes.
Connected and coordinated: Personalised service delivery for the elderly | 6A new service delivery model for the elderly
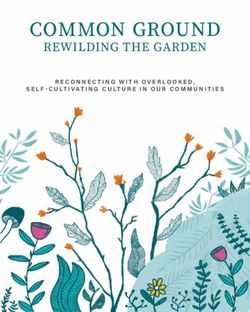
A new service delivery model for It should, furthermore, bring support The new model should also reward
the elderly should possess several services as close to the citizen as outcomes – as defined by elderly
fundamental characteristics, as possible. Companies like Apple, Google people themselves – rather than
illustrated in Figure 2. It should be and Amazon have upended retailing by activities, since it is not the number of
far more holistic, with the emphasis taking the store to the customer – and interventions but their effectiveness
on vitality and inclusion as much as the online experiences they offer are that counts. But for many systems
on care, and focused on self-rated shaping the expectations consumers this will require a shift in how we
quality of life and wellbeing, instead carry over to other industries, as many measure results. If quality of life is the
of focussing on illness. It should also of the companies now breaking into goal, client experience surveys can
be organised around communities, the healthcare business recognise. add valuable insight on how we rate
not institutions, with clusters of care These disruptive new players are outcomes, for example.
providers sharing accountability capitalising on wireless connectivity
for the budgets they manage and and advanced mobile devices to erase Lastly, it should be collaborative.
quality of the personalised services traditional healthcare boundaries Delivering individualised, integrated
they supply. and deliver health and wellbeing care entails dissolving ‘the classic
services anywhere.10 divide between family doctors and
hospitals, between physical and
mental health, between health and
Figure 2: We need to adopt a more personalised and integrated approach to service
social care, between prevention and
delivery for elderly in healthcare.
treatment’11 and between private and
public. Indeed, many of the factors
that influence wellbeing and quality of
Puts the individual at the heart of
the system
life – nutritious food, the right housing
stock, a reliable communications
infrastructure and the like – lie outside
Brings service delivery as close to the control of healthcare and social
the citizen as possible care providers. Maintaining a healthy
The core
population is not, therefore, just a
features Measures and rewards outcomes, job for the doctor, nurse or social
of a new not activities worker; it’s a collective challenge and
care model opportunity for many organisations
in many different industries. With
Treats health as a shared endeavour the powerful disruption of new
technologies and new entrants who
are entering healthcare from outside
Focuses on wellness and prevention, industries, this collective approach
not just care and cure empowers the elderly to co-create the
health support system we all need, and
Source: PwC analysis in a cost-effective way.
Connected and coordinated: Personalised service delivery for the elderly | 7Addressing needs in a personalised way
Attending to the diverse needs of #1. Helping older benefits, while (digital) befriending
an ageing society is a key challenge. schemes and group activities can
A more personalised model would
people stay independent alleviate social isolation – which
allow providers flexibility to address and healthy for as long doubles the risk of early death.13
population heterogeneity – to cope as possible
with differences between genders, The right housing (in terms of size,
“An ounce of prevention is better
socio-economic class, social network, location, layout and facilities in and
than a pound of cure,” as the saying
cognition, mood, loneliness and frailty. around homes) is equally important
goes, and some of the main causes
in helping people stay at home as they
of disease are avoidable. The first
So how does a new personalised age, so new housing stock should
step is thus educating older people to
service delivery model operate in reflect the needs of more mature
assume responsibility for their own
practice? We’ll touch briefly on the populations. Older housing stock
wellbeing and providing them with the
core features. can also be adapted with living aids,
necessary support. Some measures –
ranging from door-entry intercoms
such as dietary guidance and smoking
and stair rails to fully-fledged ‘smart
cessation aids – fall squarely within
homes’ and mobile technology.
the realm of healthcare. Others – such
In fact, technology can make a
as smoking bans, tobacco taxes and
major contribution to helping older
economic access to exercise facilities –
people maintain their health and
may require political intervention.
independence, be it through living
aids, diet and exercise apps, gaming
The next step is reducing the risks
and e-books for mental stimulation or
to which the elderly are especially
social networking for companionship.
vulnerable. Older people are, for
The elderly also need access to
example, more susceptible to infection,
transportation to stay connected to
more unstable on their feet and more
their community, friends and family.
likely to be lonely. Various studies
The advent of driverless cars may be
show that immunisation against flu,
a solution in the future, but in the
pneumonia and shingles reduces
meantime the benefit of transportation
the number of hospital admissions
services for the elderly should not
and associated mortalities.12 Fall
be overlooked.
