COVID-19 Current epidemiologic assessment of the pandemic - Updated on 20 May 2020 - NFP.com
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVID-19
Current epidemiologic
assessment of the
pandemic
Updated on 20 May 2020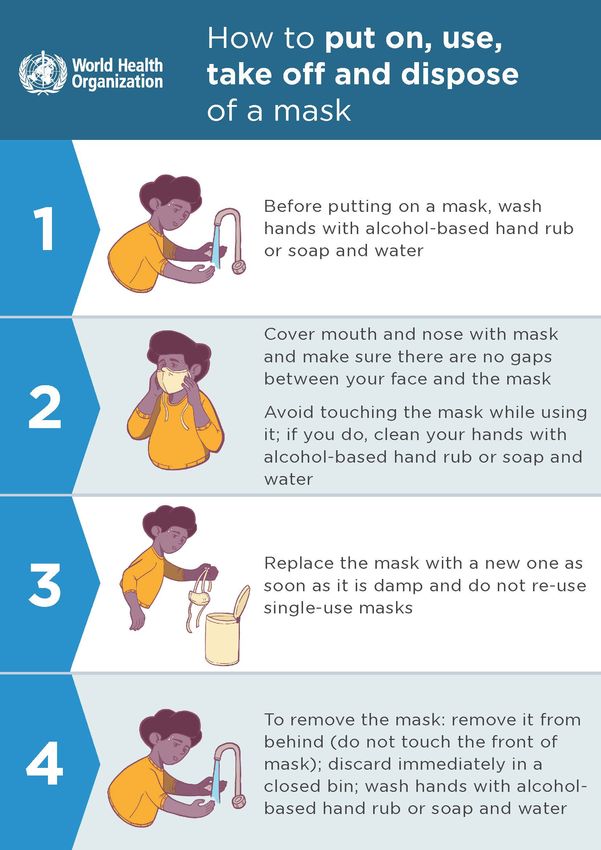
TABLE OF CONTENTS COVID-19 DIAGNOSIS, TESTING AND
TREATMENT 29
KEY MESSAGES & HIGHLIGHTS 3 How is a COVID-19 case defined? 29
Selection of the population to test 29
CONTEXT OF COVID-19 4
Undocumented infections 30
EPIDEMIOLOGICAL
CHARACTERISTICS OF COVID-19 15 DEEP DIVE - Diagnostic testing for
COVID-19 31
The mortality rate of the disease: the
case fatality rate (CFR) 15 DEEP DIVE - Investigational Drugs For
Covid-19 35
Covid-19 Clinical evolution and
frequency 177 DEEP DIVE - Vaccines For Covid-19 37
Ways of COVID-19 transmission 17
DEEP DIVE - Analyzing the efficiency of
RISK FACTORS, SEQUALAE AND
masks to fight COVID-19 19
INDIRECT EFFECTS 40
Factors for COVID-19 infection 40
WHO Advanced Analytics and
Mathematical Modelling 22 Factors for COVID-19 deaths 43
INTERVIEW: Understanding how Complications & sequalae 49
immunity against COVID-19 works 23 Indirect effects of COVID-19 52
DEEP DIVE – Gastroentorology,
Hepatology and COVID-19 27
SOURCES, BIBLIOGRAPHY AND
DEEP DIVE – Kawasaki Disease and APPENDICES 58
COVID-19 28
This document is a collective work of SCOR Global Life’s
Knowledge Community. List of main contributors:
Dr. Gabriela Buffet, Xiao Gao, Manuel Plisson, Marius Pascariu,
Pierre Gilloury, Xuefeng Xu, Dr. Pierre Sabouret, Dr. Eric Raymond, Odile Koehren
Dr. Dominique Lannes, Dr. Marinos Fysekidis, Dr. Richard Braun, Lars Pralle
DISCLAIMER
The information provided in this presentation represents only
SCOR’s view as of May 20th 2020 and does in no way whatsoever
constitute legal, accounting, tax or other professional advice by
SCOR SE (“SCOR”). While SCOR has endeavoured to include in this
presentation information it believes to be reliable, complete and
up-to-date, the company does not make any representation or
warranty, express or implied, as to the accuracy, completeness or
updated status of such information.
Therefore, in no case whatsoever will SCOR be liable to anyone for
any decision made or action taken in conjunction with the
information in this presentation or for any related damages.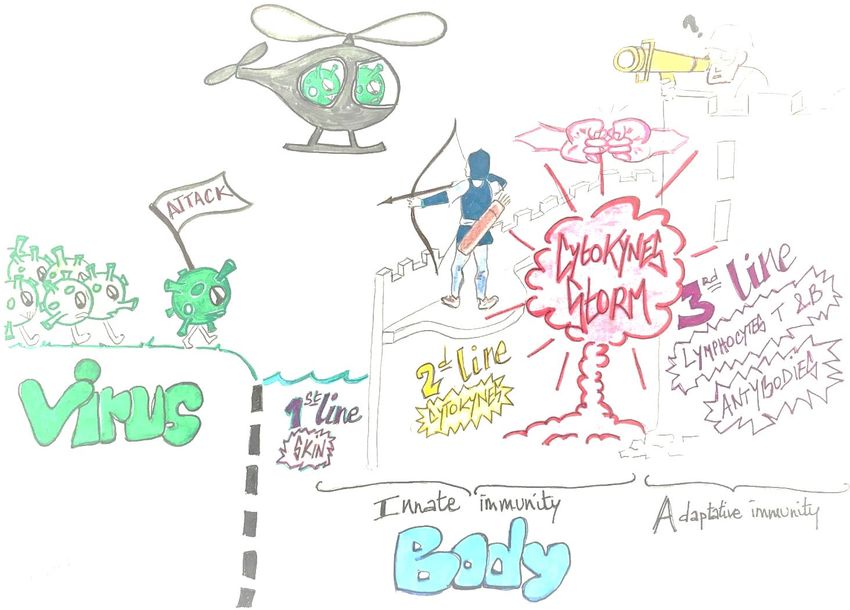
Please note all updates vs. previous versions are highlighted in yellow.
KEY MESSAGES
• This edition includes a new section providing a comprehensive analysis of the risk factors linked to being infected by
COVID-19, developing a severe form or dying from the disease as well as information on potential sequalae and
indirect effects of the disease
• More than 4.8 million confirmed cases have been reported globally since the beginning of the pandemic including
around 323,000 deaths. On May 19th, more than 95,500 new cases have been confirmed and new deaths amounted
to 4,804 people globally.
• While Western Europe and the US used to represent the bulk of new cases in early April, the countries having the
most new cases today are the US (21% of new cases on May 19), Brazil (17%) and Russia (10%), the last two
approaching 300,000 total cases, which is more than any European country. The pandemic also seems to accelerate
in India (6% of daily new cases on May 19th).
HIGHLIGHTS ON THE CURRENT SITUATION
• In the US, daily new cases amounted to 20,260 on May 19th and the country has the highest number of both
recorded cases and deaths from COVID-19 worldwide, with now more than 1.5m cases and 91,000 deaths reported.
That said, number of daily new cases US-wide seems to have reached a plateau around April 7th and seems to have
started decreasing since beginning of May.
