Department of Health and Social Care (DHSC) COVID-19 Response National Testing Programme Clinical Standard Operating Procedure (SOP) for Mass ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Department of Health and Social Care (DHSC) COVID-19 Response National Testing Programme Clinical Standard Operating Procedure (SOP) for Mass Testing with Lateral Flow Antigen Testing Devices in Schools and Colleges Version 2.3 Date of publication:31/12/2020 Contents
1. Introduction ....................................................................................................................................................................6
2. Public Health Objectives .................................................................................................................................................6
2.1 Programme Overview ...............................................................................................................................................6
2.2 Public Health Aims ....................................................................................................................................................8
2.3 Evaluation .................................................................................................................................................................9
3. Clinical Governance ........................................................................................................................................................9
3.1 Clinical governance framework ................................................................................................................................9
4. Testing Technology .......................................................................................................................................................13
4.1 Lateral Flow Antigen test ........................................................................................................................................13
4.1.1 How the test works .........................................................................................................................................13
4.1.2 Implication of LFD results ................................................................................................................................13
4.1.3 Product specifics..............................................................................................................................................14
4.1.4 Temperature control .......................................................................................................................................14
4.1.5 Instructions for use (IFU) .................................................................................................................................14
5. Workforce .....................................................................................................................................................................14
5.1 Roles and responsibilities .......................................................................................................................................14
5.2 Training and competence .......................................................................................................................................16
6. Site Set-up.....................................................................................................................................................................16
6.1 General site selection criteria .................................................................................................................................16
6.2 Co-located sites: .....................................................................................................................................................17
6.3 Testing site set-up: .................................................................................................................................................17
7. Testing Process .............................................................................................................................................................18
7.1 Consent...................................................................................................................................................................18
7.2 Eligibility .................................................................................................................................................................19
7.3 Test Register ...........................................................................................................................................................20
7.4 Registration of each test for Test & Trace purposes ...............................................................................................20
(Using the Register a coronavirus test (lateral flow test) service) .................................................................................20
7.5 Face coverings ........................................................................................................................................................21
7.6 End to end testing process overview ......................................................................................................................21
7.7 Detailed testing process for on-site testing ............................................................................................................23
7.7.1 Self-swabbing sample collection procedure:...................................................................................................23
7.7.2 Administered Swabbing ..................................................................................................................................25
7.7.3 Sample processing and analysis procedure .....................................................................................................25
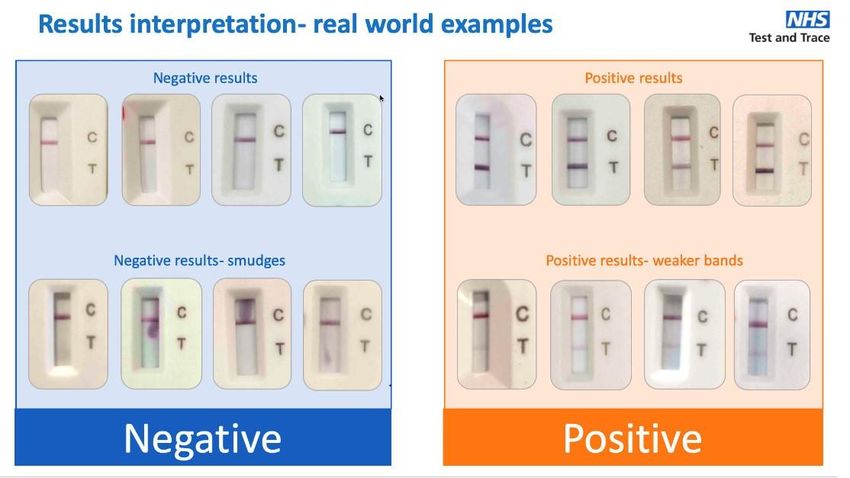
7.7.4 Reading and interpreting LFD result................................................................................................................26
7.7.5 Recording of results.........................................................................................................................................28
7.7.6 Communication of results ...............................................................................................................................29
Schools and Colleges Clinical Standard Operating Procedure 2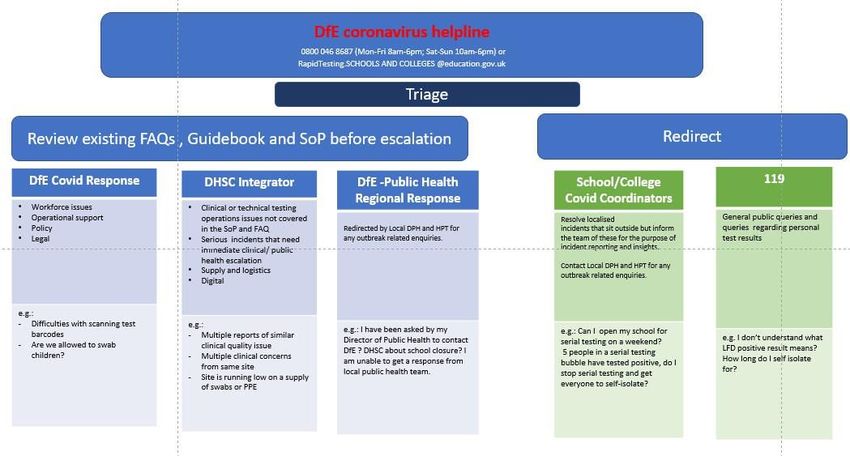
7.7.7 Reporting .........................................................................................................................................................29
7.7.8 Negative results...............................................................................................................................................29
7.7.9 Invalid results ..................................................................................................................................................30
7.7.10 Positive results ..............................................................................................................................................30
7.7.11 Confirmatory PCR ..........................................................................................................................................30
7.7.12 Travel advice for positive results ...................................................................................................................30
8. Daily contact testing after a positive case ....................................................................................................................31
8.1 Initial case finding ...................................................................................................................................................31
8.2 Daily Contact Testing ..............................................................................................................................................31
8.2.1 Daily testing over weekends and holidays ......................................................................................................32
8.2.2 Contacts who do not wish to be part of the process.......................................................................................32
8.2.3 Persons who become symptomatic during the process ..................................................................................32
9. Quality management ....................................................................................................................................................33
9.1 On-going programme-level evaluation...................................................................................................................33
9.2 Site level quality management plan .......................................................................................................................33
10. PPE ...............................................................................................................................................................................34
10.1 PPE by roles ..........................................................................................................................................................34
10.2 Other IPC precautions...........................................................................................................................................34
10.3 Infection prevention and control: equipment ......................................................................................................35
11. Data Management .......................................................................................................................................................35
11.1 Data control ..........................................................................................................................................................35
11.2 Data Protection Responsibilities ...........................................................................................................................35
12. Appendix A: Infection Prevention and Control (IPC)....................................................................................................36
12.1 General guidance..................................................................................................................................................36
12.2 Cleaning policy......................................................................................................................................................36
12.3 Hand sanitisation ..................................................................................................................................................38
13. Appendix B: Waste Management ................................................................................................................................38
14. Appendix C: Site Layout ...............................................................................................................................................40
14.1 Organisations to build their own site ...................................................................................................................40
15. Appendix D: Self-swabbing Instructions ......................................................................................................................42
16. Appendix E: PPE instructions – putting on and taking off............................................................................................43
17. APPENDIX F: MHRA WEEKLY REPORTING TEMPLATE .................................................................................................44
18. Appendix G: COVID-19 Testing Privacy Statement for Educational Establishments ....................................................45
19. Appendix H: Consent Template ...................................................................................................................................49
20. Appendix I: ATS Risk Log ................................................................................................. Error! Bookmark not defined.