prevention programmes have similar
Connected and coordinated: Personalised service delivery for the elderly | 8#2. Helping older Effective intervention is likewise Technology, including telehealth,
essential, and the key here is wearable devices, and sensor driven
people manage simple collaborative personalised planning detection software in homes, are
chronic conditions (see Figure 3). People with chronic increasingly helping older people
Much can be done to help older people conditions spend relatively little time and their relatives to engage and
manage simple chronic conditions, in contact with their professional care communicate with service providers
too. Early detection, supported by big providers, relying more on their own on their own terms.
data analytics which provide insights resources or peer-to-peer healthcare
and presights, is critical, but the jury communities such as C3N, Connected The most progressive doctors, nurses
is still out on the value of annual Living and PatientsLikeMe. Combining and social workers already recognise
health checks.14 Conversely, national the perspectives and expertise of older this. They know that the best care
screening programmes have proved people and their healthcare providers is shared care – where people make
very successful.15 Risk stratification enables those with long-term diseases choices informed by the expertise of
also enables doctors to identify high- to express their needs and preferences the professionals they consult, but
risk, high-cost patients and manage for treatment. It also encourages them choices that are still theirs. Alloheim
their care more proactively. to take better care of their own health is a fast growing elderly care provider
and wellbeing. in Germany with a strong client focus.
Figure 3: Collaborative personalised planning lets the individual participate in
the care process
A new consultation approach
Listen to
! Share professional
MIND THE GAP
personal life story insights
Information sharing
Agreed goal setting
and shared action
and care plan
Ask for state Each client &
of affairs first family contact
Then deliver care and
upgrade care plan
Source: Adapted from Angela Coulter et al., ‘Delivering better services for people with long-term conditions:
Building the house of care’, The King’s Fund, (October 2013).
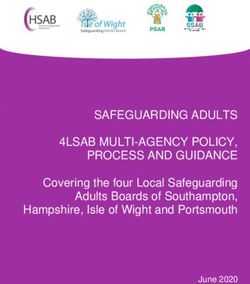
Connected and coordinated: Personalised service delivery for the elderly | 9Alloheim’s mission “Wir dienen ihrer Figure 4: Some care workers don’t listen to their clients as much as they claim
Lebensqualität” (We serve your quality
Survey responses from nursing home staff and residents showing percentage that agree with
of life) is an example of a successful each statement
company that proactively trains their
workers to be focused on the needs
and wishes of the elderly clients The client always has a ‘voice’
56.0%
to deliver a personalised service. in the care he or she needs
70.2%
However, not all care workers are so
enlightened. The multidimensional
benchmarking surveys conducted
47.8%
from 2010 till 2015 by ActiZ, the The provider is always open
to the client’s requests
Dutch association for healthcare 80.0%
entrepreneurs, show that those who
receive care are much less likely to Client Employee
agree they have a ‘voice’ in their care
compared to the professionals who Source: Aad Koster (CEO, ActiZ) and Robbert-Jan Poerstamper (Partner, PwC Netherlands) “Multidimensional
provide it (see Figure 4). benchmarking in elderly care”, Presentation at IAHSA 10th International Conference (Shanghai, 18 November 2013).
#3. Helping older people with complex
co-morbidities remain independent
Yet at some point in their lives, due Canadian geriatric hospital found that,
to ageing, many older people will on average, they were each taking 15
develop co-morbidities – no matter medications, with 8.9 drug-related
how well they look after themselves problems apiece.17
or how good the care they receive.16 In
such instances, it’s crucial to perform The final element in helping older
a multidimensional frailty assessment people with complex co-morbidities
covering the elderly person’s physical stay out of hospital is round-the-clock
and mental health, functional capacity, access to support services within the
social circumstances and home community. Three components are
environment. This should form the vital: multi-disciplinary community
basis for a holistic treatment, support teams to meet people’s everyday
and follow-up plan. health and social care needs;
ambulatory care clinics to provide
Since older people with co- specialist advice; and out-of-hours
morbidities often have to take multiple services to deliver urgent care. Current
medications, it’s also important to hospital-centred health systems are
review their regimens regularly to not designed to deliver care in a cost
reduce inappropriate polypharmacy. effective way for older people who
One study of people aged 80+ in a have multiple co-morbidities.
