Pathways for Cardiology Symptoms in Primary Care - Dr Ivan Benett On behalf of the Leading Light's A Group of Primary Care Practitioners with a ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pathways for Cardiology Symptoms in
Primary Care
Dr Ivan Benett
On behalf of the Leading Light’s
A Group of Primary Care Practitioners with a Special Interest in Cardiology
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 1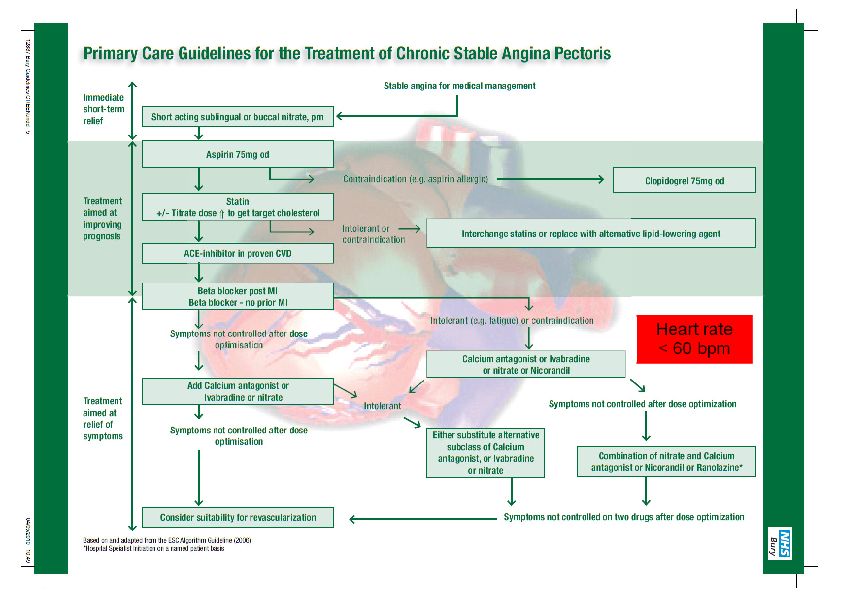
Acknowledgement
On behalf of the Greater Manchester & Cheshire Cardiac and Stroke Network (GMCCSN), I
would like to take this opportunity to thank Dr Ivan Benett, Dr Naresh Kanumilli and Dr Washik
Parkar for their enthusiasm, commitment, motivation and dedication in developing these
Guidelines to such a high standard. Our thanks also go to the Leading Lights Group, the
Cardiac Network Clinical Leads and the Collaboration for Leadership in Applied Health
Research and Care (CLAHRC) Team who have equally contributed with their knowledge and
expertise in cardiology.
We would also like to acknowledge the contributions of Dr Avril Danczak and Dr Selina Dunn,
for their involvement in the Heart Failure Guidelines and Dr Alan Fitchet and Dr Adam
Fitzpatrick (Consultant Cardiologists) who were joint authors with Dr Washik Parkar in the
Palpitations Guidelines.
Now the pathways have been endorsed by the GMCCSN Cardiac Board in it is envisaged that
these Guidelines will be adopted across the Network and be embedded within primary care.
Amanda J Schofield
Cardiac Programme Manager
Document V7.
Role Department Name (Title)
Owner GMC Cardiac & Stroke Network Amanda J Schofield (Programme Manager)
www.gmccsn.nhs.uk a.schofield1@nhs.net
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 2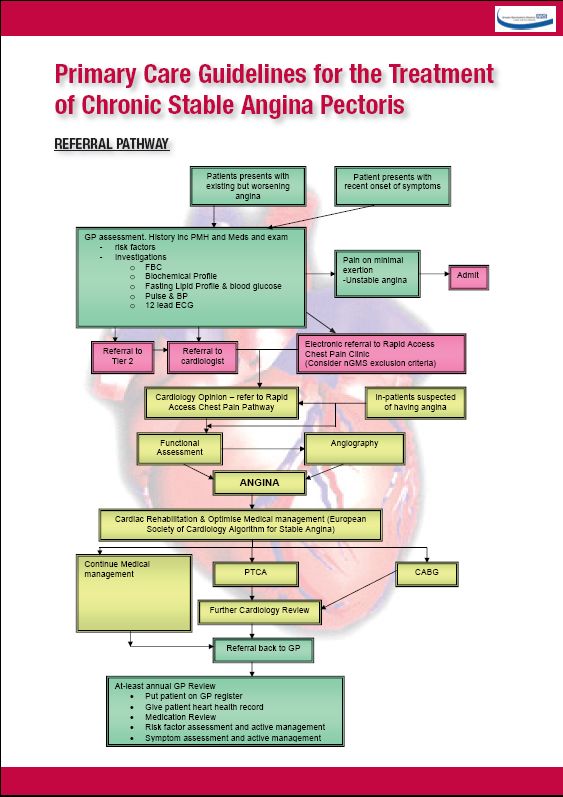
Table of Contents Page
Introduction ................................................................................................................................ 4
Aims........................................................................................................................................... 5
The Pathways Summary ............................................................................................................ 6
The Primary Care Chest Pain Pathway ...................................................................................... 7
i. Management of Acute Chest Pain .................................................................................... 8
ii. Management of Non-current but Acute Chest Pain ........................................................... 8
iii. Clinical Assessment of Chest Pain .................................................................................... 9
iv. Diagnostic Strategy in Patients with Chronic Chest Pain of Suspected Cardiac Origin .....10
v. Stable Angina Pathway .....................................................................................................11
vi. Primary Care Guidelines for the Treatment of Chronic Stable Angina Pectoris ................18
The Primary Care Palpitations Pathway ....................................................................................24
i. Palpitations Algorithm ......................................................................................................25
ii. Primary Care Palpitations Pathway Algorithm Notes ........................................................27
iii. Clinical Guidance for Management of AF in PC................................................................34
iv. CHA 2 DS 2 -VASc Scoring System .....................................................................................38
v. HAS-BLED Score ............................................................................................................40
vi. ECG Library .....................................................................................................................47
vii. Appendix 1. CHADS2 Score...........................................................................................53
The Primary Care Heart Failure Pathway ..................................................................................54
i. Initial Management of Chronic Heart Failure ....................................................................56
ii. Algorithm for the Diagnosis of HF ....................................................................................59
iii. Discharge after Acute Admission and On-going Follow-up ...............................................61
iv. Managing the Population .................................................................................................62
Reassurance to Patients without a Serious Heart Condition......................................................66
Preparing for and Managing People with Heart Failure at the End of Life..................................70
Appendix 2 Governance Structure ............................................................................................74
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 3Introduction
According to the Quality and Outcomes Framework (QOF), NHS Manchester has a prevalence
of coronary heart disease (CHD) of 3.2%, atrial fibrillation (AF) of 0.9% and heart failure (HF) of
0.6%. Manchester has a young population, so the prevalence is below the national average.