Schools and Colleges Clinical Standard Operating Procedure 3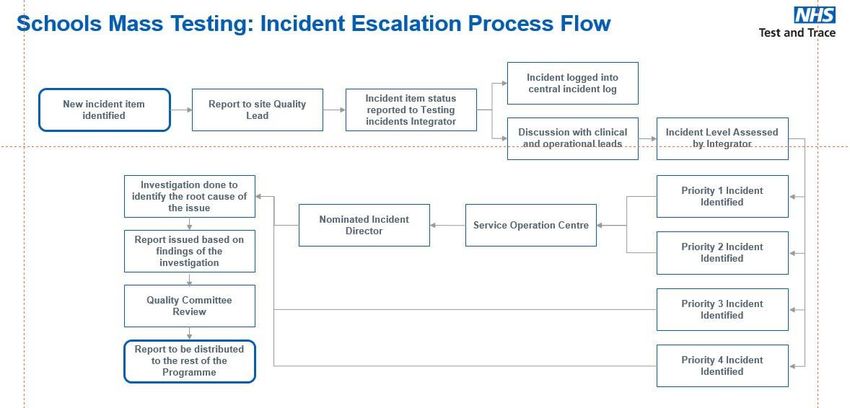
Document Control and Approval Version Control
Version Author Summary of Changes Reviewed By Date
1.0 Schools and Adapted for schools and colleges usecase from ATS Master NHS T&T 23/12/2020
colleges Mass SOP template v2.8 released 09/12/2020 and daily contact Schools Mass
Testing Team testing template. Testing Lead
1.1 NHS T&T Policy Daily Contact Testing to replace serial contact testing;
Team changes to 10 days for quarantine.
2.0 Schools and Changes made in response to feedback by DfE NHS T&T 28/12/2020
colleges Mass Schools Mass
Testing Team Testing Lead 30/12/2020
2.1 Schools and Changes made to recorder PPE and results recording IPC Specialist 30/12/2020
colleges Mass section PHCO,
Testing Team DHSC
2.2 Schools and Changes made following Julia Dudley feedback for user DfE 31/12/2020
colleges Mass journey and test registration
Testing Team
Approval
Cell Name / Role Review / Approval Version
Reviewed /
Approved
Review & Approval Dr Tom
National Testing Programme Alan
Health Protection and Public Fowler Dr
Peter
Health Leads, DHSC
Marks
Approval Chief
Medical
NHS Test & Trace
Advisor
Department for Education Review
Schools and Colleges Clinical Standard Operating Procedure 4
Lateral Flow Device SOP Scope Summary
Use Case: Schools and FE colleges
Institution: National roll-out
1. Public health aim
Active case finding through regular asymptomatic testing
☒
Enablement through daily contact testing
☒
Surveillance ☒
2. Testing frequency
Frequency of Testing 1. Test on Return: Only for Students; Two tests 3-5 days parts
(per individual within population) 2. Routine case Finding: Only for Staff; weekly testing
3. Daily Contact Testing: 7 days* for staff and student contacts of staff who
have tested positive
3. Pilot includes a research study?
Click the relevant box below to mark with an ‘X’
☒ No, not a pilot ☐ Yes, ethics approval granted ☐ Yes, ethics approval required
4. Lateral Flow Device
At the time of writing this document, only the Innova SARS-Cov-2 Antigen Test feature in this SOP, once additional devices are approved for testing, they
will be updated into the SOP
Innova SARS-CoV-2 Antigen Test IFU ☒
5. Situation in which LFD will be used
Post-Pilot Roll Out – DHSC clinical responsibility ☒
6. Population tested
This document has been written on the basis for asymptomatic testing only
Click the relevant box below to mark with an ‘x’
☐ Symptomatic ☒ Asymptomatic
7. Sample type
Throat and Mid-turbinate Nose Swab (where possible) X
8. Sample collection method
☒ Administered (specific scenarios) ☒ Self-swabbed
9. Sample preparation, application to LFD and results interpretation
☒ Assisted ☐ Self-implemented
Schools and Colleges Clinical Standard Operating Procedure 5
1. Introduction
This is the standard operating procedure (SoP) for mass asymptomatic testing case finding and daily contact
testing using lateral flow antigen testing in schools and colleges in the UK.
The SOP is designed for safe implementation of approved lateral flow antigen testing processes where on-site
clinical oversight is not required. The document describes the appropriate clinical governance and infection
control for sampling and testing procedures at asymptomatic testing sites (ATSs), responsibilities of site staff,
how to conduct interactions with people being tested, and clinical data management principles. The document
also covers self-administration of the test, where appropriate.
