COVID-19 Monoclonal antibody use in post-acute, long-term care settings - Monday, September 13, 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

COVID-19 Monoclonal antibody use in
post-acute, long-term care settings
Monday, September 13, 2021
4:00pm – 5:00pm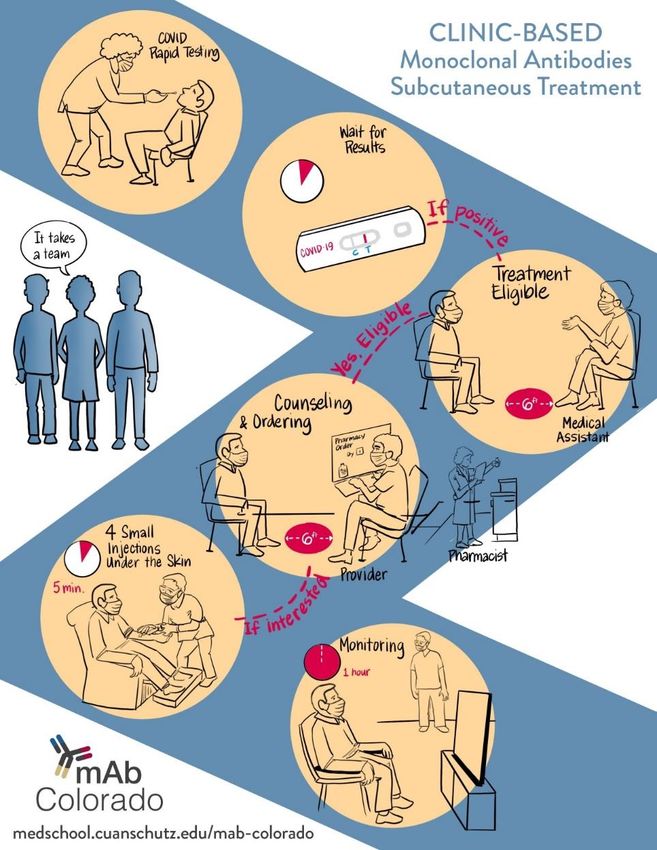
Presenters
• Presenters/ Panelists:
• Diana Tapay, MD
• Hillary Lum, MD PhD
• Allison Villegas, PA-C
• Jennifer Connelly, PharmD, BCACP, BCGP
• Clay Watson, MD
• Moderators: Sing Palat, MD CMD and Leslie Eber, MD CMD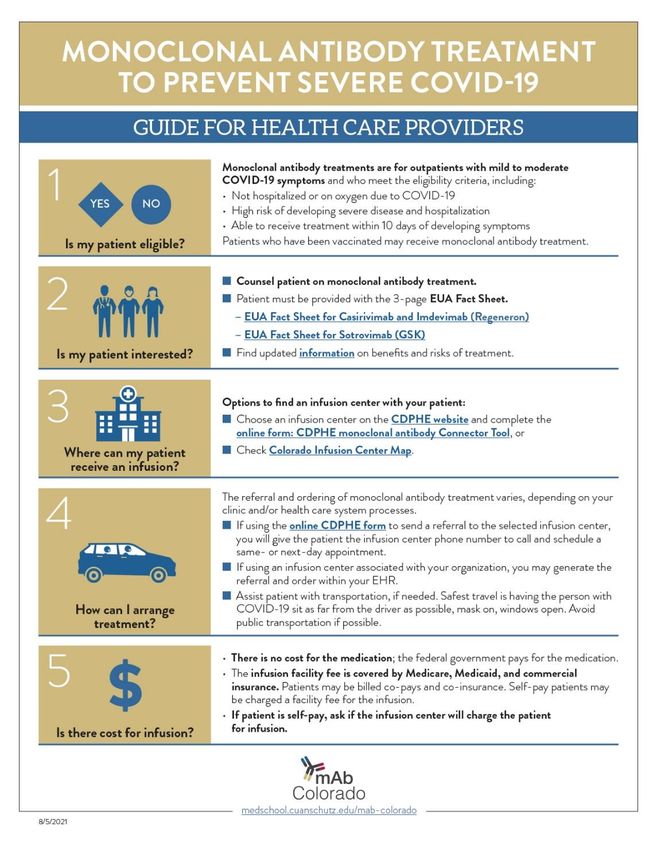
COVID-19 Cases in Colorado
3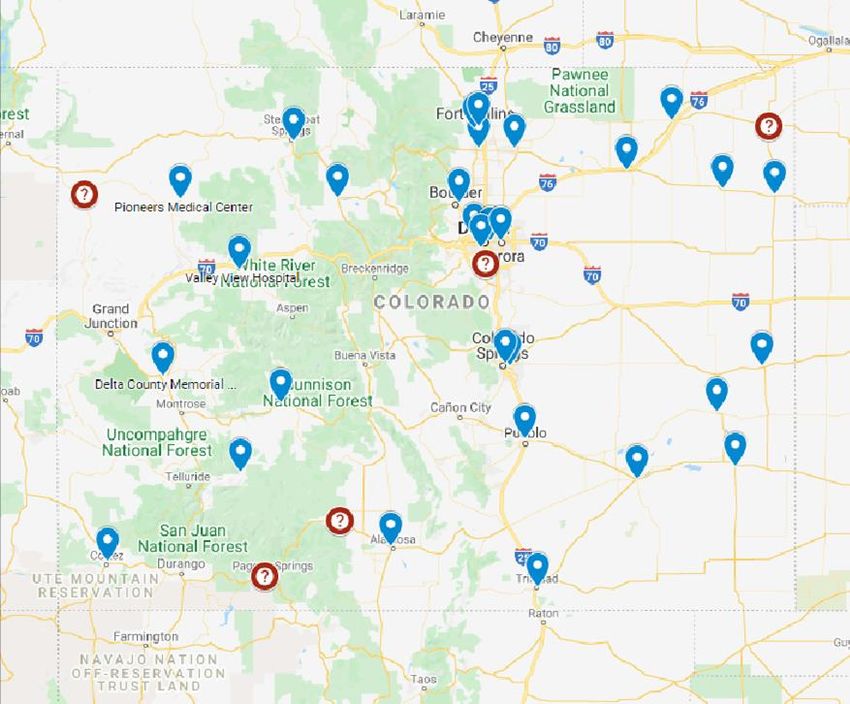
COVID-19 Cases in Colorado
4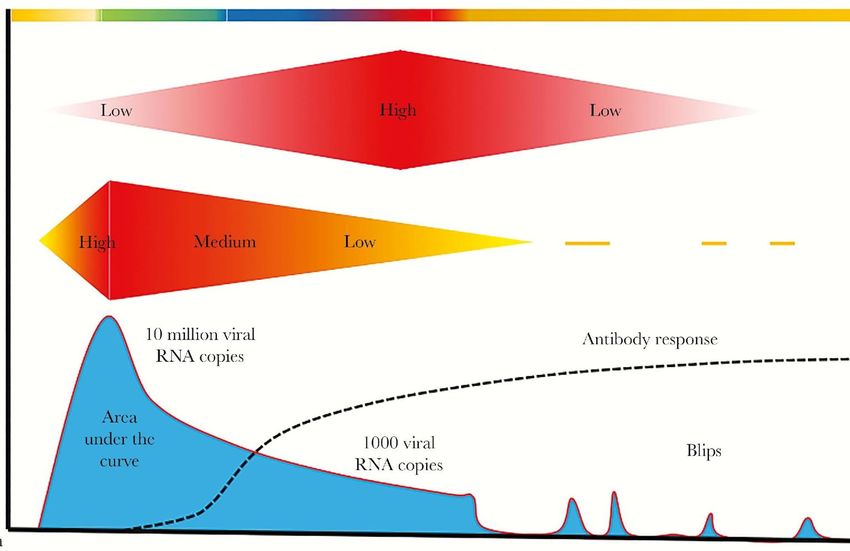
Available Monoclonal Antibodies
Use Formulation
Post-exposure
Treatment IV SQ
Product Prophylaxis
Casirivimab/imdevim
✔ ✔ ✔ ✔1
ab
sotrovimab ✔ ✔
bamlanivimab/etesevi
✔ ✔
mab2
1 - For treatment, IV is preferred but SQ may be used if administering IV would delay treatment
