Development At The Speed Of Light: Pharma's Search For A COVID-19 Vaccine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Development At The Speed Of Light: Pharma’s Search For A COVID-19 Vaccine

Agenda
Vaccine landscape and frontrunners
Pipeline snapshot
Who are the frontrunners?
Potential launch timelines and upcoming catalysts
Clinical data – what do we know and what questions remain?
Regulatory hurdles
Compressed clinical development timelines
FDA guidance maintains high standards for pivotal efficacy trials
Enrolling clinically-relevant populations
Optimal clinical trial site selection
Commercialization challenges
How large will vaccine demand be?
Can manufacturing capacity meet demand? (active ingredient + fill-finish)
How can equitable access to a limited supply of doses be achieved?
Pricing dilemma – how to profit without impairing market access?
2
Vaccine landscape

Explosion in industry-sponsored trials as developers race for approval 121 planned or ongoing trials for preventative and therapeutic vaccines Source: Trialtrove, 17 July 2020 informa | Pharma Intelligence 4
Unprecedented interest in vaccine development from both established and newcomer companies 168 pipeline vaccines 22 vaccines in clinical development *Showing top 25 companies 6 technologies - inactivated, viral vector, DNA, RNA, recombinant protein, virus-like particle (VLP) Source: Pharmaprojects, 17 July 2020 informa | Pharma Intelligence 5

Public funding and partnerships have provided an opportunity
for smaller players to evaluate new technologies
Vaccine Company Phase Technology Public funding
AZD1222 University of III ChAdOx1 vector vaccine £65.5m from UK government and up to $1.2bn
Oxford/Vaccitech/AstraZeneca from BARDA
Sinopharm inactivated vaccine Sinopharm (China National III Inactivated vaccine China state-owned
Pharmaceutical Group Corp)
PiCoVacc Sinovac II Inactivated vaccine $8.5m from Chinese government
mRNA-1273 Moderna II mRNA vaccine $483m from BARDA
BNT162 BioNTech/Pfizer/Fosun Pharma II mRNA vaccine €100m from European Investment Bank (Pfizer
has declined US funding)
Ad5-nCoV CanSino Biologics/Beijing Institute II Ad5 vector vaccine R&D support from Chinese Academy of Military
of Biotechnology Medical Sciences
NVX-CoV2373 Novavax I/II Recombinant protein $1.6bn from US government and $384m from
nanoparticle vaccine CEPI
INO-4800 Inovio I/II DNA vaccine $71m from US Department of Defense and
$17.2m from CEPI
Trimer-Tag vaccine Clover/GSK/Dynavax I Spike trimer subunit $69.5m from CEPI
vaccine + adjuvant
CureVac mRNA vaccine CureVac I mRNA vaccine €100m from European Investment Bank and
€300m from German government
Medicago VLP vaccine Medicago/GSK/Dynavax I VLP Undisclosed funding from Canadian government
Imperial College London vaccine Imperial College London I Self-amplifying mRNA £41m from UK government
vaccine
Source: Datamonitor Healthcare, July 2020
informa | Pharma Intelligence 6
Who are the frontrunners?
Front runners with potential 2020 Emergency Use Authorization
Phase I/II
Phase II/III
Possible EUA in October 2020
(September in UK)
Possible EUA in October 2020
Possible EUA in November 2020
Possible EUA by year end
Possible EUA by year end
Possible EUA by year end
Possible EUA by year end
Source: Datamonitor Healthcare, July 2020
informa | Pharma Intelligence 8
Later market entrants will play crucial role in boosting supply
Vaccine Phase Catalyst
NVX-CoV2373 I/II Phase I immunogenicity data expected in July. Phase III to
(Novavax) initiate in Autumn, utilizing Warp Speed funds
Ad26.COV2-S Preclinical Phase I/II trial initiating in July with Phase III targeted for
(Johnson & Johnson) September 2020 and EUA in Q1 2021
Adjuvanted subunit vaccine (Sanofi/GSK) Preclinical Phase I expected in H2 2020, anticipated approval in H2
2021
Measles vector-based vaccine Preclinical Phase I trials in H2 2020
(Merck/Themis)
VSV vector-based vaccine
(Merck/IAVI)
Novavax, J&J, and Merck & Co are part of the “Operation Warp Speed” program. All three have