• In Western Europe (Spain, Italy, France, Germany, UK), the number of daily new cases is on the way down and most
countries are gradually easing their lockdowns as a result (except in the UK, currently the European country with the
highest death toll, where lockdown easing will only start on June 1st)
• The pandemic seems to continue expanding in Russia, as the country now has the second highest number of total
cases worldwide (close to 300,000 total cases). That said, Russia seems to maintain a comparatively limited number
of reported deaths for the time being.
• The pandemic also seems to continue to spread in Brazil, that is now the country with the second highest number of
daily new cases behind the US. This might change over time as some regions are gradually issuing stay at home
orders (generating some legal disputes with the central government)
• The pandemic is accelerating in India, that represents ca. 6% of new cases globally on May 19th (6,147 new cases,
which is 2.5 times more than on May 1st).
Regions with the highest number of COVID-19 cases (May 19th 2020 data)
Note: The Case Fatality Rate given by WHO is a best estimate which doesn’t take into consideration differences between countries. CFR
can vary greatly between countries, depending on access to healthcare, the excessive burden on the healthcare system and overcrowding
of the emergency rooms. * Case fatality rate=Total # of death/Total # of cases. ^active cases=total number of cases – recovered – death.
^ R0 is the basic reproduction number, the average number of people get infected by each infected case.
CONTEXT
In early December 2019, a rapidly growing infectious disease among human population was identified in the
region of Wuhan in the People's Republic of China. The disease is caused by severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) and was named Coronavirus disease 2019 (COVID-19).
The outbreak spread quickly to numerous countries and territories all over the world, affecting significantly the
social and economic activities. On March 11, 2020, the World Health Organization (WHO) declared the
coronavirus outbreak an official pandemic.
Date
Below graphs are summarizing the latest developments of the pandemic worldwide, and for a selection of the
countries that are currently the most affected: The United States, Italy, Spain, Germany France, Russia, Brazil,
the UK, India.
• The first graph (top left) shows the total cumulative number of cases reported daily
• The second graph (down left) shows estimations of the doubling time of COVID-19, i.e. the time it
would take for the number of confirmed cases to double.
• The third graph (top right) shows the reported daily new cases, providing both reported data points
and a simple trend. Beyond the data points, a simple trend has been drawn to indicate possible
changes of direction.
• The fourth graph (down right) shows the reported number of daily new deaths, as well as the trend of
daily new deaths (similar as above).
4
WORLDWIDE
95,549 new COVID-19 cases were reported globally on May 19th. While the trend of daily new reported cases seemed to have reached a plateau at beginning of April, it seems that the
trend of daily new cases has been increasing again since beginning of May. This might be driven by the slowing down of the disease in Western Europe (driven by lockdown measures)
and its take off in other geographical areas such as Brazil and Russia. While Western Europe and the US used to represent the bulk of new cases in early April, the countries having the
most new cases today are the US (21% of new cases on May 19), Brazil (17%), Russia (10%) and India (6%). No significant impact of this increasing trend of new daily cases has been
noticed yet on the trend of daily new deaths, which continues to decrease. This could be linked to the fact that new cases have not materialized in new deaths yet or that the increasing
number of new cases is actually linked to more widespread testing which would help identify asymptomatic or mild cases (this could be the case in Russia, where the fatality ratio is
currently lower than in Western Europe).
95,549
34.6
4,804
5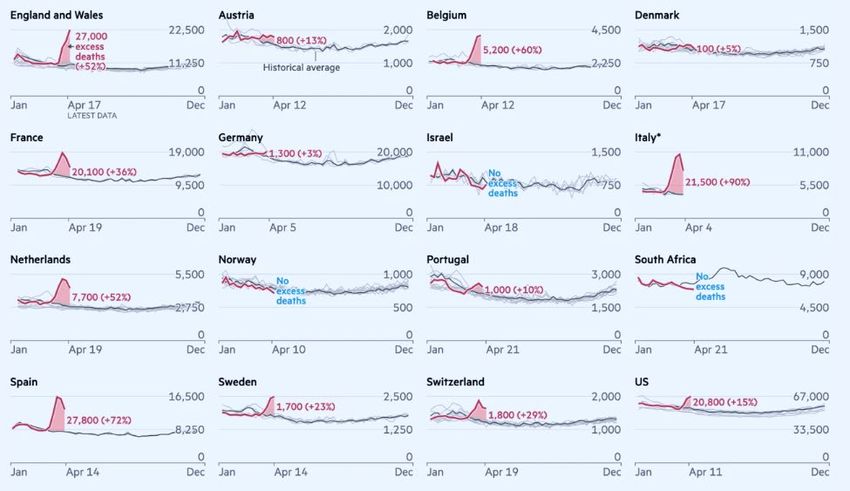
USA
In the US, daily new cases amounted to 20,260 on May 19th and the country still has the highest number of both recorded cases and deaths from COVID-19 worldwide with now more
than 1.5m cases and 91,000 deaths reported. The daily reported new cases seem to have reached a plateau around April 7th, and seem to be slowly decreasing since then. New deaths
have amounted to 1,574 on May 19th. The share of New York in those daily figures is gradually going down (NY only represents 11% of deaths and 10.3% of new cases on May 10th),
which means the pandemic is now more active in other states. As of May 19th, 5 US Sates (in addition to Washington DC and Puerto Rico) had ongoing stay-at-home orders (vs. 21 on
May 9th) and 25% of the US population currently remains in some form of lockdown (vs. 60% on May 9th).
20,260
1,574
1,474
219
(7.3% of US)
(14% of US)
6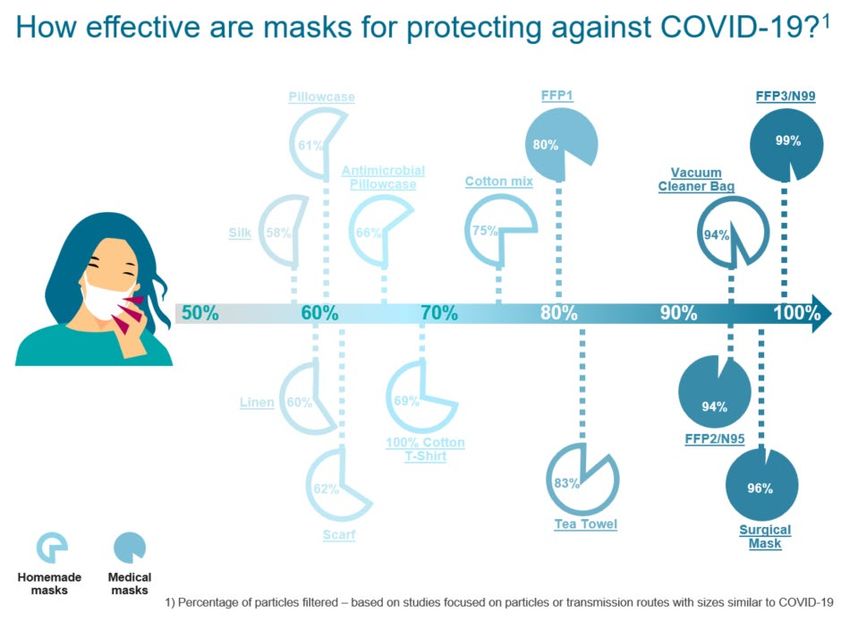
ITALY
In Italy, the pandemic has reached a plateau in late March (both in terms of daily new cases and deaths). On May 19th, 813 new cases and 162 new deaths were reported (which are
some of the lowest figures since beginning of March). The general lockdown put in place on March 9th therefore seems to be a success and May 4th marked the beginning of a
transition phase: since then, Italians can go out for strolls and visit relatives while some businesses are allowed to reopen. The situation needs to be closely monitored in terms of how
the disease might evolve now that the lockdown is eased. On May 18th, restaurants, cafés, bars, shops, hairdressers etc. were allowed to reopen in their turn.