2 - Distribution and use of bamlanivimab/etesevimab was recently restarted
5
Bamlanivimab/etesevimab timeline
11/9/2020 2/9/2021 4/16/2021 6/25/2021 8/27/2021
Bamlanivimab Bamlanivimab/ Bamlanivimab Bamlanivimab/ Bamlanivimab/
authorized etesevimab authorization etesevimab etesevimab
authorized REVOKED distribution distribution
Etesevimab not Due to increase in PAUSED RESUMED
authorized as circulation of resistant Due to increase in For areas where
monotherapy variants circulation of resistant resistant variants
variants: B.1.351 (Beta) (B.1.351/Beta,
and P.1 (Gamma) P.1/Gamma, AY.1, AY.2,
B.1.621) are less than 5%
of circulating variants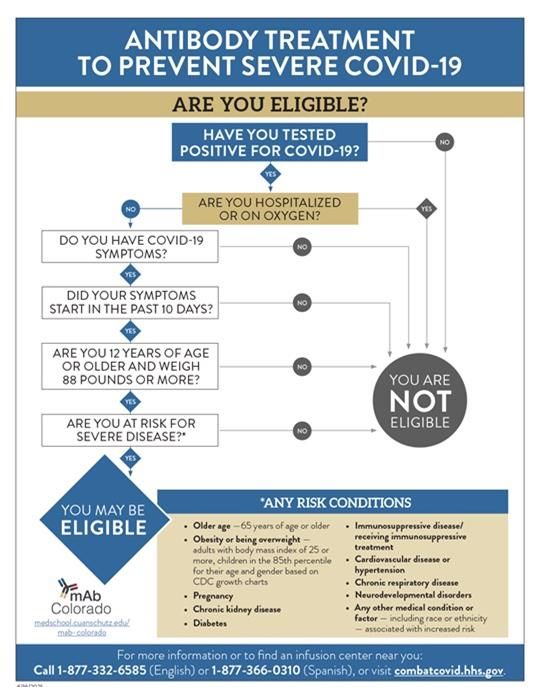
Residential Care Facility
Comprehensive Mitigation Guidance
https://drive.google.com/file/d/1TCZVpFTZVkJntn0cmlJT5JCr9mPFoJvS/view
CDPHE website COVID-19 Treatments https://covid19.colorado.gov/for-coloradans/covid-19-treatments
Evidence for Monoclonal Antibody Therapy for COVID-19 & Treatment Considerations
Provider Survey Results:
Top Barriers to Referral Key Points:
• Need to simplify
1. The process for ordering mAb treatment is too the ordering
complicated (32% major barrier, 34% moderate barrier)
process
2. The process for getting mAb treatment takes too long
(23% major barrier, 28% moderate barrier)
• Providers want
3. I have concerns about out-of-pocket costs to my more information
patients (18% major barrier, 30% moderate barrier)
about availability of
4. I don't know enough about mAb treatment (16% major
barrier, 35% moderate barrier) treatment, cost,
5. My patients are no longer eligible by the time I see
and need for
them (14% major barrier, 39% moderate barrier) timely action
**CMDA members received the surveyClinical Course of SARS-CoV-2 Infection
Figure 1. Schematic of severe acute respiratory syndrome
coronavirus 2 infection in a symptomatic person. RNA, ...
