CVS Caremark: An Alarming Merger, Two Years Later
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CVS Caremark:
An Alarming Merger,
Two Years Later
How the CVS-Caremark merger increases health plan
costs, creates obstacles to oversight, and threatens
patient privacy
An Update on Change to Win’s Report:
CVS Caremark: An Alarming Prescription
November 2009
5
Change to Win is a six million member partnership of unions founded in 2005 to represent workers in the industries and occupations of the 21st century economy. Change to Win is committed to restoring the American Dream for a new generation of workers—wages that can support a family, affordable health care, a secure retirement, and opportunity for the future. www.ChangeToWin.org Alarmed About CVS Caremark is a Change to Win initiative to educate health plan managers and trustees as well as consumers about CVS Caremark, now the country’s largest pharmacy benefits manager (PBM) and largest retail pharmacy chain. This report details the troubling patterns exhibited by both CVS and Caremark prior to their merger, and explores the new risks presented by the merged entity CVS Caremark, in such vital areas to health plans and consumers as patient privacy, patient health versus PBM profits, value to plans, conflicts of interest, and quality of service. Change to Win represents workers in CVS Caremark plans that cover more than 10 million people. On behalf of these health plan members, our initiative seeks legislative reform of the PBM industry to protect plan members’ health and privacy. www.AlarmedAboutCVSCaremark.org info@alarmedaboutcvscaremark.org
CVS Caremark:
An Alarming Merger,
Two Years Later
How the CVS-Caremark merger increases health plan
costs, creates obstacles to oversight, and threatens
patient privacy
An Update on Change to Win’s Report:
CVS Caremark: An Alarming Prescription
November 2009
Table of Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
I. CVS Caremark’s Business Model Drives Up Costs and Reduces Quality . . . . . . . 2
A. Driving PBM Clients into CVS stores . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
B. CVS Drives Up Costs Through Drug Switching . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
C. CVS Caremark Pushes Expensive Medications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
D. Profit-Driven Drug Reclassification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
E. Keeping the Difference: Pricing Disparities that Favor CVS Caremark . . . . . . . . . . 7
F. Audits Raise Concerns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
G. Federal Employee Benefits Program Has the Highest Drug Cost
of Any Federal Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
II. CVS Caremark’s Strong Resistance to Transparency . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
A. CVS Caremark Loses Significant Contracts to More Transparent PBMs . . . . . . . . . . 11
B. CVS Caremark Takes Legal Action and Pressures Clients to keep
Taxpayer-Funded Contracts From the Public . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
C. CVS Caremark Opposes Legislative Action Supporting Transparency . . . . . . . . . . . . . . 14
III. CVS Caremark’s Unparalleled Access to Patient Data
and Potential Threats to Privacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
A. Using Private Patient Information for Unsolicited Marketing . . . . . . . . . . . . . . . . . . 15
B. Settlements with the FTC and HHS Office of Civil Rights on
Improper Disposal of Medical Information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
C. Consent Agreement with State of California on Privacy and Expired Goods . . . . . . 17
IV. Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Introduction
THE 2007 MERGER of CVS and Caremark Rx brought together the country’s larg-
est retail pharmacy chain and second-largest pharmacy benefit manager (PBM). After
the merger, the company became a healthcare behemoth. CVS Caremark is the nation’s
largest purchaser of drugs, fills or manages nearly one in every three prescriptions in the
nation, and counts one of every two Americans as a customer.1 The merger provides the
combined company unprecedented access to patient and pricing data that it may be us-
ing to increase its own profits at the expense of health plan sponsors and patients.
In November 2008, Change to Win released CVS Caremark: An Alarming Prescription,
How CVS Caremark may be putting patient privacy at risk, putting profits over
patient health, and taking advantage of its clients,2 a report that detailed over a decade
of questionable and allegedly illegal practices by CVS Caremark and its predecessor
companies. The report also outlined the new risks presented by the merged retail drug-
store and PBM company in areas vital to health plans and consumers such as as patient
privacy, patient health versus PBM profits, value to plans, conflicts of interest, and
quality of service.
Since the report’s release, clients and consumers have seen firsthand the negative im-
pacts Change to Win predicted of the CVS Caremark merger, often on an even larger
scale than expected. Change to Win has also undertaken an ambitious PBM reform ini-
tiative, engaging health plans and consumers as well as regulators and legislators in an
effort to make the PBM industry more accountable and transparent. As patients, plans,
and pharmacists have shared their experiences, more evidence has surfaced that the
CVS Caremark merger has negative consequences for healthcare payers and consumers.
As the country contemplates healthcare reform, this report seeks to demonstrate that
CVS Caremark is quietly using its power as a market leader to squeeze the prescription
drug distribution chain for savings while not passing these savings on to plans and
patients. The results of this activity may:
• Drive up costs for health plans and reduce quality for patients
• Reduce transparency and hamper oversight for health plans
• Compromise the privacy of health plan participants
Fortunately, CVS Caremark’s conduct has caught the attention of Attorneys General and
local regulators around the nation. In fact, the Federal Trade Commission (FTC)
recently began investigating CVS Caremark after receiving expressions of concern from
health plans, independent pharmacists, and consumer groups.3 In addition, five U.S.
Senators and over a dozen members of the House of Representatives have asked the FTC
to investigate the potential anti-competitive effects of the merged retail-PBM business
model and evaluate the potential risks for consumers and health plans when such a large
portion of the pharmaceutical supply chain is controlled by one company.
1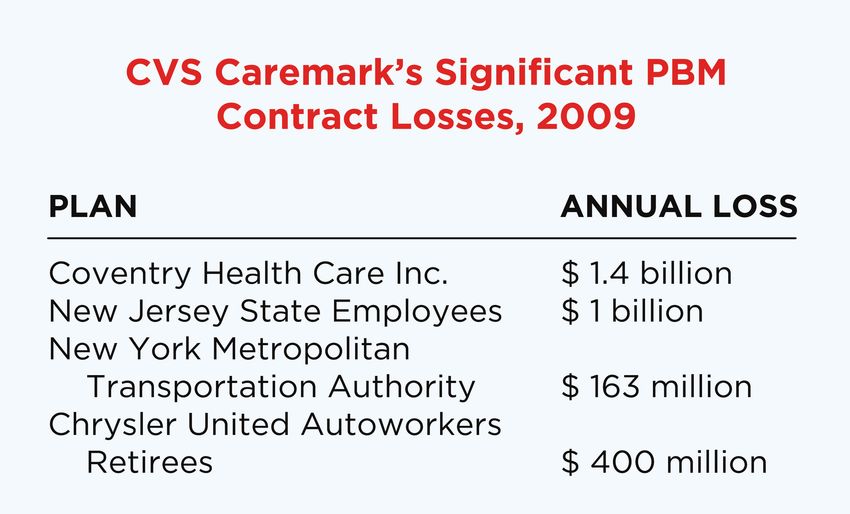
I. CVS Caremark’s Business Model Drives Up Costs
and Reduces Quality
CVS Caremark, the combined drugstore-PBM giant, has relationships with over 150
million consumers, one of every two Americans, and has access to data on 30 percent of
all prescriptions in the United States. CVS Caremark’s mammoth size and scope give it
an unmatched ability to influence consumers, health plans, doctors, and drug
manufacturers, and to drive up costs.