This SoP applies to schools and colleges in England. For Devolved Administrations, the SOP will be reviewed
and adapted by the respective agencies for roll-out.
The SoP is the foundation document for this programme. DHSC will review incident reports/ feedback and
regularly update the SoP if there are common issues that require a response.
2. Public Health Objectives
2.1 Programme Overview
(1) Test on Return: Rapid asymptomatic tests using Lateral Flow Devices (LFDs) to test as many
secondary-age and further education students as possible, who will resume face to face education in
January.
Rationale: Mass rapid asymptomatic testing is aimed at reducing the risk of spread of Covid-19. It will help to
identify more infectious cases before a full return of students and help maximise attendance when schools
and colleges return to face-to-face teaching while minimising community transmission in this age group.
This one-off testing is undertaken to reduce risk of individuals entering into a new environment where there
is substantial risk of onward spread, especially subsequent to an event that has increased overall risk that
those individuals have infection (e.g. relaxation of rules over Christmas). The following has been taken into
account in deciding that two LFD tests are appropriate and the timing between those tests:
• Antigen LFD tests have higher sensitivities with higher viral loads. Given this variation in sensitivity,
one LFD test may miss people who are in the early stages of COVID infection with lower but
increasing viral loads and give a false negative result1.
• Repeating the test a number of days later may pick up some of these false negatives as the viral load
becomes higher2. The period of infectiousness of 4.32+/-1.09 days3 would support an interval
between two tests of 3-5 days apart for students and weekly tests for staff.
• There is currently no quantitative evidence to demonstrate how many additional cases would be
picked up by the second test therefore continuous evaluation during these rollouts will help quantify
the benefits of a two-test regime.
1 https://www.ox.ac.uk/sites/files/oxford/media_wysiwyg/UK%20evaluation_PHE%20Porton%20Down%20%20University%20of%20Oxfor
d_final.pdf
2 https://www.nejm.org/doi/pdf/10.1056/NEJMp2025631?articleTools=true
3 https://cmmid.github.io/topics/covid19/reports/2020-12-04-quar_test_contact_tracing.pdf
Schools and Colleges Clinical Standard Operating Procedure 6
Target population: Secondary schools (including all-through schools and middle deemed secondary schools),
colleges, special schools and colleges and AP students. In middle deemed secondary schools, testing would be
for Year 7 and 8 pupils.
Testing regime: Two LFD tests spaced 3-5 days apart for students, and weekly tests for staff, from 4 January
2021, with confirmatory PCR for positive cases.
Methodology:
Tests will be based on self-swabbing model with the processing and other roles being undertaken by trained
workforce.
The groups attending school and college from 4 January will be prioritised for rapid asymptomatic testing,
alongside the school workforce.
Those who test positive from an LFD test will be required to self-isolate in line with the Stay at home: guidance for
households with possible or confirmed coronavirus (COVID-19) infection and to take a confirmatory PCR test.
PCR kits will be provided to the schools to be hand out to parents / guardians in the event of a positive LFD
test result to support swift access to these tests.
(2) Routine Case Finding: designed for rapid identification of asymptomatic positive cases to reduce
onward transmission within the schools and colleges
Rationale: Up to a third of people with Covid-19 infection can be asymptomatic. These people can still spread
infection4. School closures have had major academic, psychological and societal ramifications for students
and are expected to worsen inequality in education5.
These educational settings have been prioritised for testing because they have seen more disruption so far,
associated with older children and young adults having recently had higher rates of coronavirus (COVID-19)6.
They are therefore more likely to spread the disease so targeting them will help to reduce transmission in
these settings. The testing has been initiated first with school/college staff to balance operational feasibility
and impact of teacher absence on continuity of education.
Target population: Staff in secondary schools and colleges (including all-through schools and middle deemed
secondary schools, special schools and AP)
Testing regime: once weekly routine LFD testing for all participants with confirmatory PCR for positive cases.
First test will take place as soon as possible on physical return to school for each member of staff to avoid
transmission, followed by weekly tests.
Methodology: Onsite self-swabbing followed by processing of swabs by trained staff
(3) Daily Contact Testing: The close contacts of positive cases can be tested daily, to quickly find further
positive cases. If close contacts agree to be tested each day for 7 days, and they test negative each time, they
will be allowed to remain in school/college each day. Should a close contact be unable to test due to absence
or it being a non-school day they are required to self-isolate for those days.
4
Cevik, M. et al. https://www.medrxiv.org/content/10.1101/2020.07.25.20162107v2
5 https://en.unesco.org/covid19/educationresponse/consequences
6 School Infection Survey.
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/covid19schools and
collegesinfectionsurveyround1england/november2020#background-to-the-survey
Schools and Colleges Clinical Standard Operating Procedure 7
Rationale: Evidence indicates that regular LFD testing for 7 days appears to avert a similar proportion of
transmitted cases to that of the 10 day quarantine, allowing for the reduction of or removal of the quarantine
requirement for traced contacts7.
Target population: Staff and students in secondary schools/colleges (including all-through schools and middle
deemed secondary schools, special schools and AP) who are key stage 3 or above and have been contacted
by Test and Trace and told to self-isolate because they are contacts of those who test positive on LFD during
routine case finding.
Testing regime: daily LFD testing for a 7day period as an alternative to self-isolating for individuals who test
negative, with isolation for weekend days when not attending the college or school
Identification of contacts and daily contact testing should start from the day a positive case is identified on
LFD and continued until or unless the confirmatory PCR test is negative for that contact.
If anyone participating in daily contact testing is found positive, they will undertake a confirmatory PCR test
and self-isolate for 10 days from the date of the positive test result (and while waiting for confirmatory PCR
result).
If PCR is positive, daily contact testing restarts for another 7 days.
The intention is for daily contact testing to be conducted by consenting contacts for 7 days following contact
with a positive case. Where the school/college is not open to support daily contact testing over the weekend
or bank holidays, participants will be required to self-isolate on days where a test has not been performed.
If the last day of daily contact testing is on a day when testing is not available (e.g. the weekend), a further
negative test on first day back to school/college will be required to complete release from daily contact
testing.