received US-government funding to fund clinical development and scale up manufacturing capacity
Novavax is targeting 100m doses by the end of 2020, and up to 1bn dose by the end of 2021
J&J is also targeting 1bn doses by the end of 2021 with a single-dose schedule
Merck & Co is ultimately targeting 1bn doses, and replicative nature of viral vectors may facilitate
single-dose schedules
Source: Datamonitor Healthcare, July 2020
informa | Pharma Intelligence 9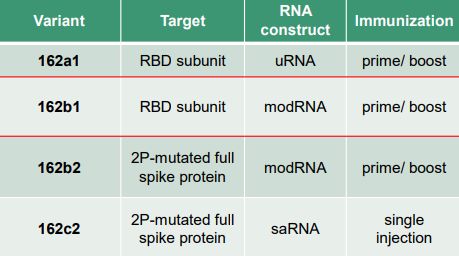
Phase I insights and remaining questions
mRNA vaccines have shown great promise in Phase I
Compelling immunogenicity as measured by neutralizing antibody titers
BNT162b1 (Pfizer/BioNTech) which encodes S protein receptor-binding domain, and mRNA-1273 (Moderna) which encodes
full S protein, have both demonstrated ability to induce neutralizing antibody titers that were comparable to or exceeded
those observed in sera of convalescent patients
Caveat is that serum panels in both studies were primarily from patients with mild-moderate disease, who have lower
antibody titers. Pfizer/BioNTech panel may also not have been at peak of immune response (“at least 14 days after
confirmed diagnosis”) and included individuals older than those who were vaccinated (18-83 years vs. 19-54 years,
respectively). Moderna panel were 23-60 days post-symptom onset, age not specified.
Moderna also released data on cellular immunogenicity showing Th1-biased CD4 T-cell responses without significant
elevation of Th2-biased CD4 T-cell responses
Cellular immunogenicity data are expected from ongoing BioNTech European study, as well as additional data on the three
other constructs being evaluated.
BNT162 constructs under evaluation
Vaccine (Phase III Vaccine GMTs Convalescent
dose) sera Nab GMTs
BNT162b1 (30ug) 267 94
(Day 28; PRNT50)
mRNA-1273 (100ug) 654 (Day 43, PRNT80) 158 (n=3)
344 (Day 57, PsVNA ID50) 109 (n=38)
Source: BioNTech, July 2020; Moderna, July 2020
informa | Pharma Intelligence 11Key remaining questions:
Will antibodies/T-cell responses confer protection?
Correlates of protection are still unknown meaning there is no guarantee that immunogenicity will translate into protective
efficacy in pivotal studies
How durable are neutralizing antibody responses?
Follow-up has been limited to one month post-vaccination thus far. If responses are not durable, intra-season protection
could be compromised and seasonal vaccination may be required
Will similar immunogenicity be observed in elderly, ethnic minorities, and patients with co-morbidities?
Both studies were limited to healthy adults aged 18-55 years, but the elderly is a key risk group and immune responses tend
to be lower due to immunosenescence. Future pivotal studies aim to enrol diverse patient groups considered at high-risk
Reactogenicity a potential weakness?
Severe fatigue and severe chills occurred in one patient each in BNT162 30ug arm (post-2nd dose), and severe erythema was observed
in 1 patient in mRNA-1273 100ug arm (post-2nd dose). Highest doses discontinued due to high frequency of severe adverse events.
Not a barrier to approval, but could emerge as a weakness if other approaches are less reactogenic. We note that all adverse events in
Inovio’s Phase I trial (INO-4800, n=40) were mild.
Source: Datamonitor Healthcare
informa | Pharma Intelligence 12Mixed data for adenoviral vector vaccines thus far
CanSino Ad5 vaccine immunogenicity impaired by pre-existing anti-vector antibodies
Disappointingly low rates of seroconversion for neutralizing antibodies to live SARS-CoV-2 observed in 108 healthy adults
aged 18-60 years, though T-cell responses were observed
Single dose administered at three dosing levels (5x1010 vp/ml, 1x1011 vp/ml, 1.5x1011 vp/ml)
Pre-existing anti-vector antibodies compromised immunogenicity of the vaccine. In addition, recipients aged 45-60 years had
lower neutralizing antibody titers than younger participants.