The combination of a PBM and drug retailer puts together two businesses that have
inherent conflicts of interest. As a PBM, CVS Caremark is expected to save health plans
money by negotiating lower drug prices with manufacturers and by promoting lower-
cost drugs to participants, while ensuring that plan participants have access to medicine
in a broad pharmacy network. As a retailer, CVS Pharmacy has an incentive to drive
plan participants into its stores so it can fill the maximum number of prescriptions,
particularly those with high markups, and has little incentive to help save health plans
money. Pressuring health plan participants to fill prescriptions at CVS also has the
intended consequence of increasing retail sales of other, more profitable items, like soda
and candy, which certainly do not serve the interests of healthcare. CVS Caremark
employs the most pharmacists and nurse practitioners of any corporation in the nation,
yet pharmacists report that they barely have time to counsel patients because they have
to meet quotas at the retail store. To make matters worse, CVS Caremark is requiring
pharmacists to use some of their scarce time with patients to urge them to consolidate
all of their prescriptions at CVS.
Pharmacies can act as a check on
PBMs, but the merged CVS
Caremark seemingly has little
interest in limiting its own PBM’s
profits. The merger thus creates a
model for pharmacy benefits that
may decrease health plans’ ability
to provide affordable, quality care
to their members. In its new
incarnation, CVS Caremark is not
just focused on influencing
consumers—it could be tilting the
prescription drug market in its
favor behind the scenes. Both the retail and PBM segments of the company may have
access to information on their competitors through CVS Pharmacy’s contracts with
other PBMs and Caremark’s PBM contracts with other pharmacies – information that
would give CVS Caremark an unfair advantage over both its competitors and its clients.
Finally, CVS Caremark’s practice of working closely with pharmaceutical manufacturers
to promote their blockbuster drugs may be all the more profitable after the merger.
2
Now, in addition to collecting the health plan’s payment for an expensive brand-name
drug, Caremark may be able to manipulate the reimbursement rate to CVS Pharmacy in
order to collect a higher profit.
A. Driving PBM Clients into CVS Stores
One way CVS Caremark is capitalizing on the merger is by driving Caremark clients into
CVS Pharmacies to purchase their prescription drugs as well as the thousands of other
products available in the stores.
CVS Caremark often uses PBM-related programs to drive plan participants into CVS
Pharmacy stores to increase store sales. For example, some PBM contracts have
provisions that automatically enroll PBM plan members in a version of CVS Caremark’s
loyalty program, ExtraCare, after which they receive an ExtraCare Health card in the
mail.4 Highly-touted by the Company as the largest loyalty program in the world with
over 50 million members, the ExtraCare card entitles card holders to in-store product
discounts on a variety of items from CVS brand over-the-counter medications or laundry
detergent to unhealthy soda and snack food.5
CVS Caremark also works to increase CVS Pharmacy sales, by urging Caremark plan
members to obtain prescription refills at CVS stores, consolidate all their prescriptions
at CVS, and switch from competing pharmacies to CVS.6 As CVS increasingly builds its
pharmacy market share by leveraging its PBM relationships, health plans may be less
able to negotiate good contracts for their members, and patients’ choices may suffer.
B. CVS Drives Up Costs Through Drug Switching
As we discussed in our previous report, PBMs have significant power in selecting the
medications patients receive because they determine the formulary list of “preferred”
drugs for plan members and engage in drug interchange, the practice of switching a
patient from a specific drug prescribed by their doctor to another drug that is
“preferred” by the PBM.7 While substituting a therapeutically-equivalent generic for a
name brand drug is a cost-effective form of drug switching, CVS Caremark and its
predecessor companies have been repeatedly accused of favoring drugs and improperly
switching patient medications in ways that increase the costs to plans or patients. In
2008, CVS Caremark paid out over $75 million to settle lawsuits that included improper
drug switching claims.8 As a result of these lawsuits and others, the company currently
operates under several agreements with state and federal agencies that regulate the
company’s practices involving rebates from drug manufacturers, management of its
formulary and preferred drug lists, contracts with retail pharmacies, and drug
interchange programs.9
Despite those high profile settlements, evidence has emerged that CVS Caremark has
continued to switch drugs and raise costs. Claim histories demonstrate that CVS
Caremark continues to reject claims for some generic medications in favor of more
3
expensive name brand drugs, for which they may receive payments from drug
manufacturers. This practice drives up prescription costs for health plans and co-pays
for patients. For example, CVS Caremark has recently rejected claims for generic Ocella,
a birth control medication. These claim rejections instructed pharmacists to substitute
the “preferred drug” Yasmin, which is the higher cost name brand version of the drug.10
In another instance, CVS Caremark rejected a patient’s claim for generic Aderall
(Dextroamp-Amphet ER), a medication used to treat Attention Deficit Hyperactivity
Disorder, and directed the pharmacist to fill the prescription with the more expensive
brand name drug, Adderall XR.13 These recent examples of switching a more expensive
brand drug for a prescribed generic belie CVS Caremark’s stated commitment to
reducing drug costs and could violate CVS Caremark’s obligations under multiple
consent agreements.