Connected and coordinated: Personalised service delivery for the elderly | 10#4. Helping older experience less anxiety at home.19
Several proven techniques exist for
people minimise the minimising the time the elderly have
time they have to spend to spend in hospital. Many older
in hospital people are admitted with ‘non-specific’
problems that are dismissed as social
Of course, proactive care doesn’t
or acopic. Conducting comprehensive
preclude the need for good acute
geriatric assessments, including
care in the event of an accident or
screening for malnutrition and
emergency. But many older people
dehydration, makes it easier to identify
don’t have to be admitted – and the
reversible medical problems and plan
best way of helping those who do is
all the elements required to discharge
to discharge them as soon as they
these patients safely. Specialist
are well enough to complete their
elderly care units and wards can also
recovery at home. This is not only
improve the quality of the care older
more economical; it also produces
people receive and reduce the length
better outcomes. Older people are
of hospital stays (see sidebar, Rapid
more vulnerable to hospital-acquired
access delivers results).20
infections, for example.18 And recent
research shows that most patients
Other techniques include discharge-
to-assess and continuous discharge
planning. The former entails
stabilising patients and then referring
them to a community care team to
Rapid access delivers results complete the assessment and organise
support for them in their own homes
In June 2010, Poole Hospital in Dorset, England, set up a specialist acute (see Figure 5). The latter involves
geriatric ward with a dedicated admissions system, rapid-access assessment conducting discharge reviews every
clinic, ‘triage’ rounds every morning for patients who were thought to be day. Many hospitals don’t discharge
well enough to discharge within 48 hours. There are daily multi-disciplinary patients on a Saturday or Sunday,
meetings involving medical staff and social services representatives and close partly because they have no senior
links with community care and intermediate care providers. The result? The staff qualified to discharge patients
proportion of patients discharged within 48 hours rose from 20.8% to 36.5%; working at weekends. But it’s far better
the mean length of stay fell by 14%; and average monthly occupied bed-days to hold daily reviews, include patients
dropped by 22%. and their relatives in the planning
process and discharge patients as soon
as they are ready.21
Connected and coordinated: Personalised service delivery for the elderly | 11Figure 5: Discharge-to-assess models direct patients to the most appropriate sources of further care
Coordination & crisis hub
Multi-disciplinary • Multi-disciplinary
team teams
• Family doctors/
Multi-disciplinary Out-of-hours Signposting
team doctors
• Paramedics • Medical
Integrated Integrated
Multi-disciplinary • Emergency • Nursing area team area team
team telephone line
• Mental health A&E/
• Social workers Medical Discharge
• Social care Integrated
• District nurse • Accident & assessment to assess
Emergency (A&E) • Therapy area team unit/Ward
• Community matron
• Social worker
• Community mental
health worker
Risk stratification, care planning
• Pharmacist
• Family doctor
Source: PwC whole system elderly care design with client in the UK
If such strategies are to work, though, nurses, 424,200 home health aides and
there must be adequate community 312,200 nursing assistants by 2022.22
care facilities at all times – and this
is one of several areas in which To prepare for this shortage, municipal
many countries at the moment are governments can invest in ‘re-
experiencing huge shortages. The US ablement’ care in the home (including
Bureau of Labor Statistics estimates, physical therapy and speech-language
for example, that if we don’t change therapy) and other policies and
the current health system, the United programs that encourage recovery
States would need another 580,800 at home, which may save money and
personal care aides, 526,800 registered improve quality.
Connected and coordinated: Personalised service delivery for the elderly | 12#5. Helping older people find the right residential
care, when they require it
Inevitably, some elderly people The quality of the care provided in
eventually reach the stage where they some care homes needs to improve
can no longer look after themselves. dramatically as well. A recent
Care in a residential home or nursing inspection of nearly 1,000 care homes
home is more costly than care in England found “appalling” failings.
delivered in a patient’s own home. Nearly one in ten residential homes
Even so, it is far less expensive than did not provide adequate care and
hospital care. In the United States, for welfare. The situation was even worse
example, the average cost of a semi- in nursing homes for elderly people
private room in a nursing home was with medical problems.25
US$222 per day in 201223 – nine times
less than the average inpatient day rate Detailed individual care plans and
of US$2,090.24 accurate record keeping – with up-to-
date information on every resident’s
medical history, psychological and
emotional profile, current medications,
communication needs and preferences
– would resolve some of these issues.
Comprehensive staff training to ensure
widespread understanding of clinical
guidelines and best practice, including
the importance of treating the elderly
with respect, would alleviate others.
Systematic sharing of information
with other care providers is also vital.