Neutralizing antibodies (live Low dose (n=36) Middle dose (n=36) High dose (n=36)
SARS-CoV-2 assay)
GMTs (day 28) 14.5 16.2 34.0
≥4-fold increase (day 28) 18 (50%) 18 (50%) 27 (75%)
Highest dose (1.5x1011 vp/ml) discontinued due to higher frequency of severe adverse events (17%)
Positive Phase I data for AZD1222, but preclinical model suggests it may only provide partial protection
Phase I data from 500 subjects showed stimulation of both humoral and cellular immunity after a single dose
However, preclinical challenge study in six rhesus macaques showed that the vaccine did not prevent infection, but did provide
protection from pneumonia compared to unvaccinated controls. No difference in viral loads in nose swabs also suggests vaccine
will not prevent individuals transmitting the virus, which has implications for efforts to achieve herd immunity
Source: Doremalen et al., 2020; Zhu et al., 2020
informa | Pharma Intelligence 13Regulatory requirements
Some helpful definitions for the next slide… Probability of Success (PoS): The probability of successfully advancing from one clinical stage to another, or from NDA/BLA to approval. PoS is expressed as a percentage. It represents the percentage of products that successfully transitioned through a phase, divided by the number of products in that Phase that have undergone a Phase transition (either successfully or unsuccessfully). For example, if there were 100 drugs in Phase II development and 50 transitioned to Phase III, 20 were suspended and 30 remained in Phase II development, the probability of success would be: 50/70 = 71.4%. Likelihood of Approval (LOA): The probability of a drug gaining FDA regulatory approval from its current phase of development. For example, if a drug is currently in Phase II, and the probability of success for Phase II is 30%, Phase III is 50%, and NDA/BLA is 80%, then the likelihood of approval for the Phase II drug would be: (30%*50%*80%) = 12% Source: Pharmapremia, July 2020 informa | Pharma Intelligence 15
Urgency has led to unprecedented compression of clinical development timelines Average clinical development duration for vaccines is 11 years Average likelihood of approval for a a Phase I vaccine is 16.5% Pfizer/BioNTech, Moderna, CanSino, and AstraZeneca/University of Oxford have all progressed from Phase I to Phase III within 2–4 months, with fastest possible approval within a 5-month clinical development timeframe (Pfizer/BioNTech) BUT… regulators are rightly insisting on large-scale trials, in at-risk patients, with robust efficacy and safety endpoints Source: Pharmapremia, July 2020 informa | Pharma Intelligence 16
FDA guidance sets a rigorous standard for clinical trial design
“There are currently no accepted surrogate endpoints that are reasonably likely to predict clinical benefit
of a COVID-19 vaccine. Thus, at this time, the goal of development programs should be to pursue
traditional approval via direct evidence of vaccine safety and efficacy in protecting humans from SARS-
CoV-2 infection and/or clinical disease.”
Key requirements/recommendations:
Trial size recommendations: Several thousand participants required to have reasonable probability of demonstrating protective
efficacy. Moderna/AstraZeneca/Pfizer pivotal trials are targeting 30,000 patients each
Must enroll ‘at-risk’ patients: This includes the elderly, ethnic minorities, and patients with relevant co-morbidities. This is
essential for both clinical relevance and to maximize the probability of demonstrating efficacy
Acceptable efficacy endpoints: Either laboratory-confirmed COVID-19 or laboratory-confirmed SARS-CoV-2 infection is an
acceptable primary endpoint. Reduction in severe COVID-19 disease should be evaluated as a secondary endpoint (if not a
primary endpoint), and incidence of both symptomatic and asymptomatic infections should be evaluated.
Required safety endpoints: Solicited local and systemic AEs for at least 7 days after vaccination, unsolicited AEs for at least 21–
28 days after vaccination, and serious and other medically attended AEs for at least 6 months after final dose
Follow-up: At least 1–2 years to gauge longevity and potential for vaccine-associated enhanced respiratory disease
Comparator: Placebo control arm is necessary, but active comparators may be possible in future
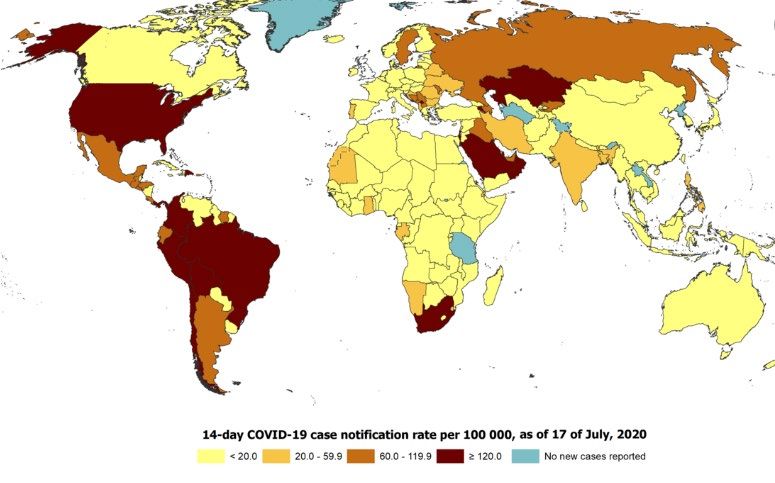
Source: FDA, June 2020 informa | Pharma Intelligence 17Choice of clinical site locations must reflect changing
epicenter of the pandemic
14-day cumulative reported COVID-19 cases per 100,000
Trial site selection is crucial to
ensure a high enough COVID-19
attack rate in the placebo arm to
be able to demonstrate vaccines
have statistically significant
protective efficacy
Brazil, Chile, Russia, South Africa,
Saudi Arabia, UAE, and US are sites
in announced pivotal trials
Source: ECDC, July 2020 informa | Pharma Intelligence 18Key Commercialization Challenges
Key challenges:
How large will vaccine demand be?