However, the standardised mortality rate (SMR) for heart disease is twice the national average.
For people under 75 years, the SMR is five times that of the leafier parts of England. In Greater
Manchester the prevalence is even higher, since the population is older.
If we assume a population of about 300,000 for NHS Manchester alone, then there are 10,000
people with CHD, 3,000 people with AF, and 1,600 people with HF. For every new person
diagnosed with any of these conditions there are probably nine who have presented to primary
care with symptoms which might have pointed to a cardiological diagnosis.
These numbers are too large to be managed in secondary care alone. Primary care must play a
greater part in being able to assess presenting symptoms and manage stable chronic disease.
The starting point is to define the role of primary care, in the form of a pathway. This needs to
be backed up with education, resources, and incentives.
PATHWAYS AIM TO MANAGE 80% OF PATIENT FLOWS, THERE WILL ALWAYS BE
EXCEPTIONS WHO DON’T FIT
This document attempts to define the pathways for the three conditions mentioned above.
Namely, angina, AF and HF. Education, resources and incentives are up to commissioners to
provide. In addition there is a statement about best practice for gathering information from
patients and offering reassurance, and care at the end of life.
PATHWAYS BRING GUIDELINES TO LIFE
Dr Ivan Benett, on behalf of the Leading Lights Group of Primary Care Practitioners with a
Special Interest in Cardiology (PwSI).
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 4Aims
The aim of these pathways is to:
i. Increase effectiveness of ‘primary assessment’ - 'From symptoms to secondary care.'
This is about getting the right people on the right pathway; the symptoms to look out for
and ask about; the examination to perform; the investigations to do. For example, when
to use a cardiac monitor for palpitations, or Brain Natriuretic Peptide (BNP) for HF?
ii. Improve the interface between primary and secondary care – referrals in, and
discharge out of hospital. This is about defining referral criteria. When to refer but also
when not to refer, if that is possible. For example, which chest pain NOT to refer to the
Rapid Access Chest Pain Clinic (RACPC). When should secondary care release
patients from follow-up back to the primary care, community or Tier 2 clinics?
iii. Manage stable long term conditions and palliative care in community clinics or
enhanced primary care. This is about defining primary care management of stable
angina, AF and HF. It includes drug titration, but also risk stratification, patient
education, self management and monitoring by patients, and when to contact the
practice for early advice before they need urgent admission. Managing patients’
adjustment to chronic disease, their ideas, concerns, fears and expectations, and
ensuring appropriate palliative care are generic to all pathways.
iv. Delivering quality of care. This is measured by audit, both quantitative and qualitative.
Each pathway will have a defined quantitative audit, with criteria and standards.
Qualitative ‘significant events analysis’ of significant events will be performed, for
example, hospital admissions. Finally, patients’ views of the service, their
understanding of their condition and symptom control is necessary.
So each pathway will include sections with these headings. In addition, there will be two other
generic sections that apply generically.
The first is a section on consultation skills about how to break bad news, and offer reassurance
and explanation effectively. Nine out of ten people who present to primary care with symptoms
that may relate to the heart end up needing to be reassured. Clinicians should to be able to offer
reassurance effectively. If there is a cardiology diagnosis, then the primary clinician needs to
have the skills to break bad news, explain the diagnosis and share an understanding of what
needs to be done.
Secondly, there will be a section on palliative care. ‘The final common pathway’ will define how
this can be delivered, to ensure people die with dignity in the place of their choice.
Establishing the learning needs and resources implications for delivering the pathways will need
to be done by each Primary Care Trust (PCT) or GP Consortium, as they develop.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 5The Pathways Summary
Many aspects of each pathway are not contentious, and often replicate National Guidelines. For
example:
• The need to case find as early as possible, especially in those at high risk.
• Effective primary assessment by the clinician who first sees the patient, which is usually the
GP, but could be specialist nurse, or in Accident and Emergency (A&E).
• Accurate, validated primary care register of patients.
• Providing the optimal evidence-based interventions that ease symptoms, reduce
hospitalisation and prolong quality of life.
• Effective patient education and support for self management, and support for carers.
• Specialist assessment, intervention and management planning.
• Continued management of people with stable disease.
Other aspects are more controversial. Some are common to all three pathways:
• The use of an intermediate clinic to filter patients going onto the pathway, and to manage
people, once stable, back into primary care.
• When to refer for a specialist opinion.
• Retrieval from out-patient follow-up of people once their condition is stable.
• The discharge process after acute admission, to prevent re-admission.
• Education and accreditation of practices.
Other controversies are more specific to each pathway.
The Primary Care Chest Pain Pathway
• The use of calcium scores in people presenting with chest pain.
• The importance of heart rate control for managing symptoms.
The Primary Care Atrial Fibrillation Pathway
• The method of identifying new patients with AF, both symptomatic and asymptomatic.
• Risk stratification for stroke and appropriate management.
• Strategies for rate and/or rhythm control.
• Referral for ablation.
The Primary Care Heart Failure Pathway
• Whether to use BNP (or NT-pro BNP), and what cut-offs, as a rule out test.
• When to refer for echocardiography.
The Final Common Pathway
• Planning for death and care at the end of life.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 6The Primary Care Chest Pain Pathway
By Dr Naresh Kanumilli
Background
The working group has agreed the use of GMCCSN Primary Care Angina Guidelines. These
were based on the European Society of Cardiology (ESC) Angina Guidelines already agreed by
NHS Bury. The GMCCSN Imaging Pathway is also to be adopted.
In common with other pathways, the group recommends the need for a Tier 2/PwSI led service
to:
• Assess referrals, manage or refer on to secondary/tertiary care.
• Improved symptom control.
• Up-titration of secondary prevention medication.
• Lifestyle modification and education.
• Ensuring referral to cardiac rehabilitation where appropriate.
• Discharge to/communication with GP.
Placement of Tier 2/PwSI service may differ both geographically and within the pathway itself
depending upon local service requirement.
CASE FINDING
People with QRISK of > 30%, hypertension or diabetes are at risk for developing ischaemic
heart disease. They should be asked explicitly about chest pain symptoms at annual review.
THE PRIMARY ASSESSMENT
The primary assessment of chest pain requires a careful history of the nature of the pain. The
three features to ask about specifically are:
• Association with exertion or stress.
• Relief by rest.
• Relief by nitrates.