C. CVS Caremark Pushes Expensive Medications
CVS Caremark has also been accused of drug pushing, the practice of promoting specific
brand drugs to patients and/or doctors at the behest of large pharmaceutical producers
who compensate CVS Caremark for the promotion. CVS Caremark’s deals with drug
manufacturers to promote expensive brand name drugs conflict with its responsibility as
a PBM to save its clients money by negotiating lower drug prices with those same
pharmaceutical companies. Last year, doctors protested CVS Caremark’s practice of
sending them letters with the names of their diabetic patients listed, recommending
they prescribe Merck’s new diabetes drug Januvia,14 which is 5 to 10 times more
expensive than generic options.15
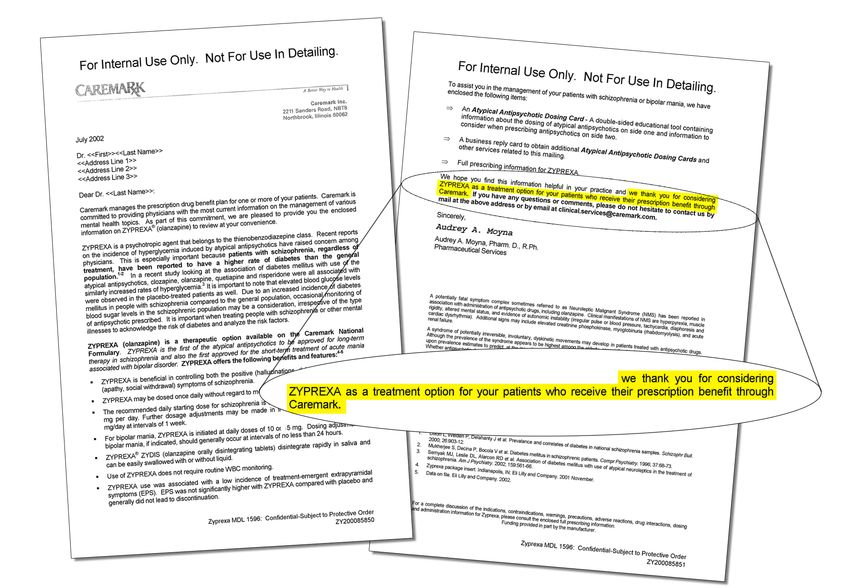
A recent lawsuit against Eli Lilly revealed that a CVS Caremark subsidiary, AdvancePCS,
offered to send 120,000 letters to doctors promoting Eli Lilly’s antipsychotic drug
Zyprexa for $5 per letter.16 At the same time Eli Lilly was trying to increase profits by
allegedly downplaying Zyprexa’s health risks and marketing it for uses not approved by
the FDA.17 Emails between Lilly and CVS
Caremark show that officials at the two
companies worked together to develop
content for the physician letters.18
In October 2009, the Indianapolis Star
published an in-depth article depicting CVS
Caremark’s continuing collaboration with
drug manufacturers to use patients’ private
health information for deceptive marketing
purposes. Letters mailed to physicians
promoting drugs including Lilly’s
controversial Cymbalta antidepressant are
“designed to look like the informational
mailings you often get from pharmacy
management firms that tell you things
4
about your prescribing patterns as a
physician, or about problems with a certain
group or class of drugs, so in that sense, it is
designed to be deceptive,” according to Dr.
Howard Brody, a director for the Institute for
the Medical Humanities at the University of
Texas in Galveston.19
Dr. Jack Freer, Associate Director of the
Center for Clinical Ethics and Humanities in
Health Care at the University of Buffalo told
the Star, “Benefits companies are using
patient information as a commercial pitch to
drug companies. Is it an abuse of that
relationship? Of course it is.”20
CVS Caremark now has information on 30% of all prescriptions filled in
the U.S. and uses the data for purposes like promoting drugs to doctors.
5
The conflicts of interest inherent in collaboration between a PBM and a drug
manufacturer are exacerbated by the CVS-Caremark combination. After the merger, the
company has information on 30 percent of all prescriptions filled in the country and
uses the data for purposes like the Zyprexa, Cymbalta and Januvia doctor letters. Lost in
the leveraging of CVS Caremark’s unprecedented access to patient data are the financial
and health care interests of health plans and patients.
D. Profit-Driven Drug Reclassification
As we detailed in our previous report, there are many ways in which CVS Caremark may
be using its PBM-drugstore model to inflate its profits at the expense of patients, health
plans, and competitors. One example of this problem is the company’s apparent efforts
to drive its PBM customers to CVS stores to fill their most expensive prescriptions.
There is mounting evidence suggesting that CVS Caremark steers the most profitable
Caremark prescriptions to CVS pharmacies by including exclusive provider language
for “specialty” medications in its PBM contracts and then reclassifying costly drugs
as “specialty” medications. Although there is no regulated definition of “specialty
medications,” typically they are drugs prescribed for chronic or complex conditions
such as cancer, anemia, HIV/AIDS, hepatitis C, multiple sclerosis, growth hormone
deficiency, and hemophilia that typically require special dosing or administration (e.g.,
injectables), special handling (e.g., refrigeration), and/or particularly close monitoring
of the patient.
Although specialty drugs represent a small number of total prescriptions dispensed,
they make up a disproportionate segment of expenditures because each dose can cost
thousands of dollars.21 While prescription drug costs have risen sharply across the
board, the cost of specialty drugs has been rising far faster. The wholesale price of
specialty drugs rose nearly nine percent in 2007, three times the rate of inflation.22
During the same year, the cost of branded drugs rose seven percent and the price of
generic drugs fell by ten percent.23 Specialty drugs also make up an increasing share
of prescription drug expenditures for health plan sponsors. CVS Caremark reported
in its 2008 TrendsRx report that specialty pharmacy spending grew from 9.9% of the
company’s book-of-business in 2007 to 13.4% in 2009.24 Given the lack of a regulated
definition of specialty drugs, CVS Caremark is able to manipulate its classification of
specialty medications to suit its profit-driven motives.
It appears as though CVS Caremark uses specialty drugs as one way to increase profits
by inserting clauses into its PBM contracts that grant it exclusive provider status
for plan members’ specialty medications. This has allowed CVS Caremark to drive
its clients’ members’ most profitable prescriptions to its own mail order specialty
pharmacies. The contract between CVS Caremark and the Los Angeles Unified School
District states, “Caremark shall be the exclusive provider of Specialty Drugs.”25
6Moreover, a pharmacists’ advocate, who is also a pharmacist by training, explains
that he and his colleagues initially observed that Caremark referred to refrigerated
injectable medications as “specialty” drugs, and required those to be filled exclusively by
Caremark – even though every pharmacy in the state is required to have a refrigerator.
Then Caremark began classifying high-cost oral oncology drugs like Gleevec, which
costs around $3000, as “specialty” medications, even though they do not require any
special care or administration. According to this pharmacist, Caremark tends to classify
medications costing approximately $500 and higher as specialty drugs, even including
oral tablets that do not require any special handling or monitoring by pharmacists or
prescribing physicians. For example, Coumadin, a popular blood thinner, costs about
$35 per month; however, Caremark does not classify it as a specialty medication, even
though patients taking Coumadin have to be monitored on a monthly basis.26
CVS Caremark Leads in Profits Per Prescription Filled
CVS Caremark has the highest
profit margins in the
industry. Over the two
fiscal years that the merged
company has operated, CVS
earned $3.94 in gross profit
per prescription filled,
amounting to 37% more in
profit per prescription than
its nearest competitor, Medco
Health Solutions Inc., and 57%
more in profit than the third
largest PBM, Express Scripts.27
E. Keeping the Difference: Pricing Disparities that Favor CVS Caremark
PBM critics point to a system known as “spread pricing” as one major example of PBMs
retaining profits rather than passing them on to plan sponsors. PBMs often charge
health plans more for a prescription claim than they reimburse the pharmacy filling the
prescription, with the PBM pocketing the difference. The potential for a PBM to take
advantage of spread pricing unbeknownst to the health plan is greatly enhanced when
the retail pharmacy and PBM are the same company.28
Some patients have also reported spiking costs when they are required or encouraged
to switch to CVS pharmacies. A woman in North Carolina paid $300 more for fertility
7treatments at CVS than she would have if she were paying full retail price at another
local pharmacy.29 Non-CVS pharmacists report that CVS Caremark’s new Provider
Agreement for network pharmacies prohibits pharmacies from sharing reimbursement
information with their patients, making it more difficult for patients to alert their plans
to the company’s spread pricing practices.
