COVID-19 Provider's Forum - Harnett Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Harnett Health
COVID-19
Provider`s Forum
January 26, 2021
Presented by:
Dr. Toks Folarin
Harnett Health, CMO
United States
December 1 December 15 January 26
Coronavirus Cases: Coronavirus Cases: Coronavirus Cases:
14,046,293 17,087,922 25,969,418
Deaths: Deaths: Deaths:
276,154 310,095 434,261
Recovered: Recovered: Recovered:
8,287,295 9,963,068 15,697,204
USA USA Total New Total New Active State Cases Cases Deaths Deaths Cases California ,206,941 +7,046 37,639 +112 1,716,765 Texas 2,287,351 +12,046 35,610 +282 377,234 Florida 1,667,763 +9,594 25,675 +229 797,343 Illinois 1,108,430 +3,667 20,853 +109 188,242 New York 1,392,559 +9,397 42,751 +146 821,464 Ohio 879,221 +8,393 13,482 +179 482,465 Georgia 872,919 +4,263 10,856 +88 113,931 Pennsylvania 817,665 +4,000 20,915 +213 158,536 North Carolina 727,423 +3,978 8,776 +56 83,104
COVID-19 HHS
10/20/2020 11/3/2020 11/17/2020 12/1/2020 12/15/2020 1/12/2021 1/26/2021
Tested 2626 2904 2995 3313 3619 NA NA
+ Cases 437 489 530 595 756 1045 1206
+Expired 39 44 49 50 56 72 84
In house 3 12 17 11 26 24 34
positive positive positive positive positive positive positive
7 5 6 13 7 13 0
pending pending pending pending Pending Pending Pending
Employee 230 263 304 353 423 519 545
tested
Employee 28 positive 35 positive 49 positive 61 79 102 126 positive
+ 0 pending 4 pending 5 pending positive positive positive 5 pending
6 7 pending 4 pending
pending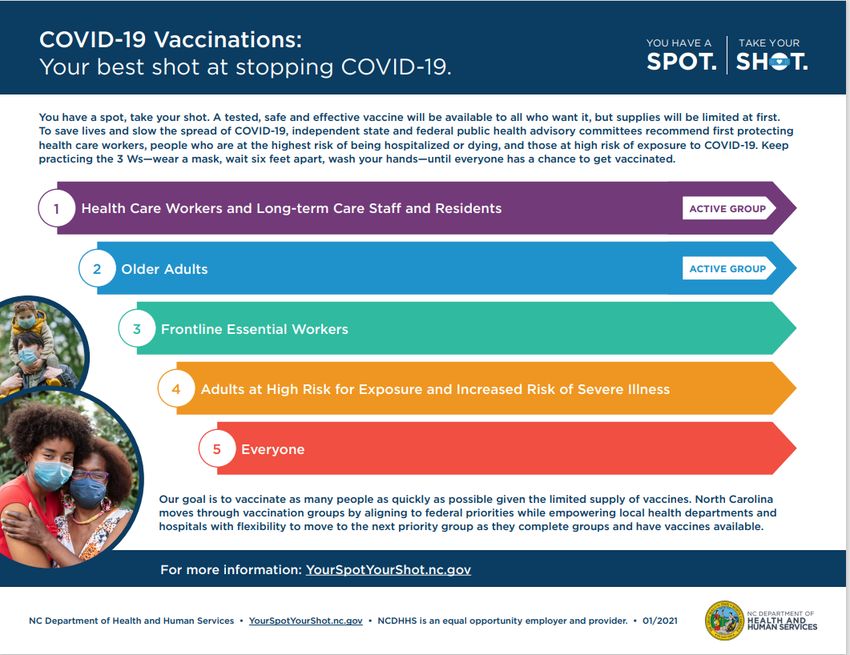
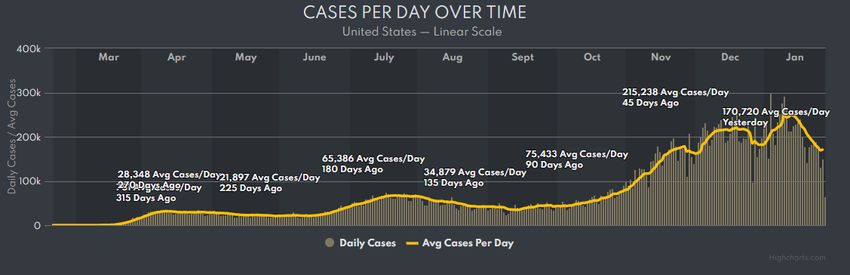
Covid surge- cases
Covid Surge- NC
Coronavirus Vaccine Update
Approved
• Pfizer-BioNTech (BNT162b2) Approved in several countries, EUA in USA, elsewhere
• Moderna (mRNA-1273) Approved in Canada, EUA in USA
• Oxford-AstraZeneca (AZD1222) EUA in UK, elsewhere
Abandoned.
