CONTRACEPTION IUS AND INTRADERMAL IMPLANT - DAVID GLENN WEISMILLER, MD, SCM, FAAFP - EFMS ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Contraception
IUS and Intradermal Implant
David Glenn Weismiller, MD, ScM, FAAFP
Department of Family and Community Medicine
University of Nevada, Las Vegas School of Medicine
Disclosure Statement I have no relevant financial relationships to disclose that would in anyway create bias in the material I am presenting.
Learning Objectives
• Describe principles of patient selection regarding
contraceptives
• Discuss the indications/contraindications for
various contraceptive methods
• Appraise recommendations for use of long-
acting reversible contraceptives
3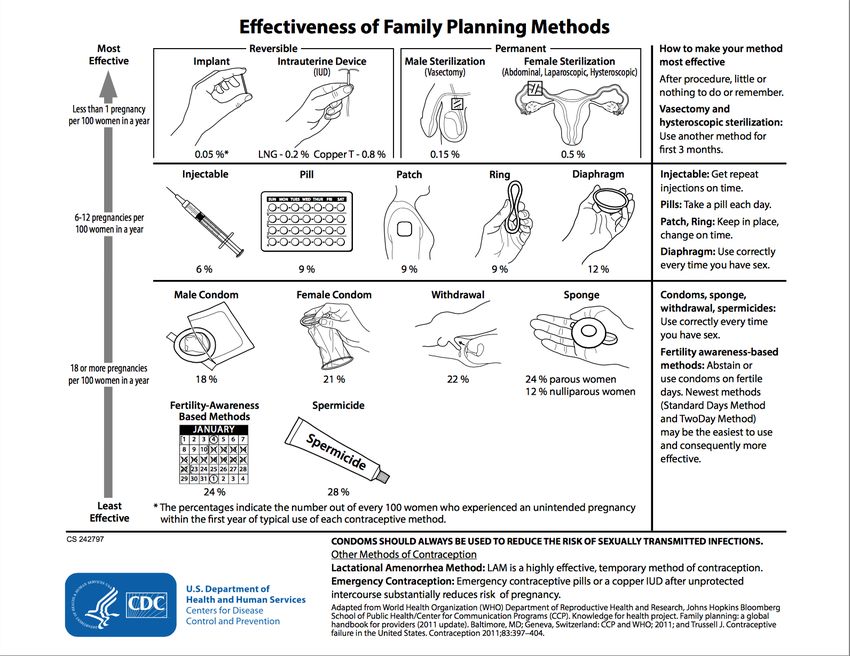
4
Helen tries out her new “Not-Tonight-Honey” nightgown 5
Why Contraception?
Families • 40% of US pregnancies (>2M)
complete are unintended
– In women ≥40y the
rate is 51%
– About a third of unintended
Unintended pregnancies occur in
pregnancies women who consider their
families complete
• Health Benefits
• Risk(s) of Pregnancy
Contraceptive Options
• Irreversible • Reversible
– Tubal ligation* – Oral contraceptives*
• Combined pills*
– Vasectomy
• Progestin-only pills
– Micro insert – Other hormonal options
• Abstinence • Implant
– Reasonable, acceptable • Injections
option; particularly in • Vaginal ring
younger patients • Patch
– Intrauterine Devices
– Intratube Device
l* Three most commonly used in US – Barrier methods
l Pregnancy poses a greater risk than any • Male condom*
contraceptive method
– Natural Family Planning
Principles
• All methods can fail
• Two methods are better than one
• Methods used wrong fail more
• Always need a backup plan
• No plan offers an 85% chance of getting
pregnant
8
9
Contraceptive Counseling
1. What are your contraceptive goals? Do you ever plan
to get pregnant? When?
2. Are you currently having sex with ♂ partner?
3. Have you tried any contraceptive methods? If so,
which one(s)?
4. What did you like/dislike about the method(s)?
5. Are you a good pill taker?
10Contraceptive Counseling
6. For user-controlled methods, how often did you forget to
use the method?
7. Are there any methods you have heard about and would
like to try?
8. How important is spontaneity of use?
9. Is protection from STIs important considering your life
situation?
10. Is cost an issue? Does your health insurance plan cover
any contraceptive method?
11Informed Consent
“BRAIDED”
• Benefits
• Risks
• Alternatives
• Inquiries
• Decision to change acceptable
• Explanation
• Documentation
12The Current State of IUDS in the USA
• 2012
– 10.3% of women using contraceptives (3,884,000 women)
– Used most by women –
• Aged 25-39
• Married and cohabitating
• Covered by Medicaid
• No religious affiliation
• Foreign-born women are three times as likely as U.S.-born women
to have ever used an IUD.