Asymptomatic Outpatient Risk of Risk of Critical Death or Reinfection
Presymptomatic Mild symptoms Hospitalization Illness/Mortality Recovery
Inflammation
Transmission
Viral Load
Immune-Based Therapies
Vaccines Antibody Therapies Modified from: Schiffer J, et al, Open Forum
Antiviral Therapies Infect Dis, Volume 7, Issue 7, July 2020,
ofaa232, https://doi.org/10.1093/ofid/ofaa232REGEN-COV Antibody Cocktail Pre-print released, June 6, 2021
Clinical Outcomes COVID-19 Outpatients
STUDY DESIGN
- 4,057 outpatients with mild-moderate COVID-19 with
one or more risk factors for severe disease
- Randomized to placebo or various doses
of CAS/IMD
- Followed for 29 days
STUDY RESULTS
- Reduced hospitalization or all-cause death
compared to placebo by 71.3%
- Symptoms resolved 4 days faster vs placebo (10
vs 14 days; pALL DOSES OF CASIRIVIMAB WITH IMDEVIMAB SHOW DECREASES FROM BASELINE
VIRAL LOAD OVER TIME
LS Mean (SE) Change from Baseline Viral Load Side-by-Side Comparison of IV and SC
(Serum-antibody negative mFAS)
LS Mean of Change From Baseline (SE)
IV SC
0
–1
–2
–3
–4
–5
–6
Baseline 3 5 7 Baseline 3 5 7
Days
Pooled placebo Casirivimab with Imdevimab (300 mg, IV) Casirivimab with Imdevimab (600 mg, IV)
Casirivimab with Imdevimab (1200 mg, IV) Casirivimab with Imdevimab (2400 mg, IV) Casirivimab with Imdevimab (600 mg, SC)
Casirivimab with Imdevimab (1200 mg, SC)
IV, intravenous; LS, least-squares; mFAS, modified full analysis set; SC, subcutaneous; SE, standard error.
13Monoclonal Antibody Therapy for Residents with a Positive Test Monoclonal antibodies are approved for treatment of patients who are diagnosed with COVID-19 and have a high risk of progression of disease, but are not yet ill enough to require hospital admission. Treatment with monoclonal antibodies has the potential to alleviate symptoms and limit progression to severe disease in patients with mild to moderate COVID-19. ● All residents who are diagnosed with COVID-19 by a PCR or antigen test for SARS CoV-2 and are not hospitalized should be evaluated by a health care provider to determine if they are eligible for monoclonal antibody therapy. ● A health care provider should be consulted immediately after the positive test result is received, as there is only a 10-day window to initiate monoclonal antibody therapy after the onset of symptoms (or documentation of a positive test in patients without symptoms). https://drive.google.com/file/d/1TCZVpFTZVkJntn0cmlJT5JCr9mPFoJvS/view Version 8/19/2021
mAbs for
• Expanded authorization enables use of REGEN-COV for
Post-Exposure post-exposure prophylaxis in certain people exposed to
Prophylaxis a SARS-CoV-2 infected individual, or who are at high risk
of exposure to an infected individual in an institutional
setting
June 30, 2021:
FDA Expands Authorized • Supported by Phase 3 data showing 81% reduced risk of
Use of REGEN-COV™ symptomatic infections in household contacts of SARS-
(casirivimab and CoV-2 infected individuals
imdevimab)
Aug 17, 2021:
NIH guidance on PEP
https://www.covid19treatm
entguidelines.nih.gov/thera
pies/statement-on-
casirivimab-plus-
imdevimab-as-pep/
O’Brien et al., NEJM. Aug 2021• In situations where it is necessary to triage
eligible patients (due to logistical
constraints), the Panel suggests:
• Prioritizing the treatment of COVID-19 over
PEP of SARS-CoV-2 infection.
• Prioritizing the following groups over
vaccinated individuals who are expected to
have mounted an adequate immune
response:
• Unvaccinated or incompletely vaccinated
individuals who are at high risk of progressing
to severe COVID-19
• Vaccinated individuals who are not expected
to mount an adequate immune response
(e.g., immunocompromised individuals).