The best care homes maintain regular
contact with local family doctors,
community health teams, chiropodists,
gerontologists and the like. They
routinely monitor their residents
to detect avoidable conditions and
organise activities to provide mental
and physical stimulation. And, where
it’s feasible, they involve the residents
in their own care.26
Australia has implemented an Aged
Care Gateway to help consumers
navigate the system to get formalized
Photo credit: Vivium zorggroep
access to care and find the most
suitable provider. It will over time
The Hogeweyk village in the Netherlands provides an infrastructure which facilitates life as usual and
also include performance and quality
wellbeing for people suffering with severe dementia. information about providers.27
Connected and coordinated: Personalised service delivery for the elderly | 13#6. Helping older people Figure 6: In many countries, most people die in hospital
to die as well as possible
with palliative care Japan
Sweden
By far the biggest share of per capita
healthcare spending typically occurs in Spain
the final phase of life. Various studies
Portugal
show that most people would prefer
to die at home, yet most deaths still Canada
happen in hospital (see Figure 6). And France
the hospital is not just the place where
people least want to die; it’s also the England & Wales
most expensive. Australia
In the United Kingdom, for example, the Belgium
cost of a specialist palliative in-patient United States
bed day in hospital is £425, compared to
New Zealand
just £145 for a day of community care at
the end of life.28 Similarly, in Australia, Netherlands
the average cost of dying in hospital
(based on final admission) is A$ 19,000, Deaths in hospital Deaths in nursing homes 6.30
Deaths in other locations, including own home
versus A$ 6,000 for community care in
the last three months of life.29 Sources: “Where do people die? An international comparison”, International Journal of Public Health, Vol. 58
(2013), pp. 257-267; Centers for Disease Control and Prevention, Health, United States, 2010: With Special
Feature on Death and Dying (2011)
Dying is an even more exorbitant
business in the United States. Eighty
percent of the 2.5 million Americans
who died in 2011 were Medicare
beneficiaries.30 The care they received Again, several changes could make assess their physical, emotional and
in the last six months of life cost about a big difference. One such measure spiritual needs, and allows them to
US$ 170 billion – or US$ 85,000 per is early identification of people at draw up living wills that specify their
patient.31 Yet much of the money that the end-of-life stage to facilitate wishes, thereby reducing the incidence
is spent on end-of-life care makes advance care planning. Unlike of ‘futile care’.
the experience of dying worse, not people who are diagnosed with a
better. Many people are subjected to terminal illness, many elderly people More investment in palliative care
aggressive and unwanted treatments don’t experience a single event that teams to provide pain management
rather than getting palliative care. heralds their demise. So the UK Royal and emotional support at home
The humanitarian argument for College of General Practitioners would likewise allow many more
helping people end their lives well is as has issued guidelines to help family people to die in their own beds,
relevant and powerful as the economic doctors identify the estimated 1% of as would lending programmes for
one. How can we ethically balance people on their registries who will specialist hospital equipment. And
the needs of the individual with those die within 12 months.33 This makes all governments would do well to
of society? Should we concentrate on it easier to ascertain peoples’ end- consider providing more financial
preserving life at all cost? Can we – as of-life preferences and deliver more support for hospices, which are mainly
political philosopher Michael Sandel coordinated care. It enables the doctor funded through charitable donations
asks – put a price tag on life?32 to initiate a conversation with them to and voluntary work.
Connected and coordinated: Personalised service delivery for the elderly | 14Bringing everything together
To sum up, this new care model isn’t However, experience shows that it’s
“rocket science”. On the contrary, many possible to provide better, faster care
of the changes it requires are simply more economically by integrating
common sense. But that doesn’t mean the interfaces between primary,
they will be easy to make or to connect. secondary, community and social care
Systemic reform is invariably more (see sidebar The Canterbury Tale).34
complex than piecemeal modification, There’s much politicians, payers and
and making the transition will entail providers can learn from the path the
managing two different systems in pioneers have forged.
parallel for some years.
The Canterbury tale
In 2007, the healthcare system in Canterbury, New Zealand, was in crisis. The
population was rapidly ageing and admissions were rising, but the main hospital
in Christchurch was already ‘gridlocked’ on a regular basis. The district health
board estimated that Canterbury would need another hospital by 2020. It would
also need many more general practitioners and nurses, as well as an extra 2,000
residential care beds. This wasn’t feasible, given a deficit of nearly NZ$17 million
on a turnover of just under $1.2 billion.
So the district health board embarked on a major programme to introduce
integrated care. Since then, Canterbury’s acute admissions rate has fallen. It also
has the country’s third-lowest length of stay and acute readmission rates. The
number of elective procedures performed has increased substantially, various
conditions that once were treated purely or mainly in hospital are now provided
in general practice and growing demand for residential care has flattened,
thanks to better care in the community.
The health board’s finances have also improved dramatically, although a big
earthquake in September 2010 wiped out a projected $8 million surplus for that
year. Even so, Canterbury’s health and social care system continues to improve,
and the board projects that it will break even by 2014/15, despite incurring costs
of $25 million as a result of the earthquake.