May 4th: Gradual
end of lockdown
March 9th: Beginning of
lock-down
813
March 9th: Beginning of
lock-down May 4th: Gradual
end of lockdown
162
7
SPAIN
Spain recorded 431 new cases and 69 new deaths on May 19th, which are both some of the lowest totals since mid- March. The trend of daily new deaths and new cases seems to
keep decreasing since beginning of April. The government announced on April 28th that lockdown rules (in place since March 15th) would be gradually eased in 4 phases, starting with
reopening of small businesses and hotels and specific hours for shopping for people age 65+. After having allowed adults to go out for walks for the first time since beginning of
lockdown this weekend, Phase 0 is effective since May 4th and some regions are now in Phase 1.
232,037 March 15th: Beginning
of lock-down in Spain
May 4th: Phase 0 of
lockdown easing
431
March 15th: Beginning
of lock-down in Spain
May 4th: Phase 0 of
lockdown easing
69
8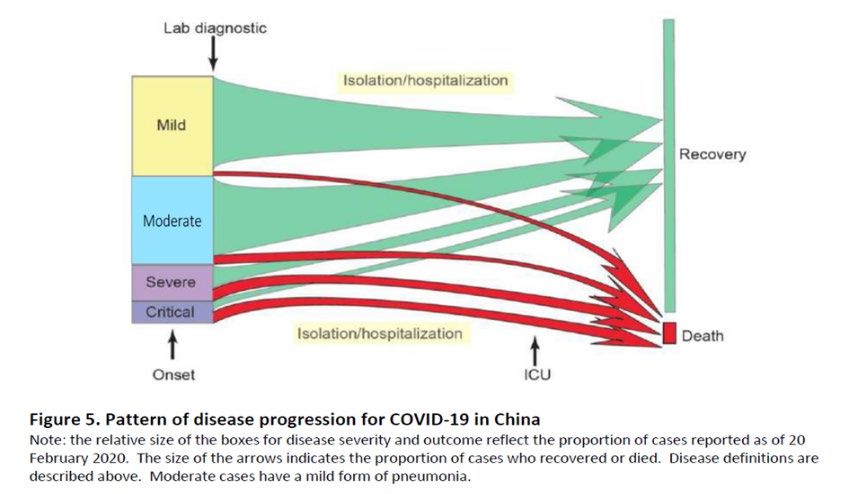
GERMANY
Germany reported 1,227 new cases on May 19th. The trend of daily new cases has started to decrease since end of March and that of new deaths around mid-April, with 78 new
deaths on May 19th. The number of deaths remains low (8,081 in total on May 19th) compared to other European countries such as France, Italy and Spain, and the fatality ratio is
amongst the lowest recorded (4.5% vs. 9.3% on average in Europe), which might be due to the testing capacities of the country that allowed to detect and isolate people that are
suspected of having the virus. Confinement measures are gradually being eased, as small shops could reopen in the week of April 18 and schools on May 4th (although under strict
conditions), all of this largely depending on local measures by the Länder. Although the Robert Koch Institute had estimated the R0 to be above 1 since last week, suggesting the
disease might take up again, the R0 is now assessed to have decreased below 1 again.
Beginning of
lockdown easing
Schools
reopening
March 14:Beginning of
containment measures in 1,227
Germany*
Beginning of
March 14: Beginning of lockdown easing
containment measures in Schools
Germany* reopening
78
* no general lockdown has been organized in Germany, but strong restrictions have been put in place (such as the
impossibility for people to gather by groups of 2 or more) – please note some regions had taken similar measures at
an earlier date (starting with Bavaria on March 14th)
9
FRANCE
***Due to data quality issues for France on May 19 in the Johns Hopkins University platform, comments for France are focused on May 18 data***
In France, daily new cases have reached 358 new cases on May 18th. The number of patients in intensive care keeps decreasing, indicating that the pressure on the health system
keeps going down. The trend of daily new deaths has kept decreasing since beginning of April, reaching 131 new deaths on May 18th. As a result, lock down measures started to be
eased from May 11th onwards, with primary school reopening and people being allowed to travel 100 kms around their home. There are however some local adaptations.
25,646
(incl 70% of cases from nursing
Beginning of lock houses not previously reported)
down in France
May 11th: easing of
lockdown
358
May 11th: easing of
lockdown
131
10UK
The United Kingdom reported 2,429 new cases and 546 new deaths on May 19th. The trend of daily new cases has been roughly stable since April 10th and seems to have started to
decrease since beginning of May. The trend of new deaths has been decreasing since mid-April. That said, the UK is now the European country with the highest death toll, with more
than 35,000 total deaths as of May 19th. On May 10th, the government announced that the lockdown would be extended until June 1st (although people who wish to go back to work
are encouraged to do so if they can).
Beginning of lock-
down in the UK
2,429
Beginning of lock-
down in the UK
546
11RUSSIA
Since beginning of April, the pandemic seems to have accelerated in Russia. With 9,263 new cases reported on May 19th (decreasing since mid May), Russia is now the country with
the third highest daily number of new cases right behind the US and Brazil and the total number of cases is the second highest globally with close to 300,000 total cases on May 19th.
The fatality ratio currently remains low at 0.95% with 2,837 deaths in total until May 19th. It remains to be seen whether this ratio remains as low over time (although it seems the
country has conducted extensive testing, with more than 5.5m tests realized since beginning of the pandemic as of May 13th). Despite the spike of new cases, the federal government
decided to gradually end the 6-weeks lock down on May 12th, though giving latitude to individual regions to decide how fast they should lift restrictions.
299,941
9,263
115
15.7
12BRAZIL
The pandemic seems to continue to be on the way up in Brazil, the country with the 2 highest number of daily new cases globally behind the US on May 19th with 16,517 new cases,
nd
bringing the total number of cases to 271,885 people. Although some states and cities are beginning to issue stay-at-home orders (and despite some legal disputes with the central
government on this aspect), the number of daily new cases and deaths is not showing signs of decrease yet.
271,885
16,517
1,130
13INDIA
The pandemic seems to have accelerated in India since beginning of May, reaching 6,147 new cases on May 19th (which is ca. 2.5 times more than on May 1st). The country represents
6% of daily new cases globally, which is the 4th highest total after the US, Brazil and Russia and the total number of deaths has crossed the 100,000 threshold this week.