Cardiovascular examination, including pulse, blood pressure and auscultation for murmurs
should be undertaken.
Initial investigations should include a full blood count, urea and electrolytes, thyroid function,
fasting lipids and blood sugar if not known to have diabetes.
A resting electrocardiogram (ECG) may reveal abnormalities and will act as a baseline.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 7The working group identified the areas that could potentially utilise a Tier 2/PwSI service
(highlighted in the orange circles or boxes) on both the imaging and Angina Guideline pathways.
Note the imaging pathway does not include calcium scoring, as this is not available at present.
The Guidelines highlight the initial requirements of the GP role, and suggests the option of
referral into Tier 2 rather than cardiology or RACPC where there is uncertainty.
Box 1 – Management of Acute Chest Pain
Do not delay transfer to the hospital.
In the order appropriate to the circumstances, offer:
• Pain relief (glyceryl trinitrate) and/or an intravenous opioid.
• A single loading dose of 300mg aspirin unless the person is allergic. Send a written
record with the person if given before arriving at hospital.
• Only offer antiplatelet agents in hospital.
• A resting 12-lead ECG. Send to hospital before the patient arrives if possible, but do not
delay transfer.
• Other therapeutic interventions∗ as necessary.
• Pulse oximetry:
offer oxygen if arterial oxygen saturation (Sa0 2 )is less than 94% with no risk of
hypercapnic respiratory failure. Aim for Sa0 2 of 94 - 98%;
people with chronic obstructive respiratory failure (COPD) are at risk of hypercapnic
respiratory failure.
Aim for Sa0 2 of 88 – 92% until blood gas analysis is available.
∗
Follow Acute Coronary Syndrome (ACS) Guideline or local protocols for ST Elevation
Myocardial Infarction (STEMI).
Box 2 – Management of Non-current but Acute Chest Pain
Chest pain within the last 12 hours and now pain free
• Clinical assessment.
• 12-lead ECG:
normal: same day (urgent) hospital referral for assessment;
suggests ACS: manage as Box 1.
Chest pain between 12 and 72 hours ago
• Detailed assessment including ECG and troponin needed.
• Need for referral and its urgency decided by local factors and clinical judgement.
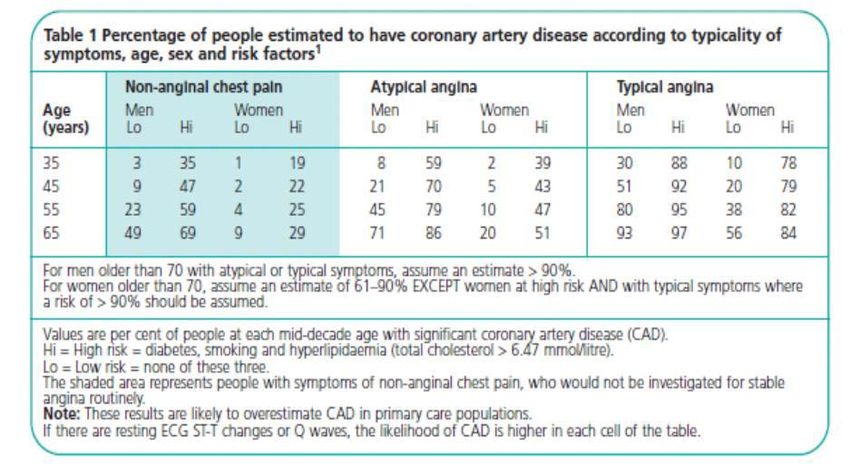
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 8Box 3 – Clinical Assessment of Chest Pain
Anginal pain is:
• Constricting discomfort in the front of the chest, or in the neck, shoulder, jaw or arms.
• Precipitated by physical exertion.
• Relieved by rest/glyceryl trinitrate within about 5 minutes.
• Three of the features above are defined as typical angina.
• Two of the three features above are defined as atypical angina.
• One or none of the features above are defined as non-anginal chest pain.
Use clinical assessment and the typicality of anginal pain features listed in Table 1 to estimate
the likelihood of coronary artery disease (CAD).
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 9Diagnostic Strategy in Patients with Chronic Chest Pain of Suspected Cardiac Origin
Prior probability of CAD Investigative strategy and rationale
Trust your clinical judgement no further testing
90% (with typical angina)
diagnosis
REFERRAL FOR SPECIALIST OPINION
Referral for Specialist Opinion
Patients with possible cardiac chest pain should be referred to the RACPC (see existing
pathway below).
Referral to an Intermediate (Tier 2) Clinic
For practices that do not have the confidence to make an effective primary assessment, or are
uncertain about whether to refer to secondary/tertiary care, a referral to a PwSI led intermediate
(Tier 2) clinic is appropriate. See existing pathways.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 10Stable Angina Pathway Referral to Rapid Access Chest Pain Clinic
Blocks shown larger in
following pages Explain the implications of a negative result or of a positive result
Low pre-test probability (see overleaf)* Medium pre-test probability( see overleaf)* OR unable to complete exercise ECG OR High pre-test probability* (see overleaf) and able to complete exercise ECG
of angina being the cause of chest pain and able to complete exercise ECG uninterpretable resting ECG OR contra-indications to exercise ECG (see medium risk box)
(see medium risk box)
Negative Non-invasive cardiac imaging, i.e. stress exercise echo, dobutamine stress echo (DSE) Exercise ECG
Strongly positive ST Segment Exercise ECG myocardial Perfusion Imaging (MPI) cardiac CT angiography (CTA) or cardiac MR (CMR)
depression with low cardiac
workload up to 4 metabolic or
Duke score -11 or worse. Discharge and reassure Negative Strongly positive ST Segment
Positive ( not Negative Low risk of CVD or inconclusive except as in box Positive depression with low cardiac
strongly) ( QRISK2) to immediate right OR workload up to 4 metabolic or
or inconclusive inconclusive but Duke score -11 or worse.
Angiography with a view to
High risk of CVD history of CVD or diabetes.
revascularisation (QRISK2) Discharge and reassure
Cardiac imaging AND Class III angina on
Review medical therapy. OR medical treatment Angiography with a view to
Angina Plan. history of CVD or diabetes
revascularisation
Low or medium Review medical therapy.
Review preventative and pre-test probability or Angina Plan.
Negative
symptomatic therapy symptoms comparable
Negative Cardiac Imaging
with class I or class II
angina
Discharge High risk pre-test probability but unable to have Review preventative and
exercise ECG or class III angina symptomatic therapy Class I or class II angina ■
Discharge and
reassure
Review at 6 months
High risk pre-test probability or
class III angina ■
Discharge
class III or IV angina
Not class III or IV angina
Angiography with a view to
Discharge and reassure revacularisation
Review medical therapy.