Connected and coordinated: Personalised service delivery for the elderly | 15The road to a new care model
So what will it take to create a new there will be five regional authorities, ever comprehensive policy around
health system to support the quality of each constituting a single-tier elderly care. The so-called SPICE
life of older people? We’ve identified administration for the delivery of care program was developed by the Agency
eight key factors. in the area it covers.35 for Integrated Care and will partner
and collaborate with numerous groups
In 2011, the government of Singapore to provide elderly day care centres
#1. Political vision responded to the needs of its “pioneer in various regions of the island (see
and courage generation” and set in place the first- sidebar SPICE from Singapore).36
Political vision – and the courage to
enact change – is crucial. Governments
alone have the mandate to formulate a
national care strategy. And the move to SPICE from Singapore
personalised care for the elderly may
require such intervention, especially The Singapore Programme for Integrated Care for the Elderly (SPICE) is a
in countries with market-oriented or model of care developed by the Agency for Integrated Care (AIC) to provide
hybrid healthcare systems. Where comprehensive, integrated centre- and home-based services to support caring
subsystems of competing payers exist, of the frail elderly.
there is more fragmentation than in
systems with single payers. SPICE enables frail elderly who have high care needs and are eligible for
admissions into nursing homes, to recover and age within the community.
Governments are likewise the only Through SPICE Centres, a multi-disciplinary team comprising medical,
entities with the power to involve nursing, allied health and ancillary professionals provides a suite of
stakeholders from other sectors. patient-centric services such as primary and preventative care, nursing
Witness the imposition of legal care, rehabilitation services, personal care and social and leisure activities.
requirements on the packaging of These services are delivered both at the centre and at the patients’ homes,
cigarettes, despite fierce opposition depending on their needs.
from the big tobacco manufacturers.
AIC will partner Volunteer Welfare Organisations (VWOs) to operate SPICE
Many countries may also need new centres in various regions of the island. The centres will collaborate with the
laws to establish an overarching, Restructured Hospitals (RHs) and surrounding general practitioners (GPs)
coordinating body or harmonise to form a seamless model of care, which will help lower the need for nursing
incompatible regimes. The Finnish home admissions, decrease hospital admissions and visits to the emergency
government has already tackled the department, reduce caregiver stress and increase patients’ and caregivers’
first of these challenges. In March satisfaction with integrated care.
2014, it approved plans to unify the
provision of all social welfare and
healthcare. Under the new model,
Connected and coordinated: Personalised service delivery for the elderly | 16#2. Embrace change Driven by megatrends like telecoms operator Telus, teamed up
demographic shifts and technological with Sanofi Canada, the Canadian
and cooperate with breakthroughs, there is another, even affiliate of pharmaceutical firm Sanofi,
new entrants bigger change that care providers to launch a web-based platform
everywhere must make: namely, in that offers patients diabetes self-
the way they interact with companies management and monitoring tools.40
from other industries and the elderly A number of companies have also
individuals they serve. New entrants developed high-tech home diagnostic
from retail, consumer products, kits – and the X Prize Foundation’s
utilities, telecommunications and contest to create a Star Trek-style
technology industries are expanding ‘tricorder’ should yield even more
and reshaping the health sector. sophisticated devices.41 Furthermore,
home devices and wearables are
Some of these firms are tapping into increasingly digital and internet
the growing market for wellness connected. The internet of things will
and fitness products and services. help the elderly and their families
US pharmacy chain Walgreens is to manage medication, monitor
one such case; it recently acquired diet and nutrition, or stimulate
Alliance Boots in a move to become physical activity.
the first ‘global health and wellbeing
enterprise’ on the high street.37 Collectively, these ‘new kids on the
block’ are revolutionising the way in
Other companies aim to help older which care and support services are
people live more comfortably and delivered and create a new experience.
safely in their own homes. So, for They are importing the economic
instance, Norwegian energy and discipline that characterises other
telecoms provider Lyse has piloted a industries, where the customer is king
fire-alarm service in several homes and revenues are based on results.
with direct alarm to the fire brigade, They are also giving older people many
and that is integrated with different of the tools they need to ‘co-produce’
home automation services like door their care.42
locks, lights, ventilation and ovens or
coffee machines to make the service That has two consequences for
safer and more preventive.38 Similarly, traditional care payers and providers.
Deutsche Post has launched a new First, it presents them with some
service called ‘Personal Post’ for elderly critical decisions about whether to
citizens who live alone. Subscribers compete or collaborate with their
pay a small monthly fee to have a new rivals. Second, it alters the
postman ring the doorbell and speak dynamics of the relationship with the
to them every Tuesday till Saturday. elderly who need support services.