• Teenagers Guttmacher Institute Data, October 2015
– 3% https://www.guttmacher.org/fact-sheet/contraceptive-use-united-statesIUDs have been used in the U.S. for decades; safety controversy in the 1970s prompted the removal of all but one IUD from the U.S. market by 1986. First new generation IUD introduced to the U.S. market in 1988, following revised FDA safety and manufacturing requirements.
Types of IUDs
IUD (Copper) Available Years Use and FDA Approved Possible side effects
Since Effective
Copper (Paragard) 1988 10 • Approved only in parous • Abnormal menstrual
women, but available to all bleeding
women regardless of parity • Higher frequency or
• Can be used as Emergency intensity of
Contraception when inserted cramps/pain
within 5 days
IUD (Hormonal)
Mirena 2001 5 Approved only in parous women, • Inter-menstrual
but available to all women spotting in the early
regardless of parity months
Skyla (slightly smaller 2013 3 Approved for women regardless of • Reduces menstrual
than Mirena) parity blood loss significantly
• Hormone-related:
Liletta* 2015 3 Approved for women regardless of headaches, nausea,
parity breast tenderness,
Kyleena (lower 2016 5 Approved for women regardless of depression, cyst
hormone levels than parity formation.
Mirena)
*Actavis in conjunction with Medicines360, a non-profit women’s pharmaceutical company, developed Liletta specifically to be low cost and available to public
health clinics enrolled in the national 340B Drug Pricing Program, which provides reduced cost pharmaceuticals to providers that serve low-income populations.Intrauterine Contraceptives
Mechanisms of Action
Source:
Barr Pharmaceuticals, Inc.
Levonorgestrel-Releasing Intrauterine Copper-Releasing
System (LNG-IUS, Mirena® and Skyla®) Intrauterine Contraceptive
(ParaGard® T380A)
v Inhibits fertilization
v Inhibits fertilization
v Thickens cervical mucous
v Releases copper ions (Cu2+) that reduce
v Inhibits sperm function sperm motility
v Thins and suppresses the v May disrupt the normal division of oocytes and
endometrium the formation of fertilizable ova
Jonsson B, et al. Contraception. 1991;43:447-458; Videla-Rivero L, et al. Contraception. 1987;36:217-226; Kulier R, et al. Cochrane Database Syst Rev.
2006;3: CD005347.
17Considerations for IUDs
• IUD insertion, not IUD use, is associated with PID
– Cochrane
– Systematic Review (Grimes, Mohllajee)
– ACOG Practice Bulletin 2011
• DO NOT cause future infertility
• Nulliparas can use an IUD
– Uterus sounds to depth of a minimum 6 cm
• The USMEC guidelines state that the advantages of using the IUD in
adolescents generally outweigh the risks.
• Risk of uterine perforation
18Candidates for IUD Use
• Multiparous and nulliparous • Medical Conditions – may be
women at low risk for STI an optimal method
• Desire long-term reversible – Diabetes
contraception – Thromboembolism
– AUB/dysmenorrhea
– Breastfeeding
– Breast cancer
– Liver disease
19WHO Medical Eligibility Criteria for IUD Use in Women
with Certain Medical Conditions
TCu-380A LNG-IUS
WHO Risk WHO Risk
Medical Conditions
Category* Category*
Hypertension (controlled) 1 1
Multiple cardiovascular risk factors 1 2
History of DVT or pulmonary embolism 1 2
Stroke 1 2
Severe valvular heart disease (complicated) 2 2
HIV infection 2 2
AIDS (clinically well on antiretroviral therapy) 2 2
AIDS = acquired immunodeficiency syndrome; DVT = deep vein thrombosis; HIV = human immunodeficiency
virus; IUD = intrauterine device; LNG-IUS = levonorgestrel-releasing IUD; TCu-380A = copper-releasing IUD;
WHO = World Health Organization
*Category 1= there are no restrictions for use of the contraceptive method; Category 2 = the benefits of
using the contraceptive method generally outweigh the theoretical or proven risk
WHO. Medical Eligibility Criteria for Contraceptive Use. 3rd ed. 2004. Available at: http://www.who.int/reproductive-health/publications/mec/iuds.html.WHO Medical Eligibility Criteria for IUD Use in Women
with Certain Medical Conditions (cont’d)
TCu-380A LNG-IUS
Medical Condition WHO Risk WHO Risk
