Solihull Alcohol Harm Reduction Strategy 2016-2021 - Social ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Solihull Alcohol Harm Reduction
Strategy
2016-2021
Solihull Alcohol Initiative
Contents
Chapter 1: Introduction
Chapter 2: Alcohol Related Harm - The National Picture
Chapter 3: Alcohol Related Harm - The Local Profile
Chapter 4: Where are we now? – Where are the gaps?
Chapter 5: Where do we want to get to? – Recommendations
Chapter 6: How are we going to get there? Implementation/Delivery plans
Chapter 7: Monitoring and review
References
AppendicesForeword “The function of a good health service should be not only to care for those with disease but also to prevent disease where possible. Many patients presenting to hospital services do not have conditions attributable to alcohol but are hazardous drinkers by virtue of their high consumption. Unless they modify their behaviour many of these will, before long, require treatment for some condition attributable to their drinking, thus adding to the burden of alcohol on hospital services.” (Alcohol: Can the NHS afford it? RCP (2001)) There can be no doubt that tackling alcohol-related harm is currently a priority both nationally and locally. The Chief Medical Officer (CMO) published new alcohol guidelines that state drinking any level of alcohol regularly carries a health risk for everyone. Men and women should limit their intake to no more than 14 units a week to keep the risk of illness like cancer and liver disease low. The vast majority of people who drink alcohol in Solihull do so responsibly, however a significant number of the Borough’s population drink more than they realise. Stronger alcohol and generous home measures are contributing to damage to people’s health, often without them realising. Every year we are seeing more and more people admitted to hospital with alcohol related conditions. There is a clear and growing evidence base of the harmful impact that alcohol misuse can have on individuals, families and communities in our borough. The levels of alcohol related health problems are increasing year on year and affect a wide cross section of our communities and contribute to health inequalities in the borough. Alcohol and drug misuse is the cause of many health and social problems and can devastate families and communities. It is a significant driver of crime and anti-social behaviour and the cost to the local economy is significant. Solihull has a history of providing quality alcohol and drug treatment services. There are effective services and interventions to help people overcome alcohol dependency but a substantial proportion of those who could benefit are not aware that they have a problem or do not know what treatment is available. Screening for alcohol problems and offering brief advice in primary care is a very effective method of helping those with harmful levels of drinking. The strategy aims to make these interventions more readily available. However, alcohol plays an important role in our communities; it has made a constructive contribution to the growth of our local economy by providing employment and encouraging visitors to the borough. Alcohol used in moderation, can form an enjoyable part of our society and lives without causing harm to those who use it or to those around them. By balancing the positive and negative influences of alcohol and tackling its misuse, it will help us to support the aspiration of residents to live longer, healthier and happier lives. This Alcohol Strategy aims to build upon the numerous approaches and interventions that have resulted in benefits for individuals, families and communities affected by alcohol misuse. It aims also to further the work with stakeholders in the borough to comprehend
our attitudes to alcohol and the root causes of alcohol misuse issues and to develop a positive culture and relationship with alcohol. The vision of the strategy highlights the need to integrate with our partners in order to educate, prevent, treat and reduce the health, social and economic harms of alcohol and drug misuse. We can do more through co-ordinated action across agencies to tackle alcohol related crime and anti-social behaviour. The strategy will promote sharing of information on impacts from alcohol that can be used by licensing agencies to limit availability in areas where problems are known to exist and support local partnerships to manage their night time economy. With such a large agenda, we need the collective focus and resources of all key partners to achieve the priority outcomes we have identified in the strategy. We need to target our efforts on areas and groups that have a disproportionate impact from alcohol misuse and we need to do so in efficient and innovative ways. These underpinning values will inform the delivery of the strategy. This strategy comes at a challenging time for public services, when resources are stretched and everyone is expected to deliver better services with less funding. However, through maintaining and developing our strong partnership approach we are confident we can make a real difference in reducing alcohol related harm across Solihull. Given the long term costs and consequences both social and health related of this rising tide of hidden alcohol misuse we really must get this right. We can’t afford not to.
Chapter 1: Introduction
Strategic Aim
The Alcohol Harm Reduction Strategy for Solihull aims to minimise the harm caused by
alcohol to individuals, families and communities in Solihull, while ensuring that people are
able to enjoy drinking alcohol sensibly and safely.
Objectives
Addressing and reducing alcohol related harm is both complex and challenging.
NICE released a local government public health briefing on alcohol in October 2012 which
recommended that local authorities could, through working in partnership, take a number
of actions. The briefing highlights that local authorities:
Have a role in promoting and advising people about sensible drinking
Have responsibility for commissioning alcohol prevention and specialist treatment
Can Influence where and when alcohol is consumed or sold, as part of planning
regulations
Have an important role in ensuring licensed premises operate responsibly and
collaborate to reduce alcohol related harm
The strategy contributes to the delivery of the Solihull Metropolitan Borough Council’s priority to
improve Health and Wellbeing by:
Developing Prevention and Early Help Services for children and adults, including support to
carers
Creating access to high quality information, advice and support-planning services that
promote health, safeguarding and independence
This new alcohol strategy has been informed by the following:
Solihull Health and Wellbeing Board Alcohol Strategy Stakeholder Workshop held in
December 2015.
SIAS service review (which included a review of performance against Key
Performance Indicators (KPIs), b) a stakeholder panel review of performance jointly
with the providers held in October 2015 and a specific presentation by, and
discussion with SIAS, held by the JCG in January 2016).
Solihull Substance Misuse needs assessment- updated April 2016.
Joint Commissioning Group Meeting for Alcohol held in April 2016.As a result of the work achieved with Solihull’s last alcohol strategy and alongside the above
work and analysis of the current picture of alcohol related need in Solihull we have
identified key thematic areas as a framework for action in 2016-21:
Prevention through education and communication
Early identification and brief interventions
Treatment and specialist treatment
Licensing, access to alcohol, alcohol related problems and community safety and
the night time economy
Partnership responsibility and governance
Each step in the alcohol care pathway is key to ensuring the success of the strategy.