If something is wrong, the postman As healthcare becomes decentralised
notifies the local help service, which and democratised, older people will
immediately contacts a relative.39 expect a greater say in determining
the care they receive. They will no
Yet other new players are capitalising longer accept being defined in terms
on technological innovations to of disease and told what they need;
‘virtualise’ care. In 2012, for example, they will insist that their opinions and
Telus Health, a division of Canadian preferences be part of the dialogue.
Connected and coordinated: Personalised service delivery for the elderly | 17#3. Reallocation of Figure 7: Many countries have too many hospital beds
resources from the Canterbury,
1.57
secondary sector New Zealand
Ireland 2.32
It will also be necessary to reallocate United States 2.82
resources from the secondary sector United Kingdom 2.89
to the primary, community and social
Spain 3.08
care sectors. The most integrated
care networks operate with about Netherlands 3.14
1.57 hospital beds per 1,000 people
Portugal 3.30
without compromising the quality of
the service they provide.43 However, as Australia 3.77
Figure 7 shows, most countries are far
Italy 3.83
from this ideal.
Germany 5.96
Concentrating acute medical services New Zealand 5.97
in fewer, bigger, more centralised units
reduces wasteful duplication of services Belgium 6.26
and enables staff to increase their skills by France 6.30
treating more people. But converting or
closing hospitals is notoriously difficult, Japan 12.33
since it often engenders local opposition.
Number of hospital beds per 1,000 people
To build trust in society, governments in
Source: Business Monitor International and Canterbury, New Zealand, case
this position need to offer access to an
alternative supply of services for elderly
care as they streamline infrastructure, and the more complex forms of care sectors will also need extra funding,
whilst emerging market countries should a consultant would previously have if they are to play a part in providing
leapfrog to new service delivery systems supplied. This is driving up demand personalised integrated services for
for the elderly and avoid copying for generalists and gerontologists. The the different types of elderly people
the 20th century hospital-centred American Geriatrics Society predicts, we identified in the beginning of this
infrastructure of western societies. for example, that the United States will report and managing the impact of
need more than 30,000 geriatricians the demographic curve. To support
Redirecting resources to other areas by 2030 – up from about 7,500 today.44 this many home care and domiciliary
is imperative to close the ‘care gap’ workers will need professional training
that has emerged over the past few However, the number of specialists focused on elderly people’s real needs
decades. Secondary care has become is rising much more rapidly than the and capabilities. As an example of
increasingly specialised as a result of number of generalists. Many countries taking the needs and abilities of the
scientific and technological advances. will therefore drastically have to elderly into account, the Municipality
But though specialisation works well improve the attractiveness of general of Copenhagen decided in 2010 to
with single diseases, it is much less practice and alter their educational change home care for older citizens,
effective in treating medical conditions systems, as well as exploring new from only providing passive help –
that span diseases, such as the co- roles for other healthcare workers. where a home aid performs daily
morbidities that arise with age. Incentives and redirecting resources tasks for the client – to also offer re-
from the secondary care sector will ablement. Re-ablement is an approach
The primary care sector has been left help to finance these changes. focused on helping older adults to
to pick up the slack. Family doctors regain ability and maintain functional
now have to provide the generalist The social, residential, home care and independence, thus allowing them to
care that has always been their remit wellness services and palliative care stay longer in their own homes.45
Connected and coordinated: Personalised service delivery for the elderly | 18#4. New payment models England’s Quality and Outcomes Germany.47 Mexico is also working on
Framework (QOF) for general prevention and performance-based
practitioners, which was introduced incentive schemes around the most
Reallocating money from one part of the in April 2004, is one such instance. prevalent and costly diseases: diabetes,
care system to others won’t solve another The QOF pays family doctors for cardiopathies, oncology and neurology.
problem: funding schemes that reward meeting certain quality targets,
activities rather than outcomes. New more than half of which have to do Other countries are testing alternative
financing incentives and mechanisms with the management of common approaches. The Dutch Ministry of
will be required to redress this issue, chronic diseases.46 Health has, for example, launched
and several innovative payment models a bundled payment scheme for
have emerged in those countries that Performance-based incentives are also treating people with diabetes, chronic
are in the vanguard of integrated care. used in the Gesundes Kinzigtal obstructive pulmonary disease and
integrated care initiative, which vascular disease.48 Similarly, Denmark
Some of these new models employ serves the 31,000 members of two is trialling an incentive scheme under
outcomes-based payment incentives. sickness funds in Kinzigtal, southern which family doctors receive an up-
front annual payment for every diabetic
patient on their registries in return for
providing them with integrated care.49
The Manises model
Meanwhile, the United States is
In 2009, Bupa-Sanitas contracted with the Government of Valencia to provide
experimenting with accountable
primary, specialised and long-term healthcare for the 200,000 residents
care organisations (ACOs), in which
of Manises on the outskirts of Valencia in eastern Spain. The agreement –
groups of doctors, hospitals and other
which runs for 15 years, with an option to extend for another five years – has
healthcare providers come together
several distinctive features. It uses a per-capita payment model, with a fixed
voluntarily to provide coordinated
fee per person irrespective of the number of treatments received, thereby
care. When an ACO succeeds both in
encouraging Bupa-Sanitas to maximise its efficiency and invest in disease
delivering high-quality care and in
prevention because a healthier population needs fewer treatments.