Even more troubling, with this PBM-retailer model, one can imagine a scenario in which
CVS Caremark is able to reimburse its own pharmacies at a very low rate for filling
Caremark prescriptions, and take a loss at retail while benefiting its PBM business by
pocketing a hefty “spread” that is hidden from the plans. That is, because of a lack of
transparency in the mechanics of these transactions, it is possible that Caremark could
then turn around and charge the plan more for the drug than what CVS was paid to fill
the prescription. On the other hand, non-CVS pharmacies may not be able to accept
reimbursement rates that are at or below the cost of the drug, leading to fewer pharmacy
choices for health plans and consumers.
F. Audits Raise Concerns
As we detailed in our last report, numerous CVS Caremark clients have accused
the company of withholding money that the plans themselves were entitled to or of
engaging in deceptive or fraudulent practices that ended up increasing client costs. In
2006, the United States Office of Personnel Management identified over $13 million in
overcharges to the Federal Employees Health Benefits Program (FEHBP) by Caremark’s
predecessor, AdvancePCS, for the years 2000 through 2005.30 These accusations have
continued in 2009, as recent audits completed by several concerned CVS Caremark
clients have revealed new evidence of plan overcharging, resulting in clients recovering
millions of dollars from the company.
• New York Metropolitan Transportation Authority (MTA): A partial
audit of CVS Caremark’s contract with the MTA turned up nearly $1 million in
overcharges. According to the office of MTA Inspector General Barry Kluger, a
“second and independent” probe has
been launched and the total amount of
overcharges could increase as MTA staff
continue to pore over records. The MTA
announced in June that it plans to end
its relationship with CVS Caremark
and expects to save $50 million under
a new PBM contract with Innoviant.31
• State of Maryland: According to an
audit released in February 2009 by
the Maryland Department of Legisla-
tive Services, while CVS Caremark
managed pharmacy benefits for the
state from 2004 to 2007 it collected
8more than $10 million in potential overpayments and undisclosed rebates. In
2007, Maryland replaced CVS Caremark with Catalyst, a smaller, transparency-
oriented PBM.32
• First Medical Health Plan, Puerto Rico: In January 2009, First Medi-
cal Health Plan, the largest insurer of government employees in Puerto Rico,
sued CVS Caremark for breach of contract. An audit conducted for First Medical
Health Plan discovered that CVS Caremark had overcharged the plan and with-
held rebates. The plan is seeking to recover approximately $34 million.33
Given CVS Caremark’s experience with audits that reveal millions of dollars in
overcharges and misclassified rebates, it is no wonder that the company erects barriers
to auditing in its contracts and fights clients who seek to audit their contracts with
CVS Caremark. For example, in a contract between CVS Caremark and the State of
New Hampshire, the company places significant restrictions on plan-initiated audits,
stating that the plan “is not entitled to audit agreements with vendors, pharmaceutical
companies, participating pharmacies or other providers of products or services to
Caremark.” Further, the contract gives Caremark the right to veto a plan’s choice of
auditor and bars plans from using auditors who are currently involved in litigation
against Caremark, even including any that are providing testimony.34
FTC Called on to Investigate Legality of CVS-Caremark Merger
There is growing consensus among health plans, plan participants, and
government officials that the CVS Caremark merger, and the new drugstore-
PBM model for pharmacy benefit services that it represents, threatens access
to affordable, high-quality prescription drug services. Because of these
concerns, a number of lawmakers and health plans have submitted letters to
the Federal Trade Commission asking the agency to investigate whether the
merger violates U.S. anti-trust laws and harms both health plan sponsors and
American consumers.
The merger between one of the
country’s biggest PBMs and the
country’s largest drugstore chain has
created the nation’s largest provider
of prescription services and may pose
serious risks for consumers and health
plans. The merged entity presents
potential risks in such vital areas as
patient privacy, drug cost to health
plans and consumers, and conflicts of
interest that result in anti-competitive
behavior and may violate American
anti-trust laws.
9In a letter to the FTC Chairman in July, Senators Byron Dorgan (D-N.D.), Russ
Feingold (D-Wis.) and Amy Klobuchar (D-Minn.), expressed their concern
about the CVS Caremark merger, stating that the PBM-retail pharmacy
combination “created a heightened opportunity for anticompetitive conduct
in the prescription drug market.”35 In a similar letter to the FTC, Senators Mark
Pryor (D-Ark.) and Roger Wicker (R-Miss.) urged the FTC to “take appropriate
action if CVS Caremark is engaging in any anticompetitive or deceptive
practices.”36 More than a dozen members of the House of Representatives
have issued similar letters to the FTC calling for an investigation of the
impacts of the CVS Caremark merger on American consumers.