Angina Plan. Review at 6 months
Very low pre-test probability (see overleaf)*
of angina being the cause of chest pain and able
to complete exercise ECG No recent angina class I or class II angina class III or IV angina
Positive
Discharge and reassure Discharge Repeat cardiac imaging Angiography with a view to
revacularisation
Without indication for immediate Review medical therapy.
angiography ( as in right arm of CCS class III angina after medical treatment.
Angina Plan.
pathway)
High-risk criteria on noninvasive testing regardless of
anginal severity (see details overleaf) ┼
Patients who have been successfully resuscitated
Medical therapy with measures to
from sudden cardiac arrest or have sustained (>30
improve adherence and angina plan
Discharge No recent angina seconds) monomorphic ventricular tachycardia or
nonsustained (* Pre test probability is based on typicality of angina symptoms and CVD risk score.
The classification of chest pain is based on:
"(i) substernal chest discomfort with a characteristic quality and duration that is (ii) produced by exertion or emotional stress and (iii) relieved on rest by nitroglycerin.
Very Low pre test probability of angina being the cause of the chest pain is when none of the above characteristics exist, there is no history of cardiovascular disease and the CVD risk, calculated
by QRISK2, is less than 20% over the next ten years .
Low pre test probability of angina being the cause of the chest pain is when only one of the above characteristics exist, there is no history of cardiovascular disease and the CVD risk, calculated by
QRISK2, is less than 20% over the next ten years .
High pre test probability is when all three of the above characteristics exist
AND EITHER
the CVD risk, calculated by QRISK2, is more than 30% over the next ten years (excluding class IV angina)
OR
there is a history of cardiovascular disease.
Medium pre test probability are all others
┼ High risk criteria on non-invasive testing regardless of anginal severity
- Severe resting left ventricular dysfunction (LVEF25% of myocardium or >25% anterior myocardium)
- Regional wall motion abnormality (≥ 4 segments)
# Factors that are more likely to lead to angiography are no or little symptomatic improvement or the previous cardiac imaging showing between 12.5 – 25% stress induced myocardial perfusion defect.
For others, there is more likely to be a review after three months but the threshold for angiography will become lower at each review.
■Patients in this box still have classical symptoms of angina but there is no evidence on investigation that they have ischaemic heart disease
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 12Very low pre-test probability (see overleaf)*
of angina being the cause of chest pain and able to complete exercise ECG
Discharge and reassure
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 13Low pre-test probability (see overleaf)*
of angina being the cause of chest pain and able to complete exercise
ECG
Strongly positive ST Segment depression with
low cardiac workload up to 4 metabolic or Duke Exercise ECG Negative
score -11 or worse.
Discharge and
Angiography with a view to revascularisation Positive ( not
reassure
Review medical therapy. strongly)
or inconclusive
Negative Cardiac Imaging
Discharge
Positive
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 14Medium pre-test probability( see overleaf)* OR unable to complete exercise ECG OR uninterpretable resting ECG OR
contra-indications to exercise ECG
Non-invasive cardiac imaging, i.e. stress exercise echo, dobutamine stress echo (DSE) myocardial Perfusion Imaging
(MPI) cardiac CT angiography (CTA) or cardiac MR (CMR)
Negative Low risk of CVD
( QRISK2)
High risk of CVD
(QRISK2) Discharge and
OR reassure
history of CVD or diabetes
Low or medium
Review preventative and symptomatic therapy pre-test probability or
symptoms comparable
with class I or class II
angina
High risk pre-test probability but unable to have
exercise ECG or class III angina
Discharge
and reassure
Review at 6 months
Not class III or IV
class III or IV angina
angina
Positive
Discharge and Angiography with a view to
reassure revacularisation
Review medical therapy
Angina plan
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 15High pre-test probability* (see overleaf) and able to complete exercise ECG
(see medium risk box)
Exercise ECG
Negative
or inconclusive except as in box to Strongly positive ST Segment
immediate right depression with low cardiac
Positive workload up to 4 metabolic or
Cardiac imaging Duke score -11 or worse.
OR
inconclusive but
history of CVD or
diabetes. AND Class III
Negative angina on medical Angiography with a view to
treatment revascularisation
Review medical therapy.
Review preventative Class I or class II
and symptomatic angina ■
therapy
Discharge and
High risk pre-test reassure
probability or class
Positive III angina ■
Review at 6 months
Repeat cardiac
No recent angina class III or IV angina
imaging
class I or class II
Discharge Angiography with a view to revacularisation
angina
Review medical therapy.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 16Positive
Without indication for immediate
angiography ( as in right arm of CCS class III angina after medical
pathway) treatment.
High-risk criteria on noninvasive
testing regardless of anginal severity
(see details overleaf) ┼
Medical therapy with measures to
improve adherence and angina plan
Angiography with a view to
No recent angina revascularisation
Review medical therapy.
Improved but not 3 months
resolved
Continue intervention
Insufficient improvement assessed
systematically #
Consider for angiography with a view
to revascularisation
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 17Tier 2 review
Highlighted areas refer to potential Tier 2 / PwSI review
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 18Pwsi / Tier 2 Role within chest pain Pathway
Cardiology clinic / racpc
initial diagnostic investigations,
ETT, functional imaging, angiography,
CTA ,CMR
Revascularisation
Tier 2 / Pwsi
Optimise medical therapy Review by cardiologist
Cardiac Rehab menu
Smoking cessation and
lifestyle modification Medium / high risk patient Symptomatic despite optimal medical therapy
Further up titration and up titration - refer for functional
imaging / angiography
Up titration complete
symptoms stable (med/high risk) or
low risk patient Cardiology to revasc without Stable, titration complete
Tier 2 referral
Cardiology to Tier 2 referral
Remains symptomatic, further up titration
Remains symptomatic despite
Discharge to GP
optimal medical therapy
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 19INITIAL MANAGEMENT Managing the Individual with Angina Time is required for people to adjust to a new diagnosis. They need information about the condition, delivered in an accessible way. Their fears, concerns and expectations must be addressed. They need to come to terms with the diagnosis cognitively and emotionally. When nearing death their wishes need to be established and accommodated whenever possible. The ANGINA PLAN should be implemented, where feasible. Symptom relief should be achieved by using a combination of drugs as indicated in the Guidelines. The heart rate is important in managing symptoms as myocardial perfusion occurs during diastole, which in turn is longer with slow pulse. Aim for < 60 beats per minute (bpm) (1,2).
(3,4) Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 21
RETRIEVAL BACK TO PRIMARY CARE
Retrieval from Out-patient Follow-up to Primary Care
• The patient is stable and secondary or precipitating factors have been managed.