Australia’s vaccine
• The researchers made a small change to the protein, unfortunately, the clamp is similar to
a protein on HIV making HIV-like antibodies. Vaccine trial participants tested positive on
HIV antibody tests, even though they were perfectly healthy.
• Merck Weakened Measles virus, provoked a weaker response than natural infection
• Merck a Vesicular Stomatitis virus pill vaccine, failed to trigger an immune responseVaccine Rollout
• The biggest vaccination campaign in history
• More than 68.1 million doses in 56 countries have been administered
• About 3.44 million doses a day
• In the USA 23.5 million people have received at least one dose of a Covid-19 vaccine
and about 3,481,921 have been fully vaccinated.
• 7.1 doses have been administered for every 100 people, and 57% of the shots distributed
to states have been administered
• The federal government has delivered 44,394,075 doses to states, territories and federal
agencies.
• 2,725,830 people in nursing homes and long-term-care centers had been given first shots.
• Most of the first vaccines have been given to front-line medical workers and nursing
home residents along with above age 65 years
• Every state was granted an amount of the vaccine roughly in proportion to its population.
NC.
• Distributed dose: 41,418,325
• Shots given: 23,461,494
• Doses Used: 57%
• Pct. Of people given a shot: 7.14%HHS Vaccination
Started vaccination on Thursday December 21
HHS deep freezer arrived
Phase 1a
HHS Employee household 75 and older
65 years and older
Second doses
Multiple drives at BJRH and CHH
City of Dunn Community Center this week
HHS vaccine allocation weekly but unpredictable
Total shots given about 6500
Harnett Health compliance
566 Employees/providers have received #1 dose
472 have received bothCOVID -19 section - Harnett Health (myharnetthealth.org)
CDC COVID-19 Response Team
January 26 Update
Morbidity and Mortality Weekly Report MMWR
• Allergic Reactions Including Anaphylaxis after Receipt of the First Dose of
Moderna COVID-19 Vaccine — United States, December 21, 2020–
January 10, 2021
• Early safety monitoring of Moderna vaccine detected 10 cases of
anaphylaxis after reported administration of 4,041,396 first doses of
Moderna COVID-19 vaccine (2.5 cases per million). No anaphylaxis-
related deaths were reported.
• Based on this, anaphylaxis after receipt of Moderna vaccine appears to
be a rare event.
• A previous analysis of the Pfizer-BioNTech COVID-19 vaccine, estimated
an initial rate of 11.1 cases per million doses administered after receipt of
the first dose.
• CDC and FDA will continue enhanced monitoring for anaphylaxis among
recipients of COVID-19 vaccines and will review case reports to VAERS.
• In nine of 10 cases of anaphylaxis after Moderna vaccine, patients had
symptom onset within 30 minutes of vaccination, and nine anaphylaxis
patients also had a history of allergies or allergic reactions, including
some with previous anaphylaxis events.CDC COVID-19 Response Team
• All 10 anaphylaxis cases reported occurred in women.
• A previous review of anaphylaxis reports to VAERS found that 80%
of cases reported in adults involved females, the current finding
could be affected by the observation that more women than men
had received the vaccine during the analytic period (61% versus
36%).
• The clinical and epidemiologic characteristics of anaphylaxis
case reports after receipt of Moderna vaccine are similar to those
reported after receipt of the Pfizer-BioNTech vaccine.
• For both vaccines, symptom onset after vaccination occurred
quickly, usually within minutes.
• A strong female predominance of anaphylaxis case reports exists
for both vaccines.