Licensing, access
to alcohol, alcohol
related problems
and community
safety and the
night time
economy
Partnership
responsibility and
governance
Whilst recognising and continuing to promote our excellent treatment services there will be
an important focus in this strategy on early identification and brief interventions (IBA) of
increasing risk and high risk drinkers in a variety of settings, with the aim of preventing them
becoming hazardous and harmful drinkers.
Addressing inequalities across the borough and the promotion of personal responsibility and
self management will be cross cutting themes across all these priorities.
Each theme is explored in more detail later in this document; with our priorities for action
being guided by strong intelligence and evidence. We also aim to co-ordinate action and
activities in a multi-agency and partnership lead approach to make best use of our resources
and target future investment.
To note this is a borough wide strategy and as such requires the commitment of a number
of different organisations including those represented on the Joint Commissioning Group aswell as commercial premises. We recognise that there is a shared interest between
organisations to ensure individuals drink responsibly.
The figure below shows how the priorities identified by this alcohol strategy relate and
contribute to wider health and community priorities.
Health
Emergency department visits
Treatment
Identification Brief Advice
Mental Health
Complex needs services
Integrated pathways
Mental and social wellbeing
Health awareness
Alcohol Awareness
Self management
Self harm
Primary Care and Hospital engagement
Targeting ‘at risk’ groups
Community Safety
Vulnerable Groups Night time economy
Young people Alcohol Strategy Priorities Domestic Abuse
Older people Violent crime
Safeguarding Education & prevention Community perception and
Age relevant education Identification and participation
Risky Behaviours treatment Licensing
Peer lead mentoring Addressing alcohol related Responsible retailing
Training for Professionals problems Binge Drinking
Parents Licensing , access & Support for Offenders
Targeting community safety Housing and homelessness
Specialist Services Partnership responsibility Anti Social Behaviour and Crime
Long term health effects Alcohol supply and cost
Sexual Health
For example Solihull’s Local Police and Crime Plan includes helping our communities develop
healthy attitudes and behaviours around alcohol and drug use, and ensure families get help
to prevent and deal with the risks to young people and relationships and making sure we
recognise and respond to the crime and antisocial behaviour linked to alcohol and drug
misuse as key objectives.
The strategy will be delivered via implementation plans that both build on existing provision
and also develop new and innovative approaches to interventions, prevention andinformation. The plans will be implemented over the next five years, and will be annually
reviewed by the Joint Commissioning Group and refreshed to ensure progress and
continued relevance.
Definitions
Alcohol misuse and alcohol dependence are categorised in a number of different ways. This
is in part because they exist on a broad spectrum which covers a wide range of need. The
point at which one group ends and another begins is not an exact point and this has given
rise to slightly different definitions. Different definitions have also arisen as categorisations
have been based variously on: level of potential/actual harms, level of consumption and
level of dependence.
Below is a brief description of the various categories that are frequently used and how they
might relate to services that can be commissioned on a local basis.
Hazardous and harmful drinking
These terms were introduced by the World Health Organisation and are used as categories
linked to the AUDIT (Alcohol Use Disorders Identification Test) screening tool. The AUDIT
screening tool is recommended by WHO (WHO 2001) as well as by NICE (PH24 and CG115).
The tool screens for potential or actual harmful drinking and possible dependence. It
indicates an appropriate intervention according the score achieved.
Hazardous
AUDIT 8-15
‘A pattern of alcohol consumption that increases someone's risk of harm.' Some
would limit this definition to the physical or mental health consequences (as in
harmful use). Others would include the social consequences. The term is currently
used by WHO to describe this pattern of alcohol consumption. It is not a diagnostic
term.’ (NICE PH24)
Harmful:
AUDIT 16-19
‘A pattern of alcohol consumption that is causing mental or physical damage’ (NICE
PH24)
Possible dependence:
AUDIT 20+.
AUDIT screens for possible dependence but does not measure level of dependence.
A specialist assessment is necessary to determine level of dependence.Increasing risk and higher risk drinking
These terms were introduced by DH. The terms are based simply on the estimated number
of units consumed per week. The view of the DH, based on expert advice was that these
simply defined categories would be more easily communicated to the general public. They
are now often now used as categories linked to the AUDIT screening tool.
Increasing risk:
AUDIT 8-15
‘Regularly consuming between 22 and 50 units per week (adult men) or between 15
and 35 units per week (adult women).’ (NICE PH24)
Higher risk
AUDIT 16-19
Higher risk and not meeting ‘possible dependence’ criteria
‘Regularly consuming over 50 alcohol units per week (adult men) or over 35 units per
week (adult women).’(NICE PH24)
Although the definitions of ‘hazardous’ and ‘harmful’ drinking are not identical to
‘increasing risk’ and ‘higher risk ‘ drinking they are broadly equivalent and can be used
interchangeably for the purposes of identifying broad categories of need and appropriate
interventions that can be commissioned.
Commissioning of IBA / brief intervention/extended brief interventions would serve the
needs of hazardous /increasing risk drinkers and most harmful/higher risk drinkers who are
not dependent.
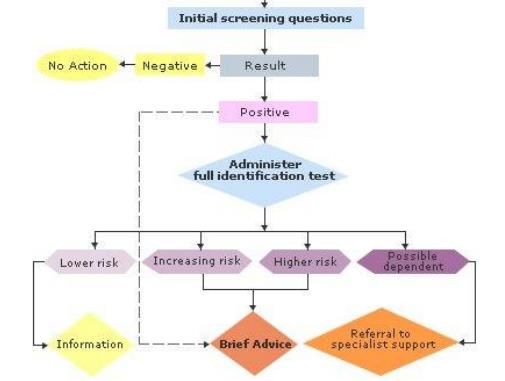
The recommendations for groups identified through IBA are as follows:
Hazardous/increasing risk
o IBA /brief intervention
Harmful/higher risk
o IBA/brief intervention; if no response, extended brief intervention and
monitoring.