Category* Category*
Known thrombogenic mutations 1 2
Migraines with aura 1 2
Epilepsy 1 1
Diabetes 1 2
Obesity 1 1
Thyroid disorders 1 1
Viral hepatitis (active infection) 1 3
Viral Hepatitis (carrier) 1 1
IUD = intrauterine device; LNG-IUS = levonorgestrel-releasing IUD; TCu-380A = copper-releasing IUD;
WHO = World Health Organization
* Category 1= there are no restrictions for use of the contraceptive method; Category 2 = the benefits of
using the contraceptive method generally outweigh the theoretical or proven risk; Category 3 = the risks
of using the method usually outweigh the benefits
WHO. Medical Eligibility Criteria for Contraceptive Use. 3rd ed. 2004. Available at: http://www.who.int/reproductive-health/publications/mec/iuds.html.Medical Contraindications for
Intrauterine Contraceptive Use
• Pregnancy
• Immediately after puerperal sepsis or a septic abortion
• Undiagnosed abnormal vaginal bleeding
• Malignancy of the genital tract
• Known anomalies or fibroids that significantly distort the uterine cavity in a
way that is incompatible with IUD insertion
• Current pelvic inflammatory disease
• Current purulent cervicitis, chlamydial infection, or gonorrhea
• Allergy to any component of an IUD or Wilson's disease (for copper-
containing IUDs)
• Known pelvic tuberculosis WHO. Medical Eligibility Criteria for Contraceptive Use. 3rd ed. 2004; FFPRHC Guidance (April 2004). J Fam Plann
Reprod Health Care. 2004;30:99-108; FFPRHC Guidance (January 2004). J Fam Plann Reprod Health Care.
2004;30:29-41; Angle MA, et al. Stud Fam Plann. 1993;24:125-131.Patient Education and Consent
• Failure Rate (Effectiveness)
– ParaGard 0.6-0.8%
– Levonorgestrel 0.2%
• Reversibility (Median time to planned pregnancy)
– ParaGard 3 months
– Levonorgestrel 2-6 months
Failure Rate
• Pregnancy Rate Method Typical use Perfect use
– 82% one year after device removal Combined OCP 9% 0.3%
– 89% two years after device removal Tubal Ligation 0.5% 0.15%
Male condom 18% 2%
Depo-Provera 6% 0.3%
23Levonorgestrel-Releasing Intrauterine System: Different
Patterns of Menstrual Bleeding*
Type of Copper Intrauterine Levonorgestrel
Menstrual Device Intrauterine System
Bleeding Cycle 1 Cycle 4 Cycle 1 Cycle 4
Amenorrhea 0% 2% 0% 16%
Infrequent bleeding 2% 2% 11% 57%
Frequent bleeding 19% 0% 13% 1%
Prolonged bleeding 24% 0% 22% 3%
Irregular bleeding 17% 20% 67% 19%
*Percentage of subjects meeting criteria for different patterns of bleeding during
a specified 90-day cycle.
24
Suvisaari J, Lahteenmaki P. Contraception. 1996;54:201-208; Luukkainen T, et al. Semin Reprod Med. 2001;19:355-363.Intrauterine Contraceptives Do Not Increase the Risk of
Ectopic Pregnancy
• A 2-year, 7-center, randomized trial (N=2,244) compared the levonorgestrel-
releasing (LNg20) and the copper-releasing (Model TCu380Ag) intrauterine
contraceptive devices (IUDs)
– No ectopic pregnancies were found
• A collaborative multicenter, case-controlled study compared women who had a
history of ectopic pregnancy (n=615) with those who did not (n=3,453)
– Women who had never used an IUD were equally likely to have had an
ectopic pregnancy as were IUD users
– IUD users were less likely to have had an ectopic pregnancy than were
women who were not currently using contraceptives
Sivin I, et al. Contraception. 1987;35:245-255;
Ory HW. Obstet. Gynecol. 1981;57:137-144.
25Intrauterine Contraceptives
Noncontraceptive Benefits
• Intrauterine contraceptives decrease the risk for endometrial
cancer
• The levonorgestrel-releasing intrauterine system (LNG-IUS)
can be used as a first-line option to treat menorrhagia
– May be used in the presence of fibroids, unless they significantly distort or enlarge the
uterine cavity
– Produces a 97% decrease in menstrual blood loss
– In a retrospective study, 80% of women who were prescribed the LNG-IUS for
menorrhagia chose not to undergo a hysterectomy, as opposed to 9% of women who
received normal care for the condition
Hubacher D, Grimes DA. Obstet Gynecol Survey. 2002;57:120-128; Castellsague X, et al.