• Finally, many persons experiencing anaphylaxis after receiving
either vaccine had a history of allergies or allergic reactions, with
several having experienced an anaphylaxis episode in the past.CDC COVID-19 Response Team • Similar patient characteristics in case reports of nonanaphylaxis allergic reactions were observed among the two vaccines. • CDC and FDA will continue to monitor for adverse events, including anaphylaxis, after administration of COVID-19 vaccines and will regularly assess the benefits and risks of vaccination in the context of the evolving epidemiology of the pandemic. • Persons with an immediate allergic reaction to the first dose of an mRNA vaccine should not receive additional doses of either of the two vaccines. • In addition to screening for contraindications and precautions before administering vaccines, vaccine locations should have the necessary supplies and trained staff members available to manage anaphylaxis, implement postvaccination observation periods, immediately treat persons experiencing anaphylaxis signs and symptoms with intramuscular injection of epinephrine, and transport patients to facilities where they can receive advanced medical care.
International Travel Order
• Issued On January 12, 2021
• Requiring all air passengers arriving to the US from a foreign
country to get tested no more than 3 days before flight departure
and to present the negative result or documentation of having
recovered from COVID-19 to the airline before boarding the flight.
• Air passengers will also be required to confirm that the
information they present is true in the form of an attestation.
• This Order is effective as of 12:01am EST on January 26, 2021.
• After You Travel
• Get tested 3-5 days after travel AND stay home for 7 days after
travel.
o Even if you test negative, stay home for the full 7 days.
o If your test is positive, isolate yourself to protect others from getting infected.
• If you don’t get tested, it’s safest to stay home for 10 days after
travel.
• Avoid being around people who are at increased risk for severe
illness for 14 days, whether you get tested or not.International Travel Order • This Order applies to all air passengers, 2 years of age or older, traveling into the US, including US citizens and legal permanent residents. • • The Order does not apply to air passengers flying from a US territory or possession to a US state. (American Samoa, Guam, the Northern Mariana Islands, the Commonwealth of Puerto Rico, and the US Virgin Islands). • The requirements of this Order only apply to air travel into the US. • Testing must be performed using a viral test (NAAT or antigen), and negative results must be presented to the airline prior to boarding. • At this time all air passengers traveling to the US, regardless of vaccination or antibody status, are required to provide a negative COVID-19 test result or documentation of recovery.
New COVID Variant Information about the characteristics of these variants is rapidly emerging. Multiple COVID-19 variants are circulating globally: In the UK, a new variant called B.1.1.7 has emerged with an unusually large number of mutations. • This variant spreads more easily and quickly than other variants. This variant is associated with increased transmissibility (i.e., more efficient and rapid transmission). • Currently there is no evidence to suggest that the variant has any impact on the severity of disease or vaccine efficacy or increased risk of death. • It has since been detected in numerous countries around the world, including the United States and Canada. • About 195 cases reported in the US
New COVID Variant • In South Africa, another variant called 1.351 has emerged independently of the UK variant. • This variant, originally detected in early October, shares some mutations with the variant detected in the UK. • There have been cases caused by this variant outside of South Africa, but it has not been detected in the US. • Currently there is no evidence to suggest that this variant has any impact on disease severity. • There is some evidence to indicate that one of the spike protein mutations, E484K, may affect neutralization by some polyclonal and monoclonal antibodies.1
New COVID Variant
In Brazil, a variant called P.1 emerged
• This variant contains a set of additional mutations that may affect its
ability to be recognized by antibodies. This variant has not been
detected in the US.
• There is evidence to suggest that some of the mutations in the P.1 variant
may affect its transmissibility and antigenic profile, which may affect the
ability of antibodies generated through a previous natural infection or
through vaccination to recognize and neutralize the virus.
• A recent study reported on a cluster of cases in Manaus brazil, in which
the P.1 variant was identified in 42% of the specimens from late
December In this region, it is estimated that approximately 75% of the
population had been infected with SARS-CoV2 as of October 2020.
However, since mid-December the region has observed a surge in cases.
• The emergence of this variant raises concerns of a potential increase in
transmissibility or propensity for SARS-CoV-2 re-infection of individuals.