The following groups should be referred for a specialist assessment (CG115):
o Those who score AUDIT 16-19 and do not respond to brief advice or
extended brief intervention and/or have complex needs = harmful drinking or
possible dependence
o Those who score 20+ AUDIT: possible dependence
These steps are shown in the pathway below:Alcohol Brief Intervention
The evidence
There is a very large body of research evidence supporting Identification and Brief Advice
(IBA) in primary care including at least 56 controlled trials (Moyer et al., 2002). A Cochrane
Collaboration review (Kaner et al., 2007) provides substantial evidence for the effectiveness
of IBA.
For every eight people who receive simple alcohol advice, one will reduce their
drinking to within lower-risk levels (Moyer et al., 2002).
This compares favourably with smoking where only one in twenty will act on the
advice given (Silagy & Stead, 2003). This improves to one in ten with nicotine
replacement therapy.
Patients who received IBA in A&E made 0.5 fewer visits to the A&E during the
following 12 months (Crawford et al., 2004).
“Brief intervention has been shown to be effective” Signs for improvement:
Commissioning interventions to reduce alcohol related harm. DH (2009).
NICE alcohol use disorders; preventing harmful drinking (2010) suggests that alcohol
screening and brief advice should be routinely delivered by staff who have receivedthe necessary training and work in emergency departments and other healthcare
services.
Identification and brief advice for alcohol is underpinned by behaviour change models, the
following research paper summarises the evidence for this:
“Identification of behaviour change techniques to reduce excessive alcohol consumption”
S.Michie, C.Whittington, Z Hamoudi, F.Zamani, G.Tober and R.West. Addiction Vol 107 Issue
8 (2012)
In addition, Professor Susan Michie has developed the Drink Less App based on behavioural
science which is currently available for free www.drinklessalcohol.com
The Process
Brief advice for alcohol involves encouraging people to drink less. These are effective interventions
directed at patients drinking at increasing or higher-risk levels that are not typically
complaining about or seeking help for an alcohol problem. Alcohol brief advice is
traditionally preceded by a validated screening tool such as the Alcohol Use Disorders
Identification test (AUDIT) or one of its validated shortened forms e.g. AUDIT C, FAST or
SASQ.
Where a positive score on one of the pre-screens has occurred, best practice is to deliver
the full AUDIT. The gold standard 10 question AUDIT screening tool enables a stratification
of risk i.e. Lower Risk drinking, Increasing Risk drinking, Higher Risk drinking and Possible
Dependence. Structured brief advice delivery then takes place, using a DH Alcohol Brief
Advice tool or similar.
Alcohol brief advice typically follows an Ask, Advise, Assist structure:
Ask: raise the issue, accompanied usually by use of a screening tool to assess risk
Advise on risk, giving personalised feedback of results of any screening assessment
Assist by offering routes to further information and support
A brief intervention should include an offer of signposting to further support. This may
include a default referral to local specialist services for patients who have been identified as
reaching agreed thresholds of risk levels. Clarity regarding the referral options and pathways
is crucial to the appropriate referral of patients to further support.
Chief Medical Officer Guidelines
The UK chief medical officer, working alongside a group of experts, has recently made
recommendations about how lower risks to health from drinking alcohol. The group looked
at the evidence about the levels and types of health harm that alcohol can cause, depending
on how much and how often people drink, and recommended that both men and women
limit their weekly intake to a maximum of 14 units.There has currently not been any change in use of AUDIT, FAST or any other pre-screening
tool as a result of new guidelines.
The new guidelines are as below:
On regular drinking
The new weekly guideline applies for people who drink regularly or frequently i.e. most
weeks. The Chief Medical Officers’ guideline for both men and women is that:
You are safest not to drink regularly more than 14 units per week, to keep health
risks from drinking alcohol to a low level.
If you do drink as much as 14 units per week, it is best to spread this evenly over 3
days or more. If you have one or two heavy drinking sessions, you increase your risks
of death from long term illnesses and from accidents and injuries.
The risk of developing a range of illnesses (including, for example, cancers of the
mouth, throat and breast) increases with any amount you drink on a regular basis.
If you wish to cut down the amount you’re drinking, a good way to help achieve this
is to have several drink-free days each week.
On single drinking episodes
This applies for drinking on any single occasion, not regular drinking, which is covered by the
weekly guideline. The Chief Medical Officers advise men and women who wish to keep their
short term health risks from a single drinking occasion to a low level that they can reduce
these risks by:
Limiting the total amount of alcohol you drink on any occasion;
drinking more slowly, drinking with food, and alternating with water;
Avoiding risky places and activities, making sure you have people you know around,
and ensuring you can get home safely.
Some groups of people are likely to be affected more by alcohol and should be more careful
of their level of drinking on any one occasion:
young adults
older people
those with low body weight
those with other health problems
those on medicines or other drugs
On pregnancy and drinking
The Chief Medical Officers’ guideline is that: If you are pregnant or planning a pregnancy, the safest approach is not to drink
alcohol at all, to keep risks to your baby to a minimum.
Drinking in pregnancy can lead to long-term harm to the baby, with the more you
drink the greater the risk.
Most women either do not drink alcohol (19%) or stop drinking during pregnancy
(40%).The risk of harm to the baby is likely to be low if a woman has drunk only small
amounts of alcohol before she knew she was pregnant or during pregnancy.