Which risk groups are likely to be prioritized? WHO suggests 24% of global population (~1.9bn) fall into highest priority groups
(healthcare workers, elderly, and individuals with certain co-morbidities such as diabetes and hypertension)
What coverage rates are required for herd immunity? What coverage can be realistically achieved? Will public perception be
affected by rushed development process and declining case numbers in some markets?
Can manufacturing capacity meet demand (both active ingredient and finish-fill capacity)?
Significant CEPI and BARDA investments have allowed manufacturers to partially de-risk scale up process ahead of demonstrating
proof-of-concept
Competition for finish-fill capacity could be a major hurdle. Manufacturing demand for therapeutics must also be considered
How can equitable access to a limited supply of doses be achieved?
Nationalistic agreements with manufacturers to secure supplies in advance will inevitably result in lower-income markets losing out
Supranational national initiatives such as COVAX (ACT-Accelerator vaccines pillar) which aims to secure 2bn doses by 2021, and the EU
Emergency Support Instrument will play crucial roles in ensuring equitable access, though the former is still far off fundraising target
($18.1bn)
What is an appropriate price to balance need for profitability with ensuring market access?
Traditional HTA processes are too slow and required data may not be available, thus short-term price agreements will be necessary
Prices must reflect substantial public investment in the R&D process and lesser ability to pay of lower-income markets
Initial altruistic approaches of certain companies could act to set short-term price cap for rivals with greater focus on profit
Possible seasonal recurrence/annual vaccination has implications for longer-term profitability
Source: UN Population Prospects, 2019; WHO, 2020
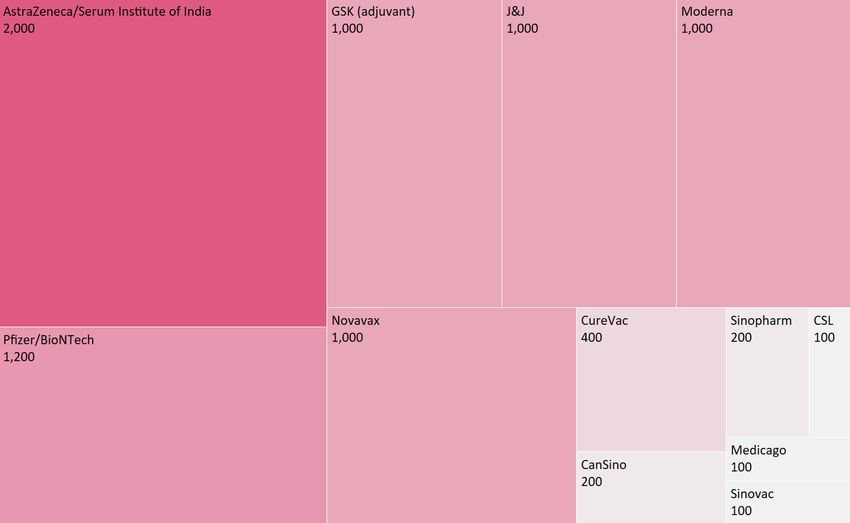
informa | Pharma Intelligence 20Vaccine supply estimates by end of 2021 = 8.3bn doses*
*Figure only includes
estimates from
companies which have
explicitly stated a
targeted dose capacity
in 2021
Source: Company statements
informa | Pharma Intelligence 21Thank you Questions? Email: pharma@informa.com
You can also read