In a Senate Finance Committee debate on PBM transparency provisions in
health care reform, Sen. Maria Cantwell (D-Wash.) also highlighted problems
with CVS Caremark: “I would be more than happy if the Judiciary Committee
looks into CVS, which is now becoming one of the largest deliverers of drugs
in America and that there could possibly be an antitrust issue here if they
then end up dominating the market and then passing their own savings on to
themselves.”37
G. Federal Employee Benefits Program Has the Highest Drug Cost of Any
Federal Plan
CVS Caremark manages 80% of pharmacy benefits for health plans within the Federal
Employees Health Benefits Program (FEHBP), which covers eight million federal
employees, dependents, and retirees, and spends over $10 billion on prescription drugs
annually.38 FEHBP carriers’ contracts with CVS Caremark lack basic transparency
provisions and appear to be a bad deal for the taxpayers who foot the bill.39 In fact,
the FEHBP spends 15 to 45 percent more for prescription drugs than other federal
programs40 and the annual FEHBP prescription claim cost per member nearly doubled,
from $591 to $1,161 between 1999 and 2007.41
In contrast, the Department of Defense’s
TRICARE health plan, covering over five
million military personnel and their families,
has changed the way it handles drug benefits
in recent years, and through these reforms
has achieved greater oversight and control
of its drug spending along with access to
federal drug discounts.42
CVS Caremark manages drug benefits
for the Blue Cross Blue Shield Federal
Employee Program, which covers more
than half of all FEHBP enrollees. This
10plan will increase premiums 15 percent for self-only coverage and 12 percent for family
coverage for 2010.43 The Government Accountability Office has cited rising drug costs as
one of the primary drivers of increased premiums for FEHBP health plans.44
The House Committee on Oversight and Government Reform’s Subcommittee on
Federal Workforce, Postal Service, and the District of Columbia is currently reviewing
options for structural reform of the FEHBP drug benefit that would enable the
government to lower costs and achieve greater oversight.45
In a hearing held in June, Subcommittee Chairman Rep. Stephen Lynch (D-Mass.) said
that “Some research even shows that Costco and Drugstore.com offer better prices for
drugs [than the FEHBP]. . . in spite of the fact that the federal program has the buying
power of 8 million members. That’s especially troubling.”46
In the same hearing, the Inspector General of the Office of Personnel Management,
the federal agency that administers the FEHBP, testified that the current hands-
off approach to the drug benefit has created cost structures that are “utterly
nontransparent,” a condition that “invites bad pricing and contracting practices.”47
II. CVS Caremark’s Strong Resistance to
Transparency
In an industry that is starting to respond to criticism that it conducts business in the
shadows, CVS Caremark stands out as resistant to transparency. In fact, the company
has taken numerous strong measures to prevent greater disclosure of its practices,
including allegedly limiting clients’ ability to audit their health plans and vigorously
opposing legislative and other measures to increase transparency in the PBM industry.
In recent years, CVS Caremark has also lost significant PBM clients to competitors that
were awarded the business partially based on providing greater levels of transparency–
including revealing manufacturer rebates and discounts and passing those savings on to
plans.
A. CVS Caremark Loses Significant Contracts to More Transparent PBMs
CVS Caremark has suffered nearly $3 billion in contract losses in 2009, including a $1.4
billion contract for the commercial business of health insurance giant Coventry Health
Care and the $400 million Chrysler United Autoworkers retirees’ contract.48
Fighting transparent contracting has been a major factor in CVS Caremark’s losses.
Several former CVS Caremark clients have cited the company’s lack of commitment
to transparent contracting as part their rationale for dropping the company as their
prescription drug provider.
11Recent clients that cite transparency concerns as a factor in dropping CVS Caremark
include:
• New Jersey: In August 2009, the State of New Jersey announced that it would
enter into a new contract with Medco Health Solutions to provide pharmacy
benefits for approximately 670,000 state employees, dependents, and retirees.
CVS Caremark previously managed the $1 billion annual contract with Horizon
Blue Cross Blue Shield. The new contract is projected to save the state $559
million over five years through a transparent, pass-through pricing model.49
The state decided on the pass-through option because it “satisfies dual goals of
attaining the greatest cost savings while achieving transparency in a time when
that keyword is paramount to business operations in the public sector.”50
• New York MTA: In June 2009 New York’s Metropolitan Transportation
Authority voted to end its relationship with CVS Caremark and expects to save
$50 million under a new PBM contract with Innoviant. The MTA reported
that among the reasons it did not consider CVS Caremark for renewal of its
$490 million, three-year contract were “exceptions taken to core requirements
contained in the RFP.”51 In its Request for Proposals, the MTA placed a priority
on transparent pass-through pricing and financial guarantees.52
• Maryland: After being a Caremark customer for over ten years, the State of
Maryland replaced CVS Caremark with a smaller, transparency-oriented PBM
called Catalyst Rx in 2007 for a $1.1 billion, five-year PBM contract for over
200,000 state employees.53 In rejecting an appeal by CVS Caremark, the state
noted that the company’s “commitment [to transparency] seemed vague - [our
evaluation] team [was] not comfortable that they will be able to audit.”54
As the company’s contract losses start to add up, investors are beginning to worry about
whether the merger is resonating with health plan sponsors. The loss of several large
marquee contracts in 2009 prompted CVS Caremark CEO Tom Ryan to admit that “the
remaining [2009 PBM contract] opportunities are probably not sizable enough to offset
12the losses . . .”55 And an August 2009 Morgan Stanley analyst report warned that the
company’s PBM losses may continue: “Caremark PBM could see another sub-par growth
year in 2010 as contract losses will outstrip wins . . .”56
B. CVS Caremark Takes Legal Action and Pressures Clients to Keep
Taxpayer-Funded Contracts from the Public
Change to Win has sought greater transparency through the disclosure of CVS Caremark
contracts with public agencies.57 Obtained through requests under state and federal
open records laws, these contracts provide for the prescription drug benefits of federal,
state, and municipal employees and are paid for with taxpayer dollars. CVS Caremark
has vigorously fought the public disclosure of its contracts and pricing information, even
when the prescription benefits are funded from the public coffers.
CVS Attempts to Block Change to Win Website
In November 2008, days after the launch of the Alarmed About CVS Caremark website
(www.AlarmedAboutCVSCaremark.org), CVS Caremark sought a temporary restraining
order and injunction against the website to block access to contracts between CVS
Caremark and public agencies, contracts that were legally obtained through open-
records requests.58 A district judge in the eastern district of Virginia denied CVS
Caremark’s request.59
Pressure on Clients to Withhold Public Contracts
While more than three dozen contracts have been released to Change to Win, many
federal, state, and local agencies have redacted key contract provisions or refused to
release contracts altogether. In several cases, CVS Caremark has directly intervened
to ask the public agency to withhold part or all of the contract to keep pricing or other
contract provisions from the light of day. For example, through public records requests,
Change to Win obtained July 2009 emails between counsel for the Los Angeles Unified
School District (LAUSD) and CVS Caremark60 that indicate CVS Caremark requested
that the contract be withheld, and agreed to defend and pay for any future litigation
accusing LAUSD of breaking public disclosure laws.61
In another incident, both CVS Caremark and the City of Providence, R.I., demanded
that Change to Win return a contract that the city had already lawfully released.62 The
city subsequently reversed its decision after its legal department conducted a review,
prompting the city’s Assistant Solicitor to comment, “we are in agreement with Change
to Win that our initial disclosure of the bid was appropriate.”63 Similar interventions by
the company have taken place in at least two other locales.64
Lawsuits Over Disclosure in Texas
In Texas, CVS Caremark has brought multiple separate suits seeking to block the release
of its contracts covering public employees, even after the Office of the Texas Attorney
General issued legal opinions in each instance stating that the CVS Caremark contract at
issue should be released as a public document under well-established Texas law.