• This variant has not yet been identified in the United States.Ivermectin
• For decades, ivermectin has served as a potent drug to treat parasitic
worms against river blindness and other diseases, while veterinarians
give dogs a different formulation to prevent heartworm.
• Studies on cells have suggested ivermectin might also kill viruses.
•
In April, Australian researchers reported that the drug blocked
coronaviruses in cell cultures, but they used a dosage that was so high it
might have dangerous side effects in people.
• Since then a number of clinical trials have been launched to see if a safe
dose of ivermectin can fight Covid-19. The results reported so far have
been mixed.
• The N.I.H. Covid-19 treatment guidelines state that there is insufficient
data to recommend for or against the use of ivermectin for the disease,
except in a clinical trial.
• Nevertheless ivermectin is being prescribed increasingly often
especially in Latin AmericaIvermectin NIH Recommendation. Updated: January 14, 2021 The COVID-19 Treatment Guidelines Panel (the Panel) has determined that currently there are insufficient data to recommend either for or against the use of ivermectin for the treatment of COVID-19. Results from adequately powered, well- designed, and well-conducted clinical trials are needed to provide more specific, evidence-based guidance on the role of ivermectin for the treatment of COVID-19. • Ivermectin is an antiparasitic drug that is approved by FDA for the treatment of onchocerciasis and strongyloidiasis. • Ivermectin is not FDA-approved for the treatment of any viral infection. • In general, the drug is well tolerated. It is currently being evaluated as a potential treatment for COVID-19.
•
Ivermectin
Reports from in vitro studies suggest that ivermectin acts by inhibiting the host
proteins, that are part of a key intracellular transport process that viruses hijack to
enhance infection by suppressing the host antiviral response.
• In addition, ivermectin docking in vitro may interfere with the attachment of the
SARS-CoV-2 spike protein to the human cell membrane.
• Ivermectin has been shown to inhibit the replication of SARS-CoV-2 in cell culture.
• However, pharmacokinetic and pharmacodynamic studies suggest that ivermectin
doses up to 100-fold higher than those approved for use in humans would be
required to achieve the plasma concentrations necessary to duplicate the drug’s
antiviral efficacy in vitro
• Even though ivermectin appears to accumulate in lung tissue, with the doses used
in most clinical trials, predicted systemic plasma and lung tissue concentrations are
much lower than 2 µM, the half-maximal inhibitory concentration (IC50) against
SARS-CoV-2 in vitro7
• Ivermectin demonstrates potential anti-inflammatory properties in some in vitro
studies properties which have been postulated to be beneficial in the treatment of
COVID-19Ivermectin
• Since the last revision of the Ivermectin section of the
Guidelines, the results of several randomized trials and
retrospective cohort studies of ivermectin use in patients with
COVID-19 have been published in peer-reviewed journals or
made available as preliminary, non-peer-reviewed reports.
• Some clinical studies showed no benefits or worsening of
disease after ivermectin use,
• whereas others reported shorter time to resolution of disease
manifestations attributed to COVID-19, greater reduction in
inflammatory markers, shorter time to viral clearance, or lower
mortality rates in patients who received ivermectin than in
patients who received comparator drugs or placebo.
• However, most of the studies reported to date had incomplete
information and significant methodological limitations, which
make it difficult to exclude common causes of bias.Ivermectin
The missing information and limitations include the following:
• The sample size of most of the trials was small.
• Various doses and schedules of ivermectin were used.
• Some of the randomized controlled trials were open-label studies in which neither
the participants nor the investigators were blinded to the treatment arms.
• In addition to ivermectin or the comparator drug, patients also received various
concomitant medications (e.g., doxycycline, hydroxychloroquine, azithromycin,
zinc, corticosteroids), confounding assessment of the true efficacy or safety of
ivermectin.
• The severity of COVID-19 in the study participants was not always well described.
• The study outcome measures were not always clearly defined.
• Because of these limitations, the Panel cannot draw definitive conclusions about
the clinical efficacy or safety of ivermectin for the treatment of COVID-19.
• Results from adequately powered, well-designed, and well-conducted clinical
trials are needed to provide more specific, evidence-based guidance on the role
of ivermectin for the treatment of COVID-19.Ivermectin
You can also read