106,475 6,147
15.7
146
14EPIDEMIOLOGICAL CHARACTERISTICS OF COVID-19
The mortality rate of the disease: the case fatality rate (CFR)
The case fatality rate (CFR) is calculated using the total number of deaths divided by the total number of reported
cases. The CFR changes over time during the pandemic and varies greatly across different regions. Depending on the
countries’ testing policies, the percentage of infected people who get tested and reported varies greatly. In South
Korea, mass testing was carried out for all suspected cases and anyone who was in contact with the cases. As a
result, Korea has one of the lowest CFR in the world because the denominator is large and covers the bulk, if not all,
of the infected population. This also applies to Germany, that also carries out a high number of tests. In comparison,
some other countries such as Italy, Spain, France or the UK have much higher CFRs, since they mostly test
hospitalized cases and not those with mild symptoms. This might change over time as some countries have
announced more extensive testing over the weeks and months to come, such as France and Italy. Furthermore, some
countries have also decided to include suspicious deaths from people that were not tested (such as New York, or
China, that has announced it would include in its official statistics people having died from the disease at home). The
table below shows CFR calculated from most recent data from the three countries. In all countries, we have observed
significant increases in CFR in older ages, especially among those over 70 years old. Mortality risk in males is higher
than in females. Additionally, we have seen elevated risk in people with comorbidities such as cardiovascular
diseases, cancer, diabetes etc. More details on risk factors can be found in the last section of this memo.
Furthermore, some initial studies are being carried out to assess the increase in mortality COVID-19 might have
caused, beyond the mere Case Fatality Ratio (which is heavily influenced by a country’s testing capacity).
According to a study published by the Financial Times on April 27th, the global death toll of COVID-19 might be 60%
higher than currently reported. Furthermore, the global mortality over March and April 2020 is 50% higher than the
average March-April mortality between 2015 and 2019. This might mean that COVID-19 would be responsible, either
directly or indirectly, for a 50% rise in mortality over March and April 2020.
That said, the mortality over the next months might be lower than in the past years due to the “Harvesting effect”: a
fraction of people who died in the past few weeks would have died in the coming months if they hadn’t been
affected by COVID-19.
15Source: “Coronavirus tracked: the latest figures as countries fight to contain the pandemic”, The Financial Times, May
1st 2020
16Covid-19 Clinical evolution and frequency29
Most people infected with COVID-19 virus have mild disease and will eventually recover. Approximately 80% of
laboratories confirmed patients have had mild to moderate disease, which includes non-pneumonia and pneumonia
cases. 13.8% have severe disease (dyspnea, respiratory frequency ≥30/minute, blood oxygen saturation ≤93%,
PaO2/FiO2 ratio 50% of the lung field within 24-48 hours) and 6.1% are critical
(respiratory failure, septic shock, and/or multiple organ dysfunction/failure).
Asymptomatic infection has been reported, but most of the relatively rare cases who are asymptomatic on the date
of identification/report went on to develop symptoms of the disease. The proportion of truly asymptomatic
infections is unclear.
Ways of COVID-19 transmission
The primary route of transmission of Covid-19 virus from human-to-human is through respiratory droplets. When an
infected person coughs, sneezes or talks, they generate droplets transporting the virus. If the droplets come into
direct contact with the mucous membranes (mainly respiratory and oral mucosa) of another person nearby, the virus
can be transmitted to this person and he/she may get infected. The droplets generally do not travel more than two
meters.
Recently, some new possible ways of transmission have been suggested, and they could be responsible for the high
rates of transmission seen53. The new routes of transmission are:
• Aerosols: There is evidence that the virus can remain viable in aerosols for at least three hours, thus
transmission through aerosol is possible. The graphs below show how the virus transmits through aerosols.
• Indirect transmission by inanimate objects (fomites): Infection can also occur if a person touches an infected
surface and then touches their nose, mouth or eyes.
Figure. Virus transmission through aerosols53.
17Several studies suggest that the virus can cause conjunctivitis, an inflammation of the inner surface of the eyelids.
The virus can possibly be transmitted by aerosol contact or indirect contact through contaminated fingers with the
conjunctiva. There is no data available on how many people are infected in this way. In precaution, ocular protection
is recommended for healthcare workers.
Since we do not fully understand the transmission mechanism of the virus, it is recommended to take precautions to
protect yourself. The measures adopted and recommended by WHO may not be efficient enough to block the virus
transmission. We would recommend that you use a mask in public confined spaces and wash your hands or use hand
sanitizers whenever you touch something indoors.
Our recommendations in details:
• Avoid crowds especially in poorly ventilated spaces.
• Avoid touching your face (eyes, nose, and mouth).
- If you have to touch your face, do it with the non-dominant hand. When you unconsciously touch
your face, most of the time it is with the dominant hand.
• Diligent hand washing, especially after touching surfaces in public places. Always use hand sanitizer that
contains at least 70% alcohol, when you touch something indoor, especially:
- after withdrawing money from the ATM
- after you use shopping carts or baskets in grocery stores and supermarkets.
• Avoid using public restrooms, elevators and other confined public spaces.
Wear a mask:
- If you are ill, to protect other people
- If you are healthy, to protect yourself from the infection
o If you have anti-pollution masks N95 or N99, use them
o If you have other protection types of mask, use them
• Clean all touchscreens and keyboards frequently.
• Clean and disinfect objects and surfaces that are frequently touched.
Applying all these measures in your daily life can protect you from Covid-19 infection.
18DEEP DIVE – ANALYZING THE EFFICIENCY OF MASKS TO
FIGHT COVID-19
By Dr. Gabriela Buffet, M.D., Associate Medical Director at SCOR Global Life
It is widely acknowledged that the COVID-19 virus is transmitted by respiratory route and through fomites
(contaminated inanimate object). Respiratory transmission occurs when an infected person emits droplets and/ or
aerosols that contaminate another person.
Several studies prove that masks can have a positive impact to reduce respiratory viruses transmission.
However, there are different types of masks offering different degrees of protection according to their filtering
efficiency.
Several types of masks can be used for medical purposes (not only related to COVID):
- Single use face masks normally have one layer and are very thin. They are generally only effective for
capturing large dust particles.
- Surgical masks: These masks are those rectangular shaped coverings (often pleated) that come with elastic
ear loops. Surgical masks are made of a paper-like nonwoven material and filter about 60 to 80 percent of
particles and, according to the Food and Drug Administration, mostly blocks “large-particle droplets, splashes,
sprays or splatter that may contain germs.”
- Respirator masks. These masks fit tightly to the face and have the highest filtration efficiency, blocking 95-99
percent of particles of 0.3 microns or larger. The respirator masks available in the USA as N95 or N99 mask
and in Europe as an equivalent FFP (‘filtering face piece’) mask, are used to prevent the user from inhaling
small airborne particles. There are three categories of FFP: FFP1, FFP2 and FFP3. FFP3 and N99 provides the
highest level of protection.
That said, other types of masks, generally not used for medical purposes can show some level of efficiency for blocking
transmission through droplets and aerosols
- Anti-pollution masks: Anti-pollution masks are designed to filter pollution particles of 0.3 - 0.1 microns large.
In theory they could therefore filter infected droplets and aerosols.