13In a ruling regarding the release of the CVS Caremark contract for the Houston
Independent School District, Texas Assistant Attorney General Reg Hargrove stated,
“We note that pricing information pertaining to a particular contract or project is
generally not a trade secret . . . Moreover, this office considers the prices charged in
government contract awards to be a matter of strong public interest.”65
C. CVS Caremark Opposes Legislative Action Supporting Transparency
There is a growing push for PBM transparency at the federal level. In August, the
House Energy and Commerce Committee passed a PBM transparency amendment to
health care reform bill HB 3200. The amendment, sponsored by Rep. Anthony Weiner
(D-N.Y.), created disclosure requirements for any PBM participating in the new health
insurance exchanges that were part of several health insurance reform bills.66 Soon
after that amendment passed the House Committee, CVS Caremark CEO Tom Ryan
told investors that transparency was less important than cost savings, and he predicted
the amendment would ultimately fail.67 But in late September the Senate Finance
Committee passed a similar amendment sponsored by Sen. Maria Cantwell (D-Wash.),
creating disclosure requirements for any PBM participating in the health insurance
exchanges and Medicare Part D.68 Contrary to Ryan’s prediction, both amendments
passed out of committee and were determined by the Congressional Budget Office to be
budget-neutral.
III. CVS Caremark’s Unparalleled Access to Patient
Data and Potential Threats to Privacy
With the completion of the merger between CVS and Caremark, the Company became
the largest provider of prescriptions in the United States, filling or managing over one
billion prescriptions annually.69 The combined drugstore-PBM giant has relationships
with over 150 million consumers, one of every two Americans, and has access to data on
approximately 30 percent of all prescriptions in the United States.70
CVS Caremark’s business model seeks to maximize the value of the private information
harvested from PBM plan participants and retail consumers.71 And the company is
unabashed about its use of patient data. As CVS Caremark CEO Tom Ryan boasts, “We
get the consumer. We have more information on the consumer and their behavior than
anybody else, and we share it with our over-the-counter suppliers. We share it with our
pharmacy suppliers. So we know how the consumer works.” 72
CVS Caremark has sold consumer information to drug manufacturers and other
third parties. These practices are often allowed under its contracts with plans. One
typical contract provides that CVS Caremark “may use, disclose, reproduce or adapt
14information obtained in connection with this Agreement, including Claims as well as
eligibility information, in any matter it deems appropriate. . .”73
A. Using Private Patient Information for Unsolicited Marketing
Some patients and pharmacists report that since the CVS Caremark merger, the
company has used its access to PBM plan members to subject individuals to unsolicited
marketing for CVS pharmacies.
For example, Caremark beneficiaries who fill prescriptions at non-CVS pharmacies
report receiving multiple harassing phone calls from CVS Caremark, encouraging them
to switch to CVS mail order pharmacies, even when their health plan permits them to
fill at the pharmacy of their choice. One beneficiary reports that CVS Caremark called
her several times and when she called the company back, she indicated that she was not
interested in switching pharmacies. Soon after, the beneficiary received an ExtraCare
Health Card in the mail, offering her discounts at CVS pharmacies. She then received
another message left on her home answering machine, with instructions to call CVS
Caremark and input a numeric code unique to her. When she did this, she heard the
following automated message:
“Hello, this is CVS Caremark, the company that manages
the prescription portion of your health benefit plan, calling
with important information for [patient’s name]. Is this
[patient’s name]? Please say yes or no after the chime.
“In times like these, we’re all looking for extra ways to save,
which is why we’re inviting you again to try CVS Caremark
Mail Service pharmacy. Getting set up is fast and easy, and
it’s already offered through your health plan. Would you like
to talk with someone to see how much you could save?”74
(emphasis added)
The patient indicated that she wished to speak with someone, and was connected to
a customer service representative. When the patient asked why she was receiving so
many confusing calls, the representative claimed that her plan had arranged the call to
inform her that she could receive her prescriptions by mail order. The customer service
representative continued to explain that “if the system shows any prescriptions filled at a
local pharmacy, the patient automatically gets a call to let them know that the mail order
option is available.”75
This patient reported feeling intimidated by these unsolicited telemarketing calls:
“When I get those calls, I want to make sure that I’m doing the right thing. . . I’m afraid I
could lose my benefits if I make the wrong decision” about where to fill prescriptions.76
CVS Caremark’s highly touted ExtraCare card is also a way CVS gathers customers’
information – in this case, their past purchase history – for unsolicited marketing.77
15The ExtraCare website enumerates the benefits of the program but does not state that
the company collects information on consumer purchases for marketing purposes.78
CVS Caremark issued 10 million ExtraCare Health cards to individuals enrolled in
CVS Caremark prescription benefit plans in 2008, enabling the company to target new
patients with specific marketing offers.79
Another CVS Caremark practice — using ExtraCare card promotions to encourage CVS
customers to switch their prescriptions to the company — suggests that the company
connects prescription information with other consumer purchasing information. For
example, CVS Pharmacy customers report being encouraged to use their ExtraCare
card when they purchase prescriptions, in exchange for which they receive $1 in ‘Extra
Bucks’ for each two prescriptions filled.80 This kind of promotion enables CVS Caremark
to collect medical information on people who may not have otherwise filled their
prescriptions at a CVS pharmacy and target unsolicited marketing at these individuals
through mailings and phone calls to their homes.