Women who find out they are pregnant after already having drunk during early
pregnancy, should avoid further drinking, but should be aware that it is unlikely in
most cases that their baby has been affected. If you are worried about how much
you have been drinking when pregnant, talk to your doctor or midwife.Chapter 2: Alcohol Related Harm – The National Picture 10.8 million adults in England are drinking at levels that pose some risk to their health. An estimated 1.6 million may have some level of alcohol dependence, some of whom will benefit from specialist treatment, often having complex needs that present a challenge when commissioning alcohol services. Alcohol has been identified as a causal factor in more than 60 medical conditions, including: mouth, throat, stomach, liver and breast cancers liver disease heart disease depression stroke accident and injury epilepsy The impact of harmful drinking and alcohol dependence effects the most vulnerable groups in society - those in the lowest income bracket, those experiencing the highest levels of deprivation and individuals with mental health problems. The effects of harmful drinking are, however, felt by all. Its impact on individuals, their families and communities is wide-ranging and the annual cost to society is £21 billion. This is made up of: £11 billion from alcohol-related crime £7billion from lost productivity through unemployment and sickness £3.5 billion to the NHS. Not all of these costs are attributed to people who are alcohol dependent, but the costs illustrate the scale of the problems caused by alcohol and the challenge we face as a nation. Investment in alcohol interventions can produce a high return. For every 100 alcohol dependent people treated at a cost of £40,000, there can be savings of £60,000, with 18 A&E visits prevented and 22 hospital admissions averted (PHE Health Matters, 2016) The most recent Government Alcohol Strategy was published in March 2012. The strategy, produced by the Home Office, has a focus on the importance of preventing and reducing the impact of alcohol on crime and disorder, as well as health. The Government's Alcohol Strategy highlights the changes in behaviour regarding the purchasing and consumption of alcohol. Over the past 40 years alcohol consumption has
doubled, with a significant increase in drinking at home. Sales from supermarkets and other
off licences now account for nearly half of the amount of alcohol sold in the UK.
Public Health England (PHE) guidance states that in each year in a community of 100,000,
21,500 people drink at hazardous or harmful levels, 13,000 binge drink, 3,000 show signs of
alcohol dependence, and 500 people are moderately or severely dependent on alcohol.
There are currently around 150,000 people in specialist alcohol treatment nationally, with
more new clients entering treatment year on year.
An estimated 1.6 million people have some degree of alcohol dependence and of these,
some 250,000 are believed to be moderately or severely dependent, and require intensive
treatment from specialist services.
In the year 2010/11 there were almost 1 million alcohol-related crimes in England and
Wales and 1.2 million alcohol-related hospital admissions.
Alcohol has become one of the three biggest lifestyle risk factors for disease and death in
the United Kingdom, after smoking and obesity.
Alcohol consumption has been identified as a risk factor for many types of violence including
child abuse, youth violence, intimate partner violence, sexual violence and elder abuse.
Around half of all violence in England and Wales is thought to be committed by individuals
who are under the influence of alcohol (44% in 2010/11); while a fifth of all violent incidents
occur in or around drinking premises.
Individuals who commence drinking at an earlier age, who drink frequently and who drink
in greater quantities are at an increased risk of involvement in violence as both victims and
perpetrators. Importantly, alcohol has a dose responsive relationship with violence, with the
acute risks of violence increasing with the amount of alcohol consumed.
Groups at particular risk of alcohol related harm
While for the most part adults still consume alcohol in moderation, various estimates show
that a significant proportion of people nationally drink above recommended UK guidelines
and national data indicates a number of groups appear to be at higher risk of problematic
use.
Children, young people and young adults
The proportion of young people aged 11-15 years who have never drunk alcohol has
risen in recent years, from 39% in 2003 to 49% in 2009.
Young people and young adults are most likely to binge drink and are at greater risk
of developing dependence. National data shows that more than 30% of young people aged 16-24 can be
categorised as hazardous or harmful drinkers, compared to 15% of those aged 55-64
years.
Binge drinking among young women has increased significantly during the past
decade.
Most alcohol-related diseases take years to develop and are comparatively rare in
young people. However, the early onset of drinking and the heavy use of alcohol
during late
Adolescence is risk factors for the development of alcohol-related problems in later
life.
Other more immediate adverse outcomes associated with alcohol use among
children and young people include increased risk of early onset sexual intercourse
and unsafe sex, which has implications for sexually transmitted infections and
teenage pregnancy.
For young people, binge drinking is also strongly associated both with being the
perpetrator and the victim of crime.
Women
Women still consume far less quantities of alcohol than men, but the proportion of
women drinking excessive amounts of alcohol has been increasing over the years.
The proportion of women drinking more than 14 units a week increased by 70%
between 1988 and 2002, with women in managerial and professional households
being more likely to drink regularly than those in routine and manual households.
Drinking patterns amongst women vary with age. Whereas young women (16 to 24)
tend to cram their drinking into heavy drinking sessions with 49% consuming their
alcohol over one to three days, older women tend to drink more regularly, with 17%
of 25 to 44 year olds and 15% of 45 to 64 year olds regularly drinking on 5 or more
days per week.
There are important differences in the way women's bodies react to alcohol
compared with men, which means alcohol can do more damage to women than to
men.
Alcohol poses greater risk of cancer, and liver, digestive and cardiovascular diseases
to women than men. In addition, serious implications of excessive drinking in women
include increased mental health and social problems, and increased vulnerability to
crime and violence.
Older People
Older people in old age even modest use of alcohol can have a significant impact on
health and wellbeing.
Alcohol use amongst older people is more widespread and harmful than is
commonly realised, and it is a largely hidden and unacknowledged problem. Alcohol
problems may go undetected for longer in older people because they tend to be
more socially isolated.
Hazardous and harmful drinking is not often recognised in this group, and although
older people do not drink at levels associated with a 'drink problems, thephysiological and lifestyle changes that come with ageing can reduce tolerance and
increase risk factors, so that even moderate or low alcohol consumption can be
harmful. It can contribute to falls, compromise memory, affect the management of
medication, and contribute to inadequate diet and limitations on independent living.
Ethnicity
In 2004 the Health Survey for England showed that people from several black and
minority
Ethnic groups in England (Indian, Pakistani, Bangladeshi, Black Caribbean and Black
African) were on average more likely to be non-drinkers, and less likely to drink
above sensible levels or binge drink than the general population.
Despite this, they have a similar prevalence of alcohol dependence compared with
the white population.
The Irish community, however, are more likely to drink above sensible levels and to
binge drink than the general population.
Marital Status
Single men and women are more likely to drink above sensible limits than those who
are married.