- Homemade masks: Although any material can be a physical barrier to infections (especially through
droplets), if it does not fit well around the nose and mouth or if the material allows for free passage of
infectious aerosols, the mask may not be efficient. Facial masks reduce exposure to aerosols by a
combination of the filtering action of the fabric and the seal between the mask and the face. Filtration
efficiency depends on a variety of factors such as the structure and composition of the tissue, as well as the
size, speed, shape and physical properties of the particles to which it is exposed.
How to assess the efficiency of masks?
Face masks’ use by the general public for limiting the spread of the COVID-19 pandemic is controversial. Key
question is what type of mask works best to prevent new infections.
It’s true that some masks seem to be more efficient than others: masks -when used correctly- decrease the effective
transmission rate in nearly linear proportion to their effectiveness (fraction of potentially infectious contacts
blocked).
Key aspect to consider when considering filtration efficiency of masks is the size of the particle that these masks can
help block. Indeed, for blocking particles sized >3 microns, all medical masks have similar levels of efficiency (filtering
>95% of particles).
For example, a study published last year shows no significant differences in efficiency between surgical masks and
N95 masks to prevent flu infection between healthcare staff.
On top of the size of the particle itself (size of COVID-19 is around 0.125 microns), size of its transmission particles
also needs to be taken into account. In the case of COVID-19, main transmission routes are droplets and aerosols,
19which have a significantly larger size. Therefore, even non-medical masks can also offer some level of efficiency and
protection.
When it comes to homemade masks for example, their efficiency was tested in a study published in 2013 (12) with
particles that have similar sizes to COVID-19. The study concluded that efficiency is variable according to the type of
fabric with least efficiency for silk and highest efficiency for masks made with vacuum cleaner bags (please note
vacuum bags can be extremely dangerous to use as masks – comment is only about their filtering efficiency).
Van der Sande et al. have studied the efficiency of respirator masks, surgical masks and homemade fabric masks by
comparing the number of particles (0.02-1 micron) on the exterior side of the mask vs. the interior side. In adults,
N95 masks offered 25 times the protection of surgical masks and 50 times the protection of homemade fabric
masks. The study also tested the effectiveness of the three types of masks in reducing emissions and found that
fabric masks reduced emitted particles by 20%, surgical masks reduced them by 50% and N95 masks reduced them
by two thirds.
In another recent study focused on COVID-19, Ma et al. found that N95 masks, medical masks, and homemade
masks made of four‐layer kitchen paper and one‐layer cloth could respectively block 99.98%, 97.14%, and 95.15% of
the COVID-19 virus transmitted through aerosols.
As a conclusion, homemade masks can provide a high degree of protection for certain types of transmission routes,
especially aerosols, although they are less solid and comprehensive than surgical masks or FFP2 masks. However,
reducing the transmissibility of the virus through homemade masks may help reduce the speed of reproduction (R0).
Here is an overview of the efficiency of different types of masks (either for medical use or homemade):
20N.B. How to wear a mask?
The World Health Organization has come up with following graph to easily explain how a mask should be properly
put on, used, taken off and disposed of. What we need to collectively keep in mind is that masks are first and
foremost useful for us to protect others and specifically the weakest among us.
More details and sources are available in appendix
21WHO Advanced Analytics and Mathematical Modelling21
WHO has been working with an international network of statisticians and mathematical modelers to estimate key
epidemiologic parameters of COVID-19, such as the incubation period (the time between infection and symptom
onset), case fatality ratio (CFR, the proportion of reported cases who die), infection fatality ratio (IFR, the portion of
all of those infected who die, including undiagnosed infections), and the serial interval (the time between symptom
onset of a primary and secondary case).
To calculate these parameters, statisticians and modelers use case-based data from COVID-19 surveillance activities,
and data captured from early investigations, such as those studies which evaluate transmission within clusters of
cases in households or other closed settings.
Preliminary estimates:
Median incubation period: 5-6 days (ranging from 0-14 days)
Median time from hospitalization to death: 12.4 days
Serial interval range: 4.4 to 7.5 days.
CFR (China): 2.3%.
Infection Fatality Ratio: is roughly 9.4 per 1000.
22months.” Hence, I can safely return to the office and get back to a normal
life
INTERVIEW: Understanding how
Aim of the serological tests that are being discussed in the media in several
immunity against COVID-19 works
With Manuel Plisson, Head of Biometric Modelling & countries is precisely to identify who has been infected by the disease and
Inclusive Underwriting and Dr. Gabriela Buffet, M.D., therefore immunized. The rationale behind this is to check whether herd
Associate Medical Director at SCOR Global Life
immunity has been achieved:
Experts say that as soon as 60% of the population is infected and
immunized, the epidemic naturally stops because the virus has no more
people to infect.
Assumption is that once you have been infected you are immunized
MANUEL PLISSON GABRIELA BUFFET
against the disease, although this generates debates within the medical
community.
One of the key questions about COVID is: Are
we sure to be immunized against COVID when we In the case of COVID-19, can this immunity
have been infected a first time? be seen? Do survivors become immune to the
For some infectious diseases like Measles, when you have been infected
disease?
and you have survived the first infection, your likelihood to be infected a
There is currently no evidence that COVID 19 survivors have immunity.
second time is extremely rare. You are immunized. This has been also the
Let me first explain the basic principles of the immune system. When
hope for COVID 19. Some people are thinking: “if I have been infected and
something is complicated to explain, I generally prefer to draw a picture:
I survived the disease, I am now immunized, at least for the coming
23Across the world, some heads of state have said we were at war against the
24Across the world, some heads of state have said we were at war against the virus. If those two initial lines of defense are inefficient
I rather agree with this image, because an infection is really a battle.
Imagine the body is a fortified castle you have to defend against an enemy: the
against COVID-19, can the body invent and produce a
virus. new weapon?
So how do you defend your castle? The innate immunity is what constitutes the
It can. This new weapon, the bazooka, is mainly Lymphocytes T and B and
defenses, the weapons you have already in stock. Innate immunity is made of 2
antibodies. This is the third line of defense.
different lines of. The moat around your castle is your first line. It is nothing more
Some people have this ability to invent and produce enough bazookas to destroy
than your skin and mucous membranes which prevent the entry of microorganisms
helicopters. Some people don’t.
inside your body. If the virus succeeds in passing this first line of defense, it reaches
• For some people who have this ability this is an asymptomatic form or a
a second line of defense: the archers, with their bows and arrows.
mild case of COVID 19.
Archers are the inflammatory response process which releases cytokines to shoot
• For the people who don’t have that ability to invent a bazooka or to
the virus and to warn the third line of defense. Cytokines are really a key element
produce enough of them to destroy COVID helicopters, this becomes a
of this second line of defense.
severe case of COVID.
Unfortunately, COVID 19 is very strong and clever and it has in its army some
helicopters. And moats and arrows are inefficient against helicopters.
When the body doesn’t find the bazooka, it keeps producing more and more
archers (cytokines) even though they are inefficient against COVID. This
overproduction of inefficient weapons leads to a surge, archers accuse each other
to be inefficient, they fight, a lot of disorganization appears: this is the cytokine
storm which is a kind of self-destruction in the body.
This is this cytokine storm which kills people.
People don’t die directly because of the virus. They die because of this self-
destruction due to inappropriate response.