Int J Cancer. 1993;54:911-916.Some other recommendations…
• IUD may be offered to women with a history of ectopic pregnancy
• Levonorgestrel system may be an acceptable alternative to
hysterectomy in women with AUB-O
• FDA recommends that IUDs be removed from pregnant women when
possible without an invasive procedure
• Remove in menopausal woman
• Counseling should include information about risk factors for STIs and
PID
-ACOG Practice Bulletin No. 59, IUD Obstet Gynecol 2005;105:223-232
- Rauramo I.et al. Obstet Gynecol 2004; 104:1314-21.
27Intrauterine Contraceptives
Management of Cramping and Bleeding
• If a patient has severe or prolonged cramping:
– Examine for partial IUD expulsion, uterine perforation, or pelvic inflammatory disease
and treat if necessary
– Remove the IUD if the severe cramping is unrelated to menses or is
unacceptable to the patient
– If symptoms are mild, they can be treated with nonsteroidal anti-
inflammatory drugs (NSAIDs)
• Heavy bleeding for more than 3 months:
– Examine the patient for infection, fibroids, or signs of anemia and treat if necessary
– Prescribe NSAIDs
– Remove the device if there is a medical contraindication or if the bleeding is
unacceptable to the patient
28Intrauterine Contraceptives
Management of Infections
• Symptoms
– Fever, chills, unusual vaginal discharge
– Severe bleeding or abdominal cramping occurring 3 to 5 days after insertion
– Pain during intercourse
• If a sexually transmitted infection (STI) is diagnosed:
– Treat the infection
– Counsel the patient about how to prevent transmission of the STI
– Removal of intrauterine contraceptive (IUD) is not necessary
• If pelvic inflammatory disease is diagnosed:
– Treat the infection
– Remove the IUD only if symptoms fail to improve within 72 hours of after treatment
begins Penney G, et al. J Fam Plann Reprod Health Care. 2004;30:29-41; WHO. Selected Practice
Recommendations for Contraceptive Use. 2002; Grimes D. Lancet. 2000;356:1013-1019.
29Intrauterine Contraceptives
Management of Perforation during Insertion
• If uterine perforation occurs at the time of
insertion:
– Remove the device
– Provide alternative contraception
– Monitor for excessive bleeding
– Follow up as appropriate
– Insert another device after next menses if desired
by patientIntrauterine Contraceptives
Management of Missing Strings
• May be the result of partial or complete expulsion of
the device or perforation of the uterus
– Rule out pregnancy
– Probe for strings in cervical canal
– Obtain ultrasound or x-ray, as needed
– Remove promptly if found outside the uterine cavity, and
advise patient she is no longer protected
– Prescribe back-up contraceptive method, if necessary
Speroff L, Darney PD. A clinical guide for contraception. 3rd ed. 2001;
Ben-Rafael Z, Bider D. Obstet Gynecol. 1996;87:785–786. 31Intrauterine Contraceptives ions
• Partial or unnoticed expulsion may present as irregular bleeding and/or
pregnancy
• Risk of expulsion related to:
– Healthcare provider’s skill at fundal placement
– Age and parity of woman
– Time since insertion
– Timing of insertion (e.g., expulsion risk is greater following a second-trimester
abortion than a first-trimester abortion)
WHO. In: Medical Eligibility Criteria for Contraceptive Use. 3rd ed. Available at: http://www.who.int/reproductive-
health/publications/mec/iuds.html.
32Billing and Coding
Contraception Code Cost of Billing amount Other Billing Billing Charge with
Device for Requirements Insertion or
Contraceptive Administration Fee
Mirena J7298 $468.71 $708.00 Bill w/ IUD insertion $1,076.00
58300/$368.00
Skylar J7301
Paragard T380-A J7300 $392.00 $431.00 Bill w/ IUD insertion $799.00
58300/$368.00
ICD-10-CM Diagnostic Codes:
Z30.430 Encounter for contraceptive management; insertion of
intrauterine contraceptive device
V30.43(_) Intrauterine contraceptive device; checking (1), reinsertion (3), or
removal of intrauterine device(2)
Z31.01 Screening pregnancy test (+)
Z32.02 Screening pregnancy test (-)
33Patient Education and Consent
Adverse
Advantages
effects/disadvantages
IUD Long term, no patient Rare uterine perforation; risk
compliance required; rapid of infection with insertion
return of fertility after removal
Paragard T380-A FDA approved for up to10 Irregular/heavy bleeding and
years; (shown to be effective dysmenorrhea
for up to 12 years)
Mirena (LNG-IUs) Decreased bleeding and Irregular bleeding initially,
dysmenorrhea; followed by amenorrhea
FDA approved for up to 5 (reported in about 20% of
years; (shown to be effective users after 1 year of use);
for up to 7 years) ovarian cysts
34So how does choice impact lactation?