• Patient education has begun.
• An individual management plan has been made.
• The practice has demonstrated competence in angina management.
• If the practice is unable to manage the patient then discharge to a community clinic (led
by PwSI or nurse specialist) is appropriate.
Discharge after Acute Admission and On-going Follow-up
As with other pathways, after acute admission and the patient is discharged home or to a
nursing home, the following should be in place:
The acute Trust should inform the general practice or primary care clinician of the planned
discharge by phone or fax. They should provide a discharge summary and management
plan.
The GP or specialist nurse should contact the patient within 48 hours to assess on-going
needs and management plan. On-going management should include completing patient
education, including when and who to access when they begin to become unwell. This will
normally be during office hours. Out of office hours and at weekends the out of hours service
should be informed, and a management plan provided, especially near the end of life.
Competence
Competence will include knowledge of the pharmacological and other interventions that
improve prognosis, manage symptoms, and keep people out of hospital. The primary
clinician will also be aware of the psychological and emotional factors affecting patients with
newly diagnosed and on-going chronic disease, and their carers; be in a position to deliver
patient focused education about the condition, including self monitoring and when to call for
help; and be aware of the reasons for referral back to secondary/tertiary care. Establishing
competence will need to be done locally.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 22MANAGING THE POPULATION An assessment of quality of care should also be performed. The following are suggested: 1) The first requirement of effective population management is to have a validated register of people with a confirmed diagnosis. 2) Quantitative audit, using locally defined criteria should be conducted. 3) Significant event analysis of, for example, hospital admissions for Myocardial Infarction (MI)/ACS. 4) An audit of the effectiveness of discharge arrangements, from both from in-patient and out-patient care. 5) An assessment of patient satisfaction with their care, understanding of the condition and symptom control. Reference [1] Fox et al. Resting Heart Rate in Cardiovascular Disease. Journal of the American College of Cardiology. 2007: Vol. 50, No. 9. [2] Diaz A, Bourassa M, Guertin M, Tardif J. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease: European Heart Journal: 2005; 10.1093/eurheartj/ehi190. [3] Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS, Ferguson TB, Jr., Fihn SD, Fraker TD Jr., Gardin JM, O’Rourke RA, Pasternak RC, Williams SV. ACC/AHA 2002 Guideline update for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for the Management of Patients with Chronic Stable Angina). 2002. Available at www.acc.org/clinical/guidelines/stable/stable./pdf [4] Fourth Joint Task Force of the ESC and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. European Guidelines on cardiovascular disease prevention in clinical practice: European Heart Journal, 2007; 10.1093/eurheartj/ehm316. Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 23
The Primary Care Palpitations Pathway By Dr Washik Parkar, Dr Alan Fitchet, Dr Adam Fitzpatrick The Palpitations Pathway for Greater Manchester Background Palpitations are common and can be defined as an uncomfortable awareness of a heart rhythm. These can be normal as in exercise, stress, emotion or taking substances affecting sympathetic and parasympathetic activity. However they can point to a cardiac arrhythmia. Arrhythmias cause significant patient morbidity and anxiety. Rarely they can cause sudden death. Early diagnosis and risk stratification is key to management. 700,000 patients in England are affected by arrhythmias, the most common being AF. The prevalence of which is 1.2% of the general population but rising with age to affect 4% of those over 65 years and 10% of those over 80 years.1 Nationally each year there are 12,500 strokes directly attributable to AF and therefore potentially preventable.2 This pathway is designed to guide and support the role of the primary care physician or specialist nurse when a patient presents with symptoms suggestive of a primary cardiac arrhythmia. This pathway is designed to aid a generic workup for patients with palpitations, aid specific interventions for defined arrhythmias such as AF and define when specialist referral is indicated. It also provides education regarding aspects of secondary and tertiary care management. Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 24
PRIMARY CARE ASSESSMENT OF PALPITATIONS The majority of people will experience palpitations at some time. A palpitation is a subjective awareness of the heart beat. It can occur with awareness of sinus rhythm, extra systoles (ectopic beats), with abnormal bursts of rapid heart rhythms (tachycardias) or with an irregularity of the heart rhythm such as in AF. Approach to the patient with palpitations (see Table 1) The aim of this approach is to: 1) Ascertain the severity and frequency of the symptoms of palpitations to gauge the effect on the patient and the best method of recording an episode; and 2) Ascertain whether there is underlying structural, ischaemic or electrical heart disease which will determine prognosis and indicate additional conditions that might require treating. For example, infrequent unifocal ventricular ectopics in the setting of a normal 12-lead ECG and no other cardiac symptoms are likely to be benign whereas in the setting of say exertional chest pain or a family history of sudden death at a young age might represent underlying ischaemic heart disease or primary electrophysiological disease. For this reason a full cardiovascular history and examination is required in all patients. Particularly consideration should be given to factors that may trigger palpitations such as caffeine, alcohol and exercise. High risk features that would necessitate specialist referral should also be sought (see Table 2). Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 25
Palpitations
Haemodynamically unstable? (2)
Clinical Assessment (1)
(symptom burden and underlying
heart disease) Emergency A&E
12-lead ECG MANDATORY referral (obtain ECG if
possible)
High risk features? (3) YES
Specialist referral
NO
Obtain symptom ECG correlation
(4)
Ectopics (5)
AF Other
Ectopic Beats Go to AF
Tachycardias (6)
Confirmed or suspected Pathway
YES
ectopics
SVT
Atrial flutter
Atrial tachycardia
Abnormal ECG and/or
Ventricular tachycardia
evidence of structural heart
disease? Specialist referral
NO Specialist referral
Reassurance and advice
Reduce aggravating factors
Anxiety management
Beta-blocker if stress related
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 26Primary Care Palpitations Pathway Algorithm Notes (1) Primary Care Assessment (Table 1) History Frequency and duration? Provocation – exertion, stress, rest? Associated symptoms – chest pain, breathlessness, light-headedness, blackouts? Pre-existing heart condition? Family history of heart disease or sudden death? Examination Pulse rate and rhythm? Heart murmur? HF? Investigations 12-lead ECG mandatory – PR interval, Wolff Parkinson White (WPW) pattern, bundle branch block, epsilon waves, brugada pattern, QT interval…? Others Thyroid Function Tests (TFTS) Full Blood Count (FBC) Ambulatory ECG monitoring (according to symptom frequency) to achieve ‘symptom- ECG correlation’ Echocardiogram if murmur or structural heart disease suspected (e.g. HF, left bundle branch block (LBBB), Left Ventricular Hypertrophy (LVH) or Q-waves on ECG) (2) Haemodynamic Instability If patient is hypotensive, light-headed, has chest pain or is significantly short of breath, refer directly to A&E. (3) High Risk Features (Table 2) History of pre-syncope/syncope Exertional cardiac symptoms Pre-existing heart disease: • HF • Ischaemic heart disease • Valvular heart disease • Congenital heart disease FH of sudden cardiac death under the age of 40 years Evidence of structural heart disease Resting ECG abnormality* • Check for pre-excitation, LBBB, prolonged QT interval and Q waves • Excluding 10 heart block, RBBB (4) Symptom-ECG Correlation Obtaining an ECG recording at the time of symptoms of palpitations, so called ‘symptom- ECG correlation’ forms the mainstay of diagnosis. This can be extremely difficult if episodes are infrequent and short lived. It is important that the correct ambulatory ECG method is employed in order to maximise the chance of success. The choice of method depends on the frequency of symptoms and whether the individual would be able to activate a recording device should activation be necessary to make an ECG recording. Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 27
Ambulatory ECG Recording
Daily symptoms 24 – 48 hour ECG
Weekly symptoms 5 – 7 day ECG event recorders
Monthly symptoms Cardio memo ECG recorder – requires
application to skin during symptoms so little
use in very short lived palpitations and
disabling symptoms such as syncope
Infrequent symptoms and/or syncope Insertable loop recorders (ILR): implantable
devices with continuously looping memory.