25So all in all, can we safely say that individuals who Up to now there is no proof that people who have already been infected are
immunized and we have to be careful.
are able to produce those bazookas are immune to a
second attack, while the others might not be? Because a first infection doesn’t guarantee immunity,
There are indeed 2 types of individuals, 2 types of fortified castles.
and because there is no evidence about it for the time
Those who find the adequate response which means a high likelihood to
produce bazookas. And we can assume that these people will be ready to being, confinement, isolation, are more than ever our
fight a second infection. They have a high likelihood to have the right best response against the virus
antibodies in their blood.
Those who have a deregulate response (and the cytokines storm) and
therefore a low likelihood to have the right antibodies in their blood. It
means that even they have survived the first attack because their archers
were very good and maybe because they were lucky (the helicopters have
crashed without bazookas), it doesn’t mean they will be properly equipped
for a second attack.
The goal of serological tests is to track the presence of antibodies in the blood. But
even if there are antibodies in the blood it doesn’t mean that those antibodies are
the right ones, the ones that are efficient for a second attack.
The link between antibodies and immunity is not direct. It is not automatic.
For all these reasons, there is a debate on how to establish whether people are
immunized against COVID when they have been infected a first time.
And further debates to define under which conditions people can be immunized
after a first infection.
26DEEP DIVE – GASTROENTEROLOGY, HEPATOLOGY AND
COVID-19
By Dr. Dominique Lannes, M.D., Gastroenterologist, Associate Medical Director at SCOR Global Life
COVID-19 and Gastroenterology
More often than not, patients infected with COVID-19 suffer from gastrointestinal symptoms, although data is
missing, and discrepancies can be observed across countries. Here are the main points to consider:
• Gastrointestinal symptoms of COVID-19 patients include nausea, vomiting (in less than 5% of cases) or
diarrhea. The reported frequency of diarrhea among COVID-19 patients has varied from 2 to 33%
depending on countries. That said, it can be considered as one of the most prominent symptoms reported
and diarrhea may be an underestimated and under-reported symptom of COVID-19 infection.
For half of infected patients, COVID-19 is detectable in stool samples, and in 20% of cases, it remains
detectable even after the virus decreased to an undetectable level in respiratory tract.
• COVID-19 can also be found detected in gastrointestinal tissues (gastric, duodenal and rectal). Although
confirmation of viability from viral culture is lacking, this does suggest that orofecal transmission could be
of potential route of infection. Regarding inflammatory digestive diseases, for patients with Crohn's
disease or Ulcerative colitis with moderate to severe disease, Immunosuppressive (eg azathioprine,
methotrexate ...) and/or immunomodulator agents (eg anti TNF) are currently the reference as long term
treatment. Today hundreds of thousands of patients with Inflammatory digestive disease benefit from
these treatments across the world, especially in economically developed countries. These treatments have
an impact on blood lymphocyte count with possible lymphopenia – and lymphopenia could be associated
with an increased progression and severity of COVID-19. That said, there is currently no data on the impact
of immunosuppressive or immunomodulator agents and no specific recommendations for people on
immunosuppression. At the present time, it is not advisable for such patients to stop their treatment as a
preventative measure against COVID infection. If a patient is infected with COVID-19 stopping
immunosuppressive treatment can be recommended, but any decision must be made on a case by case
basis.
• Interactions and effect of COVID-19 on esophagus, stomach and pancreas are unreported at present
COVID-19 and Hepatology
COVID-19 infection causes liver impairment with abnormal levels of liver transaminases ALAT and ASAT. It is
frequent and has been reported in about 10 to 50% depending on studies. Severe COVID-19 patients tend to have
more abnormal liver transaminases levels and liver dysfunction than non-severe patients. However, no studies
suggest COVID-19 frequently causes clinically severe liver injury, even for the most severe patients.
The cause of liver damage in patients with coronavirus infections remains poorly understood and might be linked
to different factors:
• Direct action of the viral infection on liver cells, a viral hepatitis
• Drug hepatotoxicity: the more severe is the infection, the more potentially hepatotoxic drugs can be used.
• Immune-mediated inflammation, such as cytokine storm and pneumonia-associated hypoxia, could be an
explanation for patients with COVID-19 who are critically ill
Chronic liver disease, including cirrhosis, represents a major disease burden globally. Chronic viral hepatitis B or C,
NASH, and alcohol-related liver disease affect several hundred million people across the world. Therefore, it is
crucial to determine the impact of COVID-19 infection on the progression, severity and mortality linked to COVID-
19 in that population. Studies currently suggest that patients with severe liver disease at the cirrhosis stage present
a higher risk to die from COVID-19. In this patient population, preventing infection is very important and more
intensive surveillance is needed in case of severe COVID-19 infection.
More details and sources are available in appendix
27DEEP DIVE – KAWASAKI DISEASE AND COVID-19
By Dr. Gabriela Buffet, M.D., Associate Medical Director at SCOR Global Life
European scientists are investigating a possible link between Kawasaki disease and Covid-19 as a significant
number of infants begin displaying high fevers and swollen arteries.
In Europe (UK, Italy, Spain and France) many children under 9 years old have reported that they are experiencing
apparent symptoms of Kawasaki Disease.
What is the Kawasaki disease?
Kawasaki disease is a rare systemic vasculitis mostly affecting medium-sized arteries. Main symptoms include fever,
conjunctivitis, skin and mucous membrane affection, and cervical lymphadenopathy. Generally, inflammatory
changes to arterial vessels of all body regions are present. However, coronary arteries are most affected and most
severe complications usually involve the heart. In the acute phase, most patients exhibit clinically inapparent
myocarditis and/or pericardial effusions. Coronary aneurysms usually develop after several weeks and can result
and cause severe sequelae, including cardiac infarctions. Additional organ manifestations include pancreatitis,
urethritis, facial palsy and anterior uveitis.
Kawasaki Disease mainly affects young children, although it can also affect people of any age. Globally, it is the
most common form of childhood primary vasculitis.
The etiology of Kawasaki Disease is not known. Various studies suggest that it is intimately linked to infectious
diseases. Kawasaki Disease is likely to be triggered by infectious agents in individuals with specific genetic
background.
Kawasaki Disease Treatment
Treatment with Intravenous immunoglobulins (IVIG) is necessary. It was demonstrated that IVIG treatment, if
applied within the first 10 days of fever, reduces the risk for the development of coronary aneurysms from 25% to
approximately 5%.
Salicylic acid and corticoids can also be associated with IVIG.
Prognosis
With timely and adequate treatment approximately only 5% of all Kawasaki disease patients develop arterial
aneurysms and need cardiac care to prevent cardiac infarctions.
Sources are available in the appendix
28COVID-19 DIAGNOSIS, TESTING AND TREATMENT
By Lars Pralle, Senior Life Underwriting Actuarial Expert, SCOR
How is a COVID-19 case defined?
Case definition is based on epidemiological, clinical and virologic criteria. Each country has its own definition.
The number of infected people can vary across countries for at least 2 reasons:
Accuracy of diagnosis test varies, depending on manufacturing laboratory. Selection criteria (epidemiological and
clinical) of population to be screened varies from one country to another and changes over time as the pandemic and
the capacity of laboratories to manufacture test kits evolve.