https://www.covid19treatmentguidelines.nih.gov/therapies/statement-on-the-prioritization-of-anti-sars-cov-2-monoclonal-antibodies/COVID-19 • Multiple studies now show mAbs avert
70-80% of hospitalizations and deaths
mAbs
• mAbs also decrease symptoms
Summary by four days
• Effective against Delta variant
• CAS/IMD (REGEN-COV2) can be given
as subcutaneous injection if IV
administration is not feasible
• mAb therapy can be given regardless of
vaccination status
• mAbs can be given as post-exposure
prophylaxisClinician Checklist 1. Determine eligibility 2. Discuss treatment with patient and care partners 3. Identify treatment location 4. Refer and order treatment 5. Address cost and access questions
Clinician Checklist — 3. Find Treatment Location
Infusion Sites in Colorado
• CDPHE - https://covid19.colorado.gov/for-coloradans/covid-19-treatments
• HHS Protect Public Data Hub – Therapeutics Distribution: https://protect-
public.hhs.gov/pages/therapeutics-distribution
• Location information includes whether site can:
• Take patients outside of healthcare network
• Take pediatric patients
•Only includes sites that have registered with
CDPHE
• Doesn’t include home health agencies, long-term care
pharmacies/facilities
• HHS Protect Public Data site has locations
that have received shipments under the EUA.Clinician Checklist
Refer and Order
Treatment
Know your local referral and
order options
• CDPHE mAb Connector tool
sends referral to selected
infusion center Case
• Direct order if infusion center
within same health system CDPHE Monoclonal Antibody
• Provide patient with a written Connector Tool
prescription https://covid19.colorado.gov/for-
coloradans/covid-19-treatmentsCost and Access Issues
• Federal government purchases doses of REGEN-COV
and Bam/Ete
• No out of pocket cost for Medicare patients
• Covered by Medicaid and most health plans (co-pay
varies)
Case
• Costs for uninsured patients - may be waived or
discounted; site charges vary (~$500-800)
• Assist with transportation as possible
• Home health injection options may be available
• Consider offering subcutaneous injection:
Four injections (2.5 ml each) may be specifically feasible
for interested care settingsResources
• CDPHE - https://covid19.colorado.gov/for-
coloradans/covid-19-treatments
• UCHealth Virtual Health Center (303-752-7732)
• Available to Health Care Providers
• NIH treatment guidelines
https://www.covid19treatmentguidelines.nih.gov/
• HHS Playbook
https://www.phe.gov/emergency/events/COVID19/inves Contact:
tigation-MCM/Documents/USG-COVID19-Tx- mAbColorado@cuanschutz.edu
Playbook.pdf
• Ordering monoclonal antibody treatment Colorado website:
• A supply of COVID-19 monoclonal antibody www.mAbColorado.org
products can be ordered directly from
AmerisourceBergen Corporation (ABC)
• Download information on how to order from ABCmAB in the LTCF 4 Easy Steps
Case of Mr. D
Step 1: Determine Treatment Eligibility Must be positive and symptomatic for COVID-19 Not hospitalized Must be within 10 days of symptom onset Must not have (new) oxygen requirement due to COVID-19 Must be over the age of 12 and weigh at least 88 lbs At risk for complications for severe COVID-19
High Risk Criteria
• Older age (for example, age ≥65 years of age)
• Obesity or overweight (for example, BMI >25 kg/m2 , or if age 12-17, have BMI ≥85th • Healthcare
percentile for their age and gender providers
• Pregnancy should consider
• Health conditions
the benefit-risk
• Chronic kidney disease
for an individual
• Diabetes
• Immunosuppressive disease or treatment
patient.
• Cardiovascular disease or hypertension • Authorization of
• Chronic lung diseases
under the EUA
• Sickle cell disease
• Neurodevelopmental disorders or other conditions that confer medical
is not limited to
complexity (for example, genetic or metabolic syndromes and severe the medical
congenital anomalies) conditions or
• Having a medical-related technological dependence (for example, factors listed.
tracheostomy, gastrostomy, or positive pressure ventilation)
• Other medical conditions or factors (for example, race or ethnicity) may also place
individual patients at high risk for progression to severe COVID-19
https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medicalconditions.htmlStep 1b: Post-exposure prophylaxis eligibility
● High risk for developing severe illness
AND
● Not fully vaccinated OR are not expected to adequately respond to COVID-19 vaccination
AND
● Have been exposed to an individual infected with COVID-19 OR are at high risk of
exposure because of occurrence of COVID-19 infection in other individuals in the same
institutional settingStep 2: Shared decision making and informed consent 1. Need for use 2. Evidence for use (treatment vs PEP) 3. Benefits 4. Risks 5. Document!