Remain in situ for up to 3 years. Highly
effective at achieving symptom-ECG
correlation. Usually reserved for syncopal
patients and those where a high risk
arrhythmia is suspected but has not been
recorded using other methods
Diagnoses made from history and initial assessment that may remain in primary
care
A normal ECG with:
Normal heart rhythm
Patients may become abnormally aware of their normal heart rhythm. This may cause
increasing concern in individuals during period of stress in their lives, patients with
anxiety disorders or patients with a family history of premature CAD. This can typically
occur during the transition from awake to sleeping or following exertion or other causes
of increased sympathetic or catecholaminergic drive. In contrast to the paroxysmal
tachycardias although symptoms might be reported to come on suddenly they often
resolve gradually as opposed to abruptly and the circumstances surrounding the
episode are as described above. Patients with periodic abnormal awareness of a
normal heart rhythm should initially be reassured and managed conservatively.
(5) Ectopic Beats
Ectopics are premature beats arising either in the atria or ventricles. They are typically
described as an awareness of the heart skipping a beat, briefly stopping followed by a
thump or extra beats. This can occur irregularly or have a repetitive sequence (e.g.
bigeminy, trigeminy, etc) such that the patient is aware of an abnormal rhythm for
minutes or hours at a time. Symptoms vary considerably and are often exacerbated by
anxiety.
Ectopic beats are often benign but can be a marker of underlying heart disease.
If no features of underlying heart disease are suggested by history, examination and 12-
lead ECG then reassurance can be offered along with advice on alleviating
exacerbating factors such as caffeine containing drinks, stress and alcohol.
If drug treatment is required Beta-blockers can be useful when stress or exercise
precipitate the ectopic beats.
If ectopic beats remain poorly controlled and symptomatic or there is evidence of
underlying heart disease consider referring for specialist advice.
If high risk factors are present refer for specialist advice.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 28Atrial Fibrillation: Follow AF pathway. (6) Paroxysmal Regular Tachycardias Paroxysmal regular tachycardias are typically described as an abrupt onset of a rapid sustained heartbeat which persists for minutes or hours. Examples include atrioventricular nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT), atrial tachycardia, atrial flutter and ventricular tachycardia. Paroxysmal tachycardias typically terminate abruptly (unlike sinus tachycardia) and atrioventricular (AV) node dependent tachycardias may be terminated by vagal manoeuvres or adenosine administration. 12-lead ECG between episodes might show pre-excitation with a short PR interval, delta wave and prolonged QRS duration (WPW ECG pattern) and provide information on the potential cause. ECG-symptom correlation should be sought through 12-lead ECG and appropriate ambulatory ECG monitoring tailored to the frequency and duration of symptoms (see Symptom-ECG Correlation). As these tachycardias are potentially curable in the majority of cases, patients with a paroxysmal tachycardia should be referred for specialist cardiological opinion. If high risk factors are present refer for specialist advice even if nature of tachycardia is yet to be diagnosed. Atrial Flutter: Atrial flutter should always be considered in the presence of a regular steady heart rate of 150BPM. Atrial flutter is a regular arrhythmia usually arising from a macro reentrant circuit within the right atrium. The atria beat at 250 – 350 BPM with every 2nd, 3rd, 4th etc… beat being conducted to the ventricles. In typical cases the atrial rate is 300BPM (1 large square on the ECG) and 2:1 block at AV nodal level results in a ventricular rate of 150BPM. Often ‘saw tooth’ flutter waves are seen in the inferior ECG leads). Atrial flutter often occurs in the presence of structural heart disease namely atrial enlargement either due to intrinsic cardiac conditions or co-morbidities such as pulmonary disease, hypertension etc… An echocardiogram should be performed to assess this. The risk of thromboembolism is similar to AF and consideration for anticoagulation should be applied according to CHA 2 DS 2 VASc criteria3 (see AF pathway). Patients with atrial flutter, paroxysmal or persistent should be referred for specialist advice for consideration of cardioversion (if 1st episode) or radio frequency ablation therapy (if recurrent). Atrial flutter radio frequency ablation is safe and effective producing a cure in 90% of cases.4 Pre-excitation /WPW Syndrome: Pre-excitation of the ventricles occurs in the setting of an accessory electrical pathway between the atria and ventricles. This produces the typical ECG pattern of a short PR interval (less than 120ms or 3 small ECG squares), a delta wave (slurring of the start of the QRS complex) and a broad QRS complex (greater than 120ms). Historically this has been called WPW Pattern. The addition to this ECG pattern of paroxysmal tachycardias (due to AVRT) is described as WPW Syndrome. In a small proportion of WPW patients the accessory pathway can conduct at sufficiently high rates, for example during AF to cause ventricular arrhythmias and sudden cardiac death. Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 29
The accessory pathway is very amenable to radio frequency ablation with cure rates of
96 – 98%.4
All patients with WPW pattern ECG whether symptomatic or not should be referred to
an arrhythmia clinic for assessment and consideration for radio frequency ablation
therapy.
In the presence of syncope specialist referral must be made as an urgency.
Ventricular Tachycardia:
Patients with documented ventricular tachycardia (VT) should be referred urgently for
specialist advice.
Patients with suspected sustained VT should be referred routinely for specialist advice.