There are 2 types of tests to diagnose Covid-19 virus:
• Virologic tests
• Clinical tests (radiological test)
Virologic tests (please refer to our deep dive below)
A few virologic tests have been developed by research institutions across the world:
Country Institute
China China CDC
Germany Charité
Hong Kong SAR HKU
National Institute of Infectious
Japan Diseases, Department of Virology
III
Thailand National Institute of Health
US US CDC
France Institut Pasteur, Paris
Clinical (radiological) tests:
The radiological exam has a better sensibility (about 80%) but it can also capture other diseases such as influenza and
other respiratory infections. The false positive rate might be higher than the WHO test. A combination of virologic
test and radiologic test might improve the test accuracy in the future, but no protocol has been developed in that
way yet.
Selection of the population to test
As stated above, the population selected to be tested can vary depending on the pandemic evolution in each
country. In the beginning of the pandemic, both epidemiological and clinical criteria are generally required for people
to be tested. That said, some countries only require clinical criteria, and there are disparities on the severity of the
symptoms required to be tested.
For example, in the US, testing criteria used to be restrictive (epidemiological criteria only). Loose testing criteria can
however lead to the situation where infected people may not be detected promptly, and the virus can disseminate in
the whole country. In Italy, when the first cases were detected, the government decided to screen everybody who
was asking for the test but as the pandemic spread, health authorities started to restrict testing for only hospitalized
cases (moderate to severe cases). Again, as the number of daily new cases is decreasing, the number of tests has
considerably increased over the past few weeks and Italy is now the country that tests its population the most (see
graph below). Likewise, in France, at the beginning of the pandemic, all the symptomatic cases and the people who
had been in contact with them were tested. Later, only hospitalized people were tested. As more tests are being
ordered and produced, authorities have decided to start broader testing, not restricted to symptomatic tests
anymore, especially in nursing houses.
29Overall, it seems that testing capabilities are ramping up in many countries, and that countries that did not use to
test massively at the beginning of the epidemic are now testing a lot more, as shown in the below.
Number of COVID-19 tests carried out for 1000 inhabitants as of April 26*, 2020, by country
Source: Statista
* except for: USA on April 25, France on April 21, Germany on April 19
The specificities of each country’s screening policy could explain why the number of infected people and the
percentage of cases requiring critical care varies across countries.
Due to the tests and selection criteria, the number of infected people may not show the real magnitude of pandemic
in each country.
Undocumented infections
During the pandemic, it is not possible to test the whole population to get the true infection rate. Most of the
countries chose to test moderate, severe and critical cases or only hospitalized cases.
Undocumented (not tested) infections often present with mild, limited or non-existent symptoms and are therefore
not detected. Depending on the number of undocumented infections and its contagiousness, it can expose a much
larger proportion of the population to the virus.
Asymptomatic and mild ill people might be responsible for the high number of infections in the population. In China,
according to Science paper, undocumented infections before the shutdown of Wuhan city, were estimated to be 86%
of all infections50 and they were the infection source for 79% of documented cases.
In Diamond Princess cruise ship, the estimated asymptomatic proportion of infected people is 17.9% (95% credible
interval (CrI): 15.5–20.2%)51.
Estimating the real number of all infected people is very difficult. Differences in viral surveillance and testing, case
definition and reporting, all can impact the documented infection rate of each country.
30DEEP DIVE - Diagnostic testing for COVID-19
In the further management of the COVID-19 pandemic, it is crucial to identify infected individuals.
Different use cases for diagnostic tests can be envisaged:
• diagnostic in pandemic or endemic setting
• triage in pandemic setting
• confirmatory testing after triage
• monitoring of infections at population level
• determination of previous infections in view of testing developed immunity
While in the diagnostic use case, the accuracy of the tests is key, in the triage testing the scalability and rapidity
of the tests may be more important, in particular in combination with confirmatory procedures in selected
cases.
For COVID-19, two different types of tests can be distinguished:
• Molecular genetic tests: tests that aim to directly detect the presence of the SARS-COV-2 virus by
using molecular genetic methods
• Serological tests: tests that use serological methods to detect proteins in the blood that are
indicators of either the presence of the virus (antigens), or of an immunological response of the
patient (antibodies).
Molecular genetic tests
These tests rely on swabs of the inner throat or noses and detection of virus in the sample. The swabs are
introduced into chemical reagents and in several thermal and chemical cycles, characteristic parts of the viral
RNA get amplified in a process called polymerase chain reaction (PCR), until sufficient material is present to
be detected in a genetic fingerprint. This requires advanced laboratory equipments (if tests are carried out
manually), or specialized automated laboratory equipment (for automized, cartridge-based PCR-test). The
processing time of such test ranges from approx. 30 mins for automated assays to several hours for the manual
procedure. Due to the required material and expertise, these tests cannot be scaled to screen entire
populations, therefore targeted testing is necessary. The genetic tests detect directly the virus in the swab.
Serological tests
Serological tests are using blood or blood parts as sampling material and their test mechanism is relying on
reactions with typical proteins that are markers for the infections. These proteins could either be linked to
antibodies that the patient's immune system in response to the virus or to antigens of the virus itself.
31Molecular genetic tests Serological tests
Mechanism Detection of viral genetic sequences Detection of viral or corporal proteins
(RNA) after amplification of RNA by that are markers for the SARS-COV-2
PCR
Requirements Advanced laboratory equipment Standardized test (ELISA) providing
and know-how yes/no response for presence of targeted
Or specialized equipment for proteins
automated tests Can be lab-based or performed at point-
Trained personnel to correct take of-care, depending on test design
the swabs
Testing time window when the virus is present in the Antibody tests: it may take two weeks
upper respiratory tract, a few days after infection until antibodies are
after infection - in later stages of the traceable - on the other hand former
infection the virus may no longer be infections (and thus potential immunity)
present in the upper respiratory can be detected
tract and thus more difficult to Antigen tests: no testing time window for
capture by swabs antigen tests (like PCR tests).
Accuracy In principle, this is the "gold Full independent validation still to be
standard" to define the infection. done
Generally, genetic tests are highly More than 100 companies have filed for
accurate. Reports on cases where approval of serological tests for Covid-19
test results had to be revised could and show sensitivities and specificities
be related to improper taking of the above 90% (up to 99%)
swabs or be timing related.
Target population Identification of currently infected Identification of cases that have had
cases that are contagious exposure to the virus and have developed
some immunity (antibody tests) or
identify cases suspected of being infected
(first triage and flag for further testing by
PCR)
Scalability limited due to complex equipment Once established, test kits will be
and know-how needed produced in large quantity, execution of
the test can be carried out at point-of-
care (or even self-testing)
Time required from test Between 30 mins and 3 hrs., plus Typically, 10 minutes
to result transport/shipping time to labs
Typical turn-around time currently 3
days
Interpretation of Confirms virus currently present, Antibody-test confirms past or recent
positive result may not be reliable in early phase of exposure to the virus
infection if viral load is insufficient Antigen-test confirms current or
suspected infection
32Virus dynamics and host response during infection by SARS-CoV-2
Knowledge of virus dynamics and host response are essential to select the appropriate test.
Diagnosis tests choice depends of infection evolution. In early infection, viral detection by molecular genetic
test is the choice.