nLAM n IUD n Progestin-only nCombined pill
nAbstinence/ n Copper nPills nPatch
Sterilization nInjectables
Periodic n nRing
Abstinence/ nImplants nInjectable
NFP Methods nLevonorgestrel
nBarrier Methods IUD
No known impact Little to no Some reports of Expected to
on lactation known impact negative impact on have negative
on lactation lactation impact on
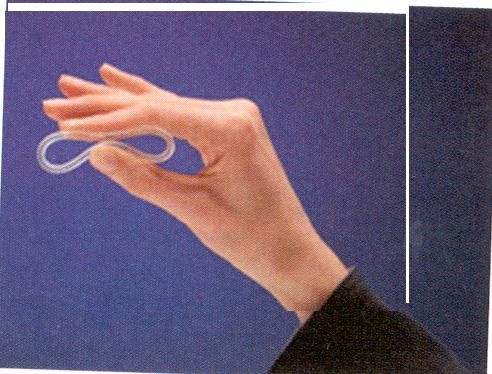
lactationTechniques for Insertion
• Copper T-380A
• Levonorgestrel (Mirena, Skylar)
• AHA Guidelines for Prophylaxis for Endocarditis
36Insertion of an Intrauterine
Contraceptive Device
• Use the proper insertion technique for
each device to decrease the risk of
uterine perforation and expulsion
• Use a sterile technique to reduce the
risk of infection
– Antibiotic prophylaxis does not
prevent infection at time of device
insertion
Johnson BA. Am Fam Physician. 2005;71:95-102
Oloto EJ, et al. Br J Fam Plann. 1997;22:177–180;
Hubacher D, et al. Am J Obstet Gynecol. 2006 Nov;195(5):1272-1277.
37When to Insert an Intrauterine Contraceptive?
• Any time during menstrual cycle
• Any other time during a woman’s cycle if:
o She used appropriate contraception
o She was not sexually active, or
o Her pregnancy test was negative
• Any time after a pregnancy, a spontaneous abortion, a
miscarriage, or an induced abortion if a woman has not
engaged in unprotected intercourse
WHO. Medical Eligibility Criteria for Contraceptive Use. 3rd ed. 2004; FFPRHC Guidance (April 2004). J Fam Plann Reprod
Health Care. 2004;30:99-108; FFPRHC Guidance (January 2004). J Fam Plann Reprod Health Care. 2004;30:29-41.Use of misoprostol before insertion?
• A 2007 study suggested that the use of misoprostol (Cytotec)
before IUD insertion allowed for easier insertion.
• However, more recent studies show no benefit and increased
side effects with misoprostol.
• The American College of Obstetricians and Gynecologists
makes no recommendation regarding the use of misoprostol
before IUD insertion.
• Edelman AB, Schaefer E, Olson A, et al. Effects of prophylactic misoprostol administration prior to intrauterine device insertion in
nulliparous women. Contraception. 2011;84(3):234-239.
• Espey E, Singh RH, Leeman L, Ogburn T, Fowler K, Greene H. Misoprostol for intrauterine device insertion in nulliparous women: a
randomized controlled trial [published ahead of print November 8, 2013]. Am J Obstet Gynecol.
http://www.sciencedirect.com/science/article/pii/ S0002937813020176
39Guidelines for IUDs
Organization Recommendation
ACOG 2007 Asymptomatic women may use an IUD within 3 months of treated pelvic
infection or septic abortion.
ACOG 2007 All adolescents should be screened for GC and chlamydia prior to
insertion.
Cochrane 2007 No benefit from doxycycline or azithromycin prior to insertion.
CDC 2010 Evidence is insufficient to recommend the removal of IUDs in
women diagnosed with acute PID. However, caution should be
exercised if the IUD remains in place, and close clinical follow-up is
mandatory. The rate of treatment failure and recurrent PID in women
continuing to use an IUD is unknown, and no data have been
collected regarding treatment outcomes by type of IUD (eg, copper
or levonorgestrel).
40Key Recommendations for Practice
Clinical Recommendation Evidence Rating
Nulliparous women and adolescents can be offered an IUD, although the 20-mcg per 24
hours levonorgestrel-releasing IUD (Mirena) is not approved by the U.S. Food and Drug C
Administration for use in nulliparous women
Women who are at high risk of STIs but have no active signs or symptoms of genital tract STI
should be tested for STIs at the time of IUD insertion. Insertion of the IUD may occur on the
same day as STI testing, without waiting for test results. If results are subsequently found to be
C
positive, treatment can be administered at that time and the IUD left in place.
For women with a known STI that causes cervical infection, it is recommended that IUD
insertion be delayed for at least three months after resolution of the infection.