Methodology: Onsite self-swabbing
2.2 Public Health Aims
Active Case Finding
Identify positive cases of COVID-19 and ensure they self-isolate to reduce transmission to other people;
Enablement
Reduce absences and minimise impact on education continuity by allowing asymptomatic contacts who
test negative on repeated daily contact testing to return to daily activities.
Surveillance
Provide further information on asymptomatic transmission in addition to the ongoing COVID19 surveillance
in the school population and targeted local public health response with LAs to prevent spread to the wider
community.
7 https://cmmid.github.io/topics/covid19/reports/2020-12-04-quar_test_contact_tracing.pdf
Schools and Colleges Clinical Standard Operating Procedure 8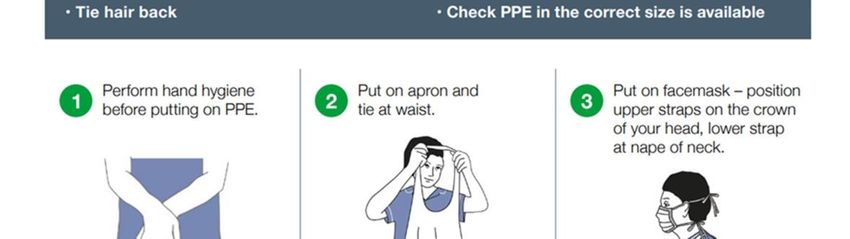
2.3 Evaluation
The evaluation of this programme will cover
1. Operational Performance
• The acceptability of the testing regime to staff, students and wider school stakeholders
• The operational burden on the school of delivery
• The operational performance of the LFD testing regime (coverage, void rates, reporting errors
etc.)
2. Clinical and Public health effectiveness
• The incremental case-finding ability of asymptomatic LFD testing
• The effectiveness of the repeat testing strategy at reducing onward transmission
• The acceptability and uptake of the intervention
• The number of daily testing bubbles that have to revert to self-isolation because of too many
positive cases found on daily testing
3. Broader societal benefit from health policy
• Reduction in in-school days lost to self-isolation
• Lower spend by school on supply teachers to replace staff who are isolating
• Benefit to parental / guardian days lost to caring for a self-isolating student
3. Clinical Governance
3.1 Clinical governance framework
The clinical oversight for this testing will be provided by NHS Test and Trace and the Department of Health and
Social Care (DHSC). Department for Education (DfE) is responsible for delivery of this programme, ensuring the
clinical requirements are in place with appropriate support, and providing information to NHS Test and Trace
that will enable their oversight.
There are 3 aspects of this process in schools and colleges:
A. Quality assurance of testing service
The clinical SoP and associated documents/ templates for consent, risk management, competency and
quality checklists will provide support to the schools and colleges to deliver the testing as a safe and
good quality service.
In addition, via the DfE Helpline, schools and colleges will be provided routine clinical operations
support.
DfE will collate and provide bi-weekly quality assurance reports to DHSC Clinical Governance Group.
These reports will cover testing operation performance, incident deep dives, learning and
improvement themes.
B. Incidents reporting and response
DfE coronavirus helpline: 0800 046 8687 (Mon-Fri 8am-6pm; Sat-Sun 10am-6pm) will be the single
point of contact for any queries. If it is confirmed that the incident is related to test kit or process
(not routine operational site management, supply, workforce etc.), the institution will be required to
Schools and Colleges Clinical Standard Operating Procedure 9
complete a DHSC LFD incident form. The DHSC incident response team will triage and report
incidents to MHRA, as needed.
All school/college testing sites will be registered with the MHRA by the NHS Test and Trace and
regular reports will be sent to MHRA using the form enclosed in Appendix F. These reports will be
collated by DfE on weekly basis
Figure 1: Schools Testing Incidents Reporting and Response Framework
Figure 2: NHS Test & Trace / DHSC Testing Incidents Escalation and Review Process
Schools and Colleges Clinical Standard Operating Procedure 10C. Managing downstream response to testing
Due to downstream implications such as local outbreak response, Directors of Public Health (DPH) and PHE
Health Protection Team need to be aware of schools and colleges plans to participate in the mass testing
programme.
In the majority of scenarios such as multiple positive cases during asymptomatic testing or multiple members
of a daily contact testing bubble turning positive during seven day testing period, the local public health and
health protection teams and Regional Schools Commissioner teams will continue to support a school/
college’s response, as they do currently, by drawing on their expertise in epidemiology, analysis, infection
control etc. to take critical decisions such as discontinuing daily contact testing to break the chain of
transmission and enhancing local contact tracing outside of school etc. In exceptional cases, if an outbreak or
incident response requires additional support or intervention, NHS Test and Trace Teams will work with local
areas to provide support. This will be done as part of the current local and regional response in the Contain
Framework.
NHS Test and Trace National Covid-19 Response Centre (NCRC) will coordinate national monitoring of
outbreaks potentially associated with daily contact testing implementation to give a programme wide
assessment of implementation. This will feed into the clinical governance structure to enable rapid action
should this be required
Regulation
Institutions in England providing Covid-19 testing under a government directive, do not need to be registered
with Care Quality Commission to provide these services.
Schools and Colleges Clinical Standard Operating Procedure 11Accountability
All school testing sites are under the clinical governance and oversight of the National Testing Programme
review.
Department for Education will be responsible for the following:
1. Overall operational delivery oversight of the programme
2. Helpline service for technical and operational aspects of lateral flow testing
3. Central incident tracking and triage system
4. Coordinate reporting back to DHSC on clinical assurance
5. Help MHRA on LFD testing
6. Support for local response by
• Central team on-call operations support
• Providing a crucial link between local, regional and national response
• Providing advice and support for escalating critical issues
• Issuing frequently asked questions and best practice advice
Department of Health and Social Care (DHSC) will provide the following:
1. Clinical Standard Operating Procedure (this document)
2. Test kits, PPE, test registration cards (physical or electronic format) and barcodes
3. Guidance for how to design, setup and run asymptomatic testing
4. Training for test site workforce (delivered digitally)
5. Example test area schematics to help design the testing site
6. Standard site collaterals (provided in electronic format)
7. Templates for Site Risk Assessment, staff competency checks, incident reporting, MHRA reporting
8. Registration and result notification system
The school is accountable for:
1. Ensuring appropriate local oversight and governance
2. Providing safe care and testing in line with the SoP, which is described in the training, ‘how to’ guide
and other supporting materials supplied by DfE.