The percentage of women reporting binge drinking is more than double the
percentage of married women: 19% compared with 8%.
Social Class
Social class is a risk factor for alcohol related mortality although the relationship is
more complex.
Generally the problems of heavy drinking are experienced more severely by people
from lower social classes.
Men in manual classes are more likely than men in professional classes to die of
alcohol related causes and this is most evident in 25 to 39 year olds.
In older women, professionals have the highest risk of dying from alcohol related
causes, in younger women; those in the manual classes are most at risk.
Other groups include ex-prisoners, homeless people, those who suffered abuse as a
child and those from a family where alcohol was misused.Chapter 3: Alcohol Related Harm – The Local Profile
Local information and data shows that alcohol misuse imposes a heavy economic, social and
personal cost on the people of Solihull.
Data from the alcohol needs assessment undertaken to inform this strategy show that:
In Solihull 44,905 people regularly drink at hazardous or harmful levels.
There are an estimated
o 21,423 abstainers
o 109,559 low risk drinkers
o 27,756 increasing risk drinkers
o 6243 higher risk drinkers
o 27,152 people who binge drink,
o 6,243 people who show signs of alcohol dependence
o 1,041 people are moderately or severely dependent on alcohol.
o Only a small proportion of these dependent drinkers are currently in
treatment services.
Alcohol specific mortality is increasing in Solihull. The directly standardised
rate/100,000 population (DSR) for the population is 10.8 (males is 13.6 and females
is 8.2).
Deaths from chronic liver disease are rising in Solihull
Alcohol attributable mortality for females is rising in Solihull.
Hospital admissions for conditions wholly attributable to alcohol have reduced for
males and females both nationally and for Solihull
The rate of male and female deaths from conditions partially attributable to alcohol
has fallen significantly in England between 2008 and 2012. Solihull has not seen the
same fall; the rates have been relatively stable.
11% of respondents felt drunkenness or rowdiness in public places was an issue for
Solihull.
There is evidence of an increasing prevalence of dual diagnosis of substance misuse
amongst individuals with a severe mental health problem in Solihull. For this client
group, the primary problem substance they present with is predominantly alcohol
(60%) then drugs (34%).
In Solihull we know that 32.2% of clients in structured alcohol treatment are living
with children
1 in 4 people in structured drug or alcohol treatment in Solihull have a housing
problem.
The proportion of Child Protection cases where the parent had a primary need code
of alcohol, accounted for 2.7% of active cases
44% of all violent offences in Solihull are alcohol relatedNight time economy
Solihull has a growing retail and leisure sector with over 16 million people visiting the
shopping centres and leisure complexes annually. There are many hotels, pubs, clubs and
restaurants in the borough that enhance and support the enjoyment of residents and
visitors. It is the intention of the Licensing Authority to encourage and facilitate a broad
range of entertainment provision by a wide cross-section of the public.
In Solihull there are thirteen premises that make up the night time economy together with a
large selection of restaurants, a cinema and other leisure activities in and around the
Touchwood Shopping Centre.
The clubs and bars all have late night licenses meaning that each of the premises close
between 23:00 through to 03:00 (the largest of these premises is Luna Nightclub with a
capacity of 950 all of the other premises have a capacity of 300 – 750).
The development of Park Gate in Shirley, Resorts World at the NEC and the proposed
developments within Solihull town centre, including the expansion of the Touchwood
shopping centre have seen and will see an increase in this sector within the borough.
Licensing policy & health
Solihull Metropolitan Borough Council is the Licensing Authority for this district and will
promote the licensing objectives set out in the Licensing Act 2003, which are:-
The prevention of crime and disorder
Public safety
The prevention of public nuisance
The protection of children from harm
Activities that require a licence under the Licensing Act 2003 and covered in the licensing
policy include:
retail sale of alcohol
supply of alcohol to club members
provision of 'regulated entertainment', to the public or to club members or with a
view to profit
The Responsible Authorities recognise that alcohol can cause harm. The Health and
Wellbeing Board and Safer Solihull Partnership are committed to reducing the harm caused
by alcohol, and will tackle the misuse of alcohol through the introduction of strategies and
approaches which aim to reduce the harm caused by alcohol to individuals, their families
and communities. This alcohol strategy forms part of this commitment and identifies
priorities for action. A number of awareness-raising campaigns and/or voluntary
arrangements may be useful in preventing/reducing alcohol related harm.Whilst public health is not a licensing objective, the Licensing Authority recognises that
there may be much input that Public Health can have in licensing in relation to the local
population and their alcohol related health needs. Health bodies may have access to data
that is not always available to other Responsible Authorities which can help inform licensing
decisions.
Public Health is able to provide useful evidence of alcohol related harm in relation to
cumulative impact. The Joint Strategic Needs Assessment which informs this alcohol
strategy, for example, has helped identify areas where there may be vulnerable groups who
may be at higher risk of alcohol-related harm and helped inform priorities for action.
Alcohol in the older population
An estimated 1.4 million people nationally in the older age group (defined as over 65)
currently exceed recommended drinking limits. From 2001 through to 2031 there is
projected to be a 50% increase in the number of older people in the United Kingdom.
Alcohol is known to have exclusive effects in the over 65’s due to co-morbidities,
pharmacological interaction, functional issues, and changes in body physiology. Indeed, the
Royal College of Physicians suggest that up to 60% of older people admitted to hospital with
heart failure, chest infections, and repetitive falls may be misdiagnosed alcohol abusers.
Alcohol misuse can also cause both structural and physiological changes to the brain and
the nervous system. It is estimated that between 50-80% of chronic alcohol abusers will
develop some element of cognitive impairment and it is likely that there is a large group of
older people with such problems that have been undetected.
There is currently no clear guidance on the safe levels of alcohol use in older people. The
Royal College of Psychiatrists (2011) has previously suggested that the recommended
drinking guidelines be reduced for older people.