cutting costs it receives a share of the
The agreement also allows the residents of Manises to attend a hospital savings, in the form of an advance fee
in another catchment area, if they want. When a resident goes elsewhere, and monthly instalments based on the
Bupa-Sanitas pays the other hospital a standard fee set by the Government. projected number of beneficiaries it
And when Bupa-Sanitas treats someone from outside its catchment area, it will cover.50
receives 85% of the fee. This creates healthy competition between hospitals
The English National Health Service
and drives up the standard of care.
(NHS) is piloting an even bolder
The results speak for themselves. In 2013, more than 90% of patients version of population-based care
attended a primary care appointment within 48 hours, up from 76% in 2009. delivery, with the devolution of
Meanwhile, waiting times for specialist consultations have fallen to about 16 control over all health and social
days, less than a third of the Spanish average of 53 days. care in Greater Manchester. The
region’s 10 councils and 15 clinical
Manises also scores highly on clinical quality and patient satisfaction commissioning groups will control a
measures. In 2012, it ranked first out of Valencia’s 24 health districts for budget of £6 billion, the goal being
improvements in maternal and palliative care, and second for improvements to provide ‘better, more joined-up
in health outcomes. And, in 2013, the average patient satisfaction score care’.51 But capitation payments to
was 8.17, out of a possible 10. Taxpayers have benefited, too; public-private institutional networks rather than
partnerships have yielded savings of about 30-37% per capita, compared to family doctors are still rare, despite the
the public-sector alternatives. advantages they offer (see sidebar, The
Manises model).52
Connected and coordinated: Personalised service delivery for the elderly | 19#5. New contractual their integration. The advantage an agreement that specifies the
of this model is that it gives the principles to be used for allocating
structures commissioning body a single point tasks, costs and any savings that
of contact. The downside is that it are achieved. Each care provider
New contractual structures will also restricts the commissioning body’s maintains its own internal controls
be needed to align the interest of ability to influence the behaviour of but is judged on the performance
payers, providers, new entrants from individual subcontractors of the entire alliance. And since
outside industries and citizens more each partner shares in the
• In a joint venture, the
effectively. The simplest solution is to profits, they all suffer if any one
commissioning body enters into a
merge all the providers in one single of the partners fails to fulfil its
contract of contracts with various
integrated organisation, but that is not obligations. Alliances are especially
third party providers. Joint
always feasible or likely to happen. suitable for complex projects where
ventures are an effective way of
Another option is to borrow from the budgets and deadlines can run
pooling expertise and increasing
various contract types used in the out of control. But they only work
operating efficiencies. But they
private sector. These include the prime when there is a good pre-existing
require a strong hand to overcome
contracting model, the joint venture relationship and the interests of
different cultures and management
and the alliance. Each has its own each partner are aligned with the
styles, and since everything is
strengths and weaknesses. aims of the alliance. Moreover,
agreed at the start, they may be
the model has not yet been
• In the prime contracting unsuitable for managing projects
thoroughly tested in the healthcare
model, a commissioning body has that evolve.
arena, although experience in
a contract with a prime contractor
• In an alliance, multiple the commercial world shows
for an agreed range of services.
commissioning bodies join forces that when alliance contracting
The prime contractor subcontracts
with multiple care providers to works well, it promotes a more
some of these services to third-
deliver a range of services (see collaborative spirit.
party providers and manages
Figure 8). The parties enter into
The particular contractual form a
commissioning body chooses will
Figure 8: Alliances are ideal for handling complex projects but largely unproven
obviously depend on the services and
in the care space
outcomes it wants and the market
in which it operates. But, whichever
structure it selects, it should be
Clinical Social care prepared to enter into a long-term
commissioning commissioning arrangement. At present, most
body body
contracts only last between one and
Care provider three years, which is a deterrent to
serious investment. In an industry
Care provider Care provider facing change and disruption,
healthcare networks will need to
be agile and adaptive, supporting
care providers to partner with
commercial companies like Apple,
Alliance todeliver services
Google, Amazon, Facebook, energy
providers, telcos and many other
big and start up organisations from
different industries.