3. Consent for testing
4. Ensuring appropriate safeguarding measures are in place
5. Ensuring staff are appropriately trained to undertake testing
6. Reporting and responding to incidents: Set up incident management system and escalation protocols
7. Appropriate Premises- identify and set-up suitable indoor site for testing and storage
8. Supplies- manage and track equipment required for the set-up and day to day running of a test site,
including site supplies besides test kits and PPE
9. Communication and engagement plan with local stakeholders
10. Operate an appropriate booking system to schedule testing
11. Alignment with local public health response to Covid-19
Schools and Colleges Clinical Standard Operating Procedure 12Designated Person
Each site will be required to designate a member of the team to act as Quality Lead who can be the site co-
ordinator or testing supervisor, as appropriate. This individual will have accountability for the quality of the
service within the context of a non-laboratory environment testing. The nominated Quality Lead will
undertake the following:
• Ensure quality assurance, incidents, risks mitigation across the testing service
• Implement appropriate quality assurance as defined by the Programme
• Implement the incident and risk reporting system that is used within the mass testing
programme
• Report data to NHS Test and Trace Mass Testing Quality Committee and MHRA through DfE
• Undertake testing staff competency and performance reviews
Testing Site and Operations Risk Assessment
Each school will need to have a risk assessment in place prior to sign off for launch. The risk assessment
should be completed jointly by the school and various service providers (such as any third party supplier of
workforce or equipment) involved in the delivery to testing.
A template for risk assessment is enclosed along with this SoP.
4. Testing Technology
4.1 Lateral Flow Antigen test
Lateral Flow Antigen testing involves the processing of human nasal and throat swab samples with a Lateral
Flow device. The device detects a protein (antigen) produced by the virus at its most infectious stage. If
present in the person’s sample, a coloured line appears on the device that can be read between 20-30
minutes.
4.1.1 How the test works
The swab sample is added to a fluid in the test kit. This fluid acts as an extraction buffer and is optimised to
release viral antigens from the specimen if they are present. During the test analysis, these antigens migrate
along the strip in the lateral flow device, binding to anti-SARS-CoV-2 antibodies located in the strip. The
antibodies are linked to coloured/ particles. The presence of a coloured band in the test region indicates a
positive result for the SARS-CoV-2 viral antigens, while its absence indicates a negative result. In general, it
takes up to 20 minutes for a positive result to appear. The manufacturer’s guidance is to wait a full 30
minutes to confirm that a result is negative.
Training in handling and analysis of the samples, including relevant principles of infection prevention and
control, will be provided to all operators at each testing site.
4.1.2 Implication of LFD results
If the result of LFD is positive, the person will be asked to undertake a confirmatory PCR test and selfisolate
while waiting for PCR results.
It should be noted that a negative result does not rule out SARS-CoV-2 infection and there can be false negative
results. If LFD test is negative but the subject has indicative clinical symptoms, a repeat test should be
undertaken using PCR to detect presence of SARS-CoV-2 RNA.
Schools and Colleges Clinical Standard Operating Procedure 134.1.3 Product specifics
The Lateral Flow Device products being used in this testing programme have undergone validation for NHS
Test and Trace. The Lateral Flow Devices are also CE certified.
Some of the operational implementation may be outside the manufacturer’s instruction for use (IFU). Risk
assessments have been conducted at the request of MHRA for these areas. MHRA has provided advice to
mitigate risks as far as possible and the DHSC have agreed to supply key information to MHRA to allow them to
monitor risks closely. These have also been validated by Public Health England Porton Down and University of
Oxford advisory group.
4.1.4 Temperature control
The test cartridge and extraction solution should be stored at ambient temperature (2-30 degrees
Centigrade). The reagents and devices must be at room temperature (15-30 degrees centigrade) when used
for testing.
4.1.5 Instructions for use (IFU)
The manufacturer’s instructions for use can be found here: Innova SARS-Cov-2 Antigen Test IFU
5. Workforce
5.1 Roles and responsibilities
Staff Key Responsibilities
Positions
Covid Responsible for the overall on-site operations at the test site, including day-to-day workforce management.
Coordinator¹/
Team Leader² 1. Oversees day-to-day operations including on-site workforce management, managing site health &
safety and receiving and managing stock
2. Point of escalation for any issues on site, and escalates to local public health officials as appropriate
3. Ensures adherence to SOP throughout operations
4. Responsible for safety and security of the site
5. Responsible for isolating positive subjects from others, informing them about their positive results,
what that means, and then providing them with the PRC kit.
6. If using post-registration journey ensures the registration takes place
7. If subjects raise any data privacy concerns, directs subjects to the Data Privacy Notice which explains
how we will use their data (https://www.gov.uk/government/publications/coronavirus-covid-
19testing-privacy-information)
Quality Lead² 1. Ensures quality assurance, incidents, risks mitigation across the testing service
2. Implements appropriate quality assurance as defined by the programme
3. Implements the incident and risk reporting system that is used within the mass testing programme
4. Reports data to the Mass Testing Quality Committee and MHRA through DHSC Schools and colleges
Team
Schools and Colleges Clinical Standard Operating Procedure 14(designated 5. Undertakes testing staff competency and performance reviews
team
member)
Queue Ensures orderly entry of subjects onto the testing site.
Coordinator¹
1. Ensures crowd control and social distancing is maintained in subject queueing areas
2. Monitors subjects in the queue who are showing symptoms of COVID.
3. Supports general site set up, including appropriate signage to manage subject flow
Registration Responsible for ensuring subjects have registered and distributing test kits on arrival.