Robinson and Harris 2011 estimate that 20% of men and 10% of women aged 65 and over
are drinking alcohol in harmful quantities and around 68% of harmful drinkers have alcohol
dependence. Applying this information as well as the General Lifestyle Survey to the over 65
population in Solihull, we can estimate that:
16,011 could be drinking as frequently as, 5 or more days in a week
13,847 could be drinking quantities above the recommended intake
3846 men and 2404 women may be drinking at harmful levels
4250 people over the age of 65 will be alcohol dependant. This equates to 2615 men
and 1635 women.
13% of drinkers in treatment in Solihull are over 60 years of age.Alcohol and young people
A significant proportion of Young People and adults consume alcohol at home, and
indications are this level is increasing in Young People. The Health Related Behaviour Survey
(HRBQ) 2014 includes data collected from a sample of primary pupils aged 6 to 11 and
secondary pupils aged 12 to 15. A total of 8,717 pupils took part in 66 Solihull Infant,
Primary, Secondary and Special schools.
Responses to the survey in Solihull seem to indicate a reduction in overall alcohol
consumption across all age ranges questioned. In 2010, 26% of pupils said they have
never had an alcoholic drink, this increased in 2012 to 32%, and 42% by 2014.
There has been a downward trend in primary pupils saying they drank alcohol in the
previous week. 17% year 6 pupils said they drank alcohol when the survey was
conducted back in 2004, this has fallen to 5% in 2012, and down further to 3% in
2014.
In 2010, 16% of year 8 pupils had an alcoholic drink in the past week, this reduced
down to 11% by 2012, and down to 5% by 2014. In relation to year 10 responses,
38% had an alcoholic drink in the past week, in 2012 this had decreased significantly
to 26%, and down further to 23% by 2014.
Responses indicate there has been a slight reduction in those pupils buying alcohol
from an off-licence. In 2010, 5% of pupils bought alcohol from an off license that
should sell only to over 18s; this had decreased down to 3% in 2012, and remained
at 3% in 2014.
Of those year 10 respondents who were drunk in the week before the survey, the
proportion was 9.9% in 2012; this had reduced down to 9% by 2014.
On the subject of drinking at home, of those Secondary pupils questioned, 8% of
pupils said their parents never or only sometimes knew if they drink at home, this
had reduced down to 6% by 2014. We know that drinking at home is increasing, so
this maybe adds evidence that parents are less aware of their drinking from home.
Tighter licensing laws in relation to selling alcohol in pubs and off-licenses in recent
years may be a contributing factor in this increase in Young People drinking at home.
The number of Young People in structured treatment continues to decrease in
Solihull.
Families and alcohol
In comparison with national figures it is clear that Solihull has a higher than average
proportion of clients in treatment who live with children.
The proportion in individuals in contact with alcohol treatment services who live
with children under the age of 18 in Solihull 2014/15 was 32.2% as compared to the
national average of 25.0% (PHE quarter 3 2014/15.) A similar theme is apparent in relation to new alcohol presentations that live with
children under the age of 18 with 30.7% in Solihull compared to 24.2% nationally.
(PHE quarter 3 2014/15).
Work conducted within SIAS over recent years to make the service more engaging
and welcoming to those clients with children, may be a reason for this high
proportion currently in treatment within SIAS, compared with the proportion
nationally.
Analysis has been conducted locally whereby a sample of Children’s Social Care assessments
during the period 1 April 2014 – 30 September 2014 were studied.
Of all assessments conducted, 8% feature alcohol and/or drugs as a factor. 5% had
alcohol misuse and 3% had both parental drug and alcohol misuse as factors.
An interesting finding was that 56% of assessments where drugs and/or alcohol are
factors, they also have Domestic Violence (DV) as a factor.
The Families First Programme in Solihull (now under Early Help) works with families that fit
the following criteria:
School attendance 85% or less over three school terms.
Unemployed and receiving Income Support.
Anti-Social Behaviour and Crime recorded for relevant individual.
Currently 75% of the families the team are working with have a substance misuse issue
within the family
As at October 2014, Families First were working with 64 families in Solihull. Of these
there were 15 cases where the family involved young people and drinking, 11 where
there were adult problematic drinkers (one known to be in structured alcohol
treatment).
Solihull alcohol awareness
Solihull’s Big Drink Debate was a resident based survey conducted in 2014, designed to
grasp the awareness of drinking behaviour and the perceptions of alcohol. The survey
sampled both Solihull residents and those that worked and socialised in Solihull. The results
showed that generally there was poor alcohol awareness in relation to recommended
quantities as well as concerning levels of reported drinking.
Only 18% of respondents knew the recommended safe drinking guidelines.
A third of men and a quarter of women drinking over the safe guidelines. Indeed,
88% of respondents had had a drink in the last week, and 7% were drinking six days
or more. A discrepancy arose in relation to the reporting of alcohol related Anti-Social
Behaviour (ASB). Although 18% of people had witnessed ASB in the last month, only
8% had reported it, suggesting that ASB is under reported.
The majority of respondents (61.7%) would prefer to get information and health
advice on safer drinking from a website/internet or from a doctor (47.3%).
With 50% of females and 30% of males believing that knowledge of the calorie
content of drinks would affect the amount they drink; initial results imply that
increasing awareness could help reduce alcohol consumption.
In order to glean a qualitative element to the survey findings, subsequent focus groups were
set up. Themes that were highlighted as to the cause for Solihull’s expansive drinking
behaviour were:
Increased availability – it was noted that with alcohol being cheap and ever-present
in the supermarket aisles, drinking has now become much easier than it has ever
been.
Drinking at home - this is related to the above point. Other reasons included the
added cost of drinking in a social setting and the normalisation of such behaviour in
current society. Drinking in isolation at home removes the monitoring of ones
drinking that can take place in the social setting.
Poor wellbeing as a cause – Both stress and boredom were highlighted as key
influences as to why people drink alcohol. Alcohol can then become a means to
cope. The focus groups highlighted that in order to combat this there should be
greater targeting of improvement of financial, psychological, and social support to
vulnerable individuals.