Not only is CVS Caremark opaque about the use of its customers’ private medical
information, it also severely limits the rights of patients who ask the company to keep
their information confidential. For concerned patients who may want to keep CVS
Caremark from sharing their medical information with third parties or using it for
marketing, the opt-out process is a laborious one and may not prevent their information
from being used in a way that they object to. Patients who want to prevent their medical
information from being used by CVS Caremark must write to the company requesting a
specific restriction on the use of their data. CVS Caremark, however, is “not required to
agree to those restrictions.”81
B. Settlements with the FTC and HHS Office of Civil Rights on Improper
Disposal of Medical Information
In February 2009, the Federal Trade Commission and the Department of Health and
Human Services announced settlement agreements with CVS Caremark over its failure
to properly dispose of personal information from customers and employees at its retail
stores. These failures violated both
the Health Insurance Portability and
Accountability Act (HIPAA) Privacy
Rule, which protects the privacy
of individually identifiable health
information, as well as federal trade
law barring unfair and deceptive
practices. The agencies alleged
that private financial and medical
information ended up in unsecured
dumpsters, including “pill bottles
with patient names, addresses,
prescribing physicians’ names,
16medication and dosages” and “employment applications, including social security
numbers; payroll information; and credit card and insurance card information.”82
C. Consent Agreement with State of California on Privacy and Expired
Goods
In June 2009, the California Attorney General reached an agreement with CVS
Caremark requiring the company to make sure expired products are not sold in its stores
and that customers’ private information is disposed of properly. The agreement followed
an investigation that found CVS regularly sold expired baby food, baby formula, over-
the-counter medications and dairy products to consumers and that a number of CVS
Pharmacies had improperly discarded more than 500 documents and prescription
bottles containing confidential medical information in dumpsters outside of stores. This
discarded information included patient names, addresses, birthdates and prescription
medications. As part of the settlement, CVS paid nearly $1 million in civil penalties,
attorney fees and costs.83
IV. Recommendations
Plan trustees, administrators and policy-makers have a responsibility to scrutinize
the actions of the nation’s largest purchaser of prescription drugs, a company that
aggregates massive amounts of private health information and leverages it to increase
its bottom line. Health plans should also remain vigilant about how their drug spend
is being managed and whether their PBM’s business model is working for them. A
growing number of large plan sponsors are opting for a more transparent Pharmacy
Benefit Administrator or Facilitator model to guarantee pass-through of all payments
from manufacturers and to secure comprehensive auditing rights. Every plan should
take steps to ensure they are getting the pricing guarantees and rebates they have been
promised by undertaking the following steps:
Carefully Negotiate Key Terms of Your Plan’s PBM Contract
Plan trustees should closely oversee their PBM contract from the request for proposals
through negotiation, implementation, and monitoring. Plans should pay particular
attention to contract terms that could harm the plan and its members, including:
• Allowing PBM retention of rebates and other payments from drug companies;
• Authorizing the PBM to use and sell the personal information of plan members;
• Allowing the PBM to switch drugs without guaranteeing the switch will result in
lower costs for the plan;
• Limiting the plan’s access to information;
• Restricting the plan’s auditing rights.
17Audit Your PBM’s Performance
Health plans have saved or recovered millions of dollars by auditing their PBM’s perfor-
mance, and plans should consider conducting regular audits to ensure that they are not
being taken advantage of. Contract language that allows the plan to conduct indepen-
dent audits is critical to exercising effective oversight.
Support Legislative Reform of PBMs
PBMs operate in a weak regulatory environment at both the state and federal levels.
Legislative reform is vital to ensuring that CVS Caremark does business honestly and
with the best interests of plans and plan members as their top priority. Key initiatives to
support include: greater PBM transparency, protection for patient privacy, limiting drug
switching to that which results in lower plan costs, and classification of PBMs as fiducia-
ries to the plans they serve.
For more information on Change to Win’s efforts to reform the PBM industry and en-
courage the Federal Trade Commission to review the CVS Caremark merger, visit our
web site, www.AlarmedAboutCVSCaremark.org.
18Endnotes
1 CVS Caremark Corporation. Slide presentation. The Power of One: 2008 Analyst/Investor Meeting.
21 May 2008 (slides 15 and 34.) Available at: http://library.corporate-ir.net/library/99/995/99533/items/
294969/2008CVSCaremarkInvestorRelationsALL.pdf; CVS – CVS Caremark Corporation 2008 Analyst/
Investor Meeting Transcript, Statement of Nancy Christal, at p. 7. 21 May 2008. Available through Thomson
StreetEvents.
2 Change to Win & Alarmed about CVS Caremark. CVS Caremark: An Alarming Prescription. Nov. 2008.
Available at: http://www.alarmedaboutcvscaremark.org/index.php?id=37
3 Providence Business Journal. “FTC competition unit to examine CVS.” 24 Jun. 2009. Available at:
http://www.pbn.com/detail/43167.html; Letters to the Federal Trade Commission calling for a review of the
CVS Caremark merger from: more than 17 members of Congress; six health plans and purchasing coalitions:
(1) Delaware Valley Health Care Coalition, (2) New York Labor Health Care Alliance, (3) Sergeants Benevolent
Association, Police Dept, City of New York, (4) 1199 New England, SEIU, (5) Sheet Metal Workers
International Union, (6) Laundry, Dry Cleaning and Allied Workers Joint Board of New York, and three
consumer groups: (1) the National Legislative Association on Prescription Drug Prices (NLARx), (2)
Consumer Federation of America, and (3) US Public Interest Research Group; and the National Community
Pharmacists Association.
4 CVS – CVS Caremark Corporation, 2008 Analyst/Investor Meeting Transcript, Statement of Helena Foulkes,
at p. 7. 21 May 2008. Available through Thomson StreetEvents.
5 CVS Caremark website: http://info.cvscaremark.com/newsroom/featured-topics/extracare;
downloaded 27 Oct. 2009.
6 CVS - CVS Caremark Corproation, 2008 Analyst/Investor Meeting Transcript, statement of Helena Foulkes,
at p. 17. 21 May 2008. Available through Thomson StreetEvents.
7 Change to Win & Alarmed about CVS Caremark. CVS Caremark: An Alarming Prescription. November 2008.
pp. 9 – 14.
8 Each of the states and D.C. that settled with CVS Caremark filed a complaint and consent order on or around
February 14, 2008. These complaints and consent orders are substantially similar. See, e.g., Illinois v.
Caremark Rx, L.L.C., No. 08-CH-05634, Circuit Court of Cook County, IL. 14 Feb. 2008 (Complaint for
Injunctive and Other Relief); State of Ohio v. Caremark Rx, L.L.C., No. 08CVH02-2251, Court of Common
Pleas, Franklin County, OH. 14 Feb 2008 (Complaint for Declaratory Judgment, Injunctive Relief and Costs):
at ¶¶ 20-24; United States ex rel. Lisitza v. CVS Caremark. 31 Jan. 2003 (Complaint): at p. 1; see also: Won
Tesoriero, Heather, and David Armstrong. “CVS Caremark Reaches Settlement.” Wall Street Journal. 9 Mar.
2008; CVS Caremark Press Release, “CVS Caremark Issues Statement on Settlement Concerning Retail
Dispensing Practices for Ranitidine.” 18 Mar. 2008. Available at: http://www.cvscaremark.com/newsroom/
press-releases/cvs-caremark-issues-statement-settlement-concerning-retail-dispensing-practi
9 Corporate Integrity Agreement between the Office of the Inspector General of the Department of Health and
Human Services and CVS Caremark Corporation. 2 Sept. 2005 (“Caremark Corporate Integrity Agreement”);
United States of America vs. AdvancePCS, Nos. 02-CV-9236 & 03-CV-5425 (E.D. Pa.) 8 Sept. 2005 (Consent
Order of Court for Injunctive and Settlement). Caremark agreed to be bound by the Corporate Integrity
Agreement to the same extent as Advance PCS.
10 Interview with confidential source who demanded anonymity based on fear of possible retaliation
by CVS Caremark.