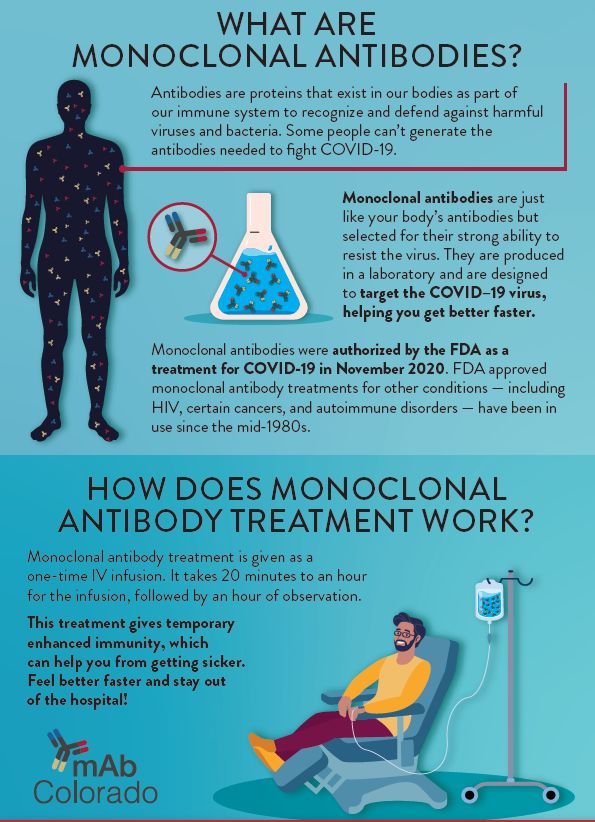
Discuss Monoclonal
Antibody Treatment with
Patients/Care Partners
● Monoclonal antibody treatments are for people who
have tested positive and are experiencing symptoms
but are not so sick they need to be hospitalized or on
oxygen
● You can get antibody treatments even if you have been
Case
vaccinated. However, vaccination protects most people
from getting very sick.
● Depending on how many people need treatment right
now, it might be hard to get you in.
● The treatment is delivered through an IV, which takes
about 20-30 minutes. The nurse will monitor you for any
reactions for about an hour after the IV is complete.
● If you get monoclonal antibody treatment, it is
recommended that you wait 3 months to receive a
COVID-19 vaccine (including a booster)Cases: Ordering challenges in
PALTCStep 3: Place the order!
Bamlanivimab 700mg & Etesevimab 1,400mg
Given IV
Discuss your orders
Less effective for variant COVID strains and treatment plan
with your nursing staff
IV: Via pump or gravity 310mL/hr (21-60min) and leadership teamStep 3: Place the order!
Sotrovimab 500mg Discuss your orders
and treatment plan
Given IV with your nursing staff
and leadership team
Active variant COVID strains
IV: Via pump or gravity 310mL/hr (21-60min)
** Do not administer as an IV push or bolus
*** Not available through federal fundingStep 3: Place the order!
Regen-COV (Casirivimab 600mg/Imdevimab 600mg)
Can be given IV or Subcutaneous Discuss your orders
and treatment plan
Active against variant COVID strains
with your nursing staff
IV: Via pump or gravity 310mL/hr (20-50min) and leadership team
SQ: Divide into 4 separate syringes with 2.5mL in each and administer
in 4 separate locations (back of upper arms, upper thighs, abdomen-
avoid waistline & 2 inches of the navel)
**Can be redosed, if needed for additional exposures, every 4 weeks, at half dose (300mg/300mg)Step 4: Administer and monitor
1. Place at room temperature 20 min prior to
administration (may be kept out up to 4 hours)
2. Administer as directed
3. Monitor resident for 1 hour.
○ Have an E-kit with Epi, diphenhydramine, and
albuterol
○ Monitor vitals!Q&A
PanelYou can also read