Solihull Community Perceptions
The Place Survey is an annual survey conducted in August, which was circulated to nearly 700
households in Solihull. Respondents were given nine types of Anti–Social Behaviour (ASB) and asked
whether each was a problem in their local area. Of those who responded to the 2014 survey people
citing drunk or rowdy behaviour as a problem saw a significant decrease in respondents
citing this as a problem. In 2014, just 7% of respondents felt this was an issue; this has
decreased from 17% in 2011, down to 16% in 2012, 11% in 2013.
Alcohol Related Crime
In Solihull the number of violent crimes are low, but the consequence of these are high. The
public are aware that alcohol is linked to crime in the borough; evidence suggests that
crimes linked to alcohol include domestic violence, violence and antisocial behaviour linked
to the nightime economy. The volume of alcohol related crimes recorded is increasing in Solihull. (663 crimes
recorded as alcohol related, compared to 482 previous year). The Key location
remains High Street, town centre.
Number of violent crimes per month has increased on average from 217 to 250 in
2015/16.
Between 1st October 2014 and 30 September 2015 there have been 663 crimes
recorded as alcohol related from 429 unique locations. There have been 100 repeat
locations but only one with an average of more than one incident each month
Half of these crimes are recorded as Violent Crime HOMC 008 (329 – 194 Assault
Occasion ABH, 84 Malicious Wounding, 27 Inflicting GBH without intent) with a
further 86 recorded as Common Assault and 65 as Criminal Damage
One in three crimes recorded as alcohol related were recorded as domestic violence
in 2014/15.
Four in ten (267) of the crimes recorded as alcohol related were recorded within a
dwelling
17% (112) were specifically linked to a licensed premises
Considering the volume of people attending the night-time economy within Solihull Town
Centre, the levels of crime and disorder are low. That said this area remains a key location
for further opportunities to reduce violent crime.
Current early identification and brief interventions
Brief / Early interventions are provided in Solihull by any service that uses the audit tool,
including:
Health Checks
GP Practices
SIAS
HEFT/MECC
Health Trainers
However there is no consistent approach to early identification and brief interventions.
An Alcohol Brief Advice audit was undertaken in Heart of England hospitals to capture the
use of alcohol screening from frontline staff in OPD, Gastroenterology, Trauma and
Orthopaedics, Respiratory, and Pre-Operative Assessment Clinics.
In Solihull OPD alcohol screening was routinely delivered on all new patients.
Surprisingly no routine screening was delivered on the gastroenterology ward in
Solihull Hospital, presumably because staff feel that if alcohol is a problem it will
have been diagnosed and treated. No alcohol screening was routinely delivered on Cardiology or Respiratory Wards nor
was alcohol screening was routinely delivered at pre-Operative Assessment Clinics or
in Trauma and Orthopaedics.
Brief advice is to be delivered when a patient scores 3 or more on the FAST pre-screening
tool.
The vast majority of staff in wards and departments where screening was routine
and who raised the issue about alcohol knew this was the score which should
prompt delivery of brief advice.
In wards and departments where screening was not a routine occurrence,
knowledge of the threshold score was much less.
Delivery of alcohol brief advice was slightly patchy; not always being delivered after
a screen had been done. Usually brief advice was delivered verbally but without the
use of a "brief advice sheet".
Brief advice for alcohol, when following a screen, should always involve discussion
with the patient of the screen result, and the meaning of that result for the patient
in particular. In some cases, brief advice consisted of a leaflet being given to a
patient to take away and read, with little verbal discussion of the screen results.
Following the alcohol screen, the threshold score for referral to specialist services (if FAST is
used) is 7.
Knowledge of this referral threshold was mixed, even in wards and departments
where screening routinely took place.
A familiarity with Specialist Service staff was welcome and increased staff's
confidence in making a referral. In some cases there seemed to be no current access
to Specialist Staff although there had been in the past
Alcohol brief advice training is available via Moodle and had been accessed by some staff,
including all OPD staff in Solihull Hospital. However, the Moodle training had been
unavailable for some months and has only recently been reinstated, so that may explain
some staff not being trained.
There were a number of barriers cited with respect to screening and brief advice.
Lack of time was referenced fairly frequently as the main barrier to either delivering
a MECC conversation or to having a lengthier brief advice discussion.
A few staff had experienced patients being offended by being asked about their
lifestyle habits and this had made them feel reluctant to deliver further MECC.
In OPD in particular it was felt that the brief advice should really comprise a leaflet or
information about where to go for more help /referral rather than any conversation
about risks due to the time constraints in a very busy department. Role legitimacy was a concern for some staff. This is reflected from the traditional
role of nursing staff in secondary care to be providers of treatment rather than
providers of preventative care.
Role adequacy was also an issue for a minority of staff. Typically, where the staff
member had experienced s difficult conversation with a resistant patient, the staff
member felt a degree of lack of confidence to manage some MECC conversations
Current treatment services
The alcohol treatment service operating within the Solihull Integrated Addiction Services
(SIAS) has been established for some five years now.
Most recent performance information indicates that there are 703 clients in contact
with alcohol treatment system in Solihull. Locally a minimum performance standard
is of 750 in treatment for 2015/16, and an aspirational target of 790, so an
improvement in current performance is required.
The number of clients presenting with alcohol as their primary problem substance in
Solihull has decreased over the last two years, from 493 in 2013/14 to 362 in
2014/15 according to the Recovery Diagnostic Tool (RDT).
Compared to the national average, Solihull has a higher proportion of clients in
treatment for over a year.
Solihull clients in alcohol treatment on average spend 247 days in treatment, 71 days
longer than the average client in alcohol treatment nationally.
A lower proportion of clients exit treatment in Solihull in the first 3 months of treatment,
whereas a higher proportion of clients exit treatment after 9 months in treatment in
Solihull. In summary clients are staying in treatment longer, and exiting treatment later
than is the case nationally.
Solihull has less early discharges than is the case nationally, less than 3 months into
treatment, Solihull has 24% discharges, nationally 38%.