C
Prophylactic antibiotics should not routinely be administered before IUD insertion. Antibiotic
prophylaxis does not have a major effect on reducing the risk of pelvic infection, and does not B
alter the need for IUD removal in the months after insertion.
Misoprostol (Cytotec) should not be administered before IUD insertion. Although an
earlier study showed easier insertion with misoprostol, subsequent studies showed no B
benefit and increased side effects.
If a woman with an IUD becomes pregnant, the IUD should be removed. C
41Intradermal Implant
Hormonal (Progestin-only) Method
• Single-rod implant (4 cm in length and 2 mm in diameter)
made of ethylene vinyl acetate and contains 68 mg of
etonogestrel
• Duration of use: 3 years
• 2012 – 1.3% (492,000 women) of contraceptive users*
*https://www.guttmacher.org/fact-sheet/contraceptive-use-united-statesImplantable Hormonal Devices
• Single rod, subdermal implantation.
• 68 mg of etonogestrel – period of up to three years Merck
– Heavier women may need a new implant every two years
• Since 1998 – > 3.5 million women (30 countries)
• Side Effects: Irregular bleeding
– HA, acne, dysmenorrhea, emotional lability
– NO significant side effect on BMD or lipid metabolismContraceptive Implant
Mechanisms of Action
• Suppresses ovulation
– Occurs within 1 day of insertion
– Ovulation inCommon Myths About Contraceptive
Implants Among Clinicians
• Insertion and removal is time-consuming and difficult to learn –
Not true!
– Time to insert is 1.1 minutes
– Time to remove is 2.6 minutes
• Implants are associated with a higher risk of ectopic pregnancy –
Not true!
– No pregnancies were reported during 5,629 woman-years of use
– The baseline ectopic pregnancy rate in the United States is 1.97%
Mascarenhas L. Eur J Contracept Reprod Health Care. 2000;5 Suppl 2:29-34; Glasier A. Contraception.
2002;65:29-37; Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 1995;44:46-48.
45Contraceptive Implant:
A 2-year study investigated the efficacy and tolerability of IMPLANONTM (N=330)
• Reasons for discontinuing participation in the study:
– Irregular bleeding: 13%
• Bleeding patterns were studied for reference periods of 90 days. The average number of bleeding or
spotting days was 17.7 every 90 days.
• Bleeding patterns that occur with IMPLANON are unpredictable and may include changes in frequency or
duration. Amenorrhea also occurs among some women. Change in the frequency or duration of bleeding is
the most common reason women discontinue IMPLANON treatment.
– Other adverse events: 23%
• Emotional lability: 14.2%
• Headache: 12.7%
• Weight gain: 12.1%
• Dysmenorrhea: 9.7%
• Depression: 7.3%
The IMPLANON US Study Group. Contraception. 2005;71:319-326.Contraceptive Implant
Funk S, et al. Contraception. 2005;71:319-326.
Noncontraceptive Benefits
Changes in Acne (n=315) Changes in Dysmenorrhea
(n=315)
Percentage change from baseline
70% 50%
60%
40%
50%
40% 30%
30%
20%
20%
10%
10%
0% 0%
Decrease No Increase No
Change Decrease Increase
Change
47Contraceptive Implantht Change
• In clinical trials, the mean cumulative weight gain was:
– End of first year: +2.8 lbs.
– End of second year: +3.7 lbs.
– Weight gain was the reason given for discontinuation of participation
by 2.3% of subjects
• In one study, 12.7% of participants reported weight gain as
an adverse event
– The majority of these adverse events were found to be related to the
study medication
The IMPLANON US Study Group. Contraception. 2005;71:319-326.
48Contraceptive Implant
• Effect
An on Bone
open, prospective, Mineral
comparative Density
two-year study of a
single-rod implant (n=44) vs. a nonhormonal intrauterine
device (n=29) found:
– Essentially similar changes in bone mineral density from baseline
– No relationship between 17β-estradiol concentrations and
changes in bone mineral density
Beerthuizen R, et al. Hum Reprod. 2000;15:118-122.
49Contraceptive Implant
•
Administration IMPLANON™ [physician insert]. 2006
If no hormonal contraceptive has been used in past month:
– Insert within 5 days of initiation of menses
• If switching from combination contraceptives, insert within
7 days of last active tablet, or during the ring-free or patch-
free period
• If switching from a progestin-only method:
– Any day if using the progestin-only pill
– Same day as intrauterine device or implant removal
– On due date for next contraceptive injection
50Contraceptive Implant
Quick Start*
• If using Quick Start to insert the implant:
– It may be inserted any time during the menstrual cycle
– Determine risk for pregnancy
• Perform pregnancy test, if indicated
• Provide emergency contraception, if indicated
• Recommend nonhormonal contraception for 7 days
*This method deviates from the manufacturers recommendations for timing of insertion and
is considered a non-FDA approved use.