Assistant¹
1. Greets subject at arrival, asks them to sanitise hands and ensures the subject is eligible for
asymptomatic testing
2. Checks and confirms relevant consent for testing.
3. Provides instructions to subjects to register their test (as per school/college’s registration plan)
4. Aids the subject in registering for the test if needed
5. Gives subjects their barcodes
6. ‘Drip feeds’ subjects into testing area, ensuring testing area does not exceed maximum capacity
7. Communicates to test subjects the purpose of participating in testing at your site and the testing
journey.
Test Provides guidance to subjects on swabbing as requested and ensures cleaning of booths or sample collection
Assistant² station.
1. Directs subject to available testing stations and directs them to the exit when they are finished
2. On hand to provide subject with additional verbal instructions if required
3. Provides regular cleaning to testing stations throughout day (subjects are also asking to self-clean
between each test)
Processing Prepares test sample for analysis and interprets result.
Operative²
1. Sets up sample for analysis, and pipettes reagent to sample
2. Times the sample analysis
3. Await and read result displayed, and mark it on device
4. Provides to Results Recorder to upload to digital platform
Results Collates results from Processing Operatives and uploads to digital solution.
Recorder¹
1. Reads test result outcome (marked by Processing Operative)
2. Enters result into the results logging web app, if using a locally provided device, or native iOS results
logging app, if using a DHSC provided managed device. This includes scanning of QR code (result is
automatically sent to Test & Trace)
Cleaner1 Keeps the test site clean to prevent cross contamination and Spread of Covid 19
1. Cleans testing bays, and other testing areas as required. As a minimum frequently touched surfaces
should be cleaned twice a day, and one of these should be at the beginning or the end of the day.
2. Cleans the testing site in the case of a spillage
Working alongside the waste services providers to ensure waste is disposed (including health waste)
Notes:
1 Roles should be fulfilled by school staff
2 Roles can be fulfilled by schools’ staff or third parties provided by DfE
The key workforce roles required for asymptomatic testing site on school premises are enclosed below.
Where smaller number of tests are preformed per day, some roles can be removed or merged. The roles
which are commonly merged are grouped by colours.
Schools and Colleges Clinical Standard Operating Procedure 15School Covid Co-ordinator: Schools and colleges may want to include a member of the staff to coordinate the
testing and linked processes such as consent, informing students and parents about positive results,
confirmatory PCR, follow-up on results of PCR test, contact tracing etc.
In case of emergencies including medical emergencies, school/ college should follow their standard response
protocol and provide first aid, contact medical emergency services or GP services, as required. All such
incidents should also be reported to the DfE single point of contact
5.2 Training and competence
An appropriate training package will be in place for operators to be trained to be able to conduct the test in a
safe and effective manner. This package would include the following:
• Watching approved video package which demonstrates how physical tests are conducted
• Read through of materials outlining the infection prevention and control measures and the
appropriate use of personal protective equipment, including the proper procedure for donning and
doffing
• Undertaking several tests under supervision
• Regular audit of performance and overall testing process PPE, dealing with any contamination or
other untoward incidents.
• Regularly (minimum six monthly) undertaking updated online training to ensure standards are
adhered to and any new requirements are included. Or as required should new training modules be
provided
6. Site Set-up
6.1 General site selection criteria
Before testing can begin, the site operator will identify and set up a clinically suitable testing environment on,
at or near their premises. The test site will make considerations for, including but not limited to:
1. Sufficient space for appropriate social distancing
2. Easy to clean floor and surfaces
3. Resistant, non-absorbent flooring
4. Airflow and ventilation, no recirculation
5. Ambient temperature 15-30 C
6. One-way flow from entry to exit as much as possible
7. Clear access to PPE donning and doffing area
8. Ready access to hand hygiene (soap and water/appropriate alcohol-based hand rub)
9. Consideration of the need for privacy for participants to self-administer a test
10. Health and safety, disability access, and fire safety regulations that govern deployment sites
11. De-cluttered surfaces with no personal or non-essential equipment
12. Enough room for storage
13. Appropriate testing site waste management arrangement
Schools and Colleges Clinical Standard Operating Procedure 166.2 Co-located sites:
If another ATS site is used for school testing by local arrangement, it should be run and reported as separate
programme.
School may run business-as-usual (BAU) activities near or at proximity to the test site. While each site setup will
be unique to each school, it is expected that schools and colleges will undertake the following site
considerations in addition to criteria in section 7.1:
1. Test Site should be separate from the main area of business operations for privacy, safe queue
management, and to limit disruption to both testing and BAU activity
2. Where space is limited, test queues should be managed safely to avoid disruption – for example, a
waiting room may be separate and adjacent to a testing room and must allow for appropriate social
distancing
3. Fire, health and safety, and evacuation routes should be clearly marked in line with the rest of the
building
4. Test site and non-healthcare BAU waste should be segregated in accordance with the waste
management section.
5. Courier and waste collection service should be easy to access from your Test Site location.
6.3 Testing site set-up:
The specific configuration of each school site will depend on the volume of tests and infrastructure
constraints. However, where possible, testing will be conducted on multiple participants in parallel. This may
be performed at adjacent sites, and/or in multiple lanes, using a one-way system. Sample lay-out plans for
on-site testing are enclosed in Appendix C.
A typical school testing site set-up will comprise the following:
a) Registration area: Subject consent is checked before providing peripherals, instructions, barcode and
registration card and directing the subject to a swabbing bay.
• If subject has pre-registered then registration desk assistant would also confirm with the
test subject that registration is complete and the barcode is still with the test subject.
b) Swabbing bay: this could be one of the following
• Booth: A dedicated test booth (minimum 1.2 X1.2 m in dimension)
• Open plan station: where “open plan” sample testing stations are provided such as tables
laid out in the school hall, these should be constructed in such a way as to maintain 2m
social distancing.
• Open plan station with screen: a screen could be used in open plan model but not
mandated. This provides some privacy and additional protection from adverse reactions to
the swabbing process (vomiting, sneezing etc.)