Solihull has more late discharges than is the case nationally, 9mths + into treatment,
25% in Solihull, just 17% nationally.
Completion rates have dropped for those at the early stages of their treatment
Rates were at 10% for 2011/12 for those new presentations that ended in an
unplanned exit within three months of starting treatment. This rate increased to
12% in 2012/13, 24% in 2013/14 and dropped slightly to 18% in 2014/15, when the
rate nationally was 17%. Solihull are also performing poorly in relation to completion rates by previous
treatment journeys, in that for those with four or more treatment journeys the
proportion was 9%, compared to 30% nationally.
There has also been a decrease for clients with no previous treatment journeys.
Re-presentation rates in Solihull are worse than the national average at 12%
compared to 10% nationally for alcohol clients. There is generally a lower
consumption of alcohol by clients in Solihull when they start treatment compared to
the national average. However, completion rates for those drinking at higher levels
are generally above the national average.
In Solihull those clients in treatment for alcohol are predominantly male (58%),
slightly lower proportion than is the case nationally. (62%)
Solihull appears to have a slightly different age range in treatment to the national
picture.
A lower proportion of people in treatment under the age of 39 in Solihull, especially
males 22% against 32% nationally.
Higher proportion of over 60’s in treatment in Solihull than is the case nationally,
15% compared to 11% nationally.
Clients in Solihull receive quick prompt access to alcohol interventions. 98% of adults
wait less than 3 weeks to start their treatment (95% nationally).
Self referrals remain the main source where clients are referred into SIAS for alcohol
treatment (51%)
Just 4% of referrals to structured treatment in Solihull come from a criminal justice
route, exactly half the proportion that enter the system nationally.
Solihull has a significant proportion referred to alcohol treatment through the
Hospital/ A & E route, 14% compared to just 8% nationally.
Solihull clients in alcohol treatment appear to have less additional substance misuse
compared to national figures.
Alcohol and opiate use 3% in Solihull compared to 7% nationally.
Alcohol and non opiate use 18% in Solihull compared to 19% nationally.
Alcohol, opiates, and non opiates use, 6% in Solihull compared to 15% nationally.
Good employment opportunities in Solihull, of those in treatment, 44% employed,
compared to 27% nationally.
In Solihull, 24% were unemployed, compared to 37% nationally.
Those in alcohol treatment, with a Housing problem in Solihull 8%, against a national
proportion of 11%.Chapter 4: Where are we now? Where are the Gaps? While the majority of people enjoy alcohol with few if any problems, it does impact on crime and the health of communities and individuals in a variety of ways that demand a coherent and sustained vision for change. The consultations that have taken place to develop this strategy have identified a wide range of interventions and activities that are already in place in Solihull and are making a contribution to tackling problems of alcohol misuse in the Borough. The consultations and service reviews also identified that there are significant gaps in provision, we can and need to do more to reduce the negative effects of alcohol use in the Borough. 1. Prevention through education and communication Current provision Schools Currently around 85% of Solihull schools are recognised as Solihull Healthy Schools. This means that they have met a range of requirements linked to the health and wellbeing of pupils and staff, this includes having a current drug and alcohol education policy including how substance related incidents are dealt with. This policy is developed and reviewed through a whole school approach including the voices of pupils, staff, governors, parents and the wider community where appropriate. Solihull Healthy Schools must also have a taught programme of PSHE which includes drug and alcohol education. Solihull Metropoliton Borough Council commission Solihull Education Improvement Service to deliver Exploratory Behaviours work which involves leading, developing, supporting models of good Substance/ Alcohol Misuse Education (SAME) practice in education settings across the Borough. The outcomes include a reduction in the likelihood of young people experimenting with or becoming addicted to illegal drugs and alcohol, a reduction in the level of substance misuse related problems within the community and reduced harm as a result of risk taking, particularly associated with alcohol. The Solihull Education Improvement Service also deliver training for foster carers about drug and alcohol education. Peer led programmes Urban Heard is a peer-peer led behavioural change Solihull Youth Engagement Programme that works to build resilience and provide effective solutions for young people’s risky behaviours. They have been involved in a number of campaigns to raise alcohol awareness in young people. They run prevention projects across Solihull which are based on a three stage model of 1) workshops 2) recruiting, training and paying young people aged 14-17 to create campaign strategies for prevention against risky behaviours 3) implementing these
campaigns in the community and on social media. They now work under the umbrella of SIAS and work closely to provide referrals into the service. Communication events Chillax events are to provide harm reduction advice and information, and signpost to treatment/support to individuals who may be at risk of consuming too much alcohol, being spiked, or taking illicit substances on a night out within the Solihull Borough, numerous Chillax events have taken place jointly with the police and SIAS staff, these events have been very well received. SIAS has delivered Alcohol awareness training as part of alcohol awareness week, which was opened up to all professionals within Solihull. These events have been planned to coincide with national campaigns etc. They also attend various team meetings for professionals across Solihull to give basic information and to discuss referral pathways. Police Patrols Officers on Night Time Economy patrols have access to non-evidential breathalysers as an engagement tool, they can engage with the revellers as they leave the licensed premises. They can identify early those that need to be engaged with and offer them the chance to see how much alcohol they have in their system at that time, by the time you have breathalysed one of them you find that the group they are with all want to know how much alcohol they have in their system and how the alcohol effects them / how long it stays in their system etc. There is an opportunity to work closer with SIAS at these times as a type of street outreach work. Outreach The main premises in Solihull have introduced the last drink to be a free bottle of Water with free toast which has proved to be very popular. They have also offered an opportunity for SIAS to have a table next to the free water and toast allowing them to engage and educate where necessary. National Campaigns There are also a number of national alcohol specific e.g. dry January and more general campaigns e.g. One You that help to raise public awareness of limiting alcohol. Gaps Parent information There have been minimal parents-focused campaigns that inform a better understanding and sense of parental responsibility in managing the risks associated with underage drinking. Such campaigns may include working directly with parents, providing the
You can also read