51Complications Insertion
• Discomfort at insertion site
• Bleeding
• Infection
52Patient Education and Consent
• Cost $524.34
– per month over 3 years ($ 14.57)
• Failure Rate 0.05%
• Very convenient
• Adverse effects/Disadvantages
– Irregular bleeding ( as with other progestin-based methods
– Removal issues Failure Rate
Method Typical use Perfect use
Combined OCP 9% 0.3%
Tubal Ligation 0.5% 0.5%
Male condom 18% 2%
Depo-Provera 6% 0.3%
53Risks to Lactation
• May decrease milk supply if initiated before milk supply is
well established
• Anecdotal reports of immediate negative impact even
when initiated after lactation is well established
• Progestin IUD typically has MINIMAL impact
– Potential to have the same impact as other progestin-only
methods
54So how does choice impact lactation?
nLAM n IUD n Progestin-only nCombined pill
nAbstinence/ n Copper nPills nPatch
Periodic n Sterilization nInjectables nRing
Abstinence/NFP nImplant nInjectable
Methods nLevonorgestrel IUD
nBarrier Methods
No known impact Little to no known Some reports of negative Expected to have
on lactation impact on lactation impact on lactation negative impact on
lactationCoding and Billing
Contraception Code Cost of Billing amount for Other Billing Billing Charge with
Device Contraceptive Requirements Insertion or
Administration Fee
Nexplanon J7307 $566.93 $914.00 Bill w/ Insertion $1,215.00
Capsule
11981/$301.00
Depo J1055 $23.17 per $85.50 per dose; Bill w/ $128.50 per dose;
Injection dose; $342.00 per year administration $514.00 per year
(DMPA)* q $92.68 per 90772/$43.00
12 weeks year
ICD-10-CM Diagnostic Codes:
Z30.49 Nexplanon, unspecified birth control
Z31.01 Screening pregnancy test (+)
Z31.02 Screening pregnancy test (-) * DMPA for comparison
56So what might we say about
hormonal contraception…
• Given the high level of anecdotal reports of the association of
hormonal contraception (including progestin-only) with milk supply
– discourage where there is
– A young infant: < six weeks for progestin-only, < 6 months for combined
– Existing low milk supply or history of lactation failure
– History of breast surgery
– Multiple birth
– Preterm birth
– Compromised health of mother and/or baby
571 – No restriction
WHO Medical Eligibility Criteria 2 – Generally use
3 – Not usually recommended
4 – Not to be used
Duration of BF Progestin- Progestin- Progestin- Combined Combined Low dose
method only pills only depots only injectable patch or combined
implants/ contracep- ring
IUD tives
< 6 weeks PP
3 3 3 4 4 4
> 6 w to < 6 m
PP (primarily
1 1 1 3 3 3
breastfeed)
> 6 m PP
1 1 1 2 2 2ACOG
Breastfeeding: Maternal and Infant Aspects Committee Opinion
• All family planning choices are available to the postpartum lactating
woman.
• Choice and clinical ramifications merit additional counseling.
• Support women in choosing breastfeeding
– Accurate information
– Problems arise
• Early discussion of contraception and follow-up
– Options to be explained in detail
– Nonhormonal methods
– Hormonal Methods
– Lactational Amenorrhea Method
59Progestin vs. Combined OCP and Lactation
Espey et al. Obstet Gynecol 2012;119(1):5-13
Objective: Estimate the effect of progestin-only
compared with combined hormonal contraceptive pills on
rates of breastfeeding continuation in postpartum women
Results: No difference in breastfeeding continuation
rates, contraceptive continuation, and infant growth
parameters at 8 weeks
Conclusion: Choice of combined hormonal or progestin-
only contraceptive pills administered 2 weeks postpartum
did not adversely affect breastfeeding continuation.