Patients with non-sustained VT should be referred routinely for specialist advice.
PRIMARY CARE MANAGEMENT OF ATRIAL FIBRILLATION
Much of AF management can be performed in primary care. However the physician
must be competent and confident in making a diagnosis with ECG confirmation,
pharmacological manipulation and risk assessment for stroke prevention.
AF is the most common sustained cardiac arrhythmia with a prevalence estimated at 1.2%
of the population. This increases with age being 4% in those aged over 65 rising to 10% in
those aged over 80.1 The most common underlying cause of AF is ischaemic heart disease.
Other risk factors include hypertension, valvular heart disease, alcohol excess,
Hyperthyroidism. Where there is no identifiable cause the term “Lone AF” is used.
AF accounts for 1% of the annual NHS budget.5
Atrial Flutter
Atrial flutter is distinct from AF in that it is difficult to treat with drugs, easy to cure with
ablation, but carries the same stroke risk as AF. Its management usually requires specialist
input.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 30ANTICOAGULATION AND STROKE RISK
AF is a major predisposing factor to stroke, with 12,500 strokes per year thought to be
directly attributable to AF.2 Strokes due to AF tend to be large with a high morbidity and
mortality.6,7
NHS Stroke Improvement Programme
It is a national priority to improve the detection of AF, its risk stratification for
thromboembolism and increase anticoagulation rates. Currently it is estimated that nearly
half (46%) of patients in primary care with AF who would benefit from anticoagulation are not
receiving it.
One group who are often prescribed aspirin rather than anticoagulation are the elderly
because of a perceived risk of increased bleeding in this age group. The BAFTA study
powerfully confirmed that warfarin is as safe as aspirin in a primary care population of over
75 years with a 50% reduction in all cause strokes including intracranial haemorrhage.9
NICE figures from 2006 indicated that 355,000 patients in the UK with AF were eligible for
anticoagulation and 166,000 of these were not getting it. This indicated that if all patients
identified as having AF and being in a high risk category for stroke were to be appropriately
anticoagulated, this could prevent up to 6,000 strokes and 4,000 deaths each year.2,9
PRIMARY CARE AF CASE FINDING
A key issue in reducing morbidity and mortality and morbidity in AF is early recognition and
active case finding. Primary care is well placed for call and recall particularly with its
registers of high risk patients namely those with CAD, HF, hypertension, and diabetes. It
also targets patients over 65 in its annual influenza vaccination clinics.
Possible case finding opportunities with annual manual pulse checks in the at risk population
include:10
• Patients attending annual chronic disease management clinics.
• Patients over 65 attending flu clinics.
• Patients attending the NHS Health Check (if extended to the over 65 year olds).
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 31THE GRASP AF 2 TOOL
Assessment of Risk in Patients already known to have AF
A database interrogation tool, GRASP-AF 2 (Guidance on Risk Assessment and Stroke
Prevention in AF) has been developed by the West Yorkshire Cardiac and Stroke Network to
aid the identification of patients already known to have AF who are at increased risk of
stroke and not anticoagulated. The programme is compatible with all major primary care
databases. It identifies patients with a READ code for AF and calculates their CHADS 2 (see
Appendix 1) score based on existing database information. It then identifies those patients
designated as at high risk with a CHADS 2 score of two or more who are not anticoagulated,
for case note review to assess individually whether that patient should be considered for
anticoagulation or whether there are specific contra-indications. This tool is freely available
to use through the NHS Improvement website at www.improvement.nhs.uk/graspaf/
(NB: This guidance will use the recently developed CHA 2 DS 2 -VASc scoring system as it is
more effective at accurately risk scoring those with a CHADS 2 score of 0 or 1 - low to
intermediate risk. It is hoped that the GRASP-AF 2 tool can be modified to adopt this scoring
system.)
THE AURICLE TOOL
Support in Decision to offer Anticoagulation
This is a web based programme devised for GPs by a GP. It is simple to use during a
consultation and provides instant relevant information and support to help in the difficult
decision to start warfarin in patients with AF. It combines the CHA 2 DS 2 -VASc scoring
system with sound advice from consultant specialists working both at a District General
Hospital (DGH) and at the Department of Health (DH). After registering, you simply click the
mouse on seven yes/no questions and add in the patient's date of birth. The programme
instantly works out the annual risk of thromboembolic stroke and this is returned in seconds
along with a few snippets of advice depending on the answers already given. This can then
be discussed with the patient in front of you and the option of electronic consultant advice
can be explored. At the click of the mouse the same pertinent patient details can be emailed
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 32to a local specialist. He/she will respond directly to you within a locally agreed timeframe and
give advice on warfarin depending both on the objective detail you have provided but also on
any relative contraindications you may have submitted at the bottom of the page in free
text.11
(NB: This guidance will use the recently developed CHA 2 DS 2 -VASc scoring system as it is
more effective at accurately risk scoring those with a CHADS 2 score of 0 or 1 - low to
intermediate risk. It is hoped that AURICLE tool can be modified to adopt this scoring
system.)
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 33Clinical Guidance for Irregular pulse?
Confirm AF with 12-lead ECG
Management of Atrial Fibrillation in
If sinus rhythm consider 24 hr ECG ?Paroxysmal AF
Primary Care
RATE OR RHYTHM CONTROL?
Consider rate control first for patients with persistent Consider rhythm control first for patients
AF: with persistent AF:
ANTI-COAGULATE? (CHA2DS2-VASc Guidance)
with HR >90 (>110 if recent onset of AF) (See CHA2DS2-VASc Score for absolute risk) (4) who are symptomatic
who are asymptomatic Adapted from: Lip et al (2010) The Euro Heart Survey on Atrial Fibrillation, Chest, vol 137(2)
who are younger
st
in whom antiarrhythmic drugs are C/I presenting for the 1 time with lone AF (2)
if unsuitable for cardioversion (1) with secondary AF (3)
Prescribe Beta Blockers
Bisoprolol 2.5-10mg OD
or rate limiting Calcium antagonist (avoid in LV
Dysfuntion
Verapamil 40-120 mg TDS or
Diltiazem (brand prescribed) dose based upon heart
rate/symptoms
If further rate control needed add Digoxin
OAC – Oral anticoagulation
Failure of rate control? – Inadequate control of
Anticoagulate If not for OAC consider aspirin
symptoms and/or heart rate
Target INR 2.5 (range 2-3) Assess CHA2DS2VASc risk yrly
Indications for AF ablation
C/I to see note (6)
anticoagulation (4) If treatment decision
prescribe aspirin complex
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 34
Refer for specialist advice
Paroxysmal AF or Atrial Flutter
(5)Primary Care Management of Atrial Fibrillation
These guidelines concern patients who have AF and are haemodynamically stable. If patient is
hypotensive, light-headed, has chest pain or is significantly short of breath, refer directly to A&E.