List of items typically required at this workstation:
i. Table
ii. Chair (optional)
iii. Mirror iv. Laminated instructions
v. Healthcare waste bins (separate bins for chemical e.g. used test kits and
PPE/wipes), vi. 70% alcohol-based
hand rub dispenser
Schools and Colleges Clinical Standard Operating Procedure 17c) Receiving area: located on the opposite side of the testing stations from where Test Assistant can
observe up to 5 booths and receive swabs from participants. List of items typically required at this
workstation:
i. Extraction fluid
ii. Extraction tubes
iii. Sterile swabs iv. Healthcare waste bins
v. Disinfectant spray bottle with paper towel/ wipes
d) Processing area:
This should have sufficient flat surface area with adequate light. The analysis area will include dedicated
space for LFD timing, reading and recording
List of items typically required at this workstation:
i. LFD cartridges
ii. Extraction solution
iii. Extraction tube nozzles
iv. Tube racks or equivalent for holding extraction tubes (schools may procure
microarray tube racks commonly used in chemistry labs)
v. Healthcare waste bins
vi. Disinfectant spray bottle with paper towel/ wipes
vii. Timing clock(s)
viii. Permanent marker pens (see below: for requirements)
ix. Trays (to be cleaned with alcohol after each LFD batch has been transferred to the
processing/results table)
e) Recording area:
This can be a separate table where the marked LFDs can be collected for scanning and
uploading.
List of items typically required at this workstation:
vi. Marked LFD cartridges
vii. Healthcare waste bins
viii. Disinfectant spray bottle with paper towel/ wipes
ix. Barcode Scanner
x. Scanning device
7. Testing Process
All subjects will be required to wear appropriate face covering or face mask at arrival and must endeavour to
maintain social distancing of at least 2 metres from each other and the staff apart from when being tested.
7.1 Consent
Participation is voluntary for the programme. Consent is required either by participants or parents /legal
guardians, as appropriate, who thereby also agree to provide any confirmatory tests results to the school.
Consent needs to be for weekly testing and for daily contact testing component of the programme.
Schools and Colleges Clinical Standard Operating Procedure 18People who decline to participate in daily contact testing will follow the usual national guidelines and are legally
obliged to self-isolate according to the advice given to them by the NHS Test and Trace service.
For looked after children, local authorities may already have arrangements in place that cover medical
treatment, which may extend to this sort of testing. Where that is not the case, parental consent should be
secured via the child’s social worker, who may need to contact the birth parents or other persons who hold
parental responsibility.
Each school is responsible for taking and tracking consent for participation and communicating the purpose of
the testing to develop an understanding of the service amongst the participants and wider community
stakeholders.
A consent template is enclosed in Appendix H.
Students under 18
11-15 year olds may self-swab with supervision of a parent /guardian/ appropriate member of staff with
consent of parent/ guardian.
Young people aged 16-17 are able to consent to their own medical treatment without parent or guardian
present and therefore can self-swab without supervision.
Young people with SEND aged 16 to 25 years old do not need parental consent, provided that they are Gillick
Competent and able to make the decision for themselves. However, the setting will need to decide whether
the pupil can reasonably provide informed consent on their own behalf and may need to consider undertaking
a Mental Capacity Assessment if appropriate. Settings may want to draw on any MCAs completed for the
student previously, including referring to parents if the parent has acted as the Appropriate Person for previous
decisions. Students themselves should be given the opportunity to express their views and preferences to the
extent that they are able. Schools should keep a record of how the decision on consent was made.
Under circumstances where a subject is unable to swab themselves such as due to physical disability or
special needs, they may be swabbed by
- a parent/ guardian, guided by a Test Assistant
- an adequately trained school staff member (where permission and consent of the parent/
guardian has been taken as part of initial consent process)
- trained swabbers who are part of testing workforce
For children or young people where it has been determined that they will be unable to swab themselves, and
the parent/guardian is not swabbing, consent should be sought to enable a third party to do this.
7.2 Eligibility
Eligibility criteria for testing includes
• Asymptomatic subjects who have provided
- Consent to LFD self-test for active case finding
- Consent to daily contact testing (optional)
- Consent to provide LFD and confirmatory PCR test results to the school - Consent to
share data with the National T&T programme
• Symptomatic individuals should be advised to book a PCR test on your NHS App, or online
https://www.gov.uk/get-coronavirus-test or by calling 119.
Schools and Colleges Clinical Standard Operating Procedure 19• Testing someone with a recent Covid-19 diagnosis: Current advice is that for most a previous
confirmed Covid-19 diagnosis in the last 90 days is likely to make testing with an LFD antigen test not
necessary. If these individuals choose to have an LFD test as part of this programme, please ensure
the LFD test is not taken whilst they are within period of isolation following the last confirmed test. If
symptoms persist, this could be longer than the normal 10day self-isolation period for confirmed
cases.
7.3 Test Register
The COVID-19 Test Register is a locally managed register each test site must maintain.
Purpose
• It allows subjects that have tested positive or have a void test to be identified locally
• It keeps a record of everyone that has taken a test at the site/institution
• It allow schools to keep their own records of results (Data retention: It should be kept a minimum of
14 days and must be securely destroyed after 1 month.)
• It helps manage consent
We recommend this is managed through a spreadsheet in a secure cloud-enabled service.
This is separate to the legal requirement of registering each test and recording the results on the systems
managed by NHS Test and Trace.
What fields does the COVID-19 Test Register need to contain?
• Name of student
• Consent given (Y/N)
• Student ID (such as DoB, Student UPN)
• Barcode
• Result
What the COVID-19 Test Register must be used for?
• Record when a subject has taken a test
• Record or attach the barcode that the subject has attached to their test kit
• Matching and recording positive and void test results with subjects
Who can handle data in the COVID-19 Test Register?
• Staff handling the register must have been recruited following Keeping Children Safe in Education
Part 3.
7.4 Registration of each test for Test & Trace purposes
(Using the Register a coronavirus test (lateral flow test) service)
There is a legal obligation to ensure all test kits are registered via the Lite Registration service, but
schools and colleges can identify their own process for enforcing this. [Details TBC later]
Tests can be registered via the Lite Registration service in the following timescales:
• up to 24 hours before a test
• up to 24 hours after a test for a positive or void result
• up to 7 days after a test for a negative result
Schools and Colleges Clinical Standard Operating Procedure 20Every new test instance requires registration.