After 10 days of infection, the choice of test depends on what we want to highlight. If it is the patient's
infectivity the choice will be for tests that detect the virus. If it is immunity the tests chosen should test the
immunoglobulins IgG (late immunity), Ig M (recent immunity).
Use of SARS-CoV-2 tests
Molecular genetic tests:
-Individual level: Diagnosis of Infection
-Health care: Patient management and treatment efficiency
-Public health: Detection of asymptomatic carriers
Serological tests:
- Individual: Detect past infection by detection of IgG.
- Public health: detect Immunity of population.
Universal populational testing
With the association of these 2 different tests, it's possible to detect asymptomatic viral carriers and individual
and populational immunity. Populational testing will be necessary to lift contention measures
33Tests for SARS-COV-2/COVID-19 and potential uses
Schematic picture of serological test
More details are provided in Appendix
34DEEP DIVE: Investigational Drugs For Covid-1973-75
As of today, no drugs or biologics have proven to be effective for the prevention or treatment of COVID-19.
That said, numerous antiviral agents, immunotherapies, and vaccines are being investigated and developed
as potential therapies, raising hopes as well as controversies across the scientific community.
Antiviral Agents
Remdesivir
The antiviral agent remdesivir is a nucleotide analog prodrug. Remdesivir has been shown to inhibit
replication of other human coronaviruses associated with high morbidity in tissue cultures, including severe
acute respiratory syndrome coronavirus (SARS-CoV) in 2003 and Middle East respiratory syndrome
coronavirus (MERS-CoV) in 2012. Efficacy in animal models has been demonstrated for SARS-CoV and MERS-
CoV.
Several phase 3 clinical trials are testing remdesivir for treatment of COVID-19 in the United States, South
Korea, and China. An adaptive randomized trial of remdesivir coordinated by the National Institute of Health
(NCT04280705) started first against placebo, but additional therapies can be added to the protocol as
evidence emerges. The first experience with this study involved passengers of the Diamond Princess cruise
ship under quarantine at the University of Nebraska Medical Center, after returning to the United States
from Japan following an on-board outbreak of COVID-19. Positive results were seen with remdesivir after use
by the University of Washington in the first case of COVID-19 documented in the US.
Lopinavir/ritonavir
Lopinavir/ritonavir is a HIV-1 protease inhibitor FDA-approved since 2000 to treat HIV-1 infection.
In a randomized, controlled, open-label trial of hospitalized adults (n=199) with confirmed SARS-CoV-2
infection, recruited patients had an oxygen saturation of 94% or less on ambient air or PaO2 of less than 300
mm Hg and were receiving a range of ventilatory support modes (eg, no support, mechanical ventilation,
extracorporeal membrane oxygenation [ECMO]). These patients were randomized to receive
lopinavir/ritonavir 400 mg/100 mg PO BID for 14 days added to standard care (n=99) or standard care alone
(n=100). Results showed that time to clinical improvement did not differ between the two groups (median,
16 days). The mortality rate at 28 days was numerically lower for lopinavir/ritonavir compared with standard
care (19.2% vs 25%) but did not reach statistical significance.
Immunomodulators and Other Investigational Therapies
Interleukin-6 inhibitors
Interleukin-6 (IL-6) inhibitors may ameliorate severe damage to lung tissue caused by cytokine release in
patients with serious COVID-19 infections. Several studies have indicated a “cytokine storm” with release of
IL-6, IL-1, IL-12, and IL-18, along with tumor necrosis factor alpha (TNFα) and other inflammatory mediators.
The increased pulmonary inflammatory response may result in increased alveolar-capillary gas exchange,
making oxygenation difficult in patients with severe illness.
Sarilumab (Kevzara)
FDA-approved since 2017 to treat Rheumatoid arthritis.
On March 16, 2020, Sanofi and Regeneron announced initiation of a phase 2/3 trial of the IL-6 inhibitor
sarilumab (Kevzara). The United States–based component of the trial will be initiated in New York. The
multicenter, double-blind, phase 2/3 trial has an adaptive design with two parts and is anticipated to enroll
up to 400 patients. The first part will recruit patients with severe COVID-19 infection across approximately
16 US sites and will evaluate the effect of sarilumab on fever and the need for supplemental oxygen. The
35second, larger, part of the trial will evaluate improvement in longer-term outcomes, including preventing
death and reducing the need for mechanical ventilation, supplemental oxygen, and/or hospitalization.
Tocilizumab (Actemra)
FDA-approved since 2010 to treat various type of arthritis, including rheumatoid arthritis, and cytokine
release syndrome.
An open label, non-controlled, non–peer reviewed study was conducted in China in 21 patients with severe
respiratory symptoms related to COVID-19. All had a confirmatory diagnosis of SARS-CoV-2 infection. The
patients in the trial had a mean age of 56.8 years (18 of 21 were male). Although all patients met enrollment
criteria of (1) respiratory rate of 30 breaths/min or more, (2) SpO2 of 93% or less, and (3) PaO2/FiO2 of 300
mm Hg or less, only two of the patients required invasive ventilation. The other 19 patients received various
forms of oxygen delivery, including nasal canula, mask, high-flow oxygen, and noninvasive ventilation. All
patients received standard of care, including lopinavir and methylprednisolone. Patients received a single
dose of 400 mg tocilizumab via intravenous infusion. In general, the patients improved with lower oxygen
requirements, lymphocyte counts returned to normal, and 19 patients were discharged with a mean of 15.5
days after tocilizumab treatment. The authors concluded that tocilizumab was an effective treatment in
patients with severe COVID-19. Nonetheless, these conclusions should be viewed with extreme caution. No
controls were used in this study, and only one patient was receiving invasive mechanical ventilation. In
addition, all patients were receiving standard therapy for at least a week before tocilizumab was started.
To confirm the efficacity of tocilizumab a randomized, double-blind, placebo-controlled phase III clinical to
evaluate the safety and efficacy of tocilizumab plus standard of care in hospitalized adult patients with
severe COVID-19 pneumonia compared to placebo plus standard of care is ongoing. The goal is to begin in
early April 2020, with a target of approximately 330 patients globally. The primary and secondary endpoints
of the study include clinical status, mortality, mechanical ventilation, and ICU variables.
Hydroxychloroquine and chloroquine
Hydroxychloroquine and chloroquine are widely used antimalarial drugs that elicit immunomodulatory
effects and are therefore also used to treat autoimmune conditions (eg, systemic lupus erythematosus,
rheumatoid arthritis). These drugs are inhibitors of heme polymerase; and are also believed to have
additional antiviral activity. According to a consensus statement from a multicenter collaboration group in
China, chloroquine phosphate 500 mg (300 mg base) twice daily in tablet form for 10 days could be
considered in patients with COVID-19 pneumonia.
A first study in France evaluated patients treated with hydroxychloroquine against a control group who
received standard care. After dropping 6 patients from the analysis for having incomplete data, the 20
remaining patients receiving hydroxychloroquine had improved nasopharyngeal clearance of the virus on
day 6 (70% [14/20] vs 12.5% [2/16]) compared with the control group. A second study with 80 patients was
published and results were similar.
All the potential agents under investigation for SARS-CoV-2 can be found in Appendix.
36You can also read