IDENTIFICATION AND DIAGNOSIS OF AF (READ CODE G573)
It is considered to be good practice to perform opportunistic manual pulse palpation in those
>65 years. It is essential in patients who present with:
• Breathlessness
• Dyspnoea
• Palpitations
• Syncope/dizziness
• Oedema
• Chest discomfort
It is equally important to ensure that the same opportunity is seized when monitoring
patients with:
• Hypertension
• Diabetes or
• existing Cardiovascular Disease
An ECG (READ code 3272) should be performed in ALL patients, whether symptomatic or not,
in whom AF is suspected because an irregular pulse has been detected.
Echocardiography – Most patients should have an echo, particularly if:
• You are considering “rhythm control”
• You suspect underlying structural or functional heart disease that would influence
management, such as choice of antiarrhythmic drug
• Help is needed with stratifying stroke risk for antithrombotic therapy, but only where
clinical evidence is needed for Left Ventricular (LV) dysfunction or valve disease
CLASSIFICATION OF AF
Paroxysmal AF (Recurrent) – Refer ALL cases to cardiology.
Terminates spontaneously within 7 days and usually < 48 hours. (Rhythm control)
Persistent AF (Recurrent)
Lasts >7 days, not self-terminating, requires electrical or pharmacological conversion to return
to sinus rhythm. (Rate or Rhythm control)
Permanent AF (Established)
No further cardioversion attempts on basis of clinical/echocardiographic features e.g. left atrium
>5.5cm, symptoms controlled with rate control. (Rate control)
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 35RATE V RHYTHM
Some patients with Persistent AF will satisfy criteria for either an initial rate-control or rhythm
control strategy i.e. age >65 but also symptomatic therefore:
• The indications for each option should not be regarded as mutually exclusive, and the
potential advantages and disadvantages of each strategy should be explained to patients
before agreeing which to adopt.
• Any co morbidities that might indicate one approach rather than the other should be taken
into account.
ALGORITHM NOTES
1) Patients unsuitable for cardioversion
Those with:
• Contraindications to anticoagulation.
• Structural heart disease that precludes long term maintenance of sinus rhythm. e.g. left
atrial size >5.5 cm.
• A long duration of AF.
• A history of multiple failed attempts at cardioversion and/or relapses.
• An ongoing but reversible cause of AF (e.g. thyrotoxicosis).
2) Lone AF
This is defined as AF without overt structural heart disease and is confirmed only if there is:
• No history of cardiovascular disease or hypertension.
• No abnormal cardiac signs on physical examination.
• A normal chest x-ray and, apart from the presence of AF, a normal ECG (i.e. no
indication of prior MI or LVH).
• Normal atria, valves and ventricular size and function by echocardiography.
3) Secondary AF
May be secondary to cardiac or non-cardiac conditions.
Cardiac Non-cardiac
Ischaemic Heart Disease Acute Infections especially Pneumonia
Valvular Heart Disease Electrolyte Depletion
Hypertension Lung Carcinoma
Sick Sinus Syndrome Pericardial Effusion
Cardiomyopathy Pulmonary Embolism
Thyrotoxicosis
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 364) CHA2 DS 2 -VASc Score Assessment of Thromboembolic Risk This recently developed scoring system endorsed by the European Society of cardiology is used to predict the risk of thromboembolic events according to clinical and echocardiographic parameters in patients with non-valvular AF1,2. CHA 2 DS 2 -VASc can either be used as a stand-alone scoring system as detailed in the algorithm or as an additional to CHADS 2 scheme to consider additional stroke risk. It has the advantage over CHADS 2 of accurately identifying those at low risk (score of 0) and places relatively few people in the ‘grey’ intermediate zone (score of 1.) Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 37
At time of press the GRASP-AF tool will not support this score.
CHA2 DS 2 -VASc Scoring System
Risk Factor Score
Congestive HF/LVSD 1
Hypertension 1
Age > 75 2
Diabetes mellitus 1
Stroke/TIA/Thromboembolism 2
Vascular disease (prev MI, PVD, aortic plaque) 1
Age 65 – 74 1
Sex 1
Female 1
Maximum Points 9
Note maximum points 9 as age can contribute 0,1 or 2
CHA2 DS 2 -VASc Score Patients (n = 7,329) Adjusted stroke rate
(% per year)
0 1 0%
1 422 1.3%
2 1,230 2.2%
3 1,730 3.2%
4 1,718 4.0%
5 1,159 6.7%
6 679 9.8%
7 294 9.6%
8 82 6.7%
9 14 15.2%
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk of stratification for predicting stroke and thromboembolism
in atrial fibrillation. Chest 2010;137:263-272
Lip GY, Frison L, Halperin J, Lane D. Identifying patients at risk of stroke despite anticoagulation. Stroke 2010;in press.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 38Approach to thromboprophylaxis using CHA2 DS 2 -VASc
CHA2 DS 2 -VASc Recommended
Risk category
Score antithrombotic therapy
One ‘major’ risk factor or
>2 ‘clinically relevant non- ≥2 OAC
major’ risk factors
Either OAC or aspirin 75–325
One ‘clinically relevant mg daily. Preferred: OAC
non-major’ risk factor 1 rather than aspirin. Requires
informed discussion with
patient
Either aspirin 75– 325 mg
daily or no antithrombotic
No risk factors 0 therapy. Preferred: no
antithrombotic therapy rather
than Aspirin
OAC – Oral anticoagulation
Risks/Benefits of Anticoagulation
Anticoagulation is often not prescribed because of perceived risks of bleeding counteracting
the benefits of thromboembolism prevention. Although there is no didactic substitute for
individual assessment the following offers guidance in common situations where
anticoagulation is perceived to confer too high risk:
• Age – The BAFTA13 study showed a significant benefit of anticoagulation over aspirin in
the over 75 year olds without a significant increased bleeding risk.
• Falls – Injurous falls but not unsteadiness or non-injurous falls should be regarded as a
contra-indication to anticoagulation.
• Peptic ulcer disease – is a contra-indication to anticoagulation only if active.
• Uncontrolled hypertension – Control first and reassess.
• Alcohol – Binge drinking can cause fluctuations in warfarin control but a constant level
of alcohol intake is unlikely to do so and should be recognised at anticoagulation checks.
• Compliance – Explore all avenues to aid compliance.
Greater Manchester and Cheshire Cardiac and Stroke Network Primary Care Pathways 39You can also read