Connected and coordinated: Personalised service delivery for the elderly | 20#6. Integrated Four general guidelines apply in #7. Effective governance
building an IT system that supports
information systems personalised service delivery:
and performance
and digitalisation management
• The needs of each of the
The ability to deliver integrated and stakeholders must be identified. Shared information is also, of
personalised services depends as much Clinical safety should obviously be a course, a prerequisite for effective
on integrated information systems top priory, as should the security of governance of any network – and this
as it does on the right financing and the system itself. The information is a much harder task than managing
contractual models, though. Care stored in electronic care records is a single organisation. The absence
services improve when doctors, social highly sensitive, so privacy should of a unified chain of command is one
workers, and family have immediate be a key consideration for both obvious distinction. But what is being
access to information. But integrated ethical and regulatory reasons. managed differs, too; orchestrating
information is not a challenge solely a network involves managing
for providers. Increasingly, the elderly • The system must work horizontally interactions rather than people.
and their caretakers will need to be as well as vertically. Most health IT
proactive owners of their own health systems are designed to perform a Moreover, while the diversity of
data. New technology, including specific set of functions in a specific the participants in a network is one
devices and wearables connected to department or organisation. of its greatest strengths, it poses
the internet, collects more and more But patients move from one equally great challenges. Each
data (big data), increasingly outside department to another and from partner specialises in a particular
existing care providers. As such, the one organisation to another, so it’s form of care, so it must have
citizen becomes the central node in vital to build a system that spans sufficient freedom to do its job
the use of his or her own information, the patient pathway. properly without compromising
and therefore involved in the seamless • The information contained within the performance of the network
delivery of the personalised services the system must also be accurate as a whole. And since the other
they need. and instantaneously available. partners lack its specific expertise,
Users must thus be able to update discerning where to draw the line can
The wave of digitalisation that it wherever they are, which means be difficult.
transformed industries like banking, that mobile access is essential.
travel and entertainment is now Robust multidimensional
disrupting healthcare. This wave • Lastly, the terminology and performance management and
will merge consumer technology and formats different care providers measurement is critical in these
medtech and bring services closer to and administrators use must be circumstances – and numerous
the consumer. standardised to encourage more measures of clinical performance
effective utilisation of existing IT have already been developed. But
Unfortunately, the IT systems and assets and minimise the amount of there are many other areas in which
software care providers use vary additional investment that is required. the indicators required to evaluate
widely. This creates numerous personalised integrated care are
problems, including errors as a These guidelines will facilitate the still missing: like the professional
result of duplicate data entry and construction of a truly interoperable involvement and capabilities to act as
difficulties in comparing data from client centred IT network. That, in a coach for elderly.
diverse sources. Furthermore, much turn, will enable multi-disciplinary
of the software that is commercially service delivery teams to manage the They can be loosely divided into two
available can’t be easily adapted elderly’s journey more effectively, let categories. The first is organisational
to reflect the requirements of people own and share their personal – the extent to which processes are
individual organisations. records, and pave the way for other integrated and the ease with which
advances based on the insights and people can be transferred from one
presights ‘Big Data’ produces.
Connected and coordinated: Personalised service delivery for the elderly | 21form of care to another. The second is experience, more efficient use of Figure 9 shows the conceptual design
the impact of personalised integrated resources, cost savings and improved and building blocks for an effective,
care and service delivery – the extent outcomes at both the personal and multi-dimensional performance
to which it produces a better client population levels. measurement system.
Figure 9: Evaluating personalised service delivery entails measuring three building blocks
Input Performance building blocks Results
On 4 levels:
Environment Population
Employee
Client engagement
Resources experience Organisation
Bench-
Strategy
marks
History Team or ward
Individual
Financial
performance
Strategic insights to improve quality & reduce costs
Source: PwC and ActiZ team analysis
The indicators used to assess these Effort Score (which measures the
dimensions may vary from one care effort it takes for a client to get things
system to another, but they must all done) give further insight into how
be relevant, reliable and viable. They satisfied people are with the service
must also be amenable to change they receive. In the Netherlands,
in the short- or mid-term, since no nationwide benchmark research shows
country can afford to wait decades that best practice organisations have
to find out whether it’s pulling the a balanced performance along the
right levers. And they must provide three building block dimensions: good
information on which the stakeholders client experiences driven by highly
can act. Indicators like the Net engaged professionals as a basis for
Promotor Score (NPS) or the Customer financial sustainability.
Connected and coordinated: Personalised service delivery for the elderly | 22You can also read