11 Ibid.
12 Ibid.
13 Ibid.
14 Gonzales, Angela. “CVS Caremark uses patient info to market drugs.” Phoenix Business Journal.
18 Aug. 2008. Available at: http://jacksonville.bizjournals.com/phoenix/stories/2008/08/18/
story14.html
15 Alexander, G.C. Archives of Internal Medicine, Vol. 168. 27 Oct. 2008: pp. 2088-2094. Summary available at:
http://www.rxlist.com/script/main/art.asp?articlekey=93738
16 Feeley, Jef, Margaret Cronin and Elizabeth Lopatto. “CVS Unit Played Both Sides, Lilly Drug Lawsuit Shows.”
Bloomberg News. 12 June 2009. Available at: http://www.bloomberg.com/apps/
news?pid=20601110&sid=aiewKdPT_wOQ
17 UCFW Local 1776 and Participating Employers Health and Welfare Fund, et. al. v. Eli Lilly and Co., No.
05-cv-4155. The case is pending in the United States District Court for the Eastern District of New York in
Brooklyn, New York.
1918 Feeley, Jef, Margaret Cronin and Elizabeth Lopatto. “CVS Unit Played Both Sides, Lilly Drug Lawsuit Shows.”
Bloomberg News. 12 June 2009. Available at: http://www.bloomberg.com/apps/
news?pid=20601110&sid=aiewKdPT_wOQ
19 Russel, John. “Lilly pays CVS Caremark to try to get doctors to prescribe Cymbalta.” Indianapolis Star.
18 Oct. 2009. Available at: http://www.indystar.com/article/20091018/BUSINESS03/910180396/1003/
BUSINESS/Lilly+pays+CVS+Caremark+to+try+to+get+doctors+to+prescribe+Cymbalta
20 Ibid.
21 Stern, Debbie and Debi Reissman. “Specialty Pharmacy Cost Management Strategies of Private Health Care
Payers.” Journal of Managed Care Pharmacy, Vol 12, No. 9. Nov./Dec. 2006, at p. 736. Available at:
http://www.amcp.org/data/jmcp/736-744.pdf
22 Goldstein, Jacob. “The Most Expensive Drugs are Getting Even More Expensive.” Wall Street Journal.
25 September 2008. Available at: http://blogs.wsj.com/health/2008/09/25/the-most-expensive-drugs-are-
getting-even-more-expensive/
23 Ibid.
24 Maas, Angela. “Pharmacy Cost Hikes for Specialty Drugs, While Still High, Are Slowing Somewhat.”
Specialty Pharmacy News. 29 Jun. 2009. Available at: http://www.aishealth.com/Bnow/hbd072909.html
25 Prescription Benefit Agreement between Caremark LLC and Los Angeles Unified School District,
1 Jan. 2009, at p. 6.
26 Interview with confidential source who demanded anonymity based on fear of possible retaliation
by CVS Caremark.
27 Average of eight quarters of fiscal year 2007 and 2008 EBITDA per Adjusted Claim. 2007 figures source:
Adler, Meredith. Lehman Brothers Food & Drug Retailing Analyst Report. CVS Corporation: Change of
Earnings Forecast. 1 Aug. 2008, at p. 3. 2008 figures source: Miller, Mark, Walania, Eric and Daniel Hofkin.
William Blair & Company Equity Research Analyst Report, CVS Caremark Corporation: Encouraging
Developments and Potential Concerns from First-Quarter Results. 6 May 2009, at p. 7.
28 Robert Garis, Bartholomew E. Clark, and Mark Siracuse. “Is the Pharmacy Benefit Manager Truly Transparent?
Trust but Verify.” U.S. Pharmacy Review. 2006, at p 1. Available at: http://www.ncpanet.org/pdf/leg/leg_
pbm_transparency_garis.pdf
29 David Balto. Report prepared for National Community Pharmacists Association, “Select Complaints against
CVS/Caremark II.” 2009.
30 Unites States Office of Personnel Management, Office of the Inspector General. Final Audit Report: Report
on the Audit of AdvancePCS. Office of Audits. Report No. 1H-01-00-04-100. Washington, D.C. 30 Mar. 2006,
at p. 4; Unites States Office of Personnel Management, Office of the Inspector General. Final Audit Report:
Report on the Audit of AdvancePCS. Office of Audits. Report No. 1H-01-00-06-063. Washington, D.C.. 7 Sep.
2006, at Executive Summary and p. 4.
31 Donohue, Pete. “CVS Reimburses MTA almost $1M after overcharging transit workers, retirees.”
New York Daily News. 22 June 2009. Available at: http://www.nydailynews.com/ny_local/2009/06/22/
2009-06-22_cvs_reimburses_mta.html
32 Office of Legislative Audits, Department of Legislative Services, Maryland General Assembly, Audit Report:
Department of Budget and Management, Office of Personnel Services and Benefits. Feb 2009, Executive
Summary at p 5. Available at: http://www.ola.state.md.us/reports/Fiscal%20Compliance/OPSB09.pdf
33 First Medical Health Plan v. CaremarkPCS Caribbean, Amended Complaint. Case No. 3:09-cv-01009-GAG,
charges at pp. 4-7; monetary damages at p. 11.
34 Local Government Center HealthTrust, New Hampshire. Prescription Benefit Services Agreement with
Caremark. 16 Feb. 2007, at p. 14. Also see: Golden Gate Bridge Highway and Transportation District,
California. Amended and Restated Prescription Benefit Services Agreement with Caremark. 1 Jul. 2006, at
p. 9; Health Action Council of Northeast Ohio, Ohio. Prescription Benefit Services Agreement with Caremark.
1 Jan. 2006, at p. 10.
35 Wolf, Carol. “Senators Urge CVS Caremark Probe in Letters to FTC.” Bloomberg News. 30 July 2009.
36 Ibid.
37 Senator Maria Cantwell speaking during the Senate Finance Committee debate on health care reform, 25
Sept. 2009, at 1:38:36 of C-SPAN video. Available at: http://www.c-span.org/Watch/Media/2009/09/25/
HP/R/23568/Senate+Finance+Cmte+concludes+first+week+of+health+care+debate.aspx
38 Wolf, Carol. “CVS’s Ryan Predicts House Drug-Plan Rules Will Fail.” Bloomberg News. 4 Aug 2009.
Available at: http://www.bloomberg.com/apps/news?pid=20601202&sid=aycgc.OnmfJM
39 Welcome Pack for the US House of Representatives Subcommittee on Federal Workforce, Postal Services
and District of Columbia Forum. “Prescribing the Right Solution: A Discussion on Improving FEHBP’s Drug
Benefit.” At p. 3.
20You can also read