Where individuals register the test themselves, those over the age of 16 can create an account to save their
personal details after the first registration, so that they only input in subsequent registrations is the test-
specific barcode.
What data is required for registration via the Lite Registration service?
• Test subject's name
• Test subject's NHS number (optional)
• Test subject's (or parent's/carer's) contact mobile number
• Test subject's (or parent's/carer's) email address
• Test-specific unique barcode
An automated notification of the test result will be sent to the mobile number and email address supplied Is
this the same as the COVID-19 Test Register?
No, the COVID-19 Test Register is locally managed and separate to the ATS Test Registration and logging
system managed by NHS Test and Trace.
How long does the registration process take?
In our University pilots it took up to 8 minutes for a student to register.
Daily contact testing
School will need to identify the contacts of a confirmed case and identify those who have consented for daily
contact testing. Registration for LFD daily test will be done as above with the Test-site web app for those being
tested at school.
7.5 Face coverings
Individuals should not attend a test site unless wearing an appropriate face covering. Face coverings are not
required for individuals who:
• cannot put on, wear or remove a face covering because of a physical or mental illness or impairment
or disability
• speak to or provide assistance to someone who relies on lip reading, clear sound or facial expression
to communicate
7.6 End to end testing process overview
The user journey for institutions to register online and set up their test sites and testing operatives is depicted
below:
Schools and Colleges Clinical Standard Operating Procedure 21The user journey for on-site self-swabbing model is depicted below:
Figure 3: NHS Test & Trace LFD user journey
Schools and Colleges Clinical Standard Operating Procedure 227.7 Detailed testing process for on-site testing
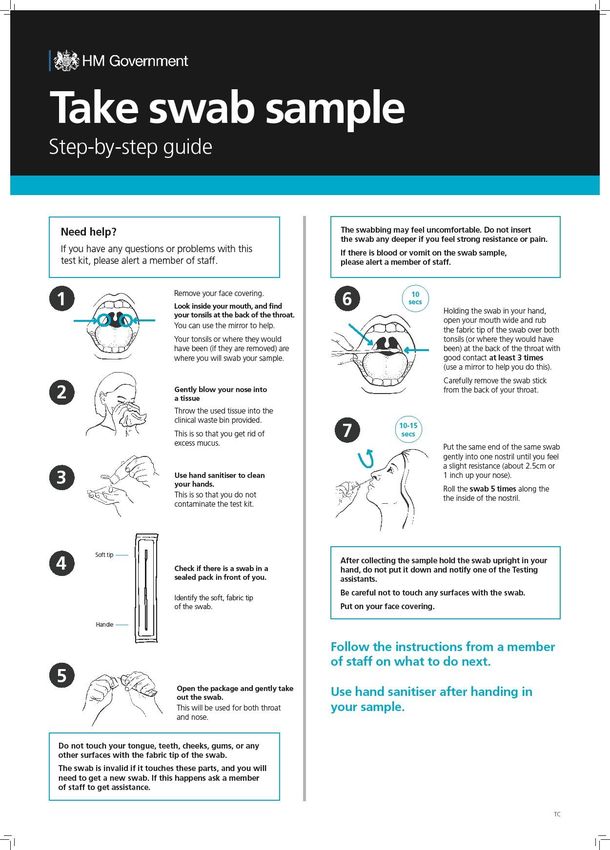
7.7.1 Self-swabbing sample collection procedure:
1. Before commencing swabbing, the process should be explained to the subject. (The subject should
also be informed that the swab may sometimes make them gag and they should use a sick bowl for
any expectoration or vomit.)
2. Subject should be given a sealed sterile swab directed to a sample collection booth from the check-in
zone.
3. Once at the sample collection station, the barcode should be handed to the Processing Operative.
4. The subject should remove mask.
5. The subject should open their mouth and visually identify the left and right tonsils (or tonsillar pits
for subjects with the previous tonsillectomy). A mirror should be provided in each booth for this.
6. The subject should complete hand hygiene using the alcohol-based hand rub provided in the booth.
7. The swab should be removed from sterile packaging by the subject.
Schools and Colleges Clinical Standard Operating Procedure 238. The swab should be kept dry before taking a sample from the back of the throat and therefore it
must not touch any surfaces including the teeth, gums, and tongue or cheek surfaces when
conducting the test.
Figure 4a Swab rubbing the tonsils Figure 4b: Swabbing one nostril
9. Holding the swab in their hand, the subject should open their mouth wide and rub the fabric tip of
the swab over both tonsils (and where they would have been) at the back of the throat with good
contact at least 3 times. Carefully remove the swab stick from the back of the throat taking care to
ensure that it does not come into contact with any other structure or surface.
Note: The swab will be invalid if it touches these parts during or after sampling and it must be put in
healthcare (chemical) waste container and a fresh swab selected.
Note: In the event that a subject vomits, operations at the testing bay shall be ceased and the site
personnel should follow the spillage guidelines until the area has been cleaned adequately to allow
resumption.
10. The subject should then insert the same swab into one nostril. The swab tip should be inserted up to
2.5 cm (1 inch) from the edge of the nostril. Roll the swab 5 times along the mucosa of the inside of
the nostril to ensure that both mucus and cells are collected.
Note: Where there are physical/medical issues or an individual has a very sensitive gag reflex that
prohibits the throat swab from being completed successfully, double nasal swabbing can be
undertaken. Under circumstances, where a nasal swab is not feasible (e.g. a student is prone to nasal
bleeds), it is acceptable to swab only the back of the throat without nostrils.
11. The subject will be required to place their swab directly into the prepared extraction tube on the
bench at the window with the cotton bud end facing down.
Note: The subject should not grasp the cotton bud end, which has been in contact with the tonsils
and nostril.
12. The subject will complete hand hygiene using alcohol-based hand rub in the booth. If the operational
model includes the subject handling any equipment (e.g. hand mirror) they should disinfect the
surfaces with anti-viral wipes
13. The subject will put back on their face covering and leave the site.
Schools and Colleges Clinical Standard Operating Procedure 24You can also read