60Contraceptive Implant
Summary
• One option available in the United States
• Easy and quick to insert and remove
• Efficacy equivalent to sterilization
• Safe and rapidly reversible
• Irregular bleeding patterns may be a problem for some patients
• Majority of reproductive-age women are candidates, including
adolescents
• Appropriate option for those preferring a long-term progestin-only
method and do not want injections or an intrauterine device
61Strategies to Reduce Barriers and Increase Use of
Implants and IUDS
• Encourage implants and IUDS for all appropriate
candidates – including nulliparous women and
adolescents
• Adopt same-day insertion protocols
– Screening for chlamydia, gonorrhea, and cervical dysplasia SHOULD
NOT be required before implant or IUD insertion, but may be obtained on
the day of insertion, if indicated
ACOG Committee Opinion No. 450. Increasing use of Contraceptive Implants and Intrauterine Devices to Reduce Unintended
Pregnancy. Obstet Gynecol. 2009;114(6):1434-1438Progestin-Only Methods More Appropriate
Than Combined
ACOG 2006
• Smoking or obesity AND over age 35 [SOR B, A; respectively]
• Hypertension with vascular disease or > age 35 [SOR B]
• Lupus with vascular disease, nephritis [SOR A]
• Migraine with focal aura [SOR B]
• Current or personal history of VTE associated with pregnancy
or estrogen unless on anticoagulation [SOR A]
• Coronary artery/cerebrovascular disease [SOR C]Management of Unscheduled Bleeding in Women
Using Contraception
Contraceptive Preferred Treatment
DMPA • Expectant management
• 7-14 days oral estrogen (1.25 mg conjugated estrogen or 2
mg micronized estradiol
• Transdermal patch (0.1 mg estradiol/24 h)
• 10-20 days of low-dose combined OCP
Etonogestrel implant • Expectant management
• Low-dose combined OCP for 10-20 days (not studied)
• NSAID for 5-7 days
Progestin pills • Take at same time each day and minimize missed doses.
Levonorgestrel IUD • NSAID for 5-7 days (eg, ibuprofen 400 mg, naproxen 250 mg,
or mefanamic acid 500 mg TID)
Edelman A and Kaneshiro B. Management of unscheduled bleeding in women using contraception. www.uptodate.com, 2017.Contraception and Adolescents
• Adolescents are capable of understanding
complex messages that include support for
abstinence, but also provide appropriate
information about sexual activity and
contraception
• It’s a conversation…at any age
65Cavazos-Rehg PA, et. al. Age of sexual debut among US adolescents. doi:10.1016/j.contraception.2009.02.014
Age of Sexual Debut
Kaplan–Meier curves: probability of surviving free of sexual debut, according to race and
gender.Abstinence • Convey to adolescents that this is expected, be realistic • Abstinence teaching programs have some success • Encouragement to practice abstinence can be a powerful tool to enhance empowerment for self care • Advantages: no STDs, no cost, no pregnancy • Disadvantages: difficult to maintain
Sexual Abstinence
• Educational programs that teach BOTH abstinence and
contraception
– Delay onset of sexual activity and reduce number of sexual
partners
• Ancheta et al. J Pediatr Adolesc Gynecol 2005;18.
• “Pledge” to remain abstinent: 50% honor pledge 12
months later
– STIs same whether pledgers or non-pledgers
• Rosenbaum et al. Am J Public Health. 2006;96Best Practice Recommendations
• Clinicians should consider a tiered approach to contraceptive counseling, whereby the most
effective and appropriate options are presented before less effective options.
• Requiring prerequisite preventive services, such as cervical cytology; breast examination; or
evaluation for sexually transmitted infections, diabetes mellitus, dyslipidemia, liver disease,
or thrombophilia, can introduce unnecessary barriers to contraceptive care.
• Family planning services should be offered to adolescents with assurances of confidentiality,
in the context of relevant law.
• Intrauterine devices and contraceptive implants are safe and effective for postmenarchal
adolescents and adults.
• The most common side effect of a progesterone only contaceptive (regardless of the the
vehicle) is irregular bleeding,
• Evidence is insufficient to recommend the removal of IUDs in women diagnosed with acute
PID.Thank You 70
References
1. ACOG Practice Bulletin 121. Long-Acting Reversible Contraception: Implants and Intrauterine
Devices. Obstet Gynecol 2011;118:184-195. (Reaffirmed 2015)
2. ACOG Practice Bulletin 152. Emergency Contraception. Obstet Gynecol 2015;126:e1-11.
3. Smoley BA, Robinson CM. Natural Family Planning. Am Fam Physician. 2012;86(10):924-928.
4. Hardeman J and Weiss BD. Intrauterine Devices: An Update. Am Fam Physician
2014;89(6):445-450.
5. Centers for Disease Control and Prevention. U.S. Medical eligibility criteria for contraceptive
use, 2010. MMWR Recomm Rep. 2010;59(RR-4):1-86.
6. Klein DA, Arnold JJ and Reese ES. Provision of Contraception: Key Recommendations from
the CDC. Am Fam Physician. 2015;91(9):625-633.
7. US Medical Eligibility Criteria (USMEC) for Contraceptive Use, 2016.
https://www.cdc.gov/reproductivehealth/contraception/usmec